
Abstract
Purpose of review
The purpose of this review is to provide an overview of ten unique breast cancer subtypes and their clinicopathologic features and treatment implications.
Recent findings
Recent findings show that while many subtypes (mucinous, papillary, tubular, apocrine) have favorable biology, with better overall survival than invasive ductal carcinoma, some (metaplastic, adenoid cystic) are more aggressive portending worse prognosis for patients.
Summary
The differences in histology represented in these breast cancer subtypes often impacts biology, behavior, and prognosis. Due to their rarity, additional research is needed to implement clear treatment protocols for each subtype.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Primary breast carcinomas are largely of ductal or lobular histology; however, there are a myriad of other subtypes less commonly seen. While most breast cancers do fit within these two primary groupings, patients may present with unique subtypes on core biopsy or final pathology that warrant individualized consideration. It is imperative for the multidisciplinary oncology team to be knowledgeable of histologies beyond the classic ductal and lobular histologies as they may impact individualized treatment plans. In this comprehensive review, we describe ten unique breast cancer subtypes, their epidemiology, clinicopathological characteristics, available outcomes data, and treatment implications.
Apocrine Breast Carcinoma
Apocrine breast carcinoma (APC) was first described as a unique pathological entity in the 1960s [1, 2]. The World Health Organization (WHO) currently requires ≥ 90% of tumor cells have apocrine morphology on microscopic examination to fit this diagnosis [3]. Histologically, APC is characterized by large cells with round nuclei, prominent nucleoli and an abundance of granular eosinophilic cytoplasm, reminiscent of apocrine sweat glands [3, 4]. In addition to characteristic morphology, APC has a distinct biomarker profile, being estrogen receptor (ER) and progesterone receptor (PR) negative and androgen receptor (AR) positive and displaying expression of either human epidermal growth factor-2 (HER2) or epidermal growth factor receptor (EGFR) [5, 6]. (Fig. 1A). APCs have also been noted to demonstrate mRNA and protein expression for the marker gross cystic disease fluid protein 15 (GCDFP-15) by immunohistochemistry (IHC) and in situ hybridization [7]. GCDFP-15 is highly specific for mammary, and apocrine differentiation as it is regulated by the AR.

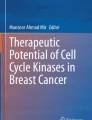
A: Apocrine carcinoma (H&E, 200x); B: Invasive ductal carcinoma with medullary pattern (H&E, 200x); C: Adenoid cystic carcinoma (H&E, 200x); D: Invasive lobular carcinoma with signet ring features (H&E, 200x);E: Tall cell carcinoma with reversed polarity (H&E, 200x); F: Spindle cell metaplastic carcinoma (H&E, 200x); G: Metaplastic carcinoma with heterologous (chondromyxoid) mesenchymal differentiation (H&E, 200x); H: Neuroendocrine carcinoma (H&E, 200x); I: Tubular carcinoma (H&E, 200x); J: Mucinous carcinoma (H&E, 200x); K: Encapsulated papillary carcinoma (H&E, 20x); L: Solid papillary carcinoma (H&E, 20x)
The annual incidence of APC is estimated to be 3–4 per 1 million women based on a 2021 analysis of the Surveillance, Epidemiology, and End Results (SEER) database which analyzed data from 2004–2017 and is currently the largest analysis of patients with APC (N = 2,234) [8]. These tumors are seen more frequently in younger women, are more commonly found in Asian women, and approximately 50% are classified as triple-negative (TN) receptor subtype. Treatment of APC is like other types of breast cancer, with multimodal management of surgery, systemic therapy, and radiation. In a cohort of 1486 cases of APC evaluated by Mills et al. using the National Cancer Database (NCDB) from 2004–2012, 57.5% received chemotherapy. In another NCDB analysis by Arciero et al., comparing triple negative APC to ductal TNBC, the rates of surgery and radiation were similar [9].
One may assume that with a less favorable receptor status, APC tumors would have poor prognosis. However, as shown in the SEER analysis, the 7-year disease specific survival of 85% appears to be similar to patients with non-APC tumors. Additionally, when compared to other triple-negative breast cancers, TN-APC have better survival (86% vs 74%, p < 0.001) [8].
In the NCDB cohort, multivariate analysis of prognostic factors related to overall survival, use of chemotherapy was not significant (p = 0.25) [10]. Similarly, a retrospective Italian study of 36 women with primary non-metastatic TN-APC who did not receive chemotherapy observed no difference in invasive-disease-free survival when compared to 24 patients with ductal TNBC and 12 patients with TN-APC who received chemotherapy [11].
Better outcomes in this subgroup of patients have resulted in question of chemotherapy benefit and de-escalation of therapy. A nomogram has been developed to predict overall survival for patients with TN-APC based on SEER data in hopes of identifying patients at lower risk [12]. Ongoing and future efforts are underway to identify specific therapeutic targets for APC and promising work has been seen in understanding the key role the androgen-receptor (AR) and p62 play in APC [13, 14].
Breast Carcinoma with Medullary Features
Medullary breast carcinoma was first described in the 1970’s and is characterized by the following 5 pathologic features: an expanding border microscopic circumscription, syncytial growth pattern, lack of ductal or tubular differentiation, high nuclear grade, and prominent associated lymphoplasmacytic infiltrate [15,16,17]. (Figure 1B). In 2012, the WHO expanded the classification of medullary carcinoma to describe features of breast carcinomas rather than classifying it as a single type of breast cancer. Currently, the WHO classifies tumors with this morphology as having “medullary pattern.” Biomarker expression varies, with the tumors most often TN but have been shown to demonstrate expression of ER and/or PR (< 10 to 32% of cases) and HER2 (11.0 to 20.5%) [18,19,20,21].
Medullary carcinoma comprises less than 5% of all mammary cancers. Affected patients tend to be younger, present with higher T stage, and there is a possible association with BRCA1/2 carriers. In a cohort study of 46 patients with medullary breast carcinoma by Vu-Nishino et al., 26% of patients were age 35 years or younger compared to only 6% in the control group.
Additionally, of the patients that underwent genetic testing, half had deleterious mutations in BRCA1/2[22]. Although these tumors are frequently TN, some retrospective studies show a more favorable prognosis compared to other TNBC of ductal histology and when compared to other stage-matched high grade breast cancers [23, 24].
Lastly, whether tumors have a typical or atypical appearance does not appear to influence patient prognosis based on a NCDB cohort analysis [25, 26••]. These findings were confirmed by a retrospective analysis from the SEER database in 2016 revealed that patients with medullary breast carcinoma were more likely to have TN disease (56.4%) but propensity score matching demonstrated no difference in overall survival (OS) or breast-cancer-specific survival when compared to other patients with IDC, or to other TNBC [27]. While the majority of these patients received systemic chemotherapy (74.5%), a separate analysis showed better OS in the 174 patients with medullary breast cancer who did not receive chemotherapy when compared to 507 who did, questioning the benefit in all patients [28].
Adenoid Cystic Breast Carcinoma
Adenoid cystic breast carcinoma (ACC) is a salivary gland-type tumor of the breast and has the most favorable long-term outcomes of any TNBC. On histopathology, it is typically a dual cell population that grows in sheets with associated fused glands comprised of myoepithelial and luminal epithelial cells arranged in tubular, cribriform, and solid nested patterns with associated basophilic matrix material [29, 30]. Figure 1C. ACC are further subtyped as classic adenoid cystic, solid-basaloid, and adenoid cystic carcinoma with high grade transformation [31]. Most ACC display MYB-NFIB gene fusion [32].
ACC is one of the rarest of the rare breast cancer subtypes (< 0.1% of all breast malignancies) with only case reports and small case series reported in the literature. This paucity of data results in lack of consensus regarding optimal therapy for these patients. Surgery is a mainstay of treatment, but the use of adjuvant chemotherapy remains controversial. In a population-based study by Li et al., utilizing the SEER database, only 12.4% of patients received adjuvant chemotherapy. Patients with lymph node metastasis, stage IIB and III, histological grade ≥ 2, and no radiation had worse breast cancer-specific survival (BCSS) (p < 0.05). Adjuvant chemotherapy did not improve OS or BCSS. [33]
In all series, > 50% of these tumors are classified as TN, appear to have a favorable prognosis with low rates of nodal involvement, and are seen in women age > 50 [34,35,36,37,38]. In NCDB analyses of TNBCs with varying pathological subtypes, ACC consistently had a significantly improved overall survival compared to non-ACC TNBC [9, 24] with 5-year overall survival rates estimated at 88.4% (all stages combined). When examining OS for all patients with ACC, researchers using the California Cancer Registry identified an OSS rate of 95.6% at 5 years and 94.9% at 10 years [36]. While a very rare and understudied pathology, ACC appears to have quite favorable outcomes – even amongst those with TN disease.
Signet Ring Cell Breast Carcinoma (SRCBC)
Signet ring cell breast carcinoma was first described in the 1970s as subtype of invasive lobular carcinoma (ILC) and was re-classified by the WHO has a unique form of breast cancer pathology in 2003 [39]. This entity is classified histologically as having the presence of intracytoplasmic, mucin rich values in ≥ 20% of the cells which attribute a signet ring shape to the cell. These tumors can sometimes be mistaken for metastasis from other organ sites, such as gastrointestinal signet ring cell carcinoma; however, SRCBC is typically keratin 7-positive and keratin 20-negative and these stains, along with ER-staining and other breast-specific markers, can be supportive of a SRCBC diagnosis [40]. (Figure 1D.) Currently, the WHO includes SRCBC as a morphologic pattern of ILC. Other ILC patterns include the histiocytoid, solid and alveolar-lobular patterns.
Similar to other subtypes, data for SRCBC consists of mostly case reports and small institutional series. The largest retrospective study identified 324 cases of SRCBC in the NCDB from.
2004–2016, representing only 0.01% of all breast carcinomas diagnosed during that time [39]. Most tumors in this series were higher grade and approximately 35% of patients had Stage IV disease at the time of diagnosis, indicative of the aggressive nature of this rare variant [39]. Previous retrospective series found 7-year disease-specific mortality rates to be as high as 70% for patients diagnosed with SRCBC but with worse outcomes for those with Stage IV disease [41,42,43]. Patients in the NCDB series with ER-positive disease had improved OS compared to those with ER-negative disease; however, receipt of adjuvant endocrine therapy for those with ER + disease was surprisingly not associated with a survival benefit – questioning whether this was endocrine resistance, lack of compliance, or other factors [39].
Tall Cell Carcinoma with Reversed Polarity
Tall cell carcinoma with revered polarity of the breast (TCCRP) is a recently described TNBC with less than 100 reported cases in the literature as of August 2023 [44]. Previously, it was thought to be a variant of papillary carcinoma but was classified as a specific breast carcinoma pathology by the WHO in recent years. Histologically, it resembles the tall cell variant of papillary thyroid carcinoma but is a primary breast carcinoma and, as such, is negative for typical thyroid immunohistochemical markers such as thyroglobulin and thyroid transcript factor 1 (TTF-1) [45,46,47]. It is characterized by columnar cells with reversed nuclear polarity (the nuclei are present at the apical poles instead of basal) arranged in a solid, papillary pattern [48]. While the etiology of TCCRP is unclear, it is hypothesized that these lesions may originate from intraductal papillomas or other papillary lesions of the breast. (Figure 1E.) TCCRP frequently harbor IDH2 p.Arg172 hotspot mutations [49].
Most cases of TCCRP have been seen in post-menopausal women and is it usually detected as a mass on breast imaging [31, 48, 50]. Over two-thirds of those described in the literature are TNBC; however, like other rare forms of TNBC, TCCRP has a more favorable prognosis [51, 52]. Limited data exists on this breast cancer subtype and future cohort studies are needed to further describe prognosis and clinical outcomes for patients diagnosed with this disease.
Metaplastic Breast Carcinoma
Metaplastic breast carcinoma (MBC) was first recognized as a unique histologic subtype in 2001 [53], at which time specific diagnosis codes were also created distinguish it from other grouped entities like breast sarcomas [54]. Metaplastic carcinomas are a group of invasive tumors with heterogeneity and differentiation toward metaplastic components [55]. Subtypes described by the latest World Health Organization (WHO) include low grade adenosquamous, fibromatosis-like metaplastic (low nuclear grade), squamous cell, spindle cell (intermediate to high nuclear grade) (Fig. 1F.), and carcinoma with heterologous mesenchymal differentiation [56, 57]. (Figure 1G.)
MBC is exceedingly rare, accounting for approximately only 0.25%-1% of breast cancer diagnoses [58]. In general, MBC differs from classic IDC in that patients present with larger primary tumors secondary to rapid growth rate. While only 5.3% of IDC are over 5 cm, > 20% of MBC are > 5 cm at diagnosis. Many (> 90%) of metaplastic carcinomas are TN, supporting their classification among basal carcinomas [59]. These aggressive tumors portend a worse prognosis than non-metaplastic breast cancers (78% vs 93%, p < 0.0001) [57].
In a NCDB series, 892 patients with MBC were identified from 2001–2003 and compared to > 200,000 patients with IDC [54]. The analysis showed that MBC is more commonly diagnosed in African American and Latinx women and despite higher AJCC stage (due to larger tumor size) MBC had a lower incidence of axillary lymph node involvement, with hematogenous spread being more common [61, 62]. While these tumors are traditionally chemoresistant, SEER analysis of 2412 patients demonstrated use of chemotherapy was associated with improved OS in non-metastatic MBC [53, 62, 63]. Outcomes have improved with multimodal treatment, but the overall survival remains poor [64]. Similar results were shown by Nelson et al. who also evaluated survival outcomes after 10 years of available data. In this matched cohort study using SEER, patients with MBC had significantly worse disease specific survival rates than patient with IDC (78% vs 93%, p < 0.001) [60].
Neuroendocrine Breast Carcinoma
Primary neuroendocrine neoplasms (NEN) of the breast are rare, accounting for 0.1–1% of all breast cancers. NEN were recognized as a distinct clinical and histopathological entity in 2003 [65]. These are subdivided into two groups: well-differentiated neuroendocrine tumors (NET) and poorly differentiated neuroendocrine carcinoma (NEC). Neuroendocrine carcinoma (NEC) is characterized by high-grade neuroendocrine morphologic features and immunophenotype and include small cell and large cell variants [66, 67]. In addition to distinct morphological features, these tumors must express markers such as chromogranin A and synaptophysin in > 50% of tumor cells [68]. (Figure 1H.) Both subtypes often demonstrate areas of necrosis and a high mitotic count but have been reported to be ER + in up to 50% of cases. [69, 70]. These tumors are also less likely to be hormone receptor positive or HER2 positive [71].
Due to their rarity, NECs have traditionally been treated like ductal or lobular carcinomas. Martinez et al. completed the largest study to date using the NCDB. They compared 1389 NEN to a matched IDC cohort and found that NEN patients were treated with surgery and radiotherapy less often than patients with IDC but received systemic treatment more often [72•]. Specifically, patients with NEC seem to garner most benefit from systemic therapy while NET show little difference in survival [71]. Yang et al. found similar results with NEN patients presenting at slightly younger age than those with IDC, higher histologic grade, and at higher clinical stage with > 10% presenting with Stage IV disease.
Information on specific systemic chemotherapy regimens is limited, but Chai et al. noted that NEN patients who received chemotherapy with anthracycline/taxane and or taxane-containing regimens had better OS and DFS than those without those regimens [73]. Patients with NEN have significantly worse overall survival than patients with IDC. The prognostic relevance of NEN remains controversial with several series showing worse clinical outcome [72, 74, 75], but others that show similar outcomes to IDC [76, 77]. Despite growing research in this area using somatostatin analogs and anti-angiogenic agents, no clear treatment protocol currently exists.
Tubular Breast Carcinoma
Tubular breast carcinomas (TC) are a variant of invasive ductal carcinoma characterized by well-formed tubular glandular structures that mimic normal mammary glands. TC account for approximately 1–2% of all breast carcinomas [78] and is a low-grade carcinoma defined by ≥ 90% simple, angulated tubules lined by a single layer of neoplastic epithelium with prominent apical tufts with infiltrative growth and associated desmoplastic stroma. (Figure 1I.)
TC has been associated with several precursor lesions, namely the “Rosen triad” of TC, lobular neoplasia, and columnar cell lesions. In a study of 147 tumors, columnar cell lesions (e.g., flat epithelial atypia) and atypical ductal hyperplasia (ADH)/ductal carcinoma in situ (DCIS) have been seen together with TCs in 95% and 89% of cases [79]. The presence of these associated lesions suggests possible biologic progression from these lesions [80].
Tubular cancers are diffusely ER positive, most often PR positive, and HER2 negative [81]. They are generally well-differentiated, early stage, node negative, with favorable biologic behavior, leading to overall good prognosis [82,83,84]. The incidence of metastasis is much lower than for IDC, ranging from 8–20% and the overall survival remains excellent even if metastasis occurs. Local and distant disease recurrence are also uncommon [85]. Treatment for tubular carcinoma is largely guided by tumor receptor status, following current protocols for HER2 + breast cancer. The surgical approach remains similar to IDC, but the importance of axillary staging remains controversial as many patients present with early stage, node negative disease. Knape et al. suggest that SLNB could be omitted in select postmenopausal women with early stage, ER/PR + HER2-, special histologic subtype, such as tubular carcinoma [86]. Per the NCCN, adjuvant endocrine therapy is standard for patients with tumors > 3 cm and/or nodal positivity, but not routinely recommended for patients with tumors < 3 cm with node-negative disease, leaving room for multidisciplinary decision making [87]. Adjuvant systemic chemotherapy can be considered for patients with node positive disease, though its efficacy remains unclear, and most providers report not offering it given the overall good prognosis of this subtype [85, 88]. Turashvili et al. explored the use 21-gene recurrence score (RS) in rare histologic subtypes. They included 10 patients with tubular carcinoma, with a median RS of 14 (range 9–23). This suggest that reflex RS testing may be deferred in subtypes with favorable histology [89].
Mucinous Breast Carcinoma
There is a spectrum of mucinous containing breast lesions that range from benign to malignant, often making the diagnosis challenging on core biopsy. For the purposes of this review, we will focus on mucinous carcinoma (2–4% of all breast cancers) but recognize that there are other malignant mucinous lesions such as mucinous ductal carcinoma in situ, mucinous cystadenocarcinoma, mucoepidermoid type lesions, all differentiated by varying amounts of extracellular and/or intracellular mucin [90, 91]. Mucinous carcinoma is characterized by epithelial cells suspended in abundant extracellular mucin. The epithelial cells may vary in size, shape, and nuclear atypia; but are predominantly low to intermediate in grade [92, 93]. Pure mucinous carcinoma requires ≥ 90% of the tumor to exhibit mucinous features, while mixed is classified from 10 to < 90%. (Figure 1J.) Pure mucinous carcinoma is typically ER/PR + , and HER2-. These tumors are generally diagnosed in peri/postmenopausal women, are low grade, and node negative [94].
The distinction between pure and mixed subtypes is important as it informs treatment. Patients with mixed mucinous tumors should be managed similar to other patients with IDC. Per NCCN guidelines, sub-centimeter pure mucinous ER/PR + tumors without nodal involvement can be treated with surgery alone with omission of endocrine therapy [95]. Lymph node metastasis can occur and are more often seen in mixed type, but less frequently than is seen in invasive ductal carcinoma [96]. Overall, they have a good prognosis with a 10-year survival of 90% for pure mucinous carcinomas [97]. Mixed type mucinous carcinoma tends to carry a worse prognosis, with more frequent nodal involvement and surgery with or without adjuvant chemotherapy remains the mainstay of treatment [98].
Papillary Breast Carcinoma
Papillary carcinomas were initially differentiated from benign papillomas of the breast in 1962 by Kraus and Nubecker [99, 100]. Papillary carcinomas of the breast are uncommon, representing approximately 0.5% of newly diagnosed cancers [101]. Like other subtypes, there are several distinct lesions within papillary carcinomas including 1) encapsulated papillary carcinoma (EPC) (Fig. 1K.), 2) solid papillary carcinoma (SPC) (Fig. 1L.), and 3) invasive papillary carcinoma, and all share an arborescent growth pattern [102, 103]. EPCs are well-circumscribed masses within cystic spaces with pushing growth surrounded by a fibrous border, while SPCs demonstrate a solid growth pattern of rounded nests within fibrotic stroma. Both EPC and SPC, when showing well-structured, circumscribed patterns of growth are classified as in situ lesions (i.e., a variant of DCIS) by the WHO (as of the 5th edition) [104]. Papillary carcinoma can rarely show infiltrative growth; when papillary features comprise > 90% of the tumor, the carcinoma is classified as invasive papillary carcinoma per WHO classification (5th edition) [104]. More often EPC or SPC is associated with more common subtypes of invasive carcinoma, most frequently ductal but also lobular and mucinous types. In these scenarios, infiltrative growth is what drives the stage. For example, if SPC with a morphologically in situ growth pattern extends over a greater extent but there is an associated microinvasive ductal component, the stage would be pT1mi based on the component of invasion. For invasive papillary carcinoma, the entire tumor would be classified as invasive and pT stage assigned accordingly (e.g., 1.3 cm would be pT1c). Papillary carcinomas are usually low to intermediate grade and may be positive for neuroendocrine markers (synaptophysin, chromogranin, etc. [102].
They are often seen in elderly women (mean of 70 years of age), and largely centrally located [102, 103]. Interestingly, papillary carcinomas are the most common unique subtype found in men. A study performed using the California Cancer Registry found that papillary subtypes were more commonly diagnosed in men in that series [105, 106]. It can present clinically with bloody nipple discharge, a palpable mass or simply seen as a radiologic abnormality [101].
Most papillary carcinomas are ER/PR + , thus portending a favorable prognosis; however, some are high grade and ER/PR- [103]. Axillary staging may be omitted for pure in situ EPCs/SPCs in the setting of breast conservation surgery. High grade EPCs/SPCs should be treated as invasive disease [106, 107]. Previous literature has found that papillary carcinoma has a better prognosis than IDC, though this is based on smaller retrospective studies [108, 109]. Huang et al. used the NCDB to evaluate 1,147 patients with papillary carcinoma compared to > 200,000 patients with IDC and found no difference in survival between papillary carcinoma and IDC, suggesting a similar prognosis [111]. Additional notable findings were that patients with papillary carcinoma were less likely to receive adjuvant chemotherapy or radiation, but rates of endocrine therapy were similar.
Conclusion
This review demonstrates the heterogeneity of breast cancer, particularly those beyond ductal and lobular histologies. The various breast cancer subtypes discussed here have not only distinct histological findings but have unique behaviors that directly impact treatment plans for patients. However, given their rarity, evidence-based treatment protocols are scarce. There is no one size fits all approach to breast cancer treatment, and this will be increasingly true as more is learned about breast cancer biology, anthropology, and the goals and advances of emerging precision medicine [109].
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Apocrine
Krompecher E. Apocrine carcinoma of the breast. Beitr Path Anat. 1916;62:403.
Frable WJ, Kay S. Carcinoma of the breast. Histologic and clinical features of apocrine tumors. Cancer. 1968;21(4):756–63.
Tan PH, Ellis I, Allison K, et al. The 2019 World Health Organization classification of tumours of the breast. Histopathology. 2020;77(2):181–5.
Mills AM, Gottlieb EC, Wendroth MS, Brenin MC, Atkins KA. Pure Apocrine Carcinomas Represent a Clinicopathologically Distinct Androgen Receptor-Positive Subset of Triple-Negative Breast Cancers. Am J Surg Pathol. 2016;40(8):1109–16. https://doi.org/10.1097/PAS.0000000000000671.
Liu X, Feng C, Liu J, et al. The importance of EGFR as a biomarker in molecular apocrine breast cancer. Hum Pathol. 2018;77:1–10. https://doi.org/10.1016/j.humpath.2018.01.016.
Vranic S, Schmitt F, Sapino A, Costa JL, Reddy S, Castro M, Gatalica Z. Apocrine carcinoma of the breast: A comprehensive review. Histol Histopathol. 2013;28:1393–409.
Nozaki F, Hirotani Y, Nakanishi Y, et al. p62 Regulates the Proliferation of Molecular Apocrine Breast Cancer Cells. Acta Histochem Cytochem. 2016;49(4):125–30. https://doi.org/10.1267/ahc.16013.
Saridakis A, Berger ER, Harigopal M, et al. Apocrine Breast Cancer: Unique Features of a Predominantly Triple-Negative Breast Cancer. Ann Surg Oncol. 2021;28(10):5610–6. https://doi.org/10.1245/s10434-021-10518-9.
Arciero CA, Diehl AH III, Liu Y, Sun Q, Gillespie T, Li X, Subhedar P. Triple-negative apocrine carcinoma: A rare pathologic subtype with a better prognosis than other triple-negative breast cancers. J Surg Oncol. 2020Nov;122(6):1232–9.
Mills MN, Yang GQ, Oliver DE, et al. Histologic heterogeneity of triple negative breast cancer: A National Cancer Centre Database analysis. Eur J Cancer. 2018;98:48–58. https://doi.org/10.1016/j.ejca.2018.04.011.
Montagna E, Cancello G, Pagan E, et al. Prognosis of selected triple negative apocrine breast cancer patients who did not receive adjuvant chemotherapy. Breast. 2020;53:138–42. https://doi.org/10.1016/j.breast.2020.07.003.
Xu Y, Zhang W, He J, et al. Nomogram for predicting overall survival in patients with triple-negative apocrine breast cancer: Surveillance, epidemiology, and end results-based analysis. Breast. 2022;66:8–14. https://doi.org/10.1016/j.breast.2022.08.011.
Liu X, Feng C, Liu J, et al. Androgen receptor and heat shock protein 27 co-regulate the malignant potential of molecular apocrine breast cancer. J Exp Clin Cancer Res. 2018;37(1):90. https://doi.org/10.1186/s13046-018-0762-y.
Darb-Esfahani S, von Minckwitz G, Denkert C, Ataseven B, Högel B, Mehta K, Kaltenecker G, Rüdiger T, Pfitzner B, Kittel K, Fiedler B, Baumann K, Moll R, Dietel M, Eidtmann H, Thomssen C, Loibl S. Gross cystic disease fluid protein 15 (GCDFP-15) expression in breast cancer subtypes. BMC Cancer. 2014;14:546. https://doi.org/10.1186/1471-2407-14-546.
Medullary
Ridolfi RL, Rosen PP, Port A, Kinne D, Miké V. Medullary carcinoma of the breast: a clinicopathologic study with 10 year follow-up. Cancer. 1977Oct;40(4):1365–85.
Quinn, C., D’Arcy, C. (2018). Invasive Carcinoma with Medullary Features. In: van Krieken, J. (eds) Encyclopedia of Pathology. Encyclopedia of Pathology. Springer, Cham. https://doi.org/10.1007/978-3-319-28845-1_4714-2
Gaffey MJ, Mills SE, Frierson HF Jr, Zarbo RJ, Boyd JC, Simpson JF, Weiss LM. Medullary carcinoma of the breast interobserver variability in histopathologic diagnosis. Modern Pathol: Official J United States Canadian Academy Pathol, Inc. 1995;8(1):31–8.
Huober J, Gelber S, Goldhirsch A, Coates AS, Viale G, Öhlschlegel C, Price KN, Gelber RD, Regan MM, Thürlimann B. Prognosis of medullary breast cancer: analysis of 13 International Breast Cancer Study Group (IBCSG) trials. Annals Oncol : Official J Eur Soc Med Oncol. 2012;23(11):2843–51. https://doi.org/10.1093/annonc/mds105.
Jacquemier, J., Padovani, L., Rabayrol, L., Lakhani, S. R., Penault-Llorca, F., Denoux, Y., Fiche, M., Figueiro, P., Maisongrosse, V., Ledoussal, V., Martinez Penuela, J., Udvarhely, N., El Makdissi, G., Ginestier, C., Geneix, J., Charafe-Jauffret, E., Xerri, L., Eisinger, F., Birnbaum, D., Sobol, H., … Breast Cancer Linkage Consortium. Typical medullary breast carcinomas have a basal/myoepithelial phenotype. J Pathol. 2005;207(3):260–8. https://doi.org/10.1002/path.1845.
Martinez SR, Beal SH, Canter RJ, Chen SL, Khatri VP, Bold RJ. Medullary carcinoma of the breast: a population-based perspective. Med Oncol (Northwood, London, England). 2011;28(3):738–44. https://doi.org/10.1007/s12032-010-9526-z.
Cao AY, He M, Huang L, Shao ZM, Di GH. Clinicopathologic characteristics at diagnosis and the survival of patients with medullary breast carcinoma in China: a comparison with infiltrating ductal carcinoma-not otherwise specified. World J Surg Oncol. 2013;11:91. https://doi.org/10.1186/1477-7819-11-91.
Vu-Nishino H, Tavassoli FA, Ahrens WA, Haffty BG. Clinicopathologic features and long-term outcome of patients with medullary breast carcinoma managed with breast-conserving therapy (BCT). Int J Radiation Oncol Biol Phys. 2005;15;62(4):1040–7.
Kouhen F, Benhmidou N, Afif M, Rais F, Khamou M, Khanoussi B, El Menaoui O, Elkacemi H, Elmajjaoui S, Kebdani T, Benjaafar N. Prognosis of Medullary Carcinoma of the Breast: 10 years’ Experience in a Single Institution. Breast J. 2017;23(1):112–4. https://doi.org/10.1111/tbj.12699.
Thurman SA, Schnitt SJ, Connolly JL, Gelman R, Silver B, Harris JR, Recht A. Outcome after breast-conserving therapy for patients with stage I or II mucinous, medullary, or tubular breast carcinoma. Int J Radiat Oncol Biol Phys. 2004;59(1):152–9. https://doi.org/10.1016/j.ijrobp.2003.10.029.
Mateo AM, Pezzi TA, Sundermeyer M, Kelley CA, Klimberg VS, Pezzi CM. Atypical medullary carcinoma of the breast has similar prognostic factors and survival to typical medullary breast carcinoma: 3,976 cases from the National Cancer Data Base. J Surg Oncol. 2016;114(5):533–6. https://doi.org/10.1002/jso.24367.
•• Elimimian EB, Samuel TA, Liang H, Elson L, Bilani N, Nahleh ZA. Clinical and Demographic Factors, Treatment Patterns, and Overall Survival Associated With Rare Triple-Negative Breast Carcinomas in the US. JAMA Netw Open. 2021;4(4):e214123. Published 2021 Apr 1. https://doi.org/10.1001/jamanetworkopen.2021.4123. This paper explores the heterogeneity of triple negative breast cancers by evaluating rare subtypes medullary carcinoma, adenoid cystic carcinoma, and metaplastic breast carcinoma. Its findings suggest that medullary carcinomas were most common, but metaplastic had the worst overall 5-year survival.
Wang XX, Jiang YZ, Liu XY, Li JJ, Song CG, Shao ZM. Difference in characteristics and outcomes between medullary breast carcinoma and invasive ductal carcinoma: a population based study from SEER 18 database. Oncotarget. 2016;7(16):22665–73. https://doi.org/10.18632/oncotarget.8142.
Chen H, Pu S, Wang L, et al. A risk stratification model to predict chemotherapy benefit in medullary carcinoma of the breast: a population-based SEER database. Sci Rep. 2023;13(1):10704. https://doi.org/10.1038/s41598-023-37915-2.
Adenoid Cystic
Marchiò C, Weigelt B, Reis-Filho JS. Adenoid cystic carcinomas of the breast and salivary glands (or “The strange case of Dr Jekyll and Mr Hyde” of exocrine gland carcinomas). J Clin Pathol. 2010;63(3):220–8. https://doi.org/10.1136/jcp.2009.073908.
Miyai K, Schwartz MR, Divatia MK, Anton RC, Park YW, Ayala AG, et al. Adenoid cystic carcinoma of breast: Recent advances. World J Clin Cases. 2014;2(12):732–41. https://doi.org/10.12998/wjcc.v2.i12.732.
Foschini MP, Morandi L, Asioli S, Giove G, Corradini AG, Eusebi V. The morphological spectrum of salivary gland type tumours of the breast. Pathology. 2017;49(2):215–27. https://doi.org/10.1016/j.pathol.2016.10.011.
Kim J, Geyer FC, Martelotto LG, Ng CK, Lim RS, Selenica P, Li A, Pareja F, Fusco N, Edelweiss M, Kumar R. MYBL1 rearrangements and MYB amplification in breast adenoid cystic carcinomas lacking the MYB–NFIB fusion gene. J Pathol. 2018;244(2):143–50.
Li L, Zhang D, Ma F. Adenoid cystic carcinoma of the breast may be exempt from adjuvant chemotherapy. J Clin Med. 2022;11(15):4477.
Goldbach MM, Hoffman DI, Burkbauer L, Nayak A, Tchou J. Treatment Patterns and Clinical Outcomes of Adenoid Cystic Breast Carcinoma: A Single-Institution Experience. Am Surg. 2020;86(12):1684–90. https://doi.org/10.1177/0003134820942287.
Romeira D, Cardoso D, Miranda H, Martins A. Adenoid cystic carcinoma: triple negative breast cancer with good prognosis. BMJ Case Rep. 2016;2016:bcr2015213704. https://doi.org/10.1136/bcr-2015-213704.
Thompson K, Grabowski J, Saltzstein SL, Sadler GR, Blair SL. Adenoid cystic breast carcinoma: is axillary staging necessary in all cases? Results from the California Cancer Registry. Breast J. 2011;17(5):485–9. https://doi.org/10.1111/j.1524-4741.2011.01117.x.
Zhang M, Liu Y, Yang H, Jin F, Zheng A. Breast adenoid cystic carcinoma: a report of seven cases and literature review. BMC Surg. 2022;22(1):113. https://doi.org/10.1186/s12893-022-01560-9.
Treitl D, Radkani P, Rizer M, El Hussein S, Paramo JC, Mesko TW. Adenoid cystic carcinoma of the breast, 20 years of experience in a single center with review of literature. Breast Cancer. 2018;25(1):28–33. https://doi.org/10.1007/s12282-017-0780-.
Signet Ring
Kong MAL, Frebault J, Huang S, Huang CC, Cortina CS. Prognostic Outcomes of Signet Ring Cell Carcinoma of the Breast. J Surg Res. 2021;264:138–48. https://doi.org/10.1016/j.jss.2021.02.020.
Tot T. The role of cytokeratins 20 and 7 and estrogen receptor analysis in separation of metastatic lobular carcinoma of the breast and metastatic signet ring cell carcinoma of the gastrointestinal tract. APMIS. 2000;108:467–72.
Wu X, Zhang Z, Li X, et al. Poorer Prognosis of Primary Signet-Ring Cell Carcinoma of the Breast Compared with Mucinous Carcinoma. PLoS One. 2016;11(9):e0162088. https://doi.org/10.1371/journal.pone.0162088.
Yang W, Ding S, Wang L, et al. Carcinoma with signet ring cell differentiation associated with invasive breast cancer: A case report. Oncol Lett. 2023;25(5):212. https://doi.org/10.3892/ol.2023.13798.
Chatterjee D, Bal A, Das A, Kohli PS, Singh G, Mittal BR. Invasive Duct Carcinoma of the Breast With Dominant Signet-Ring Cell Differentiation: A Microsatellite Stable Tumor With Aggressive Behavior. Appl Immunohistochem Mol Morphol. 2017;25(10):720–4. https://doi.org/10.1097/PAI.0000000000000366.
Tall Cell
Arif FZ, Breese RO, Friend K. Tall Cell Variant of Invasive Papillary Breast Carcinoma [published online ahead of print, 2023 May 5]. Am Surg. 2023;31348231173978. https://doi.org/10.1177/00031348231173978
Eusebi V, Damiani S, Ellis IO, Azzopardi JG, Rosai J. Breast tumor resembling the tall cell variant of papillary thyroid carcinoma: Report of 5 cases. Am J Surg Pathol. 2003;27(8):1114–8.
Chang SY, Fleiszer DM, Mesurolle B, El Khoury M, Omeroglu A. Breast tumor resembling the tall cell variant of papillary thyroid carcinoma. Breast J. 2009;15(5):531–5.
Bhargava R, Florea AV, Pelmus M, et al. Breast tumor resembling tall cell variant of papillary thyroid carcinoma: A solid papillary neoplasm with characteristic immunohistochemical profile and few recurrent mutations. Am J Clin Pathol. 2017;147:399–404.
Foschini MP, Asioli S, Foreid S, et al. Solid papillary breast carcinomas resembling the tall cell variant of papillary thyroid neoplasms: a unique invasive tumor with indolent behavior. Am J Surg Pathol. 2017;41:887–95. https://doi.org/10.1097/PAS.0000000000000853.
Wysocka J. New WHO classification of breast tumours–as published in 2019 Nowotwory. J Oncol. 2020;70(6):250–2.
Lee NY, Chang YW, Lee EJ, Jin YM. Tall cell carcinoma with reversed polarity of breast: Sonographic and magnetic resonance imaging findings. J Clin Ultrasound. 2023;51(3):494–7. https://doi.org/10.1002/jcu.23280.
Lozada JR, Basili T, Pareja F, et al. Solid papillary breast carcinomas resembling the tall cell variant of papillary thyroid neoplasms (solid papillary carcinomas with reverse polarity) harbour recurrent mutations affecting IDH2 and PIK3CA: a validation cohort. Histopathology. 2018;73(2):339–44. https://doi.org/10.1111/his.13522.
Lozada JR, Basili T, Pareja F, Alemar B, Paula ADC, Gularte-Merida R, Giri DD, Querzoli P, Cserni G, Rakha EA, Foschini MP, Reis-Filho JS, Brogi E, Weigelt B, Geyer FC. Solid papillary breast carcinomas resembling the tall cell variant of papillary thyroid neoplasms (solid papillary carcinomas with reverse polarity) harbour recurrent mutations affecting IDH2 and PIK3CA: a validation cohort. Histopathology. 2018;73(2):339–44. https://doi.org/10.1111/his.13522.
Thomas A, Douglas E, Reis-Filho JS, Gurcan MN, Wen HY. Metaplastic Breast Cancer: Current Understanding and Future Directions. Clinical Breast Cancer. 2023 Apr 19.
Metaplastic
Pezzi CM, Patel-Parekh L, Cole K, et al. Characteristics and Treatment of Metaplastic Breast Cancer: Analysis of 892 Cases from the National Cancer Data Base. Ann Surg Oncol. 2007;14:166–73. https://doi.org/10.1245/s10434-006-9124-7.
Hoda SA, Rosen PP, Brogi E, Koerner FC. Rosen’s diagnosis of breast pathology by needle core biopsy. Lippincott Williams & Wilkins; 2016. pp. 238–58.
Dilani L, Valerie AW, Beiko W. WHO Classification of Tumours, Breast tumours. Lyon: International Agency for Research on Cancer; 2019.
Wargotz ES, Norris HJ. Metaplastic carcinomas of the breast. I Matrix-producing carcinoma Hum Pathol. 1989;20:628–35.
Thomas HR, Hu B, Boyraz B, Johnson A, Bossuyt VI, Spring L, Jimenez RB. Metaplastic breast cancer: a review. Crit Rev Oncol Hematol. 2023;22: 103924.
McCart Reed AE, Kalaw E, Nones K, et al. Phenotypic and molecular dissection of metaplastic breast cancer and the prognostic implications. J Pathol. 2019;247(2):214–27.
Nelson RA, Guye ML, Luu T, et al. Survival Outcomes of Metaplastic Breast Cancer Patients: Results from a US Population-based Analysis. Ann Surg Oncol. 2015;22:24–31. https://doi.org/10.1245/s10434-014-3890-4.
Hardy BM, Cortina CS, Javidiparsijani S, Ghai R, Madrigrano A. Hypercalcemia in Metaplastic Squamous Cell Carcinoma of the Breast. Am J Case Rep. 2019;20:366–9. https://doi.org/10.12659/AJCR.912427.
Ong CT, Campbell BM, Thomas SM, Greenup RA, Plichta JK, Rosenberger LH, Force J, Hall A, Hyslop T, Hwang ES, Fayanju OM. Metaplastic breast cancer treatment and outcomes in 2500 patients: a retrospective analysis of a national oncology database. Ann Surg Oncol. 2018;25:2249–60.
Hu J, Zhang H, Dong F, Zhang X, Wang S, Ming J, Huang T. Metaplastic breast cancer: Treatment and prognosis by molecular subtype. Translational Oncol. 2021;14(5): 101054.
Rayson D, Adjei AA, Suman VJ, Wold LE, Ingle JN. Metaplastic breast cancer: prognosis and response to systemic therapy. Ann Oncol. 1999;10(4):413–9.
Eble JN, Tavassoli FA, Devilee P, editors. Pathology and genetics of tumours of the breast and female genital organs. IARC; 2003. pp. 32–4.
Neuroendocrine
Hare F, Giri S, Patel JK, Hahn A, Martin MG. A population-based analysis of outcomes for small cell carcinoma of the breast by tumor stage and the use of radiation therapy. Springerplus. 2015;4:138. https://doi.org/10.1186/s40064-015-0913-y.
Kelten Talu C, Leblebici C, Kilicaslan Ozturk T, Hacihasanoglu E, Baykal Koca S, Gucin Z. Primary breast carcinomas with neuroendocrine features: Clinicopathological features and analysis of tumor growth patterns in 36 cases. Ann Diagn Pathol. 2018;34:122–30. https://doi.org/10.1016/j.anndiagpath.2018.03.010.
Righi L, Sapino A, Marchio C, Papotti M, Bussolati G. Neuroendocrine differentiation in breast cancer: established facts and unresolved problems. InSeminars in diagnostic pathology 2010 Feb 1 (Vol. 27, No. 1, pp. 69–76). WB Saunders. https://doi.org/10.1053/j.semdp.2009.12.003.
McCullar B, Pandey M, Yaghmour G, Hare F, Patel K, Stein K, Feldman R, Chandler JC, Martin MG. Genomic landscape of small cell carcinoma of the breast contrasted to small cell carcinoma of the lung. Breast Cancer Res Treat. 2016;158(1):195–202. https://doi.org/10.1007/s10549-016-3867-z.
Shin SJ, DeLellis RA, Ying L, Rosen PP. Small cell carcinoma of the breast: a clinicopathologic and immunohistochemical study of nine patients. Am J Surg Pathol. 2000;24(9):1231–8. https://doi.org/10.1097/00000478-200009000-00006.
Yang L, Lin H, Shen Y, et al. Clinical outcome and therapeutic impact on neuroendocrine neoplasms of the breast: a national cancer database study. Breast Cancer Res Treat. 2023;202:23–32. https://doi.org/10.1007/s10549-023-07052-5.
• Martinez EO, Jorns JM, Kong AL, Kijas J, Lee WYHuang CC, et al (2022) Primary breast neuroendocrine tumors: an analysis of the national cancer database. Ann Surg Oncol 29:6339–6346. This study showed that patients with primary breast neuroendocrine tumors have inferior overall survival compared to patients with invasive ductal carcinoma. This is likely secondary to presentation at higher clinical stages and more frequent hormone receptor negativity.
Chai Y, Liu M, Li Z, Chen Y, Qi F, Li Q, et al. Retrospective literature review of primary neuroendocrine neoplasms of the breast (BNEN) in 209 Chinese patients: Treatment and prognostic factor analysis. Breast. 2022;62:93–102.
Cloyd JM, Yang RL, Allison KH, Norton JA, Hernandez-Boussard T, Wapnir IL. Impact of histological subtype on long-term outcomes of neuroendocrine carcinoma of the breast. Breast Cancer Res Treat. 2014;148(3):637–44. https://doi.org/10.1007/s10549-014-3207-0.
Yang L, Roy M, Lin H, Shen Y, Albarracin CT, Huo L, et al. Validation of prognostic significance of the proposed uniform classification framework in neuroendoccrine neoplasms of the breast. Breast Cancer Res Treat. 2021;86(2):403–15. https://doi.org/10.1007/s10549-021-06099-6.
Bogina G, Munari E, Brunelli M, Bortesi L, Marconi M, Sommaggio M, et al. Neuroendocrine differentiation in breast carcinoma: clinicopathological features and outcome. Histopathology. 2016;68(3):422–32. https://doi.org/10.1111/his.12766.
Lavigne M, Menet E, Tille JC, Lae M, Fuhrmann L, Bonneau C, et al. Comprehensive clinical and molecular analyses of neuroendocrine carcinomas of the breast. Mod Pathol. 2018;31(1):68–82. https://doi.org/10.1038/modpathol.2017.107.
Emiroglu S, Abuaisha AM, Tukenmez M, Cabioglu N, Bayram A, Ozmen V, Muslumanoglu M. Pure Tubular Breast Carcinoma: Clinicopathological Characteristics and Clinical Outcomes. Eur J Breast Health. 2023;19(2):115–20. https://doi.org/10.4274/ejbh.galenos.2023.2022-12-9.PMID:37025580;PMCID:PMC10071886.
Tubular Carcinoma
Abdel-Fatah TM, Powe DG, Hodi Z, Lee AH, Reis-Filho JS, Ellis IO. High frequency of coexistence of columnar cell lesions, lobular neoplasia, and low grade ductal carcinoma in situ with invasive tubular carcinoma and invasive lobular carcinoma. Am J Surg Pathol. 2007;31(3):417–26. https://doi.org/10.1097/01.pas.0000213368.41251.b9.
Kunju LP, Ding Y, Kleer CG. Tubular carcinoma and grade 1 (well-differentiated) invasive ductal carcinoma: Comparison of flat epithelial atypia and other intra-epithelial lesions. Pathol Int. 2008;58(10):620–5.
Rakha EA, Lee AH, Evans AJ, Menon S, Assad NY, Hodi Z, Macmillan D, Blamey RW, Ellis IO. Tubular carcinoma of the breast: further evidence to support its excellent prognosis. J Clin Oncol: Official J Am Soc Clin Oncol. 2010;28(1):99–104. https://doi.org/10.1200/JCO.2009.23.5051.
Rosen PP. Tubular carcinoma. In: Rosen’s Breast Pathology. PA, USA: Lippincott-Raven; 1996. p. 325–6.
Kempson R. Stanford school of medicine surgical pathology criteria: tubular carcinoma of the breast; 2008. [Internet] http://surgpathcriteria.stanford.edu/breast/tubularcabr.
Jorns JM, Thomas DG, Healy PN, et al. Estrogen receptor expression is high but is of lower intensity in tubular carcinoma than in well-differentiated invasive ductal carcinoma. Arch Pathol Lab Med. 2014;138(11):1507–13. https://doi.org/10.5858/arpa.2013-0621-OA.
Cooper HS, Patchefsky AS, Krall RA. Tubular carcinoma of the breast. Cancer. 1978;42:2334–42.
Knape N, Park JH, Agala CB, et al. Can We Forgo Sentinel Lymph Node Biopsy in Women Aged ≥ 50 Years with Early-Stage Hormone-Receptor-Positive HER2-Negative Special Histologic Subtype Breast Cancer? Ann Surg Oncol. 2023;30:1042–50. https://doi.org/10.1245/s10434-022-12626-6.
Gradishar WJ, Moran MS, Abraham J, Aft R, Agnese D, Allison KH, et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2022;20:691–722.
Zhao Y, Chai N, Li S, Yan L, Zhou C, He J, Zhang H. Evaluation of the efficacy of chemotherapy for tubular carcinoma of the breast: A Surveillance, Epidemiology, and End Results cohort study. Cancer Medicine. 2023 Mar 6. https://doi.org/10.1002/cam4.5763.
Turashvili G, Brogi E, Morrow M, Hudis C, Dickler M, Norton L, Wen HY. The 21-gene recurrence score in special histologic subtypes of breast cancer with favorable prognosis. Breast Cancer Res Treat. 2017;165(1):65–76. https://doi.org/10.1007/s10549-017-4326-1.
• Upasana Joneja, Juan Palazzo; The Spectrum of Mucinous Lesions of the Breast. Arch Pathol Lab Med. 1 January 2023; 147 (1): 19–29. https://doi.org/10.5858/arpa.2022-0054-RA. This study reviewed the range of mucinous lesions and reinforced the need for sufficient tissue for pathologic diagnosis as there are unique treatments and prognoses for each. This paper includes a detailed summary chart of mucinous lesions of the breast.
Mucinous
Di Saverio S, Gutierrez J, Avisar E. A retrospective review with long-term follow-up of 11,400 cases of pure mucinous breast carcinoma. Breast Cancer Res Treat. 2008;111(3):541–7.
Collins LC, Cole KS, Marotti JD, Hu R, Schnitt SJ, Tamimi RM. Androgen receptor expression in breast cancer in relation to molecular phenotype: results from the Nurses’ Health Study. Modern Pathol: an Official J United States Canadian Acad Pathol, Inc. 2011;24(7):924–31. https://doi.org/10.1038/modpathol.2011.54.
Tan PH, Tse GM, Bay BH. Mucinous breast lesions: diagnostic challenges. J Clin Pathol. 2008;61(1):11–9. https://doi.org/10.1136/jcp.2006.046227.
Rasmussen BB, Rose C, Christensen IB. Prognostic factors in primary mucinous carcinoma. Am J Clin Pathol. 1987;87(2):155–60.
Komenaka IK, El-Tamer MB, Troxel A, et al Mucinous carcinoma of the breast. Am J Surg. 2004; 187 (4): 528– 532. National Comprehensive Cancer Network. NCCN guidelines. Breast cancer (version 2.2022). https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1419. Accessed October 2023.
Komaki K, Sakamoto G, Sugano H, Morimoto T, Monden Y, et al. Mucinous carcinoma of the breast in Japan. A Prognostic Anal Based Morphol Features Cancer. 1988;61:989–96.
Marrazzo E, Frusone F, Milana F, et al. Mucinous breast cancer: a narrative review of literature and a retrospective tertiary single-centre analysis. Breast. 2020;49:87–92.
Skotnicki P, Sas-Korczynska B, Strzepek L, Jakubowicz J, Blecharz P, Reinfuss M, Walasek T. Pure and mixed mucinous carcinoma of the breast: a comparison of clinical outcomes and treatment results. Breast J. 2016;22(5):529–34.
Fayanju OM, Ritter J, Gillanders WE, Eberlein TJ, Dietz JR, Aft R, et al. Therapeutic management of intracystic papillary carcinoma of the breast: the roles of radiation and endocrine therapy. Am J Surg. 2007;194(4):497–500.
Papillary
Ibarra JA. Papillary lesions of the breast. The breast journal. 2006 May;12(3):237–51. Pal SK, Lau SK, Kruper L, Nwoye U, Garberoglio C, Gupta RK, Paz B, Vora L, Guzman E, Artinyan A, Somlo G. Papillary carcinoma of the breast: an overview. Breast cancer research and treatment. 2010 122:637–45. https://doi.org/10.1007/s10549-010-0961-5.
Jorns JM. Papillary Lesions of the Breast: A Practical Approach to Diagnosis. Arch Pathol Lab Med. 2016;140(10):1052–9. https://doi.org/10.5858/arpa.2016-0219-RA.
Tay TK, Tan PH. Papillary neoplasms of the breast—reviewing the spectrum. Mod Pathol. 2021;34(6):1044–61.
Kulka J, Madaras L, Floris G, Lax SF. Papillary lesions of the breast. Virchows Archiv : an Int J Pathol. 2022;480(1):65–84. https://doi.org/10.1007/s00428-021-03182-7.
Anderson W, Devesa SS. In situ male breast carcinoma in the surveillance, epidemiology, and end results database of the National Cancer Institute. Cancer. 2005;104(8):1733–41.
Burga A, Fadare O, Lininger R, Tavassoli F. Invasive carcinomas of the male breast: a morphologic study of the distribution of histologic subtypes and metastatic patterns in 778 cases. Virchows Arch. 2006;449(5):507–12.
Rakha EA, Varga Z, Elsheik S, Ellis IO. High-grade encapsulated papillary carcinoma of the breast: an under-recognized entity. Histopathology. 2015;66(5):740–6.
Zheng YZ, Hu X, Shao ZM. Clinicopathological characteristics and survival outcomes in invasive papillary carcinoma of the breast: a SEER population-based study. Sci Rep. 2016;6(1):24037.
Huang K, Appiah L, Mishra A, Bagaria SP, Gabriel ME, Misra S. Clinicopathologic characteristics and prognosis of invasive papillary carcinoma of the breast. J Surg Res. 2021;1(261):105–12.
Martinez EO, Jorns JM, Kong AL, Cortina CS. ASO Author Reflections: Rare Breast Cancer Subtypes and the Role for Precision Oncology. Ann Surg Oncol. 2022;29(10):6347–8. https://doi.org/10.1245/s10434-022-12137-4.
Author information
Authors and Affiliations
Contributions
A.C and C.C. wrote the main manuscript text. J.J and R.C prepared figure 1 and associated caption. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Cobb, A.N., Czaja, R., Jorns, J. et al. Breast Cancer Subtypes: Clinicopathologic Features and Treatment Considerations. Curr Breast Cancer Rep 16, 150–160 (2024). https://doi.org/10.1007/s12609-024-00541-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12609-024-00541-6