
Abstract
Simulated human gastrointestinal (GI) tract systems are important for their applications in the fields of probiotics, nutrition and health. To date, various in vitro gut systems have been available to study GI tract dynamics and its association with health. In contrast to in vivo investigations, which are constrained by ethical considerations, in vitro models have several benefits despite the challenges involved in mimicking the GI environment. These in vitro models can be used for a range of research, from simple to dynamic, with one compartment to several compartments. In this review, we present a panoramic development of in vitro GI models for the first time through an evolutionary timeline. We tried to provide insight on designing an in vitro gut model, especially for novices. Latest developments and scope for improvement based on the limitations of the existing models were highlighted. In conclusion, designing an in vitro GI model suitable for a particular application is a multifaceted task. The bio-mimicking of the GI tract specific to geometrical, anatomical and mechanical features remains a challenge for the development of effective in vitro GI models. Advances in computer technology, artificial intelligence and nanotechnology are going to be revolutionary for further development. Besides this, in silico high-throughput technologies and miniaturisation are key players in the success of making in vitro modelling cost-effective and reducing the burden of in vivo studies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Gastrointestinal (GI) models are the investigational tools designed to understand the role of the human digestive system in the digestion of test-intervention and its association with diseases. These models mimic the GI environment through in vitro bio-chemical recreation of the human digestive system, sometimes intestinal epithelium and gut microbiota [1]. Many physicochemical and microbial aspects such as pH, bile salts, enzymes, faecal microbiota, temperature, peristaltic movement, transit times and anaerobic environment were easily reproduced in the models [2]. As like in vivo GI tract, it is not possible to investigate the interaction of test-intervention between the gut and the nervous or endocrinal system. However, these in vitro models have diverse applications in the fields of food digestion [3], gut microbiota modulation [4], survival of probiotics during GI transit [5,6,7], screening of prebiotics [8] and in vivo and in vitro correlation studies for pharmaceuticals [9]. In vitro GI tract model studies are reliable, reproducible, relatively inexpensive, convenient and free from ethical constraints [10, 11] as compared to in vivo studies. Minekus and co-workers [12] have suggested that in vitro models are useful to study substances and/or doses under controlled experimental conditions and obtain reproducible results. Clark et al. [13] suggested the use of defined microbial communities for experiments involving gut microbiota to enhance the controllability and reproducibility of the results. Moreover, the design of an in vitro model is quite challenging when considering the complexity and multifactorial processes in the human GI system.
This review presents a panoramic and evolutionary overview of in vitro gut model systems, insights on designing a new model, recent developments and scope for further advancements based on the limitations of the existing models.
Evolutionary Development
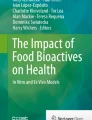
In the last six decades, in vitro GI models have been continuously gaining shape according to the technological advancements in the field. Figure 1 depicts an evolutionary overview of in vitro models encompassing different phases such as geometric evolution, high-throughput technology, miniaturisation and in silico evolution. Each model has its own salient feature and is definitely a value addition in the field. However, for practical reasons, we mainly emphasised the milestones that were transformative and are still applicable to contemporary research.

History and evolutionary milestones of in vitro gastrointestinal models
Initial demonstrations of simulated in vitro GI systems were limited to biochemical representation using simulated juice under static conditions to study drug absorption or binding or bioavailability [14,15,16]. In 1975, Braybrooks and co-workers [17] used Sartorius absorption simulator apparatus to mimic gastrointestinal tract conditions to investigate the effect of mucin on the bioavailability of tetracycline. The first milestone in the development of in vitro GI models appeared in 1981, when Miller and Wolin [18] introduced an in vitro semi-continuous fermentation system to maintain the human colonic microbial community. This single compartment system enables to study the diversity of the colonic microbial population and analyse the dynamics of the fermentation products in response to dietary components and the biotransformation of synthetic drugs. In 1989, Macfarlane and associates [19] developed a multichamber colon model to mimic the human colonic continuous fermentation system to study the degradation of pancreatic enzymes by colonic bacteria.
One of the most remarkable landmarks in the field of in vitro GI models is the Simulator of Human Intestinal Microbial Ecosystem (SHIME), which was developed by Molly and co-workers in 1993 [20]. The model was the first attempt to maintain both small and large intestinal microbial communities by continuous fermentation and formed the basis for the subsequent variations. SHIME consisted of 5 reactor vessels representing the duodenum and jejunum, ileum and caecum, ascending colon, transverse colon and descending colon. Later in 2012, Van den Abbeele and co-workers [21] developed M-SHIME, which consisted of mucosal compartments created by the addition of plastic microcosms coated with mucin type II agar. Possemiers et al. [22] co-cultured intestinal microbiota with human-derived cell lines in M-SHIME to understand the immunomodulation properties. Such in vitro findings will be useful in designing targeted clinical studies to confirm the mode of action and the significance of the observed effects. In 2014, Marzorati and co-workers [23] introduced the Host-Microbe Interaction (HMI) module with SHIME to overcome the limitation on accessibility of colonic microbiota posed by in vivo studies. During that time, the in vitro models were mainly focused on the colonic sections and microbiome. However, the work on dynamic aspects of the GI tract such as peristaltic movement, transit of chyme, secretion of digestive juices and absorption of nutrients was limited. In 1995, soon after the SHIME model was introduced, Minekus et al. [12] developed a unique, dynamic stomach-small intestinal set-up (TNO Gastro-Intestinal Model (TIM)-1). The use of flexible walls, computer-controlled transit and the flow rate of chyme brought geometrical evolution in the field. In addition to that, syringe pumps were employed to facilitate acid and alkali secretion. For the first time, absorption of nutrients was simulated via dialysis using a hollow fibre device.
Later in 1999, a TIM-1 complementary computer-controlled large intestinal simulation system (TIM-2) was developed by Minekus et al. [24]. The system was named Artificial Colon (ARCOL) model and can be used sequentially with TIM-1. It was a single-compartment semi-continuous fermentation system to maintain resident colonic microbiota under simulated colonic conditions. Apart from regulation of colonic pH, temperature and anaerobic conditions, the system was programmed to simulate ileal content feeding to the colonic chamber, retention time of chyme, absorption of water and fermentation products [25].
The geometric and mechanical evolution of in vitro gut models continued with the development of new innovative approaches to recreate digestive organ geometry and mechanical forces involved in digestion. In 2007, a patented, computer-controlled Dynamic Gastric Model (DGM) was invented by Wickham and Faulks at the Quadram Institute of Bioscience (formerly the Institute of Food Research). The model works towards mimicking human gastric processing through accurate replication of gastric mixing, shear rates and peristalsis (WO/2007/010238) [26]. The system automation controls gastric retention time, addition of gastric secretions (acid and enzyme), gastric emptying and processing of gastric contents.
Later in 2010, Kong and Singh [27] developed a latex chambered, cylindrical-shaped human gastric simulator (HGS) model connected to conveyor belts and a series of Teflon rollers. This model mimics antral contractions of the stomach and gastric emptying in a continuous and controlled manner. In 2016, Guerra and associates [28] introduced innovation in the stomach compartment to simulate the biphasic nature of gastric emptying through the Engineered Stomach and small INtestine (ESIN) model. This model allows differential gastric emptying of liquid (exponential, Elashoff model without lag period) and solid (linear emptying with a 30-min lag phase) foods [28]. In the same year, Chen et al. [29] introduced a J-shaped semi-soft silicone stomach with rope to simulate antral contractions. This ‘rope-driven’ in vitro human stomach model (RD-IV-HSM) has a unique wrinkled internal lumen (discussed in the section “Recent Advances”).
Barroso et al. [30] developed a computer-controlled multicompartmental SIMulator of the GastroIntestinal tract (SIMGI) system adapted from SHIME. This model allows joint or separated simulation of the gastric and colonic fermentative processes. Wright et al. [31] introduced the contraction-enabled human duodenum model (HDM). This sigmoidal-shaped duodenum has contraction rings attached with rubber finger cots for the peristaltic movement of digested food. In recent years, Wang et al. [32] adapted RD-IV-HSM to design a dynamic in vitro human stomach (DIVHS) system with stomach dimensions, morphology and inner wrinkles similar to those of a real human stomach. The model was fabricated with 3-D printing technology and had provision for consistent gastric emptying for both solid and liquid fractions.
Simultaneously, during the development of geometric and mechanical evolution of in vitro gut models, Berner et al. [33] introduced the first high-throughput in vitro Polyfermentor Intestinal Model (PolyFermS) in 2013. This model was designed to compare the effects of different treatments (environmental, microbes, dietary compounds and drugs) on the same complex gut microbiota in multiple reactors. Fehlbaum et al. [34] later in 2015 used PolyFermS for continuous fermentation by employing faecal microbiota immobilised in gel beads. In 2018, Cieplak et al. [35] introduced miniaturisation in the form of an in vitro The Smallest Intestine (TSI) model. This low-volume, high-throughput set-up was the first of its kind to study the small intestinal microbiota. In another high-throughput miniaturisation, Wiese et al. [36] developed Copenhagen MiniGut (CoMiniGut) for the small-volume working and investigation of rare and expensive bio-actives. This innovation was termed next-generation in vitro simulations with high statistical inference in limited resources [36].
The contemporary development of in vitro GI models also comprises in silico evolution. The investigations into pharmacokinetics, drug absorption and bioavailability were mainly involved in early in silico studies [37, 38]. In 2002, Kamerman and Wilkinson [39] developed the first model intestinal microflora in computer simulation (MIMICS) to simulate the intestinal microbiota using parallel high-performance computers. Jong et al. [40] designed an in silico GI tract tool for the interpretation of intestinal infection studies in 2007. Beside this, other population-based absorption, distribution, metabolism and excretion simulator platforms were Simcyp®, GI-Sim absorption models, GastroPlus™ and PK-SIM [41, 42]. In 2017, Barth and co-workers [43] demonstrated electrical simulation of gut motility guided by an in silico model. This integrated neuromechanical model was useful for studying the gut motility in certain GI disorders. Similar to this, AgentCell, BSim and BNSim models have been increasingly popular for in silico simulation of microbial populations during the past few years. In 2018, Lin and co-workers [44] introduced GutLogo, an agent-based modelling framework to investigate spatial and temporal dynamics in the gut microbiome. Recently, Clark et al. [13] designed a synthetic human gut microbiome assembly to understand community assembly and metabolic functions. This data-driven model was reported to perform a quantitative assessment of microbial interactions impacting growth and butyrate production.
In conclusion, in vitro GI models have a long history of development and have been divided into distinct branches that each focus on automating a different part of an in vitro model. Beginning with the simulation of GI fluids and static compartmental models, it went through several stages before being introduced to GI dynamics, geometric evolution, high-throughput technology, miniaturisation and, most recently, computer-based simulations. Undoubtedly, the growth of computers and nanotechnology will enable us to incorporate the subtleties of the GI system that were not taken into account in earlier models.
Designing a Model
Simulation of the human GI environment in vitro is a multifaceted, multistep process involving recreation and recapitulation of various anatomical, physicochemical and microbial aspects of the human GI system. We have outlined the significance of each parameter pertinent to the creation of a simulated in vitro human GI model in the sections below (Fig. 2). The selection of the appropriate parameter and the extent to which it is used in the development of a new model will typically rely on the application and study parameters involved. Moreover, it is almost never practical to include all the parameters for all underlying research issues. In fact, it should be noted that not all physiological settings that exist in vivo can be replicated in a particular in vitro model. For convenience, we have listed significant in vitro GI models in Table 1 together with information on various compartmental contents.

Designing summary of an in vitro gastrointestinal model
Number of Compartments
Up to six compartments in a simulated in vitro GI model that replicates several organs of the human GI system are possible. Under static settings, models incorporating a single compartment can simulate the complete GI system or just one specific GI compartment, typically the colon [18, 24, 25, 45, 46]. Popular GI compartmental models include those that depict the mouth, oesophagus, stomach, small intestine and large intestine. These models often represent three to five separate GI compartments [25, 47,48,49].
The literature is replete with simple in vitro models that replicated the whole small intestine. Such research is appropriate for a preliminary assessment of probiotic survival throughout GI transit; the digestion of protein, fat and carbohydrate from meals or modified carriers; the bio-accessibility of nutrients from diverse biomatrices; etc. [49,50,51], while models that elaborate on the duodenum, jejunum and ileum of the small intestine have also been used when necessary for a study or application [12, 20, 25, 35].
pH and Electrolytes
The digestive fluid pH primarily regulates the activity of the enzymes involved in digestion, which is crucial to the entire digestion process [52]. In order for enzymes to work properly during simulated GI processing, it is advised to adhere to the ideal pH ranges. Besides this, electrolytes are principally responsible for the digestive fluid ability to buffer [53].
The pH of normal saliva is just barely acidic (6.0 to 7.0). It can range from 5.3 at low flow to 7.8 at peak flow, and the flow rates under stimulated (0.1 mL/min) and unstimulated (0.2 mL/min) circumstances are different [53]. Most in vitro models used an oral compartment with a pH of 6.5, which is mildly acidic [47, 50].
The pH of the stomach compartment is influenced by the pace at which gastric acid is secreted, which in turn depends on fed or fasting state, type and quantity of food. For instance, the median pH during a fast was shown to range between 1.55 and 1.80. When food is consumed or is present, the pH gradually rises, and the gastric compartment is reacidified as a result of increased gastric acid secretion rate. For existing gut models, static pH mode (pH range = 1.2–3.0) is the most widely utilised strategy [54, 55]. In multicompartmental dynamic computer-controlled model, Minekus et al. [12] gradually acidified the stomach compartment over the course of 2 h (0 h, 4.8 to 2 h, 1.7 pH) to imitate the digestion of milk in vivo; other researchers adopted a similar modelling approach [7, 25, 47, 56].
The arrival of nutrients in the duodenum triggers pancreatic secretion, which mainly contains digestive enzymes and high bicarbonate to maintain pH between 7.4 and 7.8 [10, 57]. The overall pH range in the small intestine is from 5.5 to 7.0, which steadily increases to 6.5–7.5 in the distal ileum [58]. Studies using dynamic models showed these pH changes in different parts of the small intestine [20, 25, 35, 47]. It has been observed that static models maintain a pH of 6.5 to 7.0 in the small intestine compartment.
The composition and metabolic activity of the gut microbiota are significantly influenced by the colonic pH, which is primarily controlled by short-chain fatty acids produced by fermenting bacteria [8]. As a result, there is a coordination between the colonic pH and the gut microbiota [32]. In general, food/chyme undergoes a sharp pH dip (between 5.5 and 7.5) when it moves from the terminal ileum to the caecum, and the pH subsequently rises to between 6.1 and 7.5 in the descending colon and rectum [58,59,60].
The most commonly used electrolytes for in vitro simulations are sodium, potassium, calcium, magnesium, phosphate and bicarbonate [11]. Each electrolyte has a distinct function in nutrient digestion and absorption. The most frequent cations for preserving osmotic equilibrium are sodium and potassium, whereas chloride and bicarbonate are anions that are osmotically activated [61]. In vivo, the primary role of most of the electrolytes in the mouth is in protection. For example, calcium and phosphate help in the remineralisation of tooth enamel [62]. Bicarbonate ions produced by specialised cells neutralise HCl to protect the stomach’s cell lining [63]. Electrolyte and water absorption takes place in the small intestine via simple or facilitated diffusion and active transport [64]. Sodium, chloride, bicarbonate, calcium, iron, potassium, magnesium, phosphate and other ions are all absorbed through the mucosa. Although the ions employed in the majority of the studies are nearly identical, their concentrations may vary depending on the technique (Tables 2, 3 and 4).
Composition of Digestive Juices
Saliva is a complex exocrine secretion that is highly diluted (more than 99% water) and contains a range of electrolytes (sodium, potassium, calcium, magnesium, bicarbonate and phosphates), proteins, immunoglobulins, enzymes, mucins and nitrogenous products (urea and ammonia) [10]. Accordingly, mucin and α-amylase have been the common components of the oral fluid [47, 50, 51]. However, other enzymes present in saliva (lipase, ribonuclease and protease) have rarely been incorporated into gut model systems [62].
Gastric fluid consists of water, gastric acid, enzymes, mucus and swallowed food material [52]. In a fasted state, a mean secretion rate of approximately 1 mL/min and 0.03–0.07 mEq H+/min was reported for gastric secretion (acid secretion) [52]. Pepsin, mucus and electrolytes make up the majority of simulated gastric juice [51, 56]; however, gastric lipase and lecithin/egg phosphatidylcholine (as a fat emulsifier) have occasionally been added to more closely examine fat digestion [65, 66]. Gastric mucin is one of the crucial components of gastric juice to protect the stomach epithelium against pepsin auto-digestion and stomach acid [67].
Intestinal fluid is complex and dynamic in nature, consisting of bile salts, phospholipids, electrolytes (phosphates, potassium, sodium, chlorides, calcium, magnesium, etc.), short-chain fatty acids, enzymes (amylase, lipase, trypsin) and gases [68]. The main components of the small intestine juice are pancreatin (a mixture of pancreatic lipase, colipase, trypsin, α-chymotrypsins and α-amylase) and bile salts/bile solution (phosphatidylcholine, cholesterol, sodium taurocholate and sodium glycodeoxycholate) [55, 56, 66, 69]. Bile salts aid in the breakdown of fats, affect the composition of the ingested microbiota and function as co-factors for numerous enzymes [12]. If conditions are not ideal, the majority of the digestive juices’ enzymes are inactive. The ideal temperature for digestive enzymes is 37 °C, while the optimum pH for each of the enzymes is provided in Table 5. An important component of the colonic compartment—microbiota—is explained separately in the section “Gut Microbiota.”
Retention/Transit Time
Retention times in different GI compartments vary according to digestion processes and food type (solid, semisolid, liquid). For example, the average time of solid food mastication in the oral cavity is usually less than 2 min [51]. However, while employing the same conditions in vitro, it should be ensured that the food sample or sample under question spends sufficient time in the presence of digestive juices or undergoes relevant mechanical treatment mimicking processes such as chewing, mastication or peristalsis. Consequently, a retention time of 1–5 min has been employed by most researchers for the oral phase of digestion [47, 50, 51]. Such modifications help to achieve the accuracy and reproducibility of results under lab conditions [11]. Additionally, it is interesting to note that retention time in oral phase digestion varies under certain circumstances. For instance, studies on oral dosage forms like tablets and capsules demand very short retention times of a few seconds, as there is no role for chewing or mastication. In another example, oral phase digestion in the elderly differs considerably due to age-related factors. Some of these include the loss of natural teeth, a decrease in bite force and mandibular reflex occurrences and a decrease in saliva secretions [70]. While studying the elderly population, we recommend optimising oral food retention times in light of these changes.
In vitro GI models have used a range of stomach emptying durations, from as little as 30 min [12] to as long as 4 h [49]. It depends mostly on the liquid and solid contents, as well as on the caloric and non-caloric contents [52]. According to Braghetto et al. [71], healthy volunteers had an average gastric emptying half-time of 34.9 ± 24.6 min for 200 mL of water; however, solid dose forms could stay in the stomach for several hours. For the majority of applications, most models use a transit duration of 30 to 120 min [54, 55, 65, 69]. Furthermore, in order to simulate an in vivo environment, dynamic models can include fractional emptying of the stomach and colonic compartments [12, 25, 47].
The typical time for a meal to pass through the small intestine (from the pylorus to the ileocolonic junction) is 1 to 5 h, and the colon takes 12 to 24 h [1]. In an average of 10 mL/min, with rare spikes to 20 mL/min, the digesta passes through the small intestine. This movement is basically influenced by the viscosity of the intestinal contents, temperature and the peristalsis and sedimentation movement of the intestinal walls [31]. According to scientific data, at 6 h, non-digestible particle colon filling ranges from 11 to 70% and digestible solid colon filling ranges from 43 to 95% [60, 72]. The most widely used in vitro GI models, including TSI and TIM, put the colonic and small intestine transit durations at 2–8 h and 20–70 h, respectively [25, 35, 56, 66]. For models containing colonic compartments, significant adjustment of retention time is necessary due to the high correlation between colonic bacterial fermentation and retention times [19].
Volume of Digestive Juices
In simulated in vitro GI models, food and digestive juices have often been used in a ratio of 1:1 [51, 55]. Despite the possibility that this fact may not hold true in vivo, this ratio guarantees wetting and lubrication of the meal, turning the sample into a smooth paste and making it easier for sampling during future research [11].
The amount of gastric juice secreted is influenced by both the type of food consumed and the stomach’s fed or fasting state. For solid food, approximately two volumes of gastric juice is released [11]. Since GI secretions (including stomach acid and duodenal secretions) are produced in reaction to meals, the rate at which they are produced is more significant than the volume. With limited function in secretion, colon mostly participates in the absorption of water, electrolytes, vitamins and short-chain fatty acids. The physiological ratios of saliva, gastric juice, duodenal juice and bile are 1:1.5:3:1 [50]. Klindt-Toldam et al. [65] utilised a 1:2:50 ratio for food/saliva/gastric medium. Ceuppens et al. [47] used a 1.5:1:2:4.5 ratio for food/saliva/gastric/intestinal simulation media. Moreover, the amount of digestive fluids changes mostly according to the needs of experiments and analyses.
Gut Microbiota
The gut microbiota comprises a large pool of microorganisms inhabiting the human GI tract [73]. Approximately, 101–103 bacteria (per gram) reside in the stomach and duodenum, 104–107 bacteria/g in the jejunum and ileum, and 1011–1012 bacteria/g in the colon [8]. The Firmicutes and Bacteroidetes phyla dominate the gut microbiota of adult humans, with lower amounts of Actinobacteria, Proteobacteria and Verrucomicrobia [74]. This composition varies depending on the individuals’ age, gender, nutrition, medicine and disease state [75].
In colon, the resident bacteria play an important role in the digestion of complex carbohydrates into short-chain fatty acids (SCFAs) like acetate, propionate and butyrate [34, 76]. Besides this, it prevents enteropathogens from adhering to gut epithelium and supports the body’s immune system [34]. Moreover, the gut microbiota is linked to a variety of metabolic, neoplastic, infectious and inflammatory disorders in the colon and at extracolonic sites [77]. Thus, colonic fermentation, characterised by the inoculation of faecal or gut microbiota, is a crucial aspect of in vitro gut models [8].
A fresh faecal suspension is widely used to inoculate the colonic model to recreate the microbiological niches [35, 47, 78]. However, it is challenging to maintain microbial profiles, cell density and reproducible abundance of gut lumen and food-mucus-associated bacterial populations [34]. In order to address these issues, Clark et al. [13] suggested the use of defined microbial communities or synthetically constructed microbiomes to improve controllability, repeatability and environmental safety. Besides this, the recreation of gut microbiota in association with the mucosal environment helps to study in vivo like microbial simulation. As the presence of mucus has been shown to change the relative abundance of unique microbiota capable of utilising or degrading mucus [79].
Static vs Dynamic Models
Static in vitro models use constant variables like the ratio of the feed to enzymes, electrolytes and pH for each phase of digestion [51]. As an alternative, certain static models use constant retention time and varying digestion parameters in a single vessel [2]. Such models are unable to adequately simulate the dynamics of the GI system and cannot be used for more than 24-h experiments [68, 78]. However, because of their simplicity and high-throughput outcome, these models are better suited for screening or preliminary research, developing hypotheses and specific applications like adhesion [3, 10, 78].
Most dynamic models are either continuous or semi-continuous in nature. These models allow variations in pH and bile, fractional stomach emptying and intestinal compartment dialysis to simulate nutrition absorption in accordance with in vivo conditions [2, 12, 47]. A well-designed dynamic model enables thorough research of the gut microbiota and factors responsible for modifying the same under almost in vivo settings, making it suitable for challenging investigations [79]. Besides simulating the geometry, flow and motility of GI organs, dynamic models may replicate the mechanical and physical factors that result in non-homogenous digested materials with diverse biochemical niches [3]. Moreover, dynamic models have drawbacks since they demand trained workers, are expensive and time-consuming and are therefore unsuitable for screening tests [2].
Limitations
The GI tract is made up of several parts, each of which is difficult to replicate. Consequently, existing models have certain limitations that need to be considered while designing a new model. Each GI compartment leads to the digestion of food in a different way. Certain major processes in digestion, such as mastication, salivation, peristalsis, dynamics of digestive juice secretion and absorption of nutrients from food, are very difficult to simulate in vitro. Anatomical details such as villi, wrinkles, dimensions and geometry of organs and their mechanical action on food, along with peristaltic movements and biochemical conditions, were not yet considered properly. Furthermore, validation of in vitro trials with in vivo data is sparsely available for existing models.
The composition of digestive secretions frequently failed to replicate in vivo conditions in gut models. For example, saliva has over 30 distinct enzymes [10] but most of the in vitro models use only α-amylase. Besides this, it is difficult to check digestive enzyme (lipases, amylases and peptidases) activities when they are in a mixture. The sodium taurocholate in in vitro models only makes up 20% of the bile salts found in vivo [68]. Moreover, the compounds with varying physicochemical properties are difficult to combine and use. For example, fasted- and fed-state simulated intestinal fluids consist of lecithin but not of their hydrolysis product, lysolecithin, which has a different solubility during digestion. Similarly, pancreatin enzyme levels vary across different assay systems and the United States Pharmacopoeia recommendation for its dissolution does not depict an in vivo scenario [68].
Fecal microbiota is another important factor to consider while dealing with gut modulation studies. In the in vitro setup, the diet, lifestyle and gender-related variation in the individual gut microbiota were not considered, thus leading to the reproducibility issues [2, 80]. Sometimes, the amount and diversity of bacterial populations employed in gut model samples are different from those of faecal inoculum [81].
Batch fermentation models are restricted due to accumulation of bacterial metabolites during stationary/declining growth phase [81]. Other limitations for most in vitro digestion models are related to recreating a chewed meal, inhomogeneous mixing in the fundus, shear and mixing conditions in the antrum and the temporal delivery of gastric digesta to the duodenum. SHIME suffer from data limitation due to restricting the studies to one or two compartments [8]. Apart from this, the major limitations of the existing in vitro gut models are the lack of feedback mechanisms and immune and nervous system involvement. Lastly, results obtained using in vitro gut models describe gut microbiota responses that are independent of the host microbial community [79, 80].
Recent Advances
In vitro GI models have recently made progress in recreating anatomical, physical, mechanical and biochemical features. Chen et al. [29] developed a ‘rope-driven’ in vitro human stomach model (RD-IV-HSM) consisting of a wrinkled stomach compartment made of silicon material, a rope-driven rig (to provide peristaltic motion), the gastric fluid secretion and digesta emptying mechanism in a temperature-controlled box. Besides this, in vitro mechanical gastric system (IMGS) [82], artificial gastric digestive system (AGDS) [83] and gastric simulation model (GSM) [84] were created to simulate GI movements.
Nowadays, organoid engineering enhanced the domains of individualised medicine, food-food/drug interactions, pharmacokinetics and pharmacodynamics, host-microbe connections and other disciplines [85]. An organoid is a small, three-dimensional organ created in vitro from organ-specific stem cells (stomach and or intestine). On the other hand, mesenchymal cells and organ-specific epithelial cells are jointly developed by pluripotent stem cells [86].
Recently created gut-on-a-chip systems use microfluidics and typically have compartments that are perfused with culture media and colonised cells. Through appropriate cell configurations, the physiological simulation of the targeted tissue or organ is accomplished [87]. Co-culturing of cells to study interactions between the two tissues or organ systems is another feature of these models [88]. Beside this, it is also possible to build three-dimensional organ-specific structures such as crypts or villi, to mimic real miniaturised architecture using gut-on-a-chip models [89, 90]. Kim et al. [91] built a human gut-on-a-chip with mechanical characteristics including peristalsis and microbial growth for possible use in drug discovery and intestinal illness models.
The in silico models employed computer algorithms to recreate exact organ geometries and motility patterns, GI fluid flow, transport of nutrients, gut microbiota metabolites and their effect on gut motility [92]. The primary objective of in silico models is to reproduce the outcomes obtained in reality. Such models are developed using huge data sets on metabolites, cells, gut microbiota and their interplay derived from various in vivo and in vitro trials. There are two popular technologies used in building in silico models: (1) agent-based modelling (ABM) and (2) genome scale nodels (GSMs). ABM carries out modelling of distinct agents (e.g. cells) which encodes behavioural responses to external stimuli and their mutual interactions [93]. For example, an ABM-GutLogo has been developed by Lin et al. [44] to study spatial and temporal dynamics of four microbial genera in the ileum perturbed by factors such as diet, flow rate of the GI contents and the presence of probiotics. GSMs, on the other hand, are more complex metabolic networks that are used to understand host, diet and microbe interactions [93, 94]. Henson [95] studied changes in gut microbiota metabolism in association with gouty arthritis using a genome-scale metabolic model. A patient-specific bacterial community metabolic model revealed dominant genera with high and low gout conditions, as well as their specific metabolic products and metabolic product exchange between genera. Interestingly, the predictive ability of this model could suggest a probable biochemical marker for the disease [95].
Barth et al. [43] developed an in silico gut motility model to enable the optimization of neuromodulation therapy involving higher-frequency rectangular current pulses to increase intrinsic peristalsis. The model consisted of a network of enteric neurons, smooth muscle fibers and interstitial cells of Cajal and a simulated pellet. Sinusoidal current at 0.5 Hz was found to be more effective at increasing peristalsis and pacemaker frequency in Cajal interstitial cells. These findings were verified by in vivo experiments performed in awake rat models.
Scope of Improvement/Proposed Modifications
Even though there have been many improvements made in the development of in vitro GI models, there is still ample scope for further improvements. Innovations are required to introduce more detailed aspects of anatomy and geometry of the organs and their structures into gut models. Nutrient absorption should be based on realistic intestinal approaches such as specific transporters/receptors [35]. Endocrine and nervous system influences must be incorporated into in vitro GI models for comprehensive studies. Moreover, reliable analytical techniques and technologies with increased specificity and selectivity are essential to investigate metabolites and members of microbial communities. To get beyond the limits of clinical trials and other ethical concerns, a hassle-free in vitro recreation of microbial ecology with regard to age and health is necessary. Finally, an unbalanced or disordered environment needs to be created in order to comprehend GI illnesses and efficacy-related investigations.
Cost-effectiveness
It is worth considering the run and analysis costs of the in vitro GI systems owing to their broad applications and tremendous scope. The cost is mostly dependent on the quality of the outcome, the number of parameters to investigate and the in vivo data validity status [7]. SHIME and TIM are currently the most well-known commercial service providers in the field of in vitro gastrointestinal tract studies. The approximate base run and analysis cost starts at more than 10,000 USD and depends on the required analysis. Until now, the cost-effectiveness of the in vitro models has not received much attention. This could be due to limited commercial scope. The industries engaged in probiotics, prebiotics, nutritional supplements, drugs and formulation research were mostly availing the services from commercial GI model companies. In academia, gut models are simulated and used for research based on available data. Furthermore, we believe that the development of high-throughput technologies and miniaturisation will significantly reduce service or product costs in the long run.
Conclusion
The gastrointestinal tract plays a pivotal role in human health through digestion of food, absorption of nutrients, biotransformation, immune modulation, establishment of gut-brain axis, etc. Consequently, GI tract–related studies have a long history and the field has evolved over decades in profound ways. Due to the inherent limitations of in vivo GI studies, the need for in vitro demonstrations is highly indispensable. The design of an in vitro GI model is multifaceted and completely depends on its purpose of study or application. Models range from simple mono-compartmental static to complex multicompartmental dynamic. Considering the limitations of the existing models that fail to reproduce the anatomical and mechanical aspects of the GI tract, recent advances have taken place in the same direction. Development of gut-on-the-chip, 3D organoids, synthetic gut microbiomes and in silico simulations of GI features are the highlights of contemporary in vitro models. Undoubtedly, the field is advancing at a pace with the advent of new technologies such as artificial intelligence, artificial neural networks, automation and miniaturisation. Although in vivo studies will always remain irreplaceable, in vitro GI models are propitious and we envisage developing in vitro approaches will reduce the need for pre-clinical or clinical trials, if not completely eliminate them.
Data Availability
The data collected to write this review will be made available by the authors without undue reservation to any qualified researchers.
References
Sensoy I (2021) A review on the food digestion in the digestive tract and the used in vitro models. Curr Res Food Sci 4:308–319. https://doi.org/10.1016/j.crfs.2021.04.004
Fournier E, Roussel C, Dominicis A, Ley D, Peyron M, Collado V et al (2022) In vitro models of gut digestion across childhood: current developments, challenges and future trends. Biotechnol Adv 54:107796. https://doi.org/10.1016/j.biotechadv.2021.107796
Lucas-González R, Viuda-Martos M, Pérez-Alvarez JA, Fernández-López J (2018) In vitro digestion models suitable for foods: opportunities for new fields of application and challenges. Food Res Int 107:423–436. https://doi.org/10.1016/j.foodres.2018.02.055
Nissen L, Casciano F, Gianotti A (2020) Intestinal fermentation in vitro models to study food-induced gut microbiota shift: an updated review. FEMS Microbiol Lett 367:fnaa097. https://doi.org/10.1093/femsle/fnaa097
Ahire JJ, Kashikar MS, Madempudi RS (2020) Survival and germination of Bacillus clausii UBBC07 spores in in vitro human gastrointestinal tract simulation model and evaluation of clausin production. Front Microbiol 11:1010. https://doi.org/10.3389/fmicb.2020.01010
Ahire JJ, Neelamraju J, Madempudi RS (2020) Behavior of Bacillus coagulans Unique IS2 spores during passage through the Simulator of Human Intestinal Microbial Ecosystem (SHIME) model. LWT-Food Sci Technol 124:109196. https://doi.org/10.1016/j.lwt.2020.109196
Ahire JJ, Mokashe NU, Kashikar MS, Madempudi RS (2022) Survival of Limosilactobacillus reuteri UBLRu-87 during passage through the in vitro gut model system. LWT-Food Sci Technol 164:113652. https://doi.org/10.1016/j.lwt.2022.113652
Pham VT, Mohajeri MH (2018) The application of in vitro human intestinal models on the screening and development of pre-and probiotics. Benef Microbes 9:725–742. https://doi.org/10.3920/BM2017.0164
Kostewicz ES, Abrahamsson B, Brewster M, Brouwers J, Butler J, Carlert S et al (2014) In vitro models for the prediction of in vivo performance of oral dosage forms. Eur J Pharm Sci 57:342–366. https://doi.org/10.1016/j.ejps.2013.08.024
Li C, Yu W, Wu P, Chen XD (2020) Current in vitro digestion systems for understanding food digestion in human upper gastrointestinal tract. Trends Food Sci Technol 96:114–126. https://doi.org/10.1016/j.tifs.2019.12.015
Minekus M, Alminger M, Alvito P, Ballance S, Bohn T, Bourlieu C et al (2014) A standardised static in vitro digestion method suitable for food – an international consensus. Food Funct 5:1113–1124. https://doi.org/10.1039/C3FO60702J
Minekus M, Marteau P, Havenaar R, Veld J (1995) A multicompartmental dynamic computer-controlled model simulating the stomach and small intestine. Altern Lab Anim 23:197–209. https://doi.org/10.1177/026119299502300205
Clark RL, Connors BM, Stevenson DM, Hromada SE, Hamilton JJ, Amador-Noguez D et al (2021) Design of synthetic human gut microbiome assembly and butyrate production. Nat Commun 12:1–16. https://doi.org/10.1038/s41467-021-22938-y
Morrison AB, Campbell JA (1960) The relationship between physiological availability of salicylates and riboflavin and in vitro disintegration time of enteric coated tablets. J Am Pharm Assoc 49:473–478. https://doi.org/10.1002/jps.3030490717
Cressman WA, Janicki CA, Johnson PC, Doluisio JT, Braun GA (1969) In vitro dissolution rates of aminorex dosage forms and their correlation with in vivo availability. J Pharm Sci 58:1516–1520. https://doi.org/10.1002/jps.2600581220
Davis RE, Hartman CW, Fincher JH (1971) Dialysis of ephedrine and pentobarbital from whole human saliva and simulated saliva. J Pharm Sci 60:429–432. https://doi.org/10.1002/jps.2600600318
Braybrooks MP, Barry BW, Abbs ET (1975) The effect of mucin on the bioavailability of tetracycline from the gastrointestinal tract; in vivo, in vitro correlations. J Pharm Pharmacol 27:508–515. https://doi.org/10.1111/j.2042-7158.1975.tb09493.x
Miller TL, Wolin MJ (1981) Fermentation by the human large intestine microbial community in an in vitro semicontinuous culture system. Appl Environ Microbiol 42:400–407. https://doi.org/10.1128/aem.42.3.400-407.1981
Macfarlane GT, Cummings JH, Macfarlane S, Gibson GR (1989) Influence of retention time on degradation of pancreatic enzymes by human colonic bacteria grown in a 3-stage continuous culture system. J Appl Bacteriol 67:521–527. https://doi.org/10.1111/j.1365-2672.1989.tb02524.x
Molly K, Vande Woestyne M, Verstraete W (1993) Development of a 5-step multi-chamber reactor as a simulation of the human intestinal microbial ecosystem. Appl Microbiol Biotechnol 39:254–258. https://doi.org/10.1007/BF00228615
Van den Abbeele P, Roos S, Eeckhaut V, MacKenzie DA, Derde M, Verstraete W et al (2012) Incorporating a mucosal environment in a dynamic gut model results in a more representative colonization by lactobacilli. Microb Biotechnol 5:106–115. https://doi.org/10.1111/j.1751-7915.2011.00308.x
Possemiers S, Pinheiro I, Verhelst A, Van den Abbeele P, Maignien L, Laukens D et al (2013) A dried yeast fermentate selectively modulates both the luminal and mucosal gut microbiota and protects against inflammation, as studied in an integrated in vitro approach. J Agri Food Chem 61:9380–9392. https://doi.org/10.1021/jf402137r
Marzorati M, Vanhoecke B, De Ryck T, Sadaghian Sadabad M, Pinheiro I, Possemiers S et al (2014) The HMI™ module: a new tool to study the host-microbiota interaction in the human gastrointestinal tract in vitro. BMC Microbiol 14:1–14. https://doi.org/10.1186/1471-2180-14-133
Minekus M, Smeets-Peeters M, Bernalier A, Marol-Bonnin S, Havenaar R, Marteau P et al (1999) A computer-controlled system to simulate conditions of the large intestine with peristaltic mixing, water absorption and absorption of fermentation products. Appl Microbiol Biotechnol 53:108–114. https://doi.org/10.1007/s002530051622
Cordonnier C, Thévenot J, Etienne-Mesmin L, Denis S, Alric M, Livrelli V et al (2015) Dynamic in vitro models of the human gastrointestinal tract as relevant tools to assess the survival of probiotic strains and their interactions with gut microbiota. Microorganisms 3:725–745. https://doi.org/10.3390/microorganisms3040725
Wickham M, Faulks R (2007) WO/2007/010238 WIPO. https://patentscope.wipo.int/search/en/detail.jsf?docId=WO2007010238. Accessed 14 Nov 2022
Kong F, Singh RP (2010) A human gastric simulator (HGS) to study food digestion in human stomach. J Food Sci 75:E627–E635. https://doi.org/10.1111/j.1750-3841.2010.01856.x
Guerra A, Denis S, le Goff O, Sicardi V, François O, Yao AF et al (2016) Development and validation of a new dynamic computer-controlled model of the human stomach and small intestine. Biotechnol Bioeng 113:1325–1335. https://doi.org/10.1002/bit.25890
Chen L, Xu Y, Fan T, Liao Z, Wu P, Wu X et al (2016) Gastric emptying and morphology of a ‘near real’ in vitro human stomach model (RD-IV-HSM). J Food Eng 183:1–8. https://doi.org/10.1016/j.jfoodeng.2016.02.025
Barroso E, Cueva C, Peláez C, Martínez-Cuesta MC, Requena T (2015) Development of human colonic microbiota in the computer-controlled dynamic SIMulator of the GastroIntestinal tract SIMGI. LWT-Food Sci Technol 61:283–289. https://doi.org/10.1016/j.lwt.2014.12.014
Wright ND, Kong F, Williams BS, Fortner L (2016) A human duodenum model (HDM) to study transport and digestion of intestinal contents. J Food Eng 171:129–136. https://doi.org/10.1016/j.jfoodeng.2015.10.013
Wang P, Rubio A, Duncan H, Donachie E, Holtrop G, Lo G et al (2020) Pivotal roles for pH, lactate, and lactate-utilizing bacteria in the stability of a human colonic microbial ecosystem. mSystems 5:e00645–20. https://doi.org/10.1128/mSystems.00645-20
Berner A, Fuentes S, Dostal A, Payne AN, Vazquez Gutierrez P, Chassard C et al (2013) Novel Polyfermentor Intestinal Model (PolyFermS) for controlled ecological studies: validation and effect of pH. PloS One 8:e77772. https://doi.org/10.1371/journal.pone.0077772
Fehlbaum S, Chassard C, Haug MC, Fourmestraux C, Derrien M, Lacroix C (2015) Design and investigation of PolyFermS in vitro continuous fermentation models inoculated with immobilized fecal microbiota mimicking the elderly colon. PLoS One 10:e0142793. https://doi.org/10.1371/journal.pone.0142793
Cieplak T, Wiese M, Nielsen S, Van de Wiele T, van den Berg F, Nielsen DS (2018) The smallest intestine (TSI)—a low volume in vitro model of the small intestine with increased throughput. FEMS Microbiol Lett 365:fny231. https://doi.org/10.1093/femsle/fny231
Wiese M, Khakimov B, Nielsen S, Sørensen H, van den Berg F, Nielsen DS (2018) CoMiniGut—a small volume in vitro colon model for the screening of gut microbial fermentation processes. PeerJ 6:e4268. https://doi.org/10.7717/peerj.4268
Ekins S, Rose J (2002) In silico ADME/Tox: the state of the art. J Mol Graph Model 20:305–309. https://doi.org/10.1016/S1093-3263(01)00127-9
Yamashita F, Hashida M (2004) In silico approaches for predicting ADME properties of drugs. Drug Metab Pharmacokinet 19:327–338. https://doi.org/10.2133/dmpk.19.327
Kamerman DJ, Wilkinson MH (2002) In silico modelling of the human intestinal microflora. International Conference on Computational Science. Springer, Berlin, Heidelberg, pp 117–126
Jong P, Vissers MM, van der Meer R, Bovee-Oudenhoven IM (2007) In silico model as a tool for interpretation of intestinal infection studies. Appl Environ Microbiol 73:508–515. https://doi.org/10.1128/2FAEM.01299-06
Jamei M, Marciniak S, Feng K, Barnett A, Tucker G, Rostami-Hodjegan A (2009) The Simcyp® population-based ADME simulator. Expert Opin Drug Metab Toxicol 5:211–223. https://doi.org/10.1517/17425250802691074
Sjögren E, Westergren J, Grant I, Hanisch G, Lindfors L, Lennernäs H et al (2013) In silico predictions of gastrointestinal drug absorption in pharmaceutical product development: application of the mechanistic absorption model GI-Sim. Eur J Pharm Sci 49:679–698. https://doi.org/10.1016/j.ejps.2013.05.019
Barth BB, Henriquez CS, Grill WM, Shen X (2017) Electrical stimulation of gut motility guided by an in silico model. J Neural Eng 14:066010. https://doi.org/10.1088/1741-2552/aa86c8
Lin C, Culver J, Weston B, Underhill E, Gorky J, Dhurjati P (2018) GutLogo: agent-based modeling framework to investigate spatial and temporal dynamics in the gut microbiome. PLoS One 13:e0207072. https://doi.org/10.1371/journal.pone.0207072
Tanner SA, Chassard C, Zihler Berner A, Lacroix C (2014) Synergistic effects of Bifidobacterium thermophilum RBL67 and selected prebiotics on inhibition of Salmonella colonization in the swine proximal colon PolyFermS model. Gut Pathog 6:1–12. https://doi.org/10.1186/s13099-014-0044-y
Vamanu E (2017) Effect of gastric and small intestinal digestion on lactic acid bacteria activity in a GIS1 simulator. Saudi J Biol Sci 24:1453–1457. https://doi.org/10.1016/j.sjbs.2015.06.028
Ceuppens S, Uyttendaele M, Drieskens K, Heyndrickx M, Rajkovic A, Boon N et al (2012) Survival and germination of Bacillus cereus spores without outgrowth or enterotoxin production during in vitro simulation of gastrointestinal transit. Appl Environ Microbiol 78:7698–7705. https://doi.org/10.1128/AEM.02142-12
Molly K, Woestyne MV, Smet ID, Verstraete W (1994) Validation of the Simulator of the Human Intestinal Microbial Ecosystem (SHIME) reactor using microorganism-associated activities. Microb Ecol Health Dis 7:191–200. https://doi.org/10.3109/08910609409141354
Martoni C, Bhathena J, Jones ML, Urbanska AM, Chen H, Prakash S (2007) Investigation of microencapsulated BSH active Lactobacillus in the simulated human GI tract. J Biomed Biotechnol 2007:13684. https://doi.org/10.1155/2007/13684
Oomen AG, Rompelberg CJM, Bruil MA, Dobbe CJG, Pereboom DPKH, Sips AJAM (2003) Development of an in vitro digestion model for estimating the bioaccessibility of soil contaminants. Arch Environ Contam Toxicol 44:0281–0287. https://doi.org/10.1007/s00244-002-1278-0
Brodkorb A, Egger L, Alminger M, Alvito P, Assunção R, Ballance S et al (2019) INFOGEST static in vitro simulation of gastrointestinal food digestion. Nat Protoc 14:991–1014. https://doi.org/10.1038/s41596-018-0119-1
Van den Abeele J, Rubbens J, Brouwers J, Augustijns P (2017) The dynamic gastric environment and its impact on drug and formulation behaviour. Eur J Pharm Sci 96:207–231. https://doi.org/10.1016/j.ejps.2016.08.060
Humphrey SP, Williamson RT (2001) A review of saliva: normal composition, flow, and function. J Prosthet Dent 85:162–169. https://doi.org/10.1067/mpr.2001.113778
Hedren E, Diaz V, Svanberg U (2002) Estimation of carotenoid accessibility from carrots determined by an in vitro digestion method. Eur J Clin Nutr 56:425–430. https://doi.org/10.1038/sj.ejcn.1601329
Passannanti F, Nigro F, Gallo M, Tornatore F, Frasso A, Saccone G et al (2017) In vitro dynamic model simulating the digestive tract of 6-month-old infants. PLoS One 12:e0189807. https://doi.org/10.1371/journal.pone.0189807
Cueva C, Gil-Sánchez I, Tamargo A, Miralles B, Crespo J, Bartolomé B et al (2019) Gastrointestinal digestion of food-use silver nanoparticles in the dynamic SIMulator of the GastroIntestinal tract (simgi®). Impact on human gut microbiota. Food Chem Toxicol 132:110657. https://doi.org/10.1016/j.fct.2019.110657
Farré R, Tack J (2013) Food and symptom generation in functional gastrointestinal disorders: physiological aspects. Am J Gastroenterol 108:698–706. https://doi.org/10.1038/ajg.2013.24
Nugent SG, Kumar D, Rampton DS, Evans DF (2001) Intestinal luminal pH in inflammatory bowel disease: possible determinants and implications for therapy with aminosalicylates and other drugs. Gut 48:571–577. https://doi.org/10.1136/gut.48.4.571
Fallingborg J (1999) Intraluminal pH of the human gastrointestinal tract. Dan Med Bull 46:183–196
Maurer AH (2016) Gastrointestinal motility, part 2: small-bowel and colon transit. J Nucl Med Technol 44:12–18. https://doi.org/10.2967/jnumed.113.134551
Schneyer LH, Young JA, Schneyer CA (1972) Salivary secretion of electrolytes. Physiol Rev 52:720–777. https://doi.org/10.1152/physrev.1972.52.3.720
Varga G (2015) Physiology of the salivary glands. Surgery 33:581–586. https://doi.org/10.1016/j.mpsur.2015.09.003
Bornhorst GM, Singh RP (2014) Gastric digestion in vivo and in vitro: how the structural aspects of food influence the digestion process. Annu Rev Food Sci Technol 5:111–132. https://doi.org/10.1146/annurev-food-030713-092346
Campbell J, Berry J, Liang Y (2019) Anatomy and physiology of the small intestine. In: Yeo CJ (ed) Shackelford’s surgery of the alimentary tract. Elsevier, pp 817–841
Klindt-Toldam S, Larsen SK, Saaby L, Olsen LR, Svenstrup G, Müllertz A et al (2016) Survival of Lactobacillus acidophilus NCFM® and Bifidobacterium lactis HN019 encapsulated in chocolate during in vitro simulated passage of the upper gastrointestinal tract. LWT-Food Sci Technol 74:404–410. https://doi.org/10.1016/j.lwt.2016.07.053
Denaro M, Smeriglio A, Trombetta D (2021) Antioxidant and anti-inflammatory activity of Citrus flavanones mix and its stability after in vitro simulated digestion. Antioxidants 10:140. https://doi.org/10.3390/antiox10020140
Byrd JC, Bresalier RS (2000) Alterations in gastric mucin synthesis by Helicobacter pylori. World J Gastroenterol 6:475. https://doi.org/10.3748/2Fwjg.v6.i4.475
McConnell EL, Fadda HM, Basit AW (2008) Gut instincts: explorations in intestinal physiology and drug delivery. Int J Pharm 364:213–226. https://doi.org/10.1016/j.ijpharm.2008.05.012
Curto AL, Pitino I, Mandalari G, Dainty JR, Faulks RM, Wickham MSJ (2011) Survival of probiotic lactobacilli in the upper gastrointestinal tract using an in vitro gastric model of digestion. Food Microbiol 28:1359–1366. https://doi.org/10.1016/j.fm.2011.06.007
Rémond D, Shahar DR, Gille D, Pinto P, Kachal J, Peyron MA et al (2015) Understanding the gastrointestinal tract of the elderly to develop dietary solutions that prevent malnutrition. Oncotarget 6:13858. https://doi.org/10.18632/oncotarget.4030
Braghetto I, Davanzo C, Korn O, Csendes A, Valladares H, Herrera E et al (2009) Scintigraphic evaluation of gastric emptying in obese patients submitted to sleeve gastrectomy compared to normal subjects. Obes Surg 19:1515–1521. https://doi.org/10.1007/s11695-009-9954-z
Szarka LA, Camilleri M (2012) Methods for the assessment of small-bowel and colonic transit. Semin Nucl Med 42:113–123. https://doi.org/10.1053/j.semnuclmed.2011.10.004
Dekaboruah E, Suryavanshi MV, Chettri D, Verma AK (2020) Human microbiome: an academic update on human body site specific surveillance and its possible role. Arch Microbiol 202:2147–2167. https://doi.org/10.1007/s00203-020-01931-x
Ragonnaud E, Biragyn A (2021) Gut microbiota as the key controllers of “healthy” aging of elderly people. Immun Ageing 18:2. https://doi.org/10.1186/s12979-020-00213-w
Wall R, Ross RP, Ryan CA, Hussey S, Murphy B, Fitzgerald GF et al (2009) Role of gut microbiota in early infant development. Clin Med Insights Pediatr 3:S2008. https://doi.org/10.4137/CMPed.S2008
Valeur J, Berstad A (2010) Colonic fermentation: a neglected topic in human physiology education. Adv Physiol Educ 34:22–22. https://doi.org/10.1152/advan.00103.2009
Shanahan F (2013) The colonic microbiota in health and disease. Curr Opin Gastroenterol 29:49–54. https://doi.org/10.1097/MOG.0b013e32835a3493
Rodes L, Coussa-Charley M, Marinescu D, Paul A, Fakhoury M, Abbasi S et al (2013) Design of a novel gut bacterial adhesion model for probiotic applications. Artif Cells Nanomed Biotechnol 41:116–124. https://doi.org/10.3109/10731199.2012.712047
Venema K, Van den Abbeele P (2013) Experimental models of the gut microbiome. Best Pract Res Clin Gastroenterol 27:115–126. https://doi.org/10.1016/j.bpg.2013.03.002
Martin G, Kolida S, Marchesi JR, Want E, Sidaway JE, Swann JR (2018) In vitro modeling of bile acid processing by the human fecal microbiota. Front Microbiol 9:1153. https://doi.org/10.3389/fmicb.2018.01153
Payne AN, Zihler A, Chassard C, Lacroix C (2012) Advances and perspectives in in vitro human gut fermentation modeling. Trends Biotechnol 30:17–25. https://doi.org/10.1016/j.tibtech.2011.06.011
Barros L, Retamal C, Torres H, Zúñiga RN, Troncoso E (2016) Development of an in vitro mechanical gastric system (IMGS) with realistic peristalsis to assess lipid digestibility. Food Res Int 90:216–225. https://doi.org/10.1016/j.foodres.2016.10.049
Liu W, Fu D, Zhang X, Chai J, Tian S, Han J (2019) Development and validation of a new artificial gastric digestive system. Food Res Int 122:183–190. https://doi.org/10.1016/j.foodres.2019.04.015
Li Y, Fortner L, Kong F (2019) Development of a Gastric Simulation Model (GSM) incorporating gastric geometry and peristalsis for food digestion study. Food Res Int 125:108598. https://doi.org/10.1016/j.foodres.2019.108598
Blutt SE, Crawford SE, Ramani S, Zou WY, Estes MK (2018) Engineered human gastrointestinal cultures to study the microbiome and infectious diseases. Cell Mol Gastroenterol Hepatol 5:241–251. https://doi.org/10.1016/j.jcmgh.2017.12.001
Min S, Kim S, Cho SW (2020) Gastrointestinal tract modeling using organoids engineered with cellular and microbiota niches. Exp Mol Med 52:227–237. https://doi.org/10.1038/s12276-020-0386-0
Costa J, Ahluwalia A (2019) Advances and current challenges in intestinal in vitro model engineering: a digest. Front Bioeng Biotechnol 7:144. https://doi.org/10.3389/fbioe.2019.00144
Bricks T, Paullier P, Legendre A, Fleury MJ, Zeller P, Merlier F et al (2014) Development of a new microfluidic platform integrating co-cultures of intestinal and liver cell lines. Toxicol In-vitro 28:885–895. https://doi.org/10.1016/j.tiv.2014.02.005
Sung JH, Yu J, Luo D, Shuler ML, March JC (2011) Microscale 3-D hydrogel scaffold for biomimetic gastrointestinal (GI) tract model. Lab Chip 11:389–392. https://doi.org/10.1039/C0LC00273A
Shim KY, Lee D, Han J, Nguyen NT, Park S, Sung JH (2017) Microfluidic gut-on-a-chip with three-dimensional villi structure. Biomed Microdevices 19:1–10. https://doi.org/10.1007/s10544-017-0179-y
Kim HJ, Huh D, Hamilton G, Ingber DE (2012) Human gut-on-a-chip inhabited by microbial flora that experiences intestinal peristalsis-like motions and flow. Lab Chip 12:2165–2174. https://doi.org/10.1039/c2lc40074j
Waclawiková B, Codutti A, Alim K, El Aidy S (2022) Gut microbiota-motility interregulation: insights from in vivo, ex vivo and in silico studies. Gut Microbes 14:1997296. https://doi.org/10.1080/19490976.2021.1997296
Molina Ortiz JP, McClure DD, Shanahan ER, Dehghani F, Holmes AJ, Read MN (2021) Enabling rational gut microbiome manipulations by understanding gut ecology through experimentally-evidenced in silico models. Gut Microbes 13:1965698. https://doi.org/10.1080/19490976.2021.1965698
Sen P, Orešič M (2019) Metabolic modeling of human gut microbiota on a genome scale: an overview. Metabolites 9:22. https://doi.org/10.3390/metabo9020022
Henson MA (2021) Interrogation of the perturbed gut microbiota in gouty arthritis patients through in silico metabolic modeling. Eng Life Sci 21:489–501. https://doi.org/10.1002/elsc.202100003
Mandalari G, Adel-Patient K, Barkholt V, Baro C, Bennett L, Bublin M et al (2009) In vitro digestibility of β-casein and β-lactoglobulin under simulated human gastric and duodenal conditions: a multi-laboratory evaluation. Regul Toxicol Pharmacol 55:372–381. https://doi.org/10.1016/j.yrtph.2009.08.010
Yeo S, Lee S, Park H, Shin H, Holzapfel W, Huh CS (2016) Development of putative probiotics as feed additives: validation in a porcine-specific gastrointestinal tract model. Appl Microbiol Biotechnol 100:10043–10054. https://doi.org/10.1007/s00253-016-7812-1
Cichoke AJ (1999) The complete book of enzyme therapy. Penguin, Chapter, p 2. https://patentscope.wipo.int/search/en/detail.jsf?10.1007/s12602-023-10052-ydocId=WO2007010238. Accessed 14 Nov 2022
Acknowledgements
The authors gratefully acknowledge the support of Mr. V. L. Rathi and Mr. M. Kabra at the Advanced Enzyme Technologies Limited, India.
Author information
Authors and Affiliations
Contributions
Y. D.: formal analysis, writing including review and editing, and writing of original draft. K. K. and N. B.: writing including review and editing. D. S.: review. J. J. A.: conceptualization and writing including review and editing. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics Approval
This study does not contain any work related to the participation of humans and/or animals.
Competing Interests
Y. D., K. K., N. B., D. S. and J. J. A. were employed by the Advanced Enzyme Technologies Limited. This does not alter our adherence to journal policies on sharing data and materials.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Dixit, Y., Kanojiya, K., Bhingardeve, N. et al. In Vitro Human Gastrointestinal Tract Simulation Systems: A Panoramic Review. Probiotics & Antimicro. Prot. 16, 501–518 (2024). https://doi.org/10.1007/s12602-023-10052-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12602-023-10052-y