
Abstract
This cross-sectional study focused on the association between heart rate variability (HRV) and early repolarization pattern (ERP). It included 1236 patients categorized into three groups: ERP type 1: J-point elevation with notched/slurred QRS; ERP type 2: ST elevation without dominant J-wave; and non-ERP group. Analyzing time-domain indexes include standard deviation of NN (normal-to-normal) RR intervals (SDNN), root mean square of successive difference in NN RR intervals (RMSSD), and proportion of consecutive NN intervals that differ by more than 50 ms (PNN50), there were significant differences between any two groups (all P < 0.01). All time-domain indexes showed: ERP type 2 > ERP type 1 > non-ERP. Multivariate logistic regression analysis revealed that SDNN at nighttime and gender were independently associated with the maximum magnitude of J-point elevation ≧ 0.2 mV. The findings strongly suggested that based on electrocardiogram characteristics, parasympathetic tone denoted by HRV may be related to different types of ERP.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Early repolarization pattern (ERP) is described as J-point elevation or QRS notching or slurring on the standard 12-lead electrocardiogram (ECG). It is present in between 2.3 and 13.1% of the overall population in the world. Among them, athletes and adolescents have a higher incidence of ERP [1,2,3,4]. Previously, early repolarization was considered as a normal ECG variation. However, recent studies have shown that early repolarization is associated with arrhythmia deaths in the general population [1, 2, 5, 6]. A previous study conducted by our group revealed that the risk of arrhythmia deaths in ERP patients increased (RR 1.7, 95% CI 1.19–2.42) when adjusted with confounding factors [7]. A recent study also showed that early repolarization is associated with a significant increased risk of ventricular arrhythmias and sudden cardiac death in patients with structural heart diseases [8].
However, the pathophysiologic basis of ERP is currently not fully understood. Though research have showed that the J-point of early repolarization rises significantly during bradycardia [9,10,11], the relationship between early repolarization and parasympathetic tone remains unclear. The study therefore aimed to evaluate the possible associations between autonomic influence and ERP in individuals without structural heart disease.
The most frequently used and non-invasive method in evaluating autonomic effects is heart rate variability (HRV) analysis. HRV is an index of the influence of the sympathetic and parasympathetic systems of the heart [12, 13]. Herein, the role of autonomic influences related to early repolarization were evaluated by HRV.
Materials and Methods
Study Population
A cross-sectional study design was employed in this study. Data collection was performed prospectively. We screened all patients (N = 7624) who were referred to the First Affiliated Hospital of Sun Yat-Sen University for 24-h Holter recording between January 4, 2018 and February 28, 2019. All the patients underwent 24-h Holter recording for evaluation of chest pain, palpitations, dizziness, unexplained syncope, and other symptoms as well as preoperative risk assessment of non-heart surgeries. The study population was selected based on the following criteria: Patients aged between 18 and 60 years with no structural heart disease and whose recording time of Holter was more than 22 h and with a sinus rhythm as the dominant rhythm were included in the study. Patients diagnosed with hyperthyroidism, hypothyroidism, acute cerebrovascular accident, limited activity caused by various reasons, systemic diseases or Wolff-Parkinson-White syndrome were excluded from the study. Pregnant patients and those who had taken drugs affecting autonomic nerves or antiarrhythmic drugs within 1 month before examination, those with QRS wave width more than 110 ms, and those with a history of pacemaker implantation were also excluded. Finally, 1236 patients remained to proceed with the study. The presence of an existing structural heart disease was examined using either an electrocardiogram (ECG), or an echocardiography, or a coronary angiography. General clinical data and history of heart disease, hypertension, diabetes, smoking status, medication history, and examination results of the patients were obtained through questionnaires and electronic medical record system.
Categorization of Early Repolarization
Currently, there is no unified definition of early repolarization. Based on the American Heart Association criterion set in 2015 [14], early repolarization was categorized into two subtypes: ERP type 1 and ERP type 2 (Fig. 1). ERP type 1 referred to early repolarization in modern definition. The elevation of the J-point of two adjacent lateral or inferior leads ≥ 0.1 mV with either slurring or notching morphology regardless of the change of ST segment. ERP type 2 referred to ST segment elevation ≥ 0.1 mV without a significant J-wave. ST segment elevation is generally multilead or full lead. ERP type 2 patients had ST segment elevation of the leads whose S wave at the end of QRS wave was more significant than that of the R wave. All patients underwent 12-lead resting ECG followed by 12-channel Holter recording. Changes consistent with those of ERP type 1 and ERP type 2 that appeared in either or both ECG and Holter recording were regarded as early repolarization. All the 1236 patients were then further categorized into three groups: ERP type 1, ERP type 2, and non-ERP group based on their ECG characteristics. In the same line, patients who showed early repolarization were further categorized into two groups based on the time of the early repolarization. One group was named “all-day group” because it showed early repolarization both in the day and at night. The other group was named “nighttime group” because it only showed early repolarization when the heart rate slowed down at night.

Subtype of early repolarization pattern (ERP). a ERP type 1: ERP with notching morphology. b ERP type 1: ERP with slurring morphology. c ERP type 2
Twenty-Four-Hour Holter Recording
Twelve-channel recorders were used for all patients. All recordings were performed using the Biomedical Instruments Co., Ltd. Holter system by a trained cardiologist. Patients with recording durations less than 22 h, and those with artifacts exceeding 10% were excluded. Those with non-sinus dominant rhythms such as paroxysmal or persistent atrial flutter/atrial fibrillation, persistent atrial tachycardia, and non-transient atrioventricular block of second degree or more were also excluded.
HRV Analysis
Heart rate variability analysis was done using the Holter system. This included time-domain analysis and frequency-domain analysis. The parameters estimated were as follows: (1) SDNN—the standard deviation of NN (normal-to-normal) RR intervals, (2) RMSSD—the root mean square of successive difference in NN RR intervals; (3) PNN50—the proportion of consecutive NN intervals that differ by more than 50 ms; (4) LF—low frequency; and (5) HF—high frequency. The LF/HF ratio was then calculated and recorded above indexes in the whole day and daytime/nighttime, respectively. Daytime was defined as between 07:00 and 23:00 h while nighttime was between 23:00 and 07:00 h the next day. These time intervals were based on the living habits of the local people.
Other Variables
Premature ventricular complexes were carefully checked; the total number and nighttime number were counted. Non-sustained ventricular tachycardia was defined as that which lasted for 30 s or less. None of the patients was found to have sustained ventricular tachycardia.
Statistical Analysis
All variables were tested for normality first. Continuous variables with a normal distribution were expressed as means with standard deviation while those with a skewed distribution were expressed using their median and their 25% and 75% quartiles. The Kruskal-Wallis test was used to compare the clinical characteristics and heart rate variabilities of patients in the ERP type 1, ERP type 2, and non-ERP group. Categorical variables were reported as frequencies and were compared using the chi-square test or Fisher exact test. In subgroup analysis, the HRV of all-day group and nighttime group was compared using the Student’s t test or Mann-Whitney U test. The effects of covariates on the maximum magnitude of J-point elevation ≧ 0.2 mV of the ERP type 1 during Holter recording were analyzed using multivariate logistic regression. SPSS version 22 software was used in statistical analysis. P values less than 0.05 (P < 0.05) indicated significant differences between groups.
Results
Patient Characteristics
This study included 1236 patients aged from 18 to 60 years old of whom 47% were males. Among the patients, 30.6% showed ERP type 1, 13.9% showed ERP type 2, and the remaining 55.5% had no ERP. Table 1 shows the clinical characteristic of the study population stratified based on their early repolarization status. As shown, patients with ERP (include ERP type 1 and ERP type 2) tend to be males. They also had a lower mean heart rate and minimum heart rate compared with those in the non-ERP group. ERP type 2 group patients were younger and had a lower body mass index (BMI) and higher maximum heart rate compared with those in the ERP type 1 group. No significant differences were found in the history of diabetes, proportion of smokers, and value of premature ventricular complexes both at night and during the entire day and night. The incidence of non-sustained ventricular tachycardia was higher in patients with early repolarization type 1 compared with those in the non-ERP group. However, the incidence was very low (3.2%) and the longest ventricular tachycardia was only made up of three wide malformation QRS waves. The prevalence of hypertension in the ERP type 2 group was lower than that of the non-ERP group. This may be attributed to the relatively younger age of patients in ERP type 2.
Comparison of HRV Between ERP Type 1, ERP Type 2, and Non-ERP Group
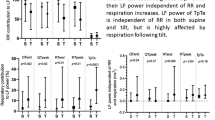
The heart rate variability values between ERP type 1, ERP type 2, and non-ERP groups were significantly different (Fig. 2). Time-domain indexes (SDNN, RMSSD, and PNN50) between any two groups were found to be significantly different (P < 0.01). All time-domain indexes showed the following: ERP type 2 > ERP type 1 > non-ERP. In frequency-domain analysis, the LF/HF ratio of ERP type 2 patients was significantly lower than that of the non-ERP patients (P = 0.009). However, there were no significant differences in the LF/HF ratio between ERP type 1 group and non-ERP group.

Comparison of heart rate variability (HRV) among ERP type 1, ERP type 2, and non-ERP groups
Daytime /Nighttime HRV Comparison in All-Day Group and Nighttime Group
Subgroup of daytime /nighttime HRV comparison in all-day group and nighttime group was analyzed to further verify the association between HRV parameters and ERP. In ERP type 2 analysis (Table 2), daytime HRV values of SDNN, RMSSD, PNN50, and HF indexes were significantly higher in the all-day group than those of the nighttime group (P < 0.05). However, there were no significant differences found in ERP type 1 analysis (Table 3).
Multivariate Analysis of Nighttime HRV with Maximum J-Point Elevation Amplitude ≥ 0.2 mV
SDNN, RMSSD, PNN50, and LF/HF ratios at nighttime were used to build different regression models to study the effects of covariates on the maximum magnitude of J-point elevation ≧ 0.2 mV during Holter recording in the ERP type 1 group. Nighttime parameters of HRV were chosen because the highest elevation of J-point often occurred at night. After adjusting for age, BMI, hypertension, diabetes, smoking status, mean heart rate, and maximum and minimum heart rates, multivariate logistic regression analysis revealed that higher SDNN at nighttime (odds ratio 1.025, 95% CI 1.009–1.040, P = 0.001) and male patients (odds ratio 4.172, 95% CI 1.016–17.125, P = 0.047) were independently associated with the maximum J-point elevation amplitude ≥ 0.2 mV of ERP type 1 during Holter recording (Table 4). No analyses were done for ERP type 2 group because of difficulties in locating a clear J-point.
Discussion
Previous epidemiological studies have reported that early repolarization occurs mostly in male and young patients. Herein, patients in the ERP type 2 group were relatively younger and had lower BMI compared with the ERP type 1 patients.
Based on electrocardiogram characteristics, parasympathetic tone denoted by HRV may be related to different types of ERP. Herein, the order of parasympathetic tension was ERP type 2, ERP type 1, and non-ERP group, respectively. In ERP type 2 group analysis, daytime HRV was higher in all-day group than in the nighttime group. This aspect strengthened the power of connection between parasympathetic tone and ERP. An increase in parasympathetic tone may be involved in the pathophysiological mechanism of early repolarization.
Currently, the pathophysiological basis of early repolarization is not entirely understood. Experimental studies by Antzelevitch C et al. (1991, 2011) and Badri M et al. (2015) showed that J-wave was formed by transmural voltage difference of 1 and 2 phases in action potential mediated by Ito current [15,16,17]. Though research has shown that the J-point of early repolarization rises significantly during bradycardia, the relationship between early repolarization and parasympathetic tone remains unclear. Shinohara T et al. (2017) pointed out that exaggerated reactivity of parasympathetic nerve was involved in ventricular fibrillation in J-wave syndrome though the number of cases included was small [18]. We speculate that the parasympathetic nerve could exhibit early repolarization by increasing the repolarization current of 1 and 2 phases of action potential or slowing inactivation of Ito current. However, this hypothesis needs to be further confirmed or disapproved.
Limitations and Future Directions
Although this study shows that increased parasympathetic tone is related to early repolarization, autonomic nerve tension is indirectly reflected by heart rate variability. Cognizant to this, the relationship between parasympathetic tone, repolarization currents, and early repolarization needs to be studied further. Herein, early repolarization patterns of individual cases were found to fluctuate between type 1 and type 2. Given that patients in the ERP type 2 group were relatively younger, whether they will change to ERP type 1 with increasing age needs further follow-up studies.
Conclusion
Based on electrocardiogram characteristics, parasympathetic tone denoted by HRV may be related to different types of ERP.
References
Tikkanen, J. T., Anttonen, O., Junttila, M. J., et al. (2009). Long-term outcome associated with early repolarization on electrocardiography [J]. N Engl J Med, 361(26), 2529–2537.
Olson, K. A., Viera, A. J., Soliman, E. Z., et al. (2011). Long-term prognosis associated with J-point elevation in a large middle-aged biracial cohort: the ARIC study [J]. Eur Heart J, 32(24), 3098–3106.
Sinner, M. F., Reinhard, W., Muller, M., et al. (2010). Association of early repolarization pattern on ECG with risk of cardiac and all-cause mortality: a population-based prospective cohort study (MONICA/KORA) [J]. PLoS Med, 7(7), e1000314.
Uberoi, A., Jain, N. A., Perez, M., et al. (2011). Early repolarization in an ambulatory clinical population [J]. Circulation, 124(20), 2208–2214.
Haruta, D., Matsuo, K., Tsuneto, A., et al. (2011). Incidence and prognostic value of early repolarization pattern in the 12-lead electrocardiogram [J]. Circulation, 123(25), 2931–2937.
Junttila, M. J., Tikkanen, J. T., Kentta, T., et al. (2014). Early repolarization as a predictor of arrhythmic and nonarrhythmic cardiac events in middle-aged subjects [J]. Heart Rhythm : the official journal of the Heart Rhythm Society, 11(10), 1701–1706.
Wu, S. H., Lin, X. X., Cheng, Y. J., et al. (2013). Early repolarization pattern and risk for arrhythmia death: a meta-analysis [J]. J Am Coll Cardiol, 61(6), 645–650.
Cheng, Y.-J., Li, Z.-Y., Yao, F.-J., et al. (2017). Early repolarization is associated with a significantly increased risk of ventricular arrhythmias and sudden cardiac death in patients with structural heart diseases [J]. Heart Rhythm : the official journal of the Heart Rhythm Society, 14(8), 1157–1164.
Rosso, R., Kogan, E., Belhassen, B., et al. (2008). J-point elevation in survivors of primary ventricular fibrillation and matched control subjects: incidence and clinical significance [J]. J Am Coll Cardiol, 52(15), 1231–1238.
Cappato, R., Furlanello, F., Giovinazzo, V., et al. (2010). J wave, QRS slurring, and ST elevation in athletes with cardiac arrest in the absence of heart disease: marker of risk or innocent bystander? [J]. Circ Arrhythm Electrophysiol, 3(4), 305–311.
Haïssaguerre, M., Derval, N., Sacher, F., et al. (2008). Sudden cardiac arrest associated with early repolarization [J]. N Engl J Med, 358(19), 2016–2023.
Levy, M. N. (1990). Autonomic interactions in cardiac control. Ann N Y Acad Sci, 601, 209–221.
Draghici, A. E., & Taylor, J. A. (2016). The physiological basis and measurement of heart rate variability in humans. J Physiol Anthropol, 35, 22.
Patton, K. K., Ellinor, P. T., Ezekowitz, M., et al. (2016). Electrocardiographic early repolarization [J]. Circulation, 133(15), 1520–1529.
Antzelevitch, C., Sicouri, S., Litovsky, S. H., et al. (1991). Heterogeneity within the ventricular wall. Electrophysiology and pharmacology of epicardial, endocardial, and M cells [J]. Circ Res, 69(6), 1427–1449.
Antzelevitch, C., & Yan, G. X. (2011). J-wave syndromes. From cell to bedside [J]. J Electrocardiol, 44(6), 656–661.
Badri, M., Patel, A., & Yan, G. X. (2015). Cellular and ionic basis of J-wave syndromes [J]. Trends Cardiovas Med, 25(1), 12–21.
Shinohara, T., Kondo, H., Otsubo, T., et al. (2017). Exaggerated reactivity of parasympathetic nerves is involved in ventricular fibrillation in J-wave syndrome [J]. J Cardiovasc Electrophysiol, 28(3), 321–326.
Funding
The study was financially supported by grants from the National Natural Science Foundation of China (Nos. 81370285 and 81970206), Guangdong Natural Science Foundation (2019A1515010269), and Guangzhou City Science and Technology key Program (No. 201508020057).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Human Subjects/Informed Consent Statement
This study was conducted with the consent of the ethics committee of the first affiliated hospital of Sun Yat-Sen University. It was conducted in accordance with the Helsinki Declaration of 1975 (revised in year 2000). The subjects of this study were 1236 patients treated in the first affiliated hospital of Sun Yat-Sen university between January 2018 and February 2019. All participants provided a written informed consent agreeing to participate in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Chen, XM., Fan, J., Cheng, YJ. et al. Autonomic Influences Related to Early Repolarization in Patients Without Structural Heart Disease. J. of Cardiovasc. Trans. Res. 13, 970–976 (2020). https://doi.org/10.1007/s12265-020-10033-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12265-020-10033-4