
Abstract
This chapter is divided into three sections, each presenting a different type of methodologies that are commonly used to study the link between food digestion and health. The first section focuses on in vivo methods, which are those that involve a living organism. The main types of epidemiological study design are presented, including observational and intervention studies. The relatively new field of nutritional epidemiology is further introduced, while animal studies are also briefly considered. The second section concerns in vitro experiments, which simulate digestive processes outside the body. The principles and practicalities of different static and dynamic in vitro models encountered in the literature are presented. Further, in silico approaches to digestion studies are discussed in the third section, with emphasis on developing understanding of digestive processes using numerical and computer techniques, with the aim to produce predictive models.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Understanding the mechanisms of digestion is important in promoting the design of food formulations with increased health benefits by tailoring their digestive profiles. Such knowledge is also important for functional foods and pharmaceuticals. However, studying digestive processes is challenging due to reasons such as the complex processes occurring during digestion (see for example chapters “The Digestive Tract” and “Consumer Psychology and Eating Behaviour” for the physiology and psychology of eating, respectively); the complex nature of foods and meals (Bornhorst, Gouseti, Wickham, & Bakalis, 2016); the vast variability between individuals (Bratten & Jones, 2009), and the limitations of currently available techniques (Gidley, 2013). To date, knowledge of digestive processes typically comes from broadly three types of research methodologies. In vivo investigations involve human or animal studies, in vitro experiments study digestion outside the body, and in silico models simulate digestive processes using numerical and computational methods.
Important advantage of in vivo studies, in particular human studies, is the high relevance of the outcomes, as the subject of the study is also the targeted end user of the foods (Hur, Lim, Decker, & McClements, 2011; Minekus et al., 2014). On the other hand, in vitro or in silico methodologies may be preferred in studies aimed at gaining mechanistic understanding of digestion, as they offer the potential to operate at simpler, well-defined conditions. However, in vitro outcomes should be interpreted with caution to ensure physiological relevance.
A tiered approach has been suggested in studying bioaccessibility and/or bioavailability of nutrients from foods, in which in silico and in vitro models are used at a first step to provide evidence for the necessity of in vivo animal and human trials (Lefebvre et al., 2015). One of the aims of computational and experimental simulations may therefore be the reduction of the necessary in vivo studies, as the latter are generally expensive, time-consuming, laborious, and often ethically compromised.
The present chapter considers the three methodologies separately and briefly presents existing approaches and techniques used in each one. It is our intention to avoid replicating information provided elsewhere in this book, and in these cases the reader is referred to the relevant chapters.
2 In Vivo Methods
While traditionally linked with the medical/pharmaceutical sciences, in vivo methods provide a powerful tool for studying the link between food and health. For example, there are in vivo studies that aim to correlate a dietary exposure (e.g. saturated fat consumption) with a biomarker (e.g. serum cholesterol level) and ultimately with a health outcome (e.g. disease prevention). This type of study often lies on the border between digestion and nutritional studies, and typically involves epidemiological study designs (discussed in Sect. 2.1).
Another type of in vivo investigations focuses on gaining insight into the mechanisms of digestion. These include, but are not limited to, imaging techniques used to characterise flow of the material in the gut, and intubation techniques used to examine gut motility. Use of imaging techniques is extensively discussed in the chapter “Quantitative Characterisation of Digestion Processes” and will not be included here; intubation will be briefly introduced in Sect. 2.2. Section 2.3 briefly introduces animal studies.
2.1 Epidemiological Studies
The term “epidemic” was introduced by Hippocrates (ca. 460–377 BC) to describe conditions that occur during finite periods of time, for example an outbreak of a disease. On the other end, diseases that occur permanently within a population or region were termed “endemic”, for example malaria in Africa is practically a permanent concern (Willett, 2013). In 1995, Last defined epidemiology as “the study of the distribution and determinants of health-related states or events (including disease), and the application of this study to the control of diseases and other health problems”. This definition is largely applicable to date.
Epidemiological studies typically seek to investigate the link between an exposure and a health outcome. The three main common elements in all epidemiological studies involve (1) identification of an exposure (for example high fat diet) and how to measure it; (2) identification and evaluation of the associated health outcome (e.g. breast cancer); and (3) statistical analysis to assess potential correlation between the exposure and the outcome (Thiese, 2014). The overall aim of epidemiological studies is to either generate hypotheses or to provide evidence for existing hypotheses.
2.1.1 Epidemiological Study Designs
A number of epidemiological studies exists differing in the study design and/or the desired outcome. These will be briefly introduced in this section and the interested reader is encouraged to seek detailed information elsewhere [for example see Carneiro and Howard (2011), Grimes and Schulz (2002), Hajat (2011), Last and International Epidemiological Association (2001), Thiese (2014), and Timmreck (2002)].
Classification of the major epidemiological study designs is schematically shown in Fig. 1 (Grimes & Schulz, 2002). Depending on whether the investigator intervenes in the subjects’ dietary habits or not, a study may be experimental (interventional) or observational, respectively. In observational designs the researcher studies the participants in their natural environments. The subjects’ individual dietary habits are therefore determined by factors such as personal preferences, availability, doctors’ prescriptions, fashion, and policy decisions (Carlson & Morrison, 2009). Further, in an observational study design, the investigator may study a single group alone (descriptive) or compare between two groups, one of which acts as the control (analytical). Individuals in the control group are expected to be unexposed to the predetermined exposure measure (or to the outcome, depending on the specific study design). Descriptive studies are often used to generate a hypothesis, while analytical studies may generate or support a hypothesis (Hajat, 2011).

Types of epidemiological studies (Grimes & Schulz, 2002)
Analytical observational studies further involve three main types of study design, depending on the relative time between exposure and health outcome. Cross-sectional studies consider exposure and associated outcome at a single point in time, and compare between the control and exposed groups. For example, between two groups of adults, one obese and the other not, the former shows higher rate of arthritis (Grimes & Schulz, 2002). This type of studies is usually inexpensive and straightforward in their design, implementation, and interpretation. However, they lack information about temporality. In the previous example, it is unclear whether the increased stress on the joints preceded arthritis or occurrence of arthritis resulted in reduced physical activity and increased body weight (Grimes & Schulz, 2002).
Cohort and case–control studies consider exposure and outcome in two reverse orders, as seen in Fig. 1. In cohort study design, the “active group” consists of individuals who are being/have been exposed to the identified risk factor (e.g. high-carbohydrate diet), while the other, the control, involves non-exposed participants. The two groups are then monitored with time and the health outcome (e.g. occurrence of diabetes) is observed. Cohort studies demonstrate temporality, as the exposure precedes the outcome. However, they require time and they may be expensive. In addition, they are ineffective in the case of rare diseases as the probability of observing a health outcome is small (Thiese, 2014).
In case–control studies, selection of the two groups is based on their disease status. The “active” group is the one affected by the disease, whereas the control group(s) is disease-free. The researcher then investigates the degree of exposure of each group to a risk factor (Hajat, 2011). Using this method, it is possible, for example, to examine outbreaks of food-borne diseases. In a real case, the passengers of a ship that showed increased cases of vomiting and diarrhoea were divided into those who became ill and those who did not. Examination of their exposure to food identified a potato salad responsible for the outbreak of shigella (Grimes & Schulz, 2002).
Observational studies are popular among researchers. Using observational studies, for example, a link between high salt consumption and overweight/obesity (Boccia, 2015), or between high dairy consumption and metabolic syndrome in adults (Moosavian, Haghighatdoost, Surkan, & Azadbakht, 2017), or children’s dietary habits and behaviour (Brown & Ogden, 2004) have been indicated. Furthermore, large-scale observational studies can provide vital information for generating and supporting generalised dietary advice and recommendations. For example, recommendations for increased consumption of vegetables or reduced consumption of salt are evidence-based on the outcomes of observational research (Gidley, 2013).
Two reported limitations of this study design involve (1) limitations on determining causality, as the evidence provided on the cause-and-effect relationship between the consumed food and the health outcome is weak, and (2) limitations on specificity, as due to the variability of human diet the effect of individual food components is unclear (Gidley, 2013).
In intervention studies, the researcher determines the degree of exposure of the “intervention group” to the exposure measure (e.g. the food under investigation) through the detailed experimental design. Intervention trials share similarities with the cohort study design in that exposure to a risk/treatment factor(s) differentiates the “intervention” from the “control” groups and participants are assessed over a period of time for health outcomes (Grimes & Schulz, 2002).
There are many elements that characterise intervention trials. Among these, the randomised, double-blind, placebo controlled study design has been reported as the optimal study design in clinical and nutritional studies (Misra, 2012; Slavin, 2013; Willett, 2013). Table 1 summarises important features and terminology of interventional studies.
Intervention studies are typically controlled trials. This is because they typically involve comparison between at least one “intervention” group that is exposed to the food under investigation and at least one “control” group that does not receive the investigated food. Control measures may vary. Placebo control refers to a measure that has the same form as the investigated treatment but it is free from the active component. As an example, the placebo sugary drink looks and tastes like the intervention sugary drink but without addition of the active component, which could be dietary fibre (Jenkins et al., 1978). The two groups may also be fed with alternative meals. For example, in a trial investigating the effect of structure and particle size on digestion, two groups were fed with an otherwise identical porridge meal prepared with either oat flakes or oat powder and the metabolic responses were measured (Mackie et al., 2017).
Another important element in intervention trials refers to how the individuals are allocated to the intervention or control group. By large, the preferred study design to assess a hypothesis is the randomised controlled study (RCT). In this method, participants with comparable baseline characteristics (e.g. age, weight, health conditions) are selected and they are randomly allocated to the intervention or control group. This process helps protecting the investigation from selection bias (Kahan, Rehal, & Cro, 2015). When RCT is considered complicated, expensive, or even not feasible, for example for ethical reasons, other study designs are employed. In quasi-randomised and non-randomised designs, no effort is taken to account for any randomisation element. For example, the investigator may allocate subjects alphabetically, in order of age, etc. (Grimes & Schulz, 2002); or the participants may select their group allocation by volunteering to be exposed to an experimental treatment. Such methods are likely to introduce a selection bias in the study, which should be taken into account when interpreting the results.
Blinding of the intervention may further help reducing bias of the experimental outcomes. In single-blinded study design, either the investigator or the subjects (but not both) are aware of who is receiving which intervention diet. In double-blinded studies, neither the researcher nor the participants know which diet is linked with which subject.
2.1.2 Nutritional Epidemiology
Nutrutional epidemiology refers to the use of epidemiological principles for the study of nutrition and health, and it can be regarded as a subdivision of epidemiology. It has been recently introduced as a distinct field of study, although the practice is not new. For example, one of the first reported intervention trials was that of Lind, who in 1753 used controlled study design to study treatment of scurvy in the Salisbury. Lind split 12 crew members affected by the disease in groups of two. All participants had the same core diet, while each of the six groups additionally received cider, elixir of vitriol, vinegar, sea water, oranges and lemons, and a purgative mixture, respectively. His findings enabled him to associate scurvy with orange and lemon consumption, which was later assigned to vitamin C (Sutton, 2003). This and many other examples gradually led to the introduction of nutritional epidemiology as a separate research field (Willett, 2013).
A distinctive aspect in nutritional epidemiological studies, when compared to medical epidemiology, is the nature of the exposure: the complexity and variability of what we eat, compared for example to the well defined nature of a medical pill (Willett, 1987; Wilson & Temple, 2001). Adding to this, the intra-human as well as interhuman variability of human metabolism, including the effect of non-dietary factors such as stress on digestion, poses further challenges to the nutritional epidemiologist and to those with interest in digestion studies. These factors are particularly challenging in the case of observational studies.
Indeed, one of the major acknowledged challenges for nutritional epidemiologists refers to the characterisation and practical measurement of dietary exposure (Willett, 1987; Wilson & Temple, 2001). Foods are inherently complex, multiphase systems that are kinetically trapped within a food structure. The way that the human digestive system acts on foods depends on food variability, including the exact food ingredients and structures, how we prepare the food (processing conditions), and the amounts and combinations that are consumed (Wilson & Temple, 2001). Even unprocessed, “simple” food ingredients, such as vegetables or fruits, can vary in their properties depending on the weather conditions, soil composition, ripening time, etc. (Wilson & Temple, 2001). In addition, it is known that the digestion of a food component may be affected by the digestion of other food components (Hur et al., 2011).
This uncertainty of determining and measuring dietary input has provoked a debate among researchers. For example, there are those who fully question the likelihood of acquiring useful dietary information of free-living individuals and therefore the usefulness of carrying out observational epidemiological studies at all. There are also those who regard diet within a country as too homogeneous to provide any useful correlations with health (Willett, 2013). In a more recent trend, some researchers take a different approach. They consider food groups or dietary patterns rather than individual dietary components and use statistical methods to link these food groups or dietary patterns with health (Hoffmann, Schulze, Schienkiewitz, Nöthlings, & Boeing, 2004; Hu, 2002; Wilson & Temple, 2001).
Compared to observational studies, quantification of diet is easier to determine in experimental trials. One reported limitation of intervention nutritional trials, however, refers to the fact that intervening to the subjects’ food consumption habits renders the diet more artificial, and therefore any results should be treated with care (Gidley, 2013). As an example, while controlled metabolic studies have demonstrated that increased consumption of cholesterol or of saturated fats, and decreased consumption of polyunsaturated fats result in an increase in serum cholesterol levels, this has not been verified in a number of observational cross-sectional studies (Willett, 2013). A possible explanation for this observation is that the amount (and combinations) of lipids typically consumed as part of a diet have marginal effect on serum cholesterol and larger quantities, such as those offered in intervention studies, are needed to create any measurable effect (Willett, 2013). Another limitation of nutritional trials refers to the fact that the outcome is often a biomarker (for example serum cholesterol levels) and it is only indirectly related to the health condition (for example heart disease or stroke) (Gidley, 2013). The link between the biomarker and the health conditions needs to be separately verified.
2.2 Other In Vivo Studies
While epidemiology is a very popular technique for studying the link between nutrition, digestion, and health, there are a number of other methods (besides imaging, described in chapter “Quantitative Characterisation of Digestion Processes”) that are used to obtain information about digestibility and bioavailability of nutrients. For example, intubation has long been used to provide insight on gut motility (Kong & Singh, 2008a). This is a highly invasive technique, which requires insertion of a measuring device into the subject’s gut. The gastric barostat falls within this category and involves introduction of a balloon (max. volume 1.0–1.2 L) that is connected to a barostat into the subject’s stomach. The intraballoon volume or pressure is measured under isobaric or isovolumic conditions, respectively, providing information on gastric response to consumption of a meal (Schwizer et al., 2002). Intraluminal manometry is another technique that determines gut motility by measuring pressure changes in the gut at fasting or during digestion (fed). It involves introduction of a catheter, typically through the nose down to the oesophagus, stomach, and small intestines, that has openings in predetermined positions to collect pressure information at different segments of the gut. In a more advanced version of this technique, the use of wireless capsules in the place of the traditional catheter that provide simultaneous information on pressure, temperature, and pH of the investigated segment has simplified the experimental set-up (Farmer, Scott, & Hobson, 2013). Other, indirect methods to assess digestibility include blood test, such as blood glucose level determination, and breath tests (Kong & Singh, 2008a).
2.3 Animal Studies
Animals are often used in nutritional studies as subjects in intervention trials. Compared to human trials, animal studies are typically cheaper and less laborious, while they may offer a degree of ethical flexibility that is prohibiting in humans (McClements, 2007). For example, one common technique to quantify digestion in animals involves animal sacrifice, where the subjects are slaughtered at a predetermined time after feeding and the contents of different sites of the gut are examined to determine progress of digestion and properties of the digested material (Bach Knudsen, Lærke, Steenfeldt, Hedemann, & Jørgensen, 2006; Bornhorst, Roman, Dreschler, & Singh, 2013). Another technique refers to the surgical introduction of one or more permanent cannula(s) to the required site(s) of digestion (e.g. stomach, small intestine) that enables sample collection and characterisation at desired time intervals (cannulation) (Bach Knudsen et al., 2006). Or a catheter can be surgically introduced to the animal’s portal vein and an artery and sampling is used to determine digestibility kinetics (Bach Knudsen et al., 2006).
An important limitation in the use of animals as subjects for studying human digestion reportedly refers to the differences between the animal and the human digestive and metabolic systems (McClements, 2007). This is often taken into account, together with other parameters such as cost and ease of handling, in the choice of animals for digestion studies (McClements, 2007). Example animals that are used in digestion experiments include rodents, pigs, cows, sheep, and horses, with the first two being the most commonly encountered (Darragh & Hodgkinson, 2000; Deglaire & Moughan, 2012; McClements, 2007). Animal selection depends on the targeted investigation, as well as on the targeted population that is studied. For example, use of 3-week-old piglet has been suggested as a model animal to study digestion in infants (Darragh & Moughan, 1995).
The use of animals in scientific studies has significantly progressed knowledge in areas such as digestion and health. In recent years there is a trend to reduce the number of in vivo tests [e.g. European Centre for the Validation of Alternative Methods (Le Ferrec et al., 2001)] and an overall tendency to provide animal-friendly scientific environments [e.g. the UK’s 3Rs initiative with the aim to promote replacement of animals with non-animal alternatives when feasible, reduction of animal use to the minimum required for the targeted scientific advancements, and refinement of experimental designs to ensure minimal animal suffering during the trials (Home Office, Department for Business Innovation & Skills, Department of Health, 2014)].
3 In Vitro Methods
Similar to in vivo, studying digestion in vitro was probably first popularised within the pharmaceutical community, where tests assessing the disintegration of drugs were officially introduced in 1907 and were made compulsory in 1933 in Switzerland by the Pharmacopoeia Helvetica and later by other countries (Al-Gousous & Langguth, 2015). At present, a number of strictly regulated apparatuses is routinely used to assess drug dissolution in vitro (Al-Gousous & Langguth, 2015; McAllister, 2010).
Use of in vitro methods to study food digestion became largely popular in the 1990s. This has significantly boosted research in this area and has led in an inspiring exponential increase in the publications on the topic. It has also led to the introduction of terms such as nutraceuticals and nutrakinetics, which are the “food” analogues of pharmaceuticals and pharmacokinetics (McClements, Li, & Xiao, 2015; Motilva, Serra, & Rubió, 2015).
Simulating digestion outside the body is challenging, due to reasons such as the complexities of the digestive system as well as of the food materials. As an example, the length scales of foods as well as of digestive organs range between at least eight orders of magnitudes, from cm (e.g. first bite, small intestinal diameter) to mm (e.g. rice granules, villi organisations on the intestinal wall), to μm (e.g. starch granules, thickness of single villi layer), down to nm (e.g. plant cell walls, absorption sites in the intestinal wall), and angstroms (e.g. single molecules of sugar, water) (Aguilera, 2005; Bornhorst et al., 2016; Cozzini, 2015).
Adding to this, the digestive system is a complex, multicompartmental organisation that operates and controls digestion through a diverse and interconnected pool of processes and feedback mechanisms (see chapter “The Digestive Tract”) (Cozzini, 2015). Variability in digestive responses between individuals may also be significant. Indicatively, in a study that compared duodenal pH of healthy individuals (control group) and patients with functional dyspepsia, “normal” pH values between four and seven were reported for the control group alone (Bratten & Jones, 2009). Digestive responses have further been associated with factors such as mood, time of the day, level of stress, consumed food, etc. (Bratten & Jones, 2009), further complicating the work of those wanting to replicate it in the laboratory.
Experimental challenges also exist. For example, some of the materials used, such as enzymes and mucins, may be biological and sensitive and/or expensive (Bongaerts, Rossetti, & Stokes, 2007). This may lead in experimental inconsistencies. Indicatively, an interlaboratory study of peanut protein gastric digestion using the same experimental protocol, reported digestion times varying from 0 to 60 min and interlaboratory agreement 77% (Thomas et al., 2004).
In vitro studies are, in principle, easy to carry out and reproducible, compared to in vivo. Ideally, they would also be cheap, high throughput and produce accurate, physiologically relevant results (Hur et al., 2011). Currently, in vitro experiments are often used for rapid screening of different food formulations (Hur et al., 2011) or to gain mechanistic understanding of digestion processes (Gidley, 2013). Besides their popularity in pharmacology, they are also widely used to study protein stability for allergenicity assessments (Dupont & Mackie, 2015; Wickham, Faulks, & Mills, 2009), and to estimate glycaemic index as well as starch fractions (i.e. rapidly, slowly, and non-digestible starch) in food materials (Englyst, Kingman, & Cummings, 1992).
3.1 In Vitro Digestion Models
In vitro models are typically application specific. For example, there are oral models that mimic biting (Meullenet & Gandhapuneni, 2006), mixing (de Wijk, Janssen, & Prinz, 2011), chewing (Salles et al., 2007), shearing (Lvova et al., 2012), tongue action (Benjamin et al., 2012), or compression (de Loubens et al., 2011; Mills, Spyropoulos, Norton, & Bakalis, 2011), and have been specifically developed to study processes such as taste and/or texture perception, or bolus formation. Model selection therefore highly depends on the scientific question of interest and, of course, on the available resources.
There is a number of physiological conditions that a model may replicate. These include, but are not limited to (see also chapter “Influence of physical and structural aspects of food on starch digestion”), the temperature, pH and pH gradients, enzyme types and concentrations, composition and quantities of digestive secretions, residence times, flow and mixing, motility, diffusion and mass transfer, or absorption mechanisms. Usually, the temperature, pH, and enzymatic secretions are among the controlled variables, though the exact selected values may considerably vary depending on the experimental protocol and the specific application (Cozzini, 2015; Donaldson, Rush, Young, & Winger, 2014; Dupont & Mackie, 2015; Marze, 2017).
In vitro models may be monocompartmental, where digestion is simulated in a single container, or multicompartmental, which uses a number of containers to simulate different digestive processes or conditions. Depending on whether the model replicates time-related aspects of digestion (such as mechanical actions, flow, mixing, gut wall contractions, or dynamic pH changes) or not, in vitro models have been characterised as dynamic or static, respectively.
3.1.1 Static In Vitro Digestion Models
Static in vitro models typically offer a simple, fast, and flexible solution to digestion studies (see also chapter “Influence of Physical and Structural Aspects of Food on Starch Digestion”). They comprise a single or a series of batch containers that replicate the different stages of digestion. Often, there are three vessels that simulate oral, gastric, and intestinal digestion, respectively, with a fourth one replicating large intestinal digestion occasionally included (Marze, 2017). The experiment typically operates at 37 °C under mixing conditions that generate homogeneous mixing using devices such as magnetic or overhead stirrers, shaking incubators, or blood rotators [see for example Englyst, Veenstra, and Hudson (2007)]. The digestive fluids usually consist of water with electrolytes, enzymes, and possibly other compounds (mucins, bile salts, etc.), depending on the experimental protocol. The pH is typically adjusted at the beginning of each step to the desired, physiologically relevant value (Marze, 2017). The volume of the material analysed in static in vitro models may vary from μL of material [see for example the OCTOPUS (Maldonado-Valderrama, Terriza, Torcello-Gómez, & Cabrerizo-Vílchez, 2013)] to tens of mL of material [see for example the pH stat (McClements & Li, 2010)]. The pH stat is a popular model that was firstly introduced for lipid digestion studies, for which it has been extensively used (Ban, Jo, Lim, & Choi, 2018; Mun & McClements, 2017; Qin, Yang, Gao, Yao, & McClements, 2016; Salvia-Trujillo, Qian, Martín-Belloso, & McClements, 2013).
Many static in vitro methods exist and it is often difficult to compare between their outcomes. This is partially due to the variability in the simulated physiological conditions used, such as pH or enzyme concentrations (Hur et al., 2011; Marze, 2017). For example, in a 2013 literature review on in vitro tests to study protein allergenicity, protease concentrations in gastric digestion studies has been reported to vary between four orders of magnitude (Mills et al. 2013). Similarly, in a 2008 review on starch digestion, 36 protocols were reported (Woolnough, Bird, Monro, & Brennan, 2010). In an attempt to harmonise static in vitro methods, a network of scientists collectively working in the European (COST) action INFOGEST has published a suggested standardised protocol, which has shown good interlaboratory reproducibility (for more details in the INFOGEST protocol see chapter “Quantitative Characterisation of Digestion Processes”) (Egger et al., 2016; Minekus et al., 2014). Applications of static models to study digestion of different components have been recently reviewed (Bohn et al., 2017; Mackie, Rigby, Macierzanka, & Bajka, 2015).
Static models have also been developed to study absorption of the digested material. These models often incorporate cell cultures (for example a monolayer of Caco2 cells or MDCK cells) (Marze, 2017). Absorption models, including cell culture models, as well as membrane models such as PAMPA and Ussing chambers, have been reviewed in relation to drug absorption studies (Deferme, Annaert, & Augustijns, 2008); however, the same principles pertain to nutrient absorption, including from functional foods (Motilva et al., 2015).
Studying starch hydrolysis is an example of simple static in vitro digestion assays and it has been used to quantify glucose release from carbohydrate food samples, such as rice (Chen et al., 2017; Dhital, Dabit, Zhang, Flanagan, & Shrestha, 2015; Hsu, Chen, Lu, & Chiang, 2015; Van Hung, Lam, Thi, & Phi, 2016), bread (Ronda, Rivero, Caballero, & Quilez, 2012), and oat (Brahma, Weier, & Rose, 2016). It can be used to estimate the glycaemic index of foods (Englyst, Vinoy, Englyst, & Lang, 2003; Goñi, Garcia-Alonso, & Saura-Calixto, 1997; Granfeldt, Bjorck, Drews, & Tovar, 1992) and to evaluate the fractions of starch that are rapidly digested (i.e. hydrolysed within 20 min), slowly digested (i.e. hydrolysed within 120 min) and not digested after the 120 min time (Englyst, Kingman, Hudson, & Cummings, 1996) (see also chapter “Influence of physical and structural aspects of food on starch digestion”).
3.1.2 Dynamic In vitro Digestion Models
The importance of the dynamic nature of digestion has been indicated long before dynamic in vitro models gained popularity (Lea, 1890). Compared to static models, dynamic models offer the potential to replicate complex digestive actions, and they are therefore preferred in studying phenomena such as the effect of fluid dynamics on digestibility. They are, however, typically more laborious and time-consuming. Like static, they may reproduce one or more sections of the digestive process (for an introduction to dynamic digestion models see also Thuenemann, 2015). Examples of dynamic in vitro models are shown in Table 2 (with references).
Oral processing signals the beginning of digestion and it causes changes such as mechanical breakdown, lubrication through mixing with saliva, bolus formation, as well as initiation of enzymatic hydrolysis through the enzymes present in the saliva (see also chapter “Influence of physical and structural aspects of food on starch digestion”). Oral processing in vitro has been simulated using commercial meat mincer (Bornhorst & Singh, 2013), commercial/laboratory blender (An, Bae, Han, Lee, & Lee, 2016; Bordoloi, Singh, & Kaur, 2012; Dhital et al., 2015; Tamura, Okazaki, Kumagai, & Ogawa, 2017), or sophisticated mouth models (Benjamin et al., 2012; Mielle et al., 2010; Panouillé, Saint-Eve, Déléris, Le Bleis, & Souchon, 2014; Salles et al., 2007). For a review of dynamic oral processing models see Peyron and Woda (2016) and Morell, Hernando, and Fiszman (2014). In vitro dynamic oral processing models typically incorporate a mechanical element of oral digestion and measure food breakdown and/or release of volatile compounds. As the mouth is also the organ where organoleptic characteristics of food are sensed, models have been developed to study texture and taste perception. For example, there are models that measure dynamic release of tastants such as salt (de Loubens et al., 2011; Mills et al., 2011), while addition of a microphone in the artificial mouth chamber has been reported, with the aim to gather acoustic information during eating. Analytical techniques, such as texture analysis or tribology, are further used to evaluate texture perception (van Aken, Vingerhoeds, & de Hoog, 2007; Vardhanabhuti, Cox, Norton, & Foegeding, 2011).
Gastric dynamic in vitro models typically incorporate a mechanical action (e.g. motility, mixing, and mechanical forces) by various techniques such as squeezing of the simulated gastric walls or relative motion between surfaces (see Table 2). They may or may not control flow rates of digesta and digestive secretions. These models typically study mechanical and/or enzymatic breakdown of the food bolus and have also been used to produce chyme that is then characterised using analytical techniques.
The chyme then passes to the small intestine, which is the site where most of the absorption occurs. Models that simulate intestinal wall motility (e.g. segmentation and peristaltic contractions) have been developed (examples shown in Table 2) and used to characterise chyme breakdown, bioaccessibility, and nutrient absorption rates. Absorption rates in these models are typically assessed by measuring the concentration of nutrients that pass through a semipermeable membrane simulating the intestinal walls. The semipermeable membrane acts as a sieve, which allows small molecules (products of digestion) to pass through the pores but retains large, undigested molecules in the luminal side. Like gastric, intestinal models may or may not incorporate fluid flow control.
In vitro models developed to study large intestinal digestion typically also consider the previous stages of digestion (oral, gastric, and small intestinal). Example models are the Spanish computer-controlled multicompartmental dynamic model of the gastrointestinal system (SIMGI) (Barroso, Cueva, Peláez, Martínez-Cuesta, & Requena, 2015) and the Belgian simulator of the human intestinal microbial ecosystem (SHIME) (Van de Wiele, Van den Abbeele, Ossieur, Possemiers, & Marzorati, 2015) used to study fermentation processes in the colon (see Table 2).
Multicompartmental digestive models to study combined digestive processes have been developed (examples shown in Table 2). The TNO’s TIM1 (gastric and small intestinal digestion) and TIM2 (large intestinal digestion) are commercially available (for details see chapter “Influence of physical and structural aspects of food on starch digestion”).
3.2 What Is Being Measured?
Typically, in vitro digestion models determine breakdown and digestibility of food materials. Measurements that determine mechanical breakdown, hydrolysis of macronutrients, release of compounds, and bioaccessibility of nutrients are often selected to quantify digestion. However, other analytical methods have been combined with in vitro digestive systems, including in situ scattering techniques such as small-angle X-ray scattering (SAXS) or neutron scattering, nuclear magnetic resonance, mass spectrometry, and techniques studying the effect of interfacial features on digestion. These have been reviewed (Marze, 2017) and will not be extensively regarded in this chapter.
3.3 In Vitro Studies: An Application-Specific Methodology
It is important to keep in mind that in vitro models are application specific. Overall, the large number of in vitro models developed in the last decades indicate the challenges involved in replicating digestive processes outside the body. The continuing efforts to understand digestion in vitro are expected to increase in the forthcoming years, in line with the efforts to reduce the need of extensive in vivo studies. However, due to the complexity of the physiological processes that are involved in digestion, it is important to understand the limitations of each in vitro model. Model selection and implementation of acquired data should therefore be treated with care (Bidlack et al., 2009).
4 In Silico Methods
Simulating digestion using numerical/computational methods can provide insight to the processes involved and mechanistic understanding of the digestion steps. In silico models may further be used as predictive tools in digestion, for example to estimate digestibility or gastric emptying, by extrapolating existing data within the model’s boundaries.
This section provides an overview of the current state of in silico modelling of the human digestive system. It will primarily focus on the gastric and small intestinal regions of the gastrointestinal tract. It will further focus on how the formulation of a meal and the body’s physiological responses can influence the gastric emptying and ultimately the nutrient absorption profile of a consumed food.
4.1 The Stomach
The stomach serves a variety of purposes when a meal has been consumed, these can be broken into four categories (Barrett, 2005):
-
Breakdown of solid food particles through the contractions of the gastric wall.
-
Breakdown of food chemically via the action of enzymatic hydrolysis.
-
Act as a reservoir to store food prior to further processing.
-
Control the rate at which food is emptied to the duodenum through contractions of the pyloric sphincter.
4.1.1 Gastric Emptying
Most models for the gastric emptying of meals fit experimental data to empirical models to try and characterise the emptying, and express it in simple terms such as the half time (t1/2), which is the time for half of the original meal content to have been emptied from the stomach. The simplest model for gastric emptying is the exponential emptying curve, expressed mathematically as the following ODE (Hellström, Grybäck, & Jacobsson, 2006):
where V is the volume of meal remaining in the stomach, t is the time since consumption, and γ is the rate of gastric emptying, which can be expressed as the half time:
By setting the initial conditions, that is, volume consumed at time zero (V0), Eq. (1) can be analytically solved:
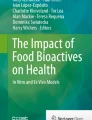
The emptying curve produced by Eq. (1) is shown in Fig. 2 over a normalised time period. The emptying begins at a faster rate, but slows as time progresses and the overall volume of the meal remaining in the stomach is reduced. We can therefore link the gastric emptying to the volume of meal in the stomach, which has been viewed in vivo by a number of authors (Brener, Hendrix, & McHugh, 1983; McHugh, 1983; McHugh & Moran, 1979).

Exponential emptying plot from the stomach, highlighting the time at which half the gastric content is emptied
This type of emptying pattern is generally seen with liquid meals, but solid meals, which require breakdown prior to emptying, usually show a lag phase (a period with low rate of emptying before a faster rate initiates). For these cases, other empirical approaches have been taken. The first requires an additional factor k, which is defined as a shape factor (Kong & Singh, 2008a; Siegel et al., 1988):
Another alternative is the delayed sigmoidal model (Eq. 5) utilised to describe the emptying of solids (Kong & Singh, 2009), where k is used here to describe the lag phase. The curves for Eqs. (4) and (5) are shown in Fig. 3.

Equation (4) (Siegel model) shows an initial lag phase, common when looking at the emptying of the solid portion of a meal (Hellström et al., 2006; Kong & Singh, 2008a). The half time of emptying for Eq. (4) is expressed by Eq. (6) (Kong & Singh, 2008a).
The delayed sigmoidal model (Eq. 5) allows for the effect of secretions upon the stomach to be considered. Meals with high-viscosity liquids (Marciani et al., 2000) or high solid content (Kong & Singh, 2009), will stimulate higher gastric secretion rates. This may be due to increased stimulation of stretch receptors in the stomach (Marciani et al., 2000). Due to these secretions the curve initially increases, with extra volume in the stomach compared to the initial meal volume. After processing [disintegration of solid particles or reduction in viscosity of high-viscosity meals (Marciani et al., 2000)] the emptying begins in a similar pattern to other models, faster initially but slowing down as the fraction of meal remaining in the stomach is reduced.
The empirical models developed do not provide any predictive ability, but allow for in vivo data to be classified. However, one aim of producing mathematical models is to allow for predictions of how a meal will behave postprandially, and as such allow for more efficient design of meals that will have certain desirable traits.
Dalla Man, Camilleri, and Cobelli (2006) assumed that the stomach could be described as two compartments. The first accounts for the solid portion of the meal, containing mass Msto1, the second accounts for the liquid portion of the meal of mass Msto2, and this is the portion which can empty (Dalla Man et al., 2006).
Equations (7)–(9) describe how the mass of both compartments changes with time (t), the input of initial meal is into the first compartment, with an initial mass D, where δ(t) is the dirac delta function (this will give an input at t = 0). The movement from compartment 1 to compartment 2 will be controlled by the rate constant k12, which can be thought of as a grinding term from the solid portion of the meal. The emptying from the second compartment will be at rate kempt; this rate was linked to the remaining mass in the stomach and the initial mass (D) via the following equation:
Equation (10) introduces a number of parameters that require estimates. kmin and kmax are the minimum and maximum rates of emptying, respectively. Parameters b and c are fractions of a meal in the stomach, b being the fraction at which the rate is at –(kmax − kmin)/2 and c when the rate is at (kmax − kmin)/2. The additional parameters are defined as follows:
Equations (10)–(12) are used with the parameters defined in Dalla Man et al. (2006) to give the plots of the fraction of meal remaining in the stomach postprandially. Results are shown in Fig. 4a, b, where the gastric contents after consumption of an Oral Glucose Tolerance Test (OGTT, comprising a drink with 75 g of dissolved glucose, Fig. 4a) and a meal (containing 45% carbohydrates, 15% protein, and 40% fats in a predominately solid form, with a low-nutrient liquid portion also included, Fig. 4b) are plotted against time postprandially. Figure 4a shows that the OGTT meal empties initially quickly, followed by a slower linear emptying. This is expected for liquid meals containing nutrients, where initial rapid emptying is followed by a controlled rate of emptying due to the feedback mechanism observed in vivo (Brener et al., 1983; Calbet & MacLean, 1997; McHugh, 1983). However, Fig. 4b shows that the mixed meal behaves slightly differently. One would expect a long initial lag period before emptying begins, as the solid portion of the meal undergoes size reduction in the stomach, to ensure particles are below the 1–2 mm diameter threshold (Kong & Singh, 2008a) before they can pass through the pyloric sphincter and exit the stomach to the proximal small intestine. It appears that the plot of gastric content tracks both the liquid and solid fraction of the meal, with the liquid portion emptying independently of the solid portion (Marciani et al., 2012). As a result, there is an initial rapid emptying rate of the low-nutrient liquid. This is higher than the initial emptying rate of the high-nutrient OGTT liquid, reflecting the feedback mechanism that controls emptying nutrients to the small intestine. When a large portion of the liquid has emptied, and the solid has been reduced in particle size sufficiently to pass through the pylorus, a much slower emptying rate of the solid meal is observed. Figure 4c, d refer to the intestinal phase of digestion and will be discussed in Sect. 4.2.

Plot of Dalla Man et al. (2006) model (Dalla Man et al., 2006), the top two plots show the fraction of a meal remaining in the stomach postprandial for a Oral Glucose Tolerance Test (OGTT) and for a model meal, under these plots are the corresponding plots of rate of glucose appearance in the plasma [adapted from Dalla Man et al. (Marteau et al., 1997)]
4.1.2 Gastric Secretions
When modelling the gastric secretions one can either study the total gastric secretions in relation to the consumption of a meal (Marciani et al., 2001; Sauter et al., 2012), or take a more intricate approach and analyse the secretions on a cellular level (Joseph, Zavros, Merchant, & Kirschner, 2003; Marino, Ganguli, Joseph, & Kirschner, 2003). Only the first approach will be presented here. This generally involves linking in vivo measurements and empirical models developed to describe the change in volume in the stomach with the gastric emptying and secretions. Marciani et al. (2000, 2001) have studied in vivo the effect of gastric viscosity upon the secretion rate. Low and high-viscosity meals with low or high nutrient content were administered to volunteers and the postprandial gastric volume was measured (Marciani et al., 2001). A model that links the secretion rates to the volume of meal and a basal secretion rate, described by Eqs. (13) and (14), was compared with experimental data.
where V is the volume at time t, of secretions (s) or meal (m), k is the secretion rate, p is the gastric emptying rate and S0 the basal rate of secretions.
This model provided results similar to the experimental measurements when the parameters were fitted, but it does not take into account the effect of viscosity on the secretion and emptying nor other factors of the meal properties. The viscosity was shown to have a major influence upon the rate of secretions when the same group was fed with non-nutrient meals of varying viscosities (Marciani et al., 2000). The secretions, on the other end, reduced the gastric viscosity to manageable levels over short periods of time (a meal of viscosity 11 Pa s was reduced to 0.3 Pa s over 40 min).
Sauter et al. (2012) proposed two approaches to modelling. The first is similar to that of Marciani et al.; however, Sauter et al. assumed that the secretions were not affected by the meal and they were a function of the maximum secretion volume. The second model linked the meal and secretion volumes, giving two coupled ODEs (Eqs. 15 and 16):
where V is the volume of secretion (s) or meal (m), k is the rate of emptying, kms is a rate constant representing the effect that the meal has upon the secretion rate, and ksm is a rate constant representing the effect that the secretions have upon delaying the gastric emptying. The authors further proposed a dimensionless term effm (=kms/(k+kms)), which represents the efficiency of a meal at stimulating secretions, taking a number between 0 and 1.
This model was fitted to experimental data for a high-nutrient viscous meal (chocolate drink). It was found that the secreted volume over the 120 min of measurement was around 48–74% of the original meal volume, and that in this case the rate constant kms was around 2.3 times larger than the rate constant ksm, indicating that the viscous meal influenced the secretion of gastric fluids to a greater extent than the gastric secretions inhibited the gastric emptying rate.
Moxon et al. (2017) linked the gastric secretion rate to the viscosity of the gastric chyme, taking into account that the secretions also had the effect of reducing the viscosity of the chyme. The secretion rate (Ksec) was defined as follows (Eq. 17):
where μ is the viscosity of the gastric chyme, Sb is the basal secretion rate, and λS and b are constants linking the rate of secretion to the viscosity. The viscosity was defined as a function of the concentration of a thickening agent; for the experimental data used in the paper Locust Bean Gum (LBG) was utilised as the thickening agent, and the following (Eq. 18) relationship was found:
where CLBG is the concentration of the LBG in the stomach.
Three ODEs were then defined (Eq. 19–21), one for the mass of nutrient in the stomach, one for the mass of non-nutrient liquid in the stomach, and one for the mass of thickener in the stomach:
Thus, the total mass in the stomach was defined as in Eq. (22):
The simulated results for a 11 Pa.s viscosity meal containing no nutrients are shown in Fig. 5. The simulated results were fitted to experimental data (Marciani et al., 2000), and highlight how large reduction in the chyme viscosity can be achieved through gastric secretions. It is anticipated that this will have a major impact on the mass transfer of nutrients in the intestine and influence the absorption rate of nutrients, which has been highlighted in-silico and during in vitro experimentation (Gouseti et al., 2014; Moxon et al., 2017; Moxon, Gouseti, & Bakalis, 2016).

4.2 The Small Intestine
Numerous authors have described the mass transfer and absorption of nutrients and/or drug compounds from the small intestine mathematically. The underlying assumption is that the mammalian digestive system can be described as a series of ideal reactor systems (Penry & Jumars, 1986; Penry & Jumars, 1987). Building upon this assumption, three types of systems are generally utilised to describe the small intestine: a single continuous stirred tank reactor (CSTR) (Dalla Man et al., 2006; Di Muria, Lamberti, & Titomanlio, 2010), multiple CSTRs in series (Bastianelli, Sauvant, & Rérat, 1996; Jumars, 2000; Yu & Amidon, 1999; Yu, Crison, & Amidon, 1996), or a plug flow reactor (PFR) (Logan, Joern, & Wolesensky, 2002; Ni, Ho, Fox, Leuenberger, & Higuchi, 1980; Stoll, Batycky, Leipold, Milstein, & Edwards, 2000). Figure 6 shows the different intestinal schematics for each set-up. Some of the models produced look only at the transit and absorption of nutrients in the small intestine (Logan et al., 2002), while others couple the model with gastric emptying (Dalla Man et al., 2006; Moxon et al., 2016), or with the nutrient/drug dynamics in the body after absorption (Dalla Man et al., 2006; Stoll et al., 2000; Yu & Amidon, 1999), or look at the whole digestive system from consumption to excretion (Bastianelli et al., 1996).

Schematic of different reactor designs used to describe the small intestine. (a) is a single CSTR design, (b) multiple CSTRs in series, (c) is a PFR set-up
One of the simplest models for the small intestine was utilised by Dalla Man et al. (2006). It was assumed that the small intestine can be described as a single CSTR , with absorption being modelled as a first order reaction term, giving the following Eq. (23) (Dalla Man et al., 2006):
where mSI is the mass of meal in the small intestine, kabs is the absorption rate, and Gempt is the rate of gastric emptying [calculated from Eqs. (5)–(12)]. Rather than validating the intestinal model against blood glucose data, the authors considered a novel technique to quantify the rate of glucose appearance in the plasma near the gut, utilising multiple tracer compounds (Dalla Man et al., 2005). The rate of appearance of glucose in the plasma (Ra) was defined as the absorption rate multiplied by a scaling factor, f, which is a fraction of the total mass of a meal nutrient that will be absorbed. This factor was set to 0.89 in the current model.
The curves for two meals (oral glucose tolerance test, OGGT, and solid meal) are shown below the corresponding gastric content curves in Fig. 4. The rate of appearance of glucose after the consumption of a OGTT meal shows an initial high peak before dropping to a lower rate, which can be explained by the initial rapid emptying period of the model followed by a more linear, slower emptying. The mixed meal showed a different response. After an initial peak there is a major drop followed by a lower rate of absorption that is steadily dropping over a period of around 4 h. Overall, Dala Man et al.’s models gave a good fit to the averages of the rate of appearances and the measurements for each individual, though they require a large number of parameters to be estimated, and they are not able to describe the intestinal transit time well due to the use of a single CSTR assumption for gastric digestion, as highlighted in the work by Yu et al. (1996).
Di Muria et al. (2010) chose to use one compartment to describe the small intestine in a whole body model for the absorption of zinc sulphate in rats. Along with the single intestinal compartment, six other compartments were defined to describe the distribution of the drug in the body: the stomach, large intestine, gastrointestinal circulatory system, liver, plasma, and tissue. In this model, the change in drug concentration in the small intestine was described as in Eq. (25):
where ASIL is the mass of drug in the small intestine, the first term on the right handside, \( S\frac{\partial r}{\partial t} \), describes the dissolution of the drug in the small intestine, JSIL describes the mass transfer between the small intestine and the gastrointestinal circulatory system, and the final term describes the elimination of the drug from the small intestine. The mass transfer between the small intestine and the circulatory system was further defined using a first order mass transfer equation (Eq. 26) with a concentration driving force:
where ka is the rate of absorption, VB is the volume of the bolus containing the drug in the intestinal tract, CGICS is the concentration of the drug in the gastrointestinal circulatory system, and RGICS is the drug partition coefficient. The formulation of equations for other compartments is not discussed here but can be found in Di Muria et al. (2010).
This model provides a good fit with experimental data, with only five parameters requiring estimation and an additional determination of the variable r (in Eq. 25) to describe the dissolution of the drug compound in the stomach, small intestine, and large intestine. Information to determine r in this model requires in vitro data [however, some methods for modelling the dissolution of drug compounds are discussed by Sugano (2009)]. Di Muria et al. (2010) applied their model to the drug Diltiazem from results on human oral consumption. Two parameters needed to be estimated from the in vivo data, the elimination of the drug from the plasma, and the distribution volume of the drug in the plasma. Three different formulations were utilised, these provided slow, medium, and high release rates for the diltiazem compound. The models described the general profile of drug concentration in the blood plasma, but underestimated the peak in both fast and slow release formulations, and overestimated the clearance from the circulatory system during the terminal phase of the profile.
Yu et al. (1996) analysed how the different types of reactor systems used to describe the small intestine affect the transit time, assuming that a drug does not degrade or get absorbed. For continuous stirred tank reactors, the Eq. (27) was used to describe the percentage of drug in each compartment:
The amount of drug leaving the small intestine was described as in Eq. (28):
where τ = Ktt, and Kt is the transit rate constant.
For the PFR assumption, a diffusion–convection equation (29) was further used:
where C is the concentration at a point z along the intestine and at time t, α is the diffusion coefficient, and ν is the axial velocity along the length of the small intestine.
These models were used to calculate the mean transit time along the small intestine, and compared to experimental data for the rate of appearance in the colon. The experimental data showed a mean small intestinal transit time of 199 min and a 95% confidence interval of 7 min, with a minimum transit time of 30 min and a maximum of 570 min, while the gathered data showed neither a Gaussian nor a lognormal distribution (Yu et al., 1996). The single compartment model showed a poor fit to the experimental distribution, with a SSE (sum of squared error) of 3542, much higher than the multiple compartment approach or the PFR approach.
For the multicompartment approach, the total number of compartments was varied to analyse the effect. Five, seven, and nine compartment models were simulated giving SSE of 79, 8, and 52, respectively. The seven compartment model gave the best fit, with the authors (Yu et al., 1996) rationalising this physiologically by stating that the first compartment represents the duodenum and proximal jejunum, the second and third compartment represent the mid jejunum and distal jejunum, respectively, and the rest of the compartments represent the ileum. Fitting the diffusion coefficient, the PFR was found to have a SSE of 20, giving a better fit to the experimental data than the single, five, and nine compartment models, but slightly worse than the seven-compartment model. The author chose the multicompartment model approach as the best when describing the intestinal transit, due to (1) the large reduction in SSE between the multicompartment and single compartment model, and (2) the fact that the multicompartment approach is simpler mathematically than the PFR model, though it should be noted that the work was published in 1996 and the complexity around solving the PDEs for the PFR model has since been reduced by the increased speed of modern computation.
According to the approach by Bastianelli et al. (1996) the small intestine is considered as two compartments [smaller than the recommended seven mentioned in the previous paragraph (Yu et al., 1996)] that are linked with one compartment for the stomach and another for the large intestine, giving a total of four compartments. All four compartments have an input of endogenous secretions, the three intestinal compartments have an additional output representing the absorption of nutrients, and the large intestinal compartment has a further additional output to represent faeces elimination. The model looks at all components of a meal given to a pig. The components in the initial feed are protein, starch, sugars, digestible cell wall, lipids, and minerals. These are hydrolysed to absorbable compounds in the different compartments (e.g. starch to sugars, and proteins to amino acids), and these absorbable compounds are absorbed via Michaelis–Menten kinetics.
Results of this model were compared to experimental data for the absorption rate of glucose, amino acids, and volatile fatty acids. The simulation underestimated the absorption rate of all three nutrients, and greater underestimation was seen with amino acids and fatty acids. The authors highlighted the need for advanced in vitro models to better understand the digestibility of a meal, so that parameters could be predicted more accurately (such as kinetics of the nutrients being absorbed). It is noted that since the publication a number of methodologies have been identified to study the in vitro digestion of food and elucidate some of these processes and parameter values, though the detailed understanding and in vitro representation of digestive processes is still not complete (see previous section). They also pointed out the added benefits of utilising a PFR style model for the intestine, which allows for the effects of viscosity and peristaltic propulsion and mixing to be included. There have been studies by later authors (Moxon et al., 2016; Taghipoor, Barles, Georgelin, Licois, & Lescoat, 2014; Taghipoor, Lescoat, Licois, Georgelin, & Barles, 2012) to look at the effect of viscosity or peristaltic waves upon absorption, but the effect of local mixing (due to segmentation waves) has not been included into models looking at absorption, though have been studied from a fluid mechanic perspective (Ferrua & Singh, 2011; Kozu et al., 2010; Love, Lentle, Asvarujanon, Hemar, & Stafford, 2012), to understand the mixing effect the gastric and intestinal wall contraction can have.
Yu and Amidon (1999) built on previous work from the group (Yu et al., 1996) by using the seven compartmental approach developed in the 1996 paper and adding two more compartments to represent the stomach and colon to look at the passage and absorption of drugs after oral consumption. It was assumed that the drug emptied exponentially from the stomach to the first intestinal compartment, and that the passage from one intestinal compartment to the next and the absorption from each compartment were both via first order kinetics (Yu & Amidon, 1999). Thus, the following Eqs. (30–32) were presented (compared to Eqs.19–21):
where m is the mass in the different compartments, and subscripts s is the stomach, c is the colon, and n is the small intestine; ka is the absorption rate, kt is the transfer rate between compartments, and ks is the emptying rate from the stomach. The rate of absorption was taken as the effective permeability and data from literature was gathered for multiple drug compounds. To fit the simulated data to that of concentrations gathered from in vivo data, a model for the distribution of drug concentration in the plasma, which included one central compartment and two peripheral compartments, was taken from literature (Mason, Winer, Kochak, Cohen, & Bell, 1979).
The models gave good fit to experimental data, using an exponential as well as a biphasic emptying rate from the stomach. The biphasic emptying gave the best fit, though it resulted in around 77% of the drug fraction being emptied in the first phase of emptying, followed by a 2-h period in which no emptying occurred, before the rest of the drug emptied. As pointed out by the authors, this is something that it is unlikely to occur in vivo (Yu & Amidon, 1999).
A model developed by Moxon et al. (2016) linked the absorption rate to the viscosity of the intestinal chyme. The model assumed the intestine could be described as a plug flow reactor and used an advection–reaction equation to describe how the mass of nutrient varied along the length of the intestine (Eqs. 33):
where mSI is the mass in the small intestine, which varies with distance along the length z (∈[0, L], where L is the total length of the intestine), and with time t. γmstom represents the rate of emptying from the stomach into the intestine, which occurs at a distance l0 along the intestine (l0 is the radius of a bolus entering), and \( \overline{u} \) is the velocity of the intestinal content along the length of the intestine. An exponential equation was assumed for the gastric content, as defined in Eq. (1). The final term (\( \frac{2f}{r_m}K{m}_{\mathrm{SI}}\Big) \) describes the absorption of the nutrients, where f is the increase in surface area due to protrusions (e.g. villi and microvilli), 2/rm represents the surface area to volume ratio of the intestine, and K is the absorption rate constant. K was further linked to the convective mass transfer coefficient of the intestinal chyme, through the relationship between Sherwood, Schmidt, and Reynolds numbers, which gave the following definition (Eq. 34) of the mass transfer coefficient (Moxon et al., 2016):
where D is the diffusivity of the nutrient calculated from the Einstein–Stokes equation, and d is the diameter of the intestine.
Two dimensionless terms, the characteristic time of mass transfer, τtransfer, and the characteristic time of gastric emptying, τempty, were defined (Eqs. 35 and 36) (Moxon et al., 2016):
In the Plot in Fig. 7, showing the relationship between the two dimensionless characteristic times, two regions are identified. The bottom region (below the black diagonal line) is controlled mainly by the emptying rate, where increasing the characteristic emptying time results in an increase in absorption of nutrients, but changes in the mass transfer rate do not have a major effect. In the top region (above the black diagonal line), the limiting factor is the mass transfer rate, and changes in gastric emptying rate do not seem to have a large effect.

Contour plot highlighting the effect of characteristic emptying time and characteristic mass transfer time upon the absorption of glucose over a 3-h period, adapted from Moxon et al. (2016)
In reality, the two factors are likely to be linked. Work by numerous authors (Brener et al., 1983; Calbet & MacLean, 1997; McHugh, 1983) has shown a nutrient based feedback mechanism that links the bioaccessibility of nutrients within the proximal small intestine to the gastric emptying rate. As such, high characteristic mass transfer rates would likely have the effect of slowing down the gastric emptying rate, thus reducing the amount of glucose in the intestine and maintaining a lower absorption rate of nutrients.
This was approached in Moxon et al. (2017), where the gastric emptying rate was linked to the bioaccessibility of the nutrients in the small intestine, through an on/off type feedback control system, as expressed in Eq. (37):
where γ is the gastric emptying rate, γ0 is the initial gastric emptying rate, and the rate is zero if the bioaccessibility is greater than a maximum value (Amax). The bioaccessibility can be defined from Eq. (38), where it will be equal to the reactive term of the equations.
This gave good fits to experimental data for both high- and low-viscosity liquid meals with high- and low-nutrient content (Fig. 8), when the parameters K, Amax, and γ0 were fit. It can be seen that for the low-nutrient meals there is little difference in the emptying rate between low- and high-viscosity meals, as confirmed by other in vivo experiments (Marciani et al., 2000). However, this is not the case of the high-nutrient meals. Here, there is a longer period of initial rapid emptying for the high-viscosity meal, compared to the low-viscosity one, prior to the initiation of the feedback mechanism. This can be attributed to the lower bioaccessibility of the nutrients in the high-viscosity meal, allowing for longer emptying times before any nutrients are detected in the small intestine signalling feedback for reduction in the gastric emptying rates.

This highlights the importance of the link between the mass transfer in the intestinal lumen and the gastric emptying rate. An additional complexity refers to the fact that the viscosity is not constant as previously demonstrated, and it will vary due to gastric and intestinal secretions. The mass transfer in the intestinal lumen will therefore vary over time and along the length of the intestine. This mass transfer will be influenced not only by the viscosity of the chyme, but also the intestinal wall contractions, something that has not been modelled so far when looking into the absorption of nutrients in silico. These contractions are expected to play a role by increasing the mass transfer rates, as demonstrated during in vitro experiments (Gouseti et al., 2014; Tharakan et al., 2010).
5 Conclusions
Studying digestive processes is challenging and research in this area is currently very active. The broad aspects of digestion, including the nature of the diet and the physiology of eating, pose fascinating questions that are yet to be understood before a complete, detailed understanding is achieved. Significant progress has been attained by studying digestion using in vivo, in vitro, and in silico approaches and this has led to improved dietary options and enhanced individual and public health. However, each methodology has its advantages and limitations that need to be taken into account when selecting an appropriate research approach and also when interpreting any acquired data. As this field of research is currently evolving, it is important to reflect on existing methodologies collectively and form the future of digestion studies according to the needs and gaps in the current practice.
References
Aguilera, J. M. (2005). Why food microstructure? Journal of Food Engineering, 67, 3–11.
Al-Gousous, J., & Langguth, P. (2015). Oral solid dosage form disintegration testing—The forgotten test. Journal of Pharmaceutical Sciences, 104, 2664–2675.
An, J. S., Bae, I. Y., Han, S.-I., Lee, S.-J., & Lee, H. G. (2016). In vitro potential of phenolic phytochemicals from black rice on starch digestibility and rheological behaviors. Journal of Cereal Science, 70, 214–220.
Bach Knudsen, K. E., Lærke, H. N., Steenfeldt, S., Hedemann, M. S., & Jørgensen, H. (2006). In vivo methods to study the digestion of starch in pigs and poultry. Animal Feed Science and Technology, 130, 114–135.
Ban, C., Jo, M., Lim, S., & Choi, Y. L. (2018). Control of the gastrointestinal digestion of solid lipid nanoparticles using PEGylated emulsifiers. Food Chemistry, 239, 442–452.
Barrett, K. E., Boitano, S., Barman, S. M., & Brooks, H. L. (2005). Gastrointestinal physiology. In K. E. Barrett (Ed.), Ganong’s review of medical physiology. New York: McGraw-Hill.
Barroso, E., Cueva, C., Peláez, C., Martínez-Cuesta, M. C., & Requena, T. (2015). The computer-controlled multicompartmental dynamic model of the gastrointestinal system SIMGI. The impact of food bioactives on health: In vitro and ex vivo models. New York: Springer. https://doi.org/10.1007/978-3-319-16104-4_28
Bastianelli, D., Sauvant, D., & Rérat, A. (1996). Mathematical modeling of digestion and nutrient absorption in pigs. Journal of Animal Science, 74, 1873–1887.
Bellmann, S., Lelieveld, J., Gorissen, T., Minekus, M., & Havenaar, R. (2016). Development of an advanced in vitro model of the stomach and its evaluation versus human gastric physiology. Food Research International, 88, 191–198.
Benjamin, O., Silcock, P., Kieser, J. A., Waddell, J. N., Swain, M. V., & Everett, D. W. (2012). Development of a model mouth containing an artificial tongue to measure the release of volatile compounds. Innovative Food Science and Emerging Technologies, 15, 96–103.
Bidlack, W. R., Birt, D., Borzelleca, J., Clemens, R., Coutrelis, N., Coughlin, J. R., et al. (2009). Expert report: Making decisions about the risks of chemicals in foods with limited scientific information. Comprehensive Reviews in Food Science and Food Safety, 8, 269–303.
Blanquet, S., Marol-Bonnin, S., Beyssac, E., Pompon, D., Renaud, M., & Alric, M. (2001). The ‘biodrug’ concept: An innovative approach to therapy. Trends in Biotechnology, 19, 393–400.
Boccia, S. (2015). Credibility of observational studies: Why public health researchers should care? European Journal of Public Health, 25, 554–555.
Bohn, T., Carriere, F., Day, L., Deglaire, A., Egger, L., Freitas, D., et al. (2017). Correlation between in vitro and in vivo data on food digestion. What can we predict with static in vitro digestion models? Critical Reviews in Food Science and Nutrition, 1–23. https://doi.org/10.1080/10408398.2017.1315362
Bongaerts, J. H. H., Rossetti, D., & Stokes, J. R. (2007). The lubricating properties of human whole saliva. Tribology Letters, 27, 277–287.
Bordoloi, A., Singh, J., & Kaur, L. (2012). In vitro digestibility of starch in cooked potatoes as affected by guar gum: Microstructural and rheological characteristics. Food Chemistry, 133, 1206–1213.
Bornhorst, G. M., Gouseti, O., Wickham, M. S. J., & Bakalis, S. (2016). Engineering digestion: Multiscale processes of food digestion. Journal of Food Science, 81, R534–R543.
Bornhorst, G. M., Roman, M. J., Dreschler, K. C., & Singh, R. P. (2013). Physical property changes in raw and roasted almonds during gastric digestion in vivo and in vitro. Food Biophysics, 9, 39–48.
Bornhorst, G. M., & Singh, R. P. (2013). Kinetics of in vitro bread bolus digestion with varying oral and gastric digestion parameters. Food Biophysics, 8, 50–59.
Brahma, S., Weier, S. A., & Rose, D. J. (2016). Effects of selected extrusion parameters on physicochemical properties and in vitro starch digestibility and β-glucan extractability of whole grain oats. Journal of Cereal Science, 70, 85–90.
Bratten, J., & Jones, M. P. (2009). Prolonged recording of duodenal acid exposure in patients with functional dyspepsia and controls using a radiotelemetry pH monitoring system. Journal of Clinical Gastroenterology, 43, 527–533.
Brener, W., Hendrix, T. R., & McHugh, P. R. (1983). Regulation of the gastric emptying of glucose. Gastroenterology, 85, 76–82.
Brown, R., & Ogden, J. (2004). Children’s eating attitudes and behaviour: A study of the modelling and control theories of parental influence. Health Education Research, 19, 261–271.
Calbet, J. A., & MacLean, D. A. (1997). Role of caloric content on gastric emptying in humans. The Journal of Physiology, 498, 553–559.
Carlson, M. D. A., & Morrison, R. S. (2009). Study design, precision, and validity in observational studies. Journal of Palliative Medicine, 12, 77–82.
Carneiro, I., & Howard, N. (2011). Introduction to epidemiology. Maidenhead: Open University Press.
Carscaddon, L. Literature reviews: Types of clinical study designs. GSU Library Research Guides.
Chen, J., Gaikwad, V., Holmes, M., Murray, B., Povey, M., Wang, Y., et al. (2011). Development of a simple model device for in vitro gastric digestion investigation. Food & Function, 2, 174–182.
Chen, L., Tian, Y., Zhang, Z., Tong, Q., Sun, B., Rashed, M. M. A., et al. (2017). Effect of pullulan on the digestible, crystalline and morphological characteristics of rice starch. Food Hydrocolloids, 63, 383–390.
Chen, L., Xu, Y., Fan, T., Liao, Z., Wu, P., Wu, X., et al. (2016). Gastric emptying and morphology of a ‘near real’ in vitro human stomach model (RD-IV-HSM). Journal of Food Engineering, 183(1–8).
Chessa, S., Huatan, H., Levina, M., Mehta, R. Y., Ferrizzi, D., Rajabi-Siahboomi, A. R., et al. (2014). Application of the dynamic gastric model to evaluate the effect of food on the drug release characteristics of a hydrophilic matrix formulation. International Journal of Pharmaceutics, 466, 359–367.
Cozzini, P. (2015). From medicinal chemistry to food science: A transfer of in silico methods applications. New York: Nova.
Dalla Man, C., Camilleri, M., & Cobelli, C. (2006). A system model of oral glucose absorption: Validation on gold standard data. IEEE Transactions on Biomedical Engineering, 53, 2472–2478.
Dalla Man, C., Yarasheski, K. E., Caumo, A., Robertson, H., Toffolo, G., Polonsky, K. S., et al. (2005). Insulin sensitivity by oral glucose minimal models: Validation against clamp. American Journal of Physiology. Endocrinology and Metabolism, 289, E954–E959.
Darragh, A. J., & Hodgkinson, S. M. (2000). Quantifying the digestibility of dietary protein. The Journal of Nutrition, 130, 1850S–1856S.
Darragh, A. J., & Moughan, P. J. (1995). The three-week-old piglet as a model animal for studying protein digestion in human infants. Journal of Pediatric Gastroenterology and Nutrition, 21, 387–393.
de Loubens, C., Panouillé, M., Saint-Eve, A., Déléris, I., Tréléa, I. C., & Souchon, I. (2011). Mechanistic model of in vitro salt release from model dairy gels based on standardized breakdown test simulating mastication. Journal of Food Engineering, 105, 161–168.
de Wijk, R. A., Janssen, A. M., & Prinz, J. F. (2011). Oral movements and the perception of semi-solid foods. Physiology and Behavior, 104, 423–428.
Deeks, J. J., Dinnes, J., D’Amico, R., Sowden, A. J., Sakarovitch, C., Song, F., et al. (2003). Evaluating non-randomised intervention studies. Health Technology Assessment, 7, iii–iix.
Deferme, S., Annaert, P., & Augustijns, P. (2008). Vitro screening models to assess intestinal drug absorption and metabolism. In C. Ehrhardt & K. J. Kim (Eds.), Drug absorption studies (pp. 182–215). Boston, MA: Springer. https://doi.org/10.1007/978-0-387-74901-3_8
Deglaire, A., & Moughan, P. J. (2012). Animal models for determining amino acid digestibility in humans – A review. The British Journal of Nutrition, 108, S273–S281.
Dhital, S., Dabit, L., Zhang, B., Flanagan, B., & Shrestha, A. K. (2015). In vitro digestibility and physicochemical properties of milled rice. Food Chemistry, 172, 757–765.
Di Muria, M., Lamberti, G., & Titomanlio, G. (2010). Physiologically based pharmacokinetics: A simple, all purpose model. Industrial and Engineering Chemistry Research, 49, 2969–2978.
Donaldson, B., Rush, E., Young, O., & Winger, R. (2014). Variation in gastric pH may determine kiwifruit’s effect on functional GI disorder: An in vitro study. Nutrients, 6, 1488–1500.
Dupont, D., & Mackie, A. R. (2015). Static and dynamic in vitro digestion models to study protein stability in the gastrointestinal tract. Drug Discovery Today: Disease Models, 17–18, 23–27.
Egger, L., Ménard, O., Delgado-Andrade, C., Alvito, P., Assunção, R., Balance, S., et al. (2016). The harmonized INFOGEST in vitro digestion method: From knowledge to action. Food Research International, 88, 217–225.
Englyst, H. N., Kingman, S. M., & Cummings, J. H. (1992). Classification and measurement of nutritionally important starch fractions. European Journal of Clinical Nutrition, 46(Suppl 2), S33–S50.
Englyst, H. N., Kingman, S. M., Hudson, G. J., & Cummings, J. H. (1996). Measurement of resistant starch in vitro and in vivo. The British Journal of Nutrition, 75, 749.
Englyst, H. N., Veenstra, J., & Hudson, G. J. (2007). Measurement of rapidly available glucose (RAG) in plant foods: A potential in vitro predictor of the glycaemic response. The British Journal of Nutrition, 75, 327.
Englyst, K. N., Vinoy, S., Englyst, H. N., & Lang, V. (2003). Glycaemic index of cereal products explained by their content of rapidly and slowly available glucose. The British Journal of Nutrition, 89, 329.
Farmer, A. D., Scott, S. M., & Hobson, A. R. (2013). Gastrointestinal motility revisited: The wireless motility capsule. United European Gastroenterology Journal, 1, 413–421.
Ferrua, M. J., & Singh, R. P. (2011). Understanding the fluid dynamics of gastric digestion using computational modeling. Procedia Food Science, 1, 1465–1472.
Gidley, M. J. (2013). Hydrocolloids in the digestive tract and related health implications. Current Opinion in Colloid and Interface Science, 18, 371–378.
Goñi, I., Garcia-Alonso, A., & Saura-Calixto, F. (1997). A starch hydrolysis procedure to estimate glycemic index. Nutrition Research, 17, 427–437.
Gouseti, O., Jaime-Fonseca, M. R., Fryer, P. J., Mills, C., Wickham, M. S. J., & Bakalis, S. (2014). Hydrocolloids in human digestion: Dynamic in-vitro assessment of the effect of food formulation on mass transfer. Food Hydrocolloids, 42, 378–385.
Granfeldt, Y., Bjorck, I., Drews, A., Tovar, J. (1992). An in vitro procedure based on chewing to predict metabolic response to starch in cereal and legume products. European Journal of Clinical Nutrition, 46, 649–660.
Grimes, D. A., & Schulz, K. F. (2002). An overview of clinical research: The lay of the land. Lancet, 359, 57–61.
Hajat C. (2011) An Introduction to Epidemiology. In: Teare M. (ed), Genetic Epidemiology. Methods in Molecular Biology (Methods and Protocols), vol 713. Humana Press, Totowa, NJ
Hellström, P. M., Grybäck, P., & Jacobsson, H. (2006). The physiology of gastric emptying. Best Practice & Research. Clinical Anaesthesiology, 20, 397–407.
Hoffmann, K., Schulze, M. B., Schienkiewitz, A., Nöthlings, U., & Boeing, H. (2004). Application of a new statistical method to derive dietary patterns in nutritional epidemiology. American Journal of Epidemiology, 159, 935–944.
Home Office, Department for Business Innovation & Skills, Department of Health, (2014). Working to reduce the use of animals in scientific research. Crown Copyright. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/277942/bis-14-589-working-to-reduce-the-use-of_animals-in-research.pdf
Hsu, R. J. C., Chen, H. J., Lu, S., & Chiang, W. (2015). Effects of cooking, retrogradation and drying on starch digestibility in instant rice making. Journal of Cereal Science, 65, 154–161.
Hu, F. B. (2002). Dietary pattern analysis: A new direction in nutritional epidemiology. Current Opinion Lipidology, 13(1), 3–9.
Hur, S. J., Lim, B. O., Decker, E. A., & McClements, D. J. (2011). In vitro human digestion models for food applications. Food Chemistry, 125, 1–12.
Jenkins, D. J., Wolever, T. M., Leeds, A. R., Gassull, M. A., Haisman, P., Dilawari, J., et al. (1978). Dietary fibres, fibre analogues, and glucose tolerance: Importance of viscosity. British Medical Journal, 1, 1392–1394.
Joseph, I. M. P., Zavros, Y., Merchant, J. L., & Kirschner, D. (2003). A model for integrative study of human gastric acid secretion. Journal of Applied Physiology, 94, 1602–1618.
Jumars, P. A. (2000). Animal guts as nonideal chemical reactors: Partial mixing and axial variation in absorption kinetics. The American Naturalist, 155, 544–555.
Kahan, B. C., Rehal, S., & Cro, S. (2015). Risk of selection bias in randomised trials. Trials, 16(405).
Kong, F., & Singh, R. P. (2008a). Disintegration of solid foods in human stomach. Journal of Food Science, 73, R67–R80.
Kong, F., & Singh, R. P. (2008b). A model stomach system to investigate disintegration kinetics of solid foods during gastric digestion. Journal of Food Science, 73, E202–E210.
Kong, F., & Singh, R. P. (2009). Modes of disintegration of solid foods in simulated gastric environment. Food Biophysics, 4, 180–190.
Kozu, H., Kobayashi, I., Neves, M. A., Nakajima, M., Uemura, K., Sato, S., et al. (2010). Analysis of flow phenomena in gastric contents induced by human gastric peristalsis using CFD. Food Biophysics, 5, 330–336.
Krul, C., Luiten-Schuite, A., Baandagger, R., Verhagen, H., Mohn, G., Feron, V., et al. (2000). Application of a dynamic in vitro gastrointestinal tract model to study the availability of food mutagens, using heterocyclic aromatic amines as model compounds. Food and Chemical Toxicology, 38, 783–792.
Last, J. M., & International Epidemiological Association. (2001). A dictionary of epidemiology. New York: Oxford University Press.
Le Ferrec, E., Chesne, C., Artusson, P., Brayden, D., Fabre, G., & Gires, P. (2001). In vitro models of the intestinal barrier. ATLA, 29, 649–668.
Lea, A. S. (1890). A comparative study of artificial and natural digestions. The Journal of Physiology, 11, 226–263.
Lefebvre, D. E., Venema, K., Gombau, L., Valerio Jr., L. G., Raju, J., Bondy, G. S., et al. (2015). Utility of models of the gastrointestinal tract for assessment of the digestion and absorption of engineered nanomaterials released from food matrices. Nanotoxicology, 9, 523–542.
Lo Curto, A., Pitino, I., Mandalari, G., Dainty, J. R., Faulks, R. M., John Wickham, M. S., et al. (2011). Survival of probiotic lactobacilli in the upper gastrointestinal tract using an in vitro gastric model of digestion. Food Microbiology, 28, 1359–1366.
Logan, J. D., Joern, A., & Wolesensky, W. (2002). Location, time, and temperature dependence of digestion in simple animal tracts. Journal of Theoretical Biology, 216, 5–18.
Love, R. J., Lentle, R. G., Asvarujanon, P., Hemar, Y., & Stafford, K. J. (2012). An expanded finite element model of the intestinal mixing of digesta. Food Digestion, 4, 26–35.
Lvova, L., Denis, S., Barra, A., Mielle, P., Salles, C., Vergoignan, C., et al. (2012). Salt release monitoring with specific sensors in ‘in vitro’ oral and digestive environments from soft cheeses. Talanta, 97, 171–180.
Mackie, A. R., Bajka, B. H., Rigby, N. M., Wilde, P. J., Alves-Pereira, F., Mosleth, E. F., et al. (2017). Oatmeal particle size alters glycemic index but not as a function of gastric emptying rate. American Journal of Physiology. Gastrointestinal and Liver Physiology, 313, G239–G246.
Mackie, A., Rigby, N., Macierzanka, A. & Bajka, B. (2015). Approaches to static digestion models. In The impact of food bioactives on health (pp. 23–31). Cham: Springer International Publishing. https://doi.org/10.1007/978-3-319-16104-4_3
Mainville, I., Arcand, Y., & Farnworth, E. R. (2005). A dynamic model that simulates the human upper gastrointestinal tract for the study of probiotics. International Journal of Food Microbiology, 99, 287–296.
Maldonado-Valderrama, J., Terriza, J. A. H., Torcello-Gómez, A., & Cabrerizo-Vílchez, M. A. (2013). In vitro digestion of interfacial protein structures. Soft Matter, 9, 1043.
Marciani, L., Gowland, P. A., Spiller, R. C., Manoj, P., Moore, R. J., Young, P., et al. (2000). Gastric response to increased meal viscosity assessed by echo-planar magnetic resonance imaging in humans. The Journal of Nutrition, 130, 122–127.
Marciani, L., Gowland, P. A., Spiller, R. C., Manoj, P., Moore, R. J., Young, P., et al. (2001). Effect of meal viscosity and nutrients on satiety, intragastric dilution, and emptying assessed by MRI. American Journal of Physiology. Gastrointestinal and Liver Physiology, 280, G1227–G1233.
Marciani, L., Hall, N., Pritchard, S. E., Cox, E. F., Totman, J. J., Lad, M., et al. (2012). Preventing gastric sieving by blending a solid/water meal enhances satiation in healthy humans. The Journal of Nutrition, 142, 1253–1258.
Marino, S., Ganguli, S., Joseph, I. M. P., & Kirschner, D. E. (2003). The importance of an inter-compartmental delay in a model for human gastric acid secretion. Bulletin of Mathematical Biology, 65, 963–990.
Marteau, P., Minekus, M., Havenaar, R., & Huis in’t Veld, J. H. (1997). Survival of lactic acid bacteria in a dynamic model of the stomach and small intestine: Validation and the effects of bile. Journal of Dairy Science, 80, 1031–1037.
Marze, S. (2017). Bioavailability of nutrients and micronutrients: Advances in modeling and in vitro approaches. Annual Review of Food Science and Technology, 8, 35–55.
Mason, W. D., Winer, N., Kochak, G., Cohen, I., & Bell, R. (1979). Kinetics and absolute bioavailability of atenolol. Clinical Pharmacology and Therapeutics, 25.
McAllister, M. (2010). Dynamic dissolution: A step closer to predictive dissolution testing? Molecular Pharmaceutics, 7, 1374–1387.
McClements, D. J. (2007). Understanding and controlling the microstructure of complex foods. Boca Raton, FL: CRC Press.
McClements, D. J., & Li, Y. (2010). Review of in vitro digestion models for rapid screening of emulsion-based systems. Food & Function, 1, 32–59.
McClements, D. J., Li, F., & Xiao, H. (2015). The nutraceutical bioavailability classification scheme: Classifying nutraceuticals according to factors limiting their oral bioavailability. Annual Review of Food Science and Technology, 6, 299–327.
McHugh, P. R. (1983). The control of gastric emptying. Journal of the Autonomic Nervous System, 9, 221–231.
McHugh, P. R., & Moran, T. H. (1979). Calories and gastric emptying: A regulatory capacity with implications for feeding. The American Journal of Physiology, 236, R254–R260.
Ménard, O., Cattenoz, T., Guillemin, H., Souchon, I., Deglaire, A., Dupont, D., et al. (2014). Validation of a new in vitro dynamic system to simulate infant digestion. Food Chemistry, 145, 1039–1045.
Mercuri, A., Lo Curto, A., Wickham, M. S. J., Craig, D. Q. M., & Barker, S. A. (2008). Dynamic gastric model (DGM): a novel in vitro apparatus to assess the impact of gastric digestion on the droplet size of self-emulsifying drug-delivery systems. Journal of Pharmacy and Pharmacology, 60, 4.
Meullenet, J.-F., & Gandhapuneni, R. K. (2006). Development of the BITE Master II and its application to the study of cheese hardness. Physiology and Behavior, 89, 39–43.
Mielle, P., Tarrega, A., Sémon, E., Maratray, J., Gorria, P., Liodenot, J. J., et al. (2010). From human to artificial mouth, from basics to results. Sensors and Actuators B: Chemical, 146, 440–445.
Mills, C.E.N., Marsh, J.T., Johnson, P.E., Boyle, R.,Hoffmann-Sommerguber, K., Dupont, D., Bartra, J., Bakalis, S., McLaughlin, J., Shewry, P.R. (2013). Literature review: ‘in vitro digestibility tests for allergenicity assessment’. EFSA supporting publications, 10(12), EN-529.
Mills, T., Spyropoulos, F., Norton, I. T., & Bakalis, S. (2011). Development of an in-vitro mouth model to quantify salt release from gels. Food Hydrocolloids, 25, 107–113.
Minekus, M., Alminger, M., Alvito, P., Ballance, S., Bohn, T., Bourlieu, C., et al. (2014). A standardised static in vitro digestion method suitable for food – An international consensus. Food and Function, 5, 1113–1124.
Minekus, M., Marteau, P., Havenaar, R., & Huis in’t Veld, J. H. J. (1995). A multicompartmental dynamic computer-controlled model simulating the stomach and small intestine. ATLA, Alternatives to Laboratory Animals, 23, 197–209.
Minekus, M., Smeets-Peeters, M., Bernalier, A., Marol-Bonnin, S., Havenaar, R., Marteau, P., et al. (1999). A computer-controlled system to simulate conditions of the large intestine with peristaltic mixing, water absorption and absorption of fermentation products. Applied Microbiology and Biotechnology, 53, 108–114.
Misra, S. (2012). Randomized double blind placebo control studies, the ‘Gold Standard’ in intervention based studies. Indian Journal of Sexually Transmitted Diseases and AIDS, 33, 131.
Moosavian, S. P., Haghighatdoost, F., Surkan, P. J., & Azadbakht, L. (2017). Salt and obesity: A systematic review and meta-analysis of observational studies. International Journal of Food Sciences and Nutrition, 68, 265–277.
Morell, P., Hernando, I., & Fiszman, S. M. (2014). Understanding the relevance of in-mouth food processing. A review of in vitro techniques. Trends in Food Science and Technology, 35, 18–31.
Motilva, M.-J., Serra, A., & Rubió, L. (2015). Nutrikinetic studies of food bioactive compounds: From in vitro to in vivo approaches. International Journal of Food Sciences and Nutrition, 66, S41–S52.
Moxon, T. E., Gouseti, O., & Bakalis, S. (2016). In silico modelling of mass transfer & absorption in the human gut. Journal of Food Engineering, 176, 110–120.
Moxon, T. E., Nimmegeers, P., Telen, D., Fryer, P. J., Van Impe, J., Bakalisa, S., et al. (2017). Effect of chyme viscosity & nutrient feedback mechanism on gastric emptying. Chemical Engineering Science, 171, 318–330.
Mun, S., & McClements, D. J. (2017). Influence of simulated in-mouth processing (size reduction and alpha-amylase addition) on lipid digestion and β-carotene bioaccessibility in starch-based filled hydrogels. LWT-Food Science and Technology, 80, 113–120.
Ni, P. F., Ho, N. F. H., Fox, J. L., Leuenberger, H., & Higuchi, W. I. (1980). Theoretical model studies of intestinal drug absorption V. Non-steady-state fluid flow and absorption. International Journal of Pharmaceutics, 5, 33–47.
Panouillé, M., Saint-Eve, A., Déléris, I., Le Bleis, F., & Souchon, I. (2014). Oral processing and bolus properties drive the dynamics of salty and texture perceptions of bread. Food Research International, 62, 238–246.
Penry, D. L., & Jumars, P. A. (1986). Chemical reactor analysis and optimal digestion. Bioscience, 36, 310–315.
Penry, D. L., & Jumars, P. A. (1987). Modeling animal guts as chemical reactors. The American Naturalist, 129, 69.
Peyron, M.-A., & Woda, A. (2016). An update about artificial mastication. Current Opinion in Food Science, 9, 21–28.
Qin, D., Yang, X., Gao, S., Yao, J., & McClements, D. J. (2016). Influence of hydrocolloids (dietary fibers) on lipid digestion of protein-stabilized emulsions: Comparison of neutral, anionic, and cationic polysaccharides. Journal of Food Science, 81, C1636–C1645.
Ronda, F., Rivero, P., Caballero, P. A., & Quilez, J. (2012). High insoluble fibre content increases in vitro starch digestibility in partially baked breads. International Journal of Food Sciences and Nutrition, 63, 971–977.
Salles, C., Tarrega, A., Mielle, P., Maratray, J., Gorria, P., Liaboeuf, J., et al. (2007). Development of a chewing simulator for food breakdown and the analysis of in vitro flavor compound release in a mouth environment. Journal of Food Engineering, 82, 189–198.
Salvia-Trujillo, L., Qian, C., Martín-Belloso, O., & McClements, D. J. (2013). Influence of particle size on lipid digestion and β-carotene bioaccessibility in emulsions and nanoemulsions. Food Chemistry, 141, 1475–1480.
Sauter, M., Curcic, J., Menne, D., Goetze, O., Fried, M., Schwizer, W., et al. (2012). Measuring the interaction of meal and gastric secretion: A combined quantitative magnetic resonance imaging and pharmacokinetic modeling approach. Neurogastroenterology and Motility, 24, 632–e273.
Schwizer, W., Steingötter, A., Fox, M., Zur, T., Thumshirn, M., Bösiger, P., et al. (2002). Non-invasive measurement of gastric accommodation in humans. Gut, 51(Suppl 1), i59–i62.
Siegel, J. A., Urbain, J. L., Adler, L. P., Charkes, N. D., Maurer, A. H., Krevsky, B., et al. (1988). Biphasic nature of gastric emptying. Gut, 29, 85–89.
Slavin, J. (2013). Fiber and prebiotics: Mechanisms and health benefits. Nutrients, 5, 1417–1435.
Stamatopoulos, K., Batchelor, H. K., & Simmons, M. J. H. (2016). Dissolution profile of theophylline modified release tablets, using a biorelevant Dynamic Colon Model (DCM). European Journal of Pharmaceutics and Biopharmaceutics, 108, 9–17.
Stoll, B. R., Batycky, R. P., Leipold, H. R., Milstein, S., & Edwards, D. A. (2000). A theory of molecular absorption from the small intestine. Chemical Engineering Science, 55, 473–489.
Sugano, K. (2009). Introduction to computational oral absorption simulation. Expert Opinion on Drug Metabolism and Toxicology, 5, 259–293.
Sutton, G. (2003). Putrid gums and ‘Dead Men’s Cloaths’: James Lind aboard the Salisbury. Journal of the Royal Society of Medicine, 96, 605–608.
Taghipoor, M., Barles, G., Georgelin, C., Licois, J.-R., & Lescoat, P. (2014). Digestion modelling in the small intestine: Impact of dietary fibre. Mathematical Biosciences, 258, 101–112.
Taghipoor, M., Lescoat, P., Licois, J. R., Georgelin, C., & Barles, G. (2012). Mathematical modeling of transport and degradation of feedstuffs in the small intestine. Journal of Theoretical Biology, 294, 114–121.
Tamura, M., Okazaki, Y., Kumagai, C., & Ogawa, Y. (2017). The importance of an oral digestion step in evaluating simulated in vitro digestibility of starch from cooked rice grain. Food Research International, 94, 6–12.
Tharakan, A., Norton, I. T., Fryer, P. J., & Bakalis, S. (2010). Mass transfer and nutrient absorption in a simulated model of small intestine. Journal of Food Science, 75, E339–E346.
Thiese, M. S. (2014). Observational and interventional study design types; an overview. Biochemia Medica, 24, 199–210.
Thomas, K., Aalbers, M., Bannon, G. A., Bartels, M., Dearman, R. J., Esdaile, D. J., et al. (2004). A multi-laboratory evaluation of a common in vitro pepsin digestion assay protocol used in assessing the safety of novel proteins. Regulatory Toxicology and Pharmacology, 39, 87–98.
Thuenemann, E. C. (2015). Dynamic digestion models: general introduction. In: Verhoeckx, K., Cotter, P., López-Expósito, I., Kleiveland, C., Lea, T., Mackie, A., Requena, T., Swiatecka, D., Wichers, H. (eds), The impact of food bioactives on health, in-vitroand ex-vivomodels. Springer, USA.
Timmreck, T. C. (2002). An introduction to epidemiology. Sudbury, MA: Jones and Bartlett Publishers.
van Aken, G. A., Vingerhoeds, M. H., & de Hoog, E. H. A. (2007). Food colloids under oral conditions. Current Opinion in Colloid & Interface Science, 12, 251–262.
Van de Wiele, T., Van den Abbeele, P., Ossieur, W., Possemiers, S., & Marzorati, M. (2015). The simulator of the human intestinal microbial ecosystem (SHIME®). In K. Verhoeckx, P. Cotter, I. López-Expósito, C. Kleiveland, T. Lea, A. Mackie, et al. (Eds.), The impact of food bioactives on health (pp. 305–317). Cham: Springer International Publishing. https://doi.org/10.1007/978-3-319-16104-4_27
Van Hung, P., Lam, N., Thi, N., & Phi, L. (2016). Resistant starch improvement of rice starches under a combination of acid and heat-moisture treatments. Food Chemistry, 191, 67–73.
Vardhanabhuti, B., Cox, P. W., Norton, I. T., & Foegeding, E. A. (2011). Lubricating properties of human whole saliva as affected by β-lactoglobulin. Food Hydrocolloids, 25, 1499–1506.
Vist, G. E., & Maughan, R. J. (1995). The effect of osmolality and carbohydrate content on the rate of gastric emptying of liquids in man. The Journal of Physiology, 486, 523–531.
Wickham, M., Faulks, R., & Mills, C. (2009). In vitro digestion methods for assessing the effect of food structure on allergen breakdown. Molecular Nutrition & Food Research, 53, 952–958.
Willett, W. (1987). Nutritional epidemiology: Issues and challenges. International Journal of Epidemiology, 16, 312–317.
Willett, W. (2013). Nutritional epidemiology. New York: Oxford University Press.
Wilson, T., & Temple, N. J. (2001). Nutritional health: Strategies for disease prevention. Totowa, NJ: Humana Press.
Woolnough, J. W., Bird, A. R., Monro, J. A., & Brennan, C. S. (2010). The effect of a brief salivary α-amylase exposure during chewing on subsequent in vitro starch digestion curve profiles. International Journal of Molecular Sciences, 11, 2780–2790.
Wright, N. D., Kong, F., Williams, B. S., & Fortner, L. (2016). A human duodenum model (HDM) to study transport and digestion of intestinal contents. Journal of Food Engineering, 171, 129–136.
Xu, W. L., Lewis, D., Bronlund, J. E., & Morgenstern, M. P. (2008). Mechanism, design and motion control of a linkage chewing device for food evaluation. Mechanism and Machine Theory, 43, 376–389.
Yu, L. X., & Amidon, G. L. (1999). A compartmental absorption and transit model for estimating oral drug absorption. International Journal of Pharmaceutics, 186, 119–125.
Yu, L. X., Crison, J. R., & Amidon, G. L. (1996). Compartmental transit and dispersion model analysis of small intestinal transit flow in humans. International Journal of Pharmaceutics, 140, 111–118.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Muttakin, S., Moxon, T.E., Gouseti, O. (2019). In vivo, In vitro, and In silico Studies of the GI Tract. In: Gouseti, O., Bornhorst, G., Bakalis, S., Mackie, A. (eds) Interdisciplinary Approaches to Food Digestion. Springer, Cham. https://doi.org/10.1007/978-3-030-03901-1_3
Download citation
DOI: https://doi.org/10.1007/978-3-030-03901-1_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-03900-4
Online ISBN: 978-3-030-03901-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)