
Abstract
The use of digital radiographic systems has decreased the frequency of image retakes due to over/underexposure in general radiography. However, image retakes owing to patient positioning errors are likely to increase because of the convenience of a real-time image check on a console table. The purpose of the present study is to propose a novel radiographic examination procedure with an ultra-low-dose pre-test exposure that may be utilized to check patient positioning prior to taking an actual image, thereby reducing unnecessary patient exposure owing to image retakes. In this study, examination data from 714 knee joint radiographs, both submitted and retaken images, were included. Twelve radiological technologists (RTs) took all images. The actual total exposure dose for each patient was compared with simulated total doses utilized in the proposed procedure. The simulation assumed that each examination was completed following pre-test exposure. Therefore, this method did not involve retaking images although at least one pre-test exposure had been applied to all patients. Pre-test exposures at four dose levels corresponding to 25, 10, 5, and 2% of the actual exposure dose were evaluated to determine whether each dose level could be used to check patient positioning. The results indicated that when the pre-test exposure dose rate was 10% or lower, the total exposure dose reduction equaled or exceeded 8% for all patients. The use of the proposed procedure reduced the total exposure dose for all patients when compared to the exposure dose calculated from records.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
The use of digital radiographic systems allows for a reduction in patient dose (corresponding to 33–50% in chest radiography) [1, 2] by decreasing the number of image retakes owing to over/under exposure in general radiography. However, digitalization is likely to increase the number of radiographic examinations [3], and image retakes caused by patient positioning errors, because of the convenience of a real-time image check on the console table.
Optimization of the patient dose is important for radiologic technologists (RTs). General radiography adopts as minimum an exposure dose as is necessary for diagnosis. However, when image retakes occur, the total exposure dose corresponds to more than double the minimum exposure dose required for diagnosis. Although it is necessary to minimize the image retake rate, there are few unavoidable clinical situations with high image retake rates, including rare examinations that use a special radiography technique, nonstandard patients, and examinations performed by an inexperienced RT. Therefore, to decrease the number of image retakes, devices to assist with patient positioning were developed, and special training programs and workshops for inexperienced RTs were implemented.
The image retake rate decreases on changing the imaging system from analog (screen-film system) to digital [4,5,6]. Digital radiography reduces the number of errors related to over/underexposure. Nevertheless, in digital radiography, patient positioning errors lead to a number of image retakes [5].
In digital amorphous silicon flat-panel detector (FPD) radiography, an image is displayed immediately after exposure. Therefore, RTs can check patient positioning without moving the patient and promptly adjust it, if unacceptable. The present study involves development of a novel radiographic examination procedure using an ultra-low-dose pre-test exposure for checking patient positioning prior to taking the actual image, thereby reducing the total patient radiation dose. To clarify the validity of the proposed novel radiographic examination procedure, a total patient dose with and without the proposed procedure is simulated using the clinical examination data for knee joint radiography.
2 Materials and methods
2.1 Database of knee joint radiographic examinations
Clinical examination records of 714 patients with 1046 knee joint radiographs (ages 6–92 years, mean 63.6 years; M:F = 4:6) were used as the research database to compare the total patient dose in the proposed procedure with that in the conventional procedure. All cases included in the database involved examination of knee joint radiographs in the three views (anteroposterior, lateral, and skyline); moreover, some patients had both submitted as well as retaken images. Twelve RTs, from October 2012 to October 2013, were engaged in radiographic examinations. Beneo (Fujifilm Medical, Tokyo, Japan) equipped with a digital amorphous selenium FPD was the digital radiography system used in this database.
2.2 Novel radiographic examination procedure with ultra-low-dose pre-test exposure
The proposed novel radiographic examination procedure uses an ultra-low-dose pre-test exposure to confirm patient positioning prior to taking an actual image. It is necessary to control the pre-test exposure dose such that it is significantly lower than the dose used for taking the actual image. After taking a pre-test image, an RT checks the patient positioning displayed on the screen of the integrated digital radiography operator’s console while the patient maintains his/her posture. If the patient positioning is acceptable, the RT immediately takes the actual image. Alternatively, the RT immediately adjusts the positioning and takes the next pre-test image. The positioning and the pre-test exposure are repeatedly adjusted until there is no problem in positioning.
2.3 Relationship between image retake rate and pre-test exposure dose
The acceptable patient radiation dose for pre-test exposure is estimated by taking into consideration the image retake rate for specific radiographic examinations (i.e., knee joint radiography, scapula radiography, and temporomandibular joint radiography). It is essential for pre-test exposure dose to be lower than the exposure dose in conventional procedures, taking into account the specific image retake rate.
It is assumed that a single exposure dose in the conventional procedure corresponds to D 100. Thus, a single exposure dose for an image retake is also assumed to be D 100. If pre-test exposure is assumed to be reduced to α% of D 100, then a single pre-test exposure dose defined as D α = (α/100) × D 100. The numbers of actual exposures and image retakes correspond to X and R, respectively; the total exposure doses using the conventional procedure and pre-test exposure are estimated based on the following equations:
To ensure that Dptotal does not exceed Dctotal, the maximum percentage of the pre-test exposure α is estimated from Eqs. (1) and (2) as follows:
Dctotal > Dptotal and, therefore, this leads to the following expression:
From Eq. (3), the following expression is obtained:
The image retake rate β is defined as R/X; hence, R/(R + X), as shown in Eq. (4), can be expressed as β/(β + 1). Therefore, the pre-test exposure dose rate α% is permissible when its value is lower than that of β/(β + 1). In the present study, the maximum pre-test exposure dose rate α max is estimated taking into account the actual image retake rate as a criterion for evaluating reduction in dose rates.
2.4 Simulation of total exposure dose
The total exposure doses of the conventional method and the pre-test exposure method were simulated using examination records of three-directional knee joint radiographies of 1046 knees in 714 patients obtained by 12 RTs. In the simulated model, each examination (1046 × 3 = 3138 submitted images in total) was completed following a pre-test exposure with ultra-low doses to check patient positioning. The examination was completed without image retakes albeit with the addition of pre-test exposure. To simplify the estimation, exposure conditions including X-ray voltage, current, exposure time, and source-surface distance of all examinations were assumed to be the same.
When knee joint radiography was performed in the three planes and the pre-test exposure dose corresponded to 10% of the actual exposure dose, the total exposure doses of the conventional and pre-test methods corresponded to 3 × D 100 = 3D 100 and (3 × D 100) + (3 × 0.1D 100) = 3.3D 100, respectively. If it was necessary to retake the image in one of the three planes, the total exposure doses of the conventional method corresponded to (3 × D 100) + (1 × D 100) = 4D 100, whereas that of the pre-test exposure method corresponded to (3 × D 100) + (4 × 0.1D 100) = 3.4D 100.
To verify the proposed method, the total exposure dose in the conventional method, Dc, and the pre-test exposure method, Dp, was calculated by changing the level of pre-test exposure doses to 25, 10, 5, and 2% of the actual exposure dose.
2.5 Determination of pre-test exposure dose to check patient positioning
According to the proposed procedure, a pre-test image is taken with an ultra-low dose to confirm patient positioning. Therefore, it is necessary to determine the minimum pre-test exposure dose required to check patient positioning. In lateral views of the knee joint, overlap between the inside and outside of the distal ends of the femur indicate the necessity for an image retake in case of positioning errors.
In the present study, a number of phantom images of the lateral aspect of the femur were taken with certain positioning errors to determine the minimum exposure dose for a pre-test image. In the sample images with positioning errors, observers were asked to measure error distances ΔX and ΔY from a complete overlap between inside and outside of the dry bone specimen, as shown in Fig. 1a, b, respectively. Three RTs participated in the observer study to measure error distances ΔX and ΔY on the images taken at different levels of pre-test exposure (10, 5, and 2% of the actual exposure dose). Figure 2 shows the alignment of an X-ray tube, objects, and a detector (FPD). We used two water equivalent phantoms as scatterers. The total thicknesses of the water phantoms (10 cm) were empirically determined from the standard thickness of knee joints. To represent various types of positioning errors, sample images were taken in the following three positions: 1: lateral rotation and a slight adduction; 2: medial rotation and clear abduction; and 3: a slight medial rotation, as shown in Fig. 3.

Measurement of error distances ΔX (a) and ΔY (b) based on the complete overlap between the inside and outside of the dry bone specimen

The alignment of the X-ray tube, objects, and detector

Sample images of the dry bone specimen obtained in three different positions by changing error distances of overlap between the inside and outside of the knee joint. 1 Lateral rotation and a slight adduction, 2 medical rotation and clear abduction, and 3 a slight medial rotation
3 Results
3.1 Image retake rate estimated from the database in the hospital
Table 1 shows the projection numbers, with and without image retakes, for knee joint radiography. Twelve RTs examined all cases. Overall, 1046 knees were exposed in all the three planes and the total number of images, with the exception of the number of retaken images, was 3138 (1046 × 3). Of the 3138 images, 2568 images were obtained without retakes (81.8%); a total of 713 images were retaken. Therefore, the image retake rate for three-directional knee joint radiography in the hospital was 22.7% (713/3138). Among the twelve RTs, the maximum and minimum number of knees examined by a single RT corresponded to 428 and 23, respectively. Individual data for the number of retakes and examinations have not been included because we believe that those data were not important for the purpose of this study.
Among the three planes of knee joint radiography, the axial view (Skyline view) exhibited the highest image retake rate (38.3%); this implies that image retakes occur approximately once every three times in this view. The image retake rates of the lateral and anterior views were 18.3 and 11.6%, respectively. It should be noted that the sum of the total number of images that did not involve retakes (2568) and the number of image retakes (713) exceeds the total number of images (3138) because an image retake in one plane occasionally occurred more than once.
3.2 Estimated total exposure dose in the proposed procedure
Table 2 presents the estimated total exposure dose ratio Dp/Dc that was simulated based on the statistical data, given in Table 1, by changing the pre-test exposure dose rate α. In the estimated total exposure dose ratio, Dp corresponds to the total exposure dose with the pre-test exposure method, and Dc corresponds to the total exposure dose with the conventional method.
The estimated maximum pre-test exposure dose rate α max was 18.5% [0.227/(1.0 + 0.227) × 100 = 18.5]; thus, when the pre-test exposure dose rate was equal to or lower than 10%, the total exposure dose reduction equaled or exceeded 8% for all patients.
3.3 Determination of the pre-test exposure dose rate for checking patient positioning
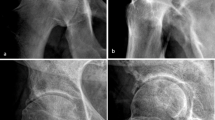
The column (a) in Fig. 4 shows the radiographic image of dry bone specimen of a femur exposed to standard exposure dose in the hospital. The columns (b), (c), and (d) in Fig. 4 show the images obtained at 10, 5, and 2% of the standard exposure dose, respectively. The rows 1, 2, and 3 in Fig. 4 show the images taken in the position of lateral rotation and a slight adduction, medial rotation and clear abduction, and a slight medial rotation, respectively. The resultant gap distances ΔX and ΔY obtained by the three RTs are presented in Table 3, respectively.

Examples of knee joint radiology with exposure dose ratios corresponding to 100% (a), 10% (b), 5% (c), and 2% (d) with the positions of lateral rotation and a slight adduction (1st row), medical rotation and clear abduction (2nd row), and a slight medial rotation (3rd row)
As observed in Table 3, all differences in the errors of the maximum gap distances (ΔX max and ΔY max) between the standard exposure dose and 10% of the standard exposure dose are equal to or less than 1 mm. Additionally, differences in the errors between the standard exposure dose and 5% of the standard exposure dose were equal to or less than 1 mm with the exception of the image involving a slight medial rotation. Moreover, majority of RTs were unable to recognize a gap distance ΔY when the pre-test exposure dose was less than 5% of the standard exposure dose.
4 Discussion
Based on the simulation results for 1046 knee joints from clinical examination records and Eq. (4), the pre-test exposure rate α was estimated for a novel radiographic examination procedure with an ultra-low-dose pre-test exposure. When the pre-test exposure dose was set at 10% of the actual exposure dose, the total patient dose for three-directional knee joint radiography was reduced when compared to that in the conventional method. However, a few considerations exist with respect to the application of the proposed pre-test exposure method.
First, although the proposed method is used to reduce patient dose in a broad manner, it can increase the patient dose in cases where an image retake is not necessary. For example, if a pre-test exposure dose is 10% of the actual exposure dose, then the actual patient exposure dose would be 1.1 times the standard exposure dose. In our study sample of 1046 knee joints, the patient exposure dose increased by 10% for 563 knee joints (53.8%), without any image retakes, on application of the pre-test exposure method when compared to the conventional method. Therefore, to effectively utilize the proposed method and avoid unnecessary radiation exposure, it is necessary to apply this method in clinical conditions only for nonstandard patients and/or some examinations with inexperienced RTs, who may display a high image retake rate.
Second, in the study, the pre-test exposure dose was evaluated using a lateral view of the dry bone specimen of a femur. Although image retaking rate of the axial view (Skyline view) was higher than that of a lateral view, we used distance errors in a lateral view for the evaluation rather than that of an axial view, because error distances in the lateral positioning could be easily and accurately measured and evaluated. However, under clinical conditions, the appropriate pre-test exposure dose could change for each patient based on the thickness of the knee joint. For example, a patient subjected to image retakes tends to have a larger knee joint when compared to a patient with a normal-sized knee joint.
From a different viewpoint, this method is applied based on a situation wherein a patient does not move until an actual exposure is completely obtained, and thus, it is extremely important to consider the manner in which patient position is maintained while checking a pre-test image. Therefore, this procedure requires additional equipment, such as an angle meter and supporting items for patient positioning, to maintain patient position. Furthermore, to improve the diagnostic performance of the proposed pre-test exposure method, it is necessary to develop a novel computerized scheme to analyze positioning errors and indicate correct methods for positioning while retaking images.
With respect to the exposure dose with the pre-test exposure method, the absorbed dose in the three-directional knee joint radiography that was estimated by the EPD (Estimation of Patient Dose in diagnostic radiographic examination) software approximately corresponded to 0.32 mGy × 3 = 0.96 mGy. When the pre-test exposure was 10% of the actual exposure dose, the total absorbed dose increased by 0.096 mGy when compared to the total absorbed dose in the conventional method.
With respect to a survey CT scan (e.g., scout view, topogram, and pilot scan) that is typically used in the CT examination prior to performing a CT scan, the absorbed dose corresponds to 0.03–0.65 mGy (3.2–74.7 mR), as reported by Jennifer et al. [7]. Thus, the absorbed dose in the pre-test exposure method for three-directional knee joint radiography was equal to or within the range of the absorbed dose of the survey CT scan.
The above discussions indicate that it is unfair to consider that the pre-test exposure method is applicable in all cases. However, the proposed method includes advantages such as improving patient positioning, relieving a patient’s distrust toward radiography because of image retakes, and reducing examination time.
5 Conclusion
In conclusion, the study demonstrated that the proposed method, utilizing a pre-test image, has the potential to reduce total exposure dose for all patients by approximately 8% when the image retake rate for the extant specific radiological procedure is relatively high, corresponding to 22.7% or more.
References
Fink C, Hallscheidt PJ, Noeldge G, Kampschulte A, Radeleff B, Hosch WP, Kauffmann GW, Hansman J. Clinical comparative study with a large-area amorphous silicon FPD: image quality and visibility of anatomic structures on chest radiography. AJR. 2002;178:481–6.
Strotzer M, Völk M, Fründ R, Hamer O, Zorger N, Feuerbach S. Routine chest radiography using an FPD: image quality at standard detector dose and 33% dose reduction. AJR. 2002;178:169–71.
Reiner BI, Siegel EL, Flagle C, Deng FJ Hooper, Cox RE, Scanlon M. Effect of filmless imaging on the utilization of radiologic services. Radiology. 2000;215:163–7.
Waaler D, Hofmann B. Image rejects/retakes—radiographic challenges. Radiat Prot Dosim. 2010;139:375–9. doi:10.1093/rpd/ncq032.
Akhtar W, Aslam M, Ali A, Mirza K, Ahmad N. Film retakes in digital and conventional radiography. J Coll Physicians Surg Pak. 2008;18:151–153. doi:03.2008/JCPSP.151153.
Peer S, Peer R, Walcher M, Pohl M, Jaschke W. Comparative reject analysis in conventional film-screen and digital storage phosphor radiography. Eur Radiol. 1999;9:1693–6.
O’ Daniel JC, Stevens DM, Cody DD. Reducing radiation exposure from survey CT scans. AJR. 2005;185:509–15.
Acknowledgements
The authors are grateful to the members of the Department of Radiological Technology, National Defense Medical College Hospital, for supporting this work. This manuscript was partly supported by Akiyoshi Ohtsuka Fellowship of the Japanese Society of Radiological Technology for improvement in English expression of a draft version of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Human rights
All study procedures involving human participants were in accordance with the ethical standards of the Institutional Review Board (IRB) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
The IRB in our institute allowed us to wave patients’ informed consent for all cases and approved to use those cases in this study.
Animal rights
This study did not involve animal models.
About this article

Cite this article
Nose, H., Shiraishi, J. Clinical utility of ultra-low-dose pre-test exposure to avoid unnecessary patient exposure due to positioning errors: a simulation study. Radiol Phys Technol 10, 489–495 (2017). https://doi.org/10.1007/s12194-017-0422-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12194-017-0422-5