
Abstract
The study examined the relationship between neuroticism and individual psychological and physiological health, particularly by analyzing how neuroticism affected stress reactivity and recovery, serving as a potential mechanism linking neuroticism to negative health outcomes. In an observational study involving 30 healthy males (mean age = 21.43, SD = 1.10 years), we employed a standardized mental arithmetic task to induce acute psychological stress. All participants completed the Big Five Personality Neuroticism Scale, a Self-Report Stress Level Scale, and measurements of heart rate (HR) and heart rate variability (HRV). The results showed that individuals characterized by high neuroticism were significantly associated with increased stress reactivity and recovery, as evidenced by elevated low-frequency (LF) components of HRV, an increased low-frequency to high-frequency ratio (LF/HF), and greater changes in heart rate. In contrast, a negative correlation was observed with the high-frequency (HF) component of HRV in terms of stress reactivity and recovery. Nonetheless, the study did not identify a significant relationship between neuroticism and the subjective experience of emotional stress. In summary, neuroticism influences the pattern of stress response in individuals, leading to heightened physiological stress reactivity and diminished physiological stress recovery. These findings suggest that individuals with elevated neuroticism may exhibit non-adaptive physiological responses to acute psychological stress, which could further contribute to negative health outcomes.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Human beings inevitably experience stress in their daily lives. Stress responses to these acute stimuli are attributed to the dynamic interplay between the sympathetic and parasympathetic nervous systems. Activation of the sympathetic nervous system heightens stress, while parasympathetic activation mitigates it (Li et al., 2020). Thus, an increased sympathetic activity along with decreased parasympathetic activity forms the physiological basis of stress. It has been suggested that heart rate variability (HRV) is directly controlled by sympathetic-parasympathetic activation. The framework posits that the power of the high-frequency (HF)component or its equivalent indices reflects parasympathetic nervous activity, while the low-frequency(LF)component or LF/HF ratio reflects sympathetic nervous activity. This conceptualization forms the cornerstone of the theoretical basis in which HRV assessments are analyzed for insights into autonomic nervous system functioning (Hayano & Yuda, 2021). Research in both clinical and general populations indicates a connection between diminished parasympathetic function and heightened cardiovascular risk, encompassing mortality from various causes, myocardial infarction, and additional cardiac incidents (Thayer & Lane, 2007). Thus, HRV is also commonly used as a non-invasive measure of cardiac performance and is a powerful predictor of cardiovascular function (Malik et al., 1996). Furthermore, psychogenic stress provokes subjective emotional responses, notably anxiety (Xin et al., 2017). Prolonged and excessive exposure to such stressors can result in persistent, severe disturbances in physiological functions, potentially culminating in psychosomatic disorders.
Neuroticism, as a broad dimension of personality, represents the degree of an individual’s emotional stability, reflecting their capacity for regulation and adaptation (Costa & McCrae, 1992). The core characteristic of neuroticism is the propensity for negative emotional experiences (Digman, 1997), making individuals more prone to feelings of anxiety, depression, anger, and guilt. Empirical studies have shown that individuals with high levels of neuroticism are often unstable, experiencing emotions that are both frequent and disproportionately intense relative to their environment (Hill et al., 2020; McCrae & Costa Jr., 2003). Moreover, high neuroticism is associated with an increased susceptibility to psychosomatic illnesses. Research has indicated varying degrees of correlation between neuroticism and psychological disorders such as anxiety, mood disorders, and depression (Akiskal et al., 2006; Malouff et al., 2007). Empirical evidence indicates a significant correlation between mood disorders, suicidal behavior, and dysregulation of the Hypothalamic-Pituitary-Adrenal (HPA) axis. This includes altered HPA axis functioning, atypical cortisol responses, and the interplay of the HPA axis with early life stress (Berardelli et al., 2020). Furthermore, elevated inflammation levels, attributed to HPA axis irregularities, may heighten the risk of depression and suicidal tendencies. Research has demonstrated elevated concentrations of inflammatory mediators both peripherally and in the brain among individuals with suicidal risk, in contrast to non-suicidal individuals (Serafini et al., 2017). In the field of acute stress research, neuroticism has consistently been shown to have a broad association with all types of emotional experiences triggered by acute stress (Görgens-Ekermans & Brand, 2012). Therefore, it represents the personality dimension that has been most extensively explored in the research on the relationship between personality and stress. HRV studies have significantly advanced our understanding of the interplay between neuroticism-related traits and autonomic stress responses. Notably, higher anxiety as a trait characteristic is often linked with diminished psychological stress responses. For instance, in public speaking scenarios used as stress-inducing tasks, individuals with pronounced trait anxiety exhibited reduced physiological responses within the hypothalamic-pituitary-adrenal (HPA) axis and sympathetic-adrenomedullary system (Jezova et al., 2004). Conversely, research by Thayer et al. highlights that anxiety disorders and their primary symptom of anxiety states correlate with decreased cardiac vagal tone, evidenced by reduced high-frequency (HF) HRV and shorter interbeat intervals (IBIs)(Foley & Kirschbaum, 2010). Furthermore, studies have also discovered that higher levels of depression are associated with greater sympathetic nervous activation and more significant vagal withdrawal in response to stress, manifested by increased heart rate and blood pressure reactivity (Grewen et al., 2004; Tafet & Nemeroff, 2016).
As previously mentioned, neuroticism is closely related to psychological and physiological health. Stress reactivity and stress recovery are crucial indicators of individual psychological and physiological well-being. They also represent significant physiological pathways to explore individual mental and physical health (McEwen, 2007; Saulsman & Page, 2004). Stress reactivity is characterized as the amalgam of psychological and physiological alterations occurring in response to an acute stressor or an external perturbation (Linden et al., 1997). The stress reactivity hypothesis’ posits that heightened cardiovascular reactivity to environmental stressors detrimentally impacts health. Nonetheless, some studies also indicate that diminished cardiovascular reactivity may adversely affect health outcomes (Schwerdtfeger & Gerteis, 2013). The concept of stress recovery pertains to the velocity and extent to which psychophysiological responses revert to pre-stressor baseline levels following cessation of the stress-inducing stimulus (Hutchinson & Ruiz, 2011). An elongated or inadequate restorative response is indicative of compromised adaptive capacity, necessary for effective adjustment to environmental demands. Consequently, psychophysiological recovery is regarded as a pivotal determinant in safeguarding against the deleterious ramifications of stress on biopsychosocial health (Brosschot et al., 2006). It has been posited that cardiovascular recovery efficacy may be a more critical predictor of disease progression than stress-induced cardiovascular reactivity (Pieper & Brosschot, 2005). HRV is a key indicator of cardiovascular function and significantly influences the body’s stress reactivity and recovery processes via the autonomic nervous system. During exposure to threats or challenges, the sympathetic nervous system is stimulated, resulting in an elevated heart rate as an adaptive response to environmental stimuli. Conversely, the activation of the parasympathetic nervous system, typically following the removal of threats or challenges, leads to a reduction in heart rate, facilitating a return to a state of equilibrium. The regulation of stress reactivity and recovery by the autonomic nervous system is predominantly mediated by the actions of the parasympathetic branch (Aubert et al., 2003; Zhang et al., 2007).Investigating this link might elucidate the role of the sympathetic-adrenal-medullary axis in mediating the relationship between neuroticism and stress-related physiological responses patterns. Currently, most studies that have examined the association between neuroticism and physiological responses induced by acute psychological stress have found that neuroticism is associated with blunted cardiovascular reactivity and poorer recovery of cardiovascular responses (Chida & Hamer, 2009; Hughes et al., 2011; Kennedy & Hughes, 2004). Conversely, it has also been found that neuroticism is associated with greater cardiovascular reactivity and poorer cardiovascular recovery (Brumbaugh et al., 2013; Kaiser et al., 1997; Norris et al., 2007), significantly increasing the risk of cardiovascular diseases (Brosschot et al., 2006; Chida & Steptoe, 2010). These studies demonstrate that neuroticism leads to maladaptive physiological responses to stressors, both individually and within specific groups. To elucidate the influence of personality traits on long-term health outcomes, large-scale prospective cohort studies show that personality traits like neuroticism, alongside stress, can indirectly elevate health risks, especially in cardiovascular diseases, by altering physiological stress responses. This underscores the significance of psychological factors in long-term health outcomes and disease risk (Batty et al., 2016; Chida & Hamer, 2009; Jokela et al., 2014; Shipley et al., 2007). Nonetheless, the observational nature of these cohorts precludes definitive conclusions about causality between neuroticism and cardiovascular outcomes. Despite previous research focusing on the stress reactivity and recovery characteristics associated with neuroticism and its facets, the inconsistency in observed results across different studies is attributed to the influence of various factors. Some studies suggest that individuals with high neuroticism typically exhibit emotional volatility, instability, and are prone to anxiety and tension (Ireland & Mehl, 2014). These characteristics may lead to significant differences in their stress responses. One the one hand, when facing stressors, individuals with high neuroticism may perceive stress more acutely and sensitively, consequently displaying more pronounced stress response. On the other hand, individuals with high neuroticism may have developed adaptive mechanisms to cope with chronic anxiety, resulting in a blunted stress response to stressors (Sapolsky, 1994). Moreover, varying cultural and environmental contexts, coupled with potential inadequacies in controlling for confounding variables, may account for inconsistencies observed in these associations (Batty et al., 2016; Jokela et al., 2014; Sun et al., 2022). There are also some studies that have failed to find evidence of a relationship between neuroticism and cardiovascular reactivity to stress due to low statistical power (Puig-Perez et al., 2016; Schneider, 2004; Stoyanov et al., 2013). Presently, the prevailing view among researchers attributes the inconsistencies in findings regarding personality and biological stress responses to various methodological limitations in the relevant studies (Bibbey et al., 2013; Verschoor & Markus, 2011). Future research should consider utilizing younger student populations (Verschoor & Markus, 2011), acknowledge the constraints posed by limited variability in trait scores (Wirtz et al., 2007), and implement comprehensive statistical adjustments to account for a wide array of potential confounding variables (Williams et al., 2009; Wirtz et al., 2007).
Considering the above circumstances, it is evident that the stress psychophysiological response pattern exhibited by neuroticism remains unclear, and most studies seldom simultaneously focus on stress reactivity and recovery. Secondly, the autonomic nervous response pattern displayed by neuroticism under stress conditions warrants further investigation. Therefore, the main aim of the current study was to further explore the relationship between neuroticism and the acute psychological stress response. Here, our aim is to comprehensively investigate and assess the following aspects by utilizing the acute physiological stress states expressed through HR and HRV (i.e., HF, LF, LF/HF):(1) the association between neuroticism and physiological stress reactivity during acute psychological stress, (2) the characteristics of physiological stress recovery in neurotic individuals exposed to stress environments, further revealing the underlying physiological mechanisms through which neuroticism affects overall health, and (3) the psychological responses to acute stress, using self-reported state impact as an indicator. Considering the above evidence, we hypothesize thatneuroticism will correlate with heightened physiological responses to stress, as indicated by increases in HR changes, augmented sympathetic nervous system activation (evidenced by larger alterations in LF and the LF/HF ratio), and a reduction in parasympathetic nervous system responses (noted by decreased HF changes). Moreover, we anticipate that neuroticism will be linked to slower physiological recovery from stress, characterized by prolonged elevated HR (significant HR changes), continued elevated sympathetic nervous system activity (greater changes in LF and LF/HF ratio), and diminished parasympathetic nervous function (reduced HF changes). Finally, we also hypothesize that neuroticism will be associated with more severe subjective emotional stress experiences, as shown by increased self-reported stress levels.
Method
Participants
The study was advertised on the University’s online research participation website from which participants were recruited. Thirty healthy men participated in this study and they each received the equivalent of $35 in Chinese yuan to compensate them for their time and effort. Participants ranged in age from 20 to 25 years (mean age = 21.43, SD = 1.10) and all were in good health with no reported history of cardiovascular disease and no history of alcohol or drug abuse. They were asked to refrain from strenuous exercise and alcohol consumption for at least 12 h before participating in the study to exclude the effects of exercise (Somers et al., 1991) and alcohol intake on cardiovascular function (Potter et al., 1986).
Procedure
To mitigate the effects of circadian rhythms, all experimental sessions were scheduled from 2:00 PM to 5:00 PM. We instructed participants to abstain from medications and vigorous exercise for at least two hours before their laboratory visit. Compliance with these prerequisites was confirmed by all participants. Upon their arrival at the laboratory, they first executed an informed consent form. This was succeeded by a 15-minute acclimation period, after which participants asked to complete various questionnaires, including demographic information (age, etc.) and personality scales. Subsequently,activated silver chloride electrode patches were attached to their neck and ankles for the acquisition of ECG signals. The stress test protocol encompasses an 8-minute baseline measurement, a subsequent 10-minute stress phase, followed by an 8-minute recovery period. Self-reported stress evaluations are conducted immediately post-baseline, stress, and recovery phases. During the experiment, participants were located approximately 80 cm from the computerized display screen, and all stimuli were presented on a white background in the center of a 17-inch display screen using E-Prime 3.0, which continuously recorded the subjects’ ECG signals from the baseline phase to the recovery phase.
Measures
Chinese big five personality inventory - brief version (CBF-PI-B)
Wang et al. (2011) revised the CBF-PI-B, a 40-item Big Five personality scale with 33 positive and 7 negative items, demonstrating strong reliability and validity. Each factor of the short-form correlates highly (> 0.85) with its full-scale counterpart, and all five dimensions show Cronbach’s alpha > 0.75 (Wang et al., 2011). The neuroticism subscale, rated on a 6-point Likert scale (1–6), measures agreement with statements, scoring 8–48. Higher scores signify stronger neurotic traits. In this study, the neuroticism subscale’s Cronbach’s alpha was 0.940.
Self-reported stress level
The self-reported stress level was used to assess participants’ levels of stress and tension at a given moment. The scale is scored using a 5-point scale, with 1 representing very relaxed, 2 representing more relaxed, 3 representing between tense and relaxed, 4 representing more tense, and 5 representing very tense (Qi et al., 2016).
Stress tasks
The stress task was a mental arithmetic task that was based on Qi et al.‘s modified version of the Montreal Brain Imaging Stress Task (Qi et al., 2016). The mental arithmetic task specifically entailed participants determining if the product of two decimal-numbered figures was less than 10 within a predetermined time frame. This task lasted for 10 min. Before the experiment commenced, participants were instructed to respond both quickly and accurately (Yang et al., 2012). Additionally, they were informed that monitoring equipment would continuously record their performance, and external observers would continually assess and evaluate it. A flowchart of this trial is presented in Fig. 1. This task induces an acute psychogenic stress response by creating uncontrollability of the subject’s performance on the task through time pressure to solve arithmetic problems, and by comparing the participant’s performance with the group’s average performance, thereby creating a socially evaluative threat (Dedovic et al., 2005; Pruessner et al., 2008).

Mental arithmetic task
Note: Each trial commenced with a fixation point displayed at the screen’s center for 300–500 ms, succeeded by a mental arithmetic task for 1500 ms, which terminated upon the subject’s keypress. Subsequently, a randomized blank screen appeared for 300–500 ms, followed by feedback for 1000 ms
Stress response measurement
A Biopac Amplifer-System (MP150; Biopac, Goleta, CA, USA) and three activated silver chloride electrode patches were used for electrocardiogram (ECG) signal acquisition. Electrode patches were affixed to the right cervical region and the medial aspects of both ankles. Signals were recorded at a sample rate of 1,000 Hz. In every time point, HR was calculated by averaging the 5-min continuous recording using the AcqKnowledge4.2 software and defined as the number of beats per minutes (bpm). In a parallel manner, a standardised 5-min measurement of HRV was used in this study. ECG waveforms underwent frequency domain analysis employing the Fast Fourier Transform (FFT) technique, i.e., time-domain signals were converted into their respective amplitude and phase data for various frequency components. Using a spectrogram, amplitude details for both high-frequency and low-frequency components were discerned and extracted. We focused on three frequency-domain metrics: High-frequency component (HF: 0.15–0.40 Hz) in ms2, indicative of the ECG’s rapid oscillations;low-frequency component (LF: 0.04–0.15 Hz) in ms2, reflecting the ECG’s slower oscillations;the LF/HF ratio, representing the power proportion of LF to HF. To rectify their skewed distributions, outcomes for HF, LF, and LF/HF underwent a natural logarithmic transformation.
Data analyses
All statistical analyses were analyzed using IBM SPSS Statistics for Windows version 26.0.0.0 (IBM Corp, Armonk, New York, USA). To determine whether the mental arithmetic task was an effective stressor and produced physiological and psychological changes, a series of repeated-measures ANOVAs (baseline, stress, and recovery periods) were performed on heart rate and heart rate variability. Similarly, to confirm whether the mental arithmetic task induced psychological stress, a repeated-measures ANOVA was conducted on self-reported stress levels (baseline period, stress period, recovery period). When Mauchly’s test for sphericity of variance was violated (p < .05), epsilon(ε) was assessed to select the appropriate correction method and the Greenhouse - Geisser correction was used when ε < 0.75, and the Huynh-Feldt correction was used when ε > 0.75.
Pearson correlations were used to explore correlations between key psychological variables. Simple correlations between HR, frequency domain indicators of heart rate variability (HF, LF, LF/HF), self-reported stress levels, and changes in those variables and neuroticism scores at each measurement stage were analyzed.
Hierarchical multiple regressions based on the correlation analyses were performed to examine the associations between neuroticism and each physiologic reactivity and recovery parameter. According to the law of initial values, it is imperative to account for the influence of baseline measurements on reactivity and recovery outcomes by calculating the delta changes between stress and recovery periods in relation to baseline values (Benjamin, 1967; de Rooij, 2013; Llabre et al., 1991). Specifically, reactivity is determined by subtracting the baseline period mean from the stress period mean, while recovery is calculated by subtracting the baseline period mean from the recovery period mean. Neuroticism was subsequently entered into the regression model as a predictor variable, and physiologic reactivity and restorative parameters were entered as outcome variables. To control for potential confounding variables, age and baseline period measurements were entered as control variables in Step 1 of the multiple regression, and neuroticism scores were entered in Step 2. Considering the effect of altered measures of reactivity on recoverability, the corresponding reactivity was also used as a control variable in the hierarchical regression when predicting recovery.
In this analysis, p-values ≤ 0.05 were deemed to hold statistical significance. We assessed the effect size of the predictors by utilizing the observed increment in R². Statistical test power analyses were conducted using G*Power software. Additionally, to mitigate the risk of inflated false discovery rates arising from multiple hypothesis testing, the p-values underwent adjustments using the Benjamini-Hochberg procedure. This approach is underpinned by a sequentially adjusted version of the Bonferroni correction, tailored to address the challenges of multiple comparisons.
Result
Manipulation check
A series of repeated measures (baseline period, stress period) ANOVAs confirmed that the mental arithmetic task successfully induced physiological and psychological stress (all ps < 0.001). All parameters showed statistically significant increases from baseline to the stress stage, as shown in Table 1. Specifically, the main effect of the stage was significant on HR, HF HRV, LF HRV, and LF/HF HRV, F (1.15, 33.40) = 22.858, p < .001, ηp2 = 0.44;F (1.45, 41.89) = 17.15, p < .001, ηp2 = 0.37; F(2, 58) = 47.14, p < .001, ηp2 = 0.62; F(1.08, 31.33) = 18.93, p < .001, ηp2 = 0.82 and multiple comparisons showed that HR, HF HRV, LF HRV, and LF/HF HRV were significantly higher during the stress period than at baseline (p < .001). In addition, a repeated measures ANOVA revealed that self-reported stress levels exhibited a significant stage main effect, F (1.76,51.19) = 73.06, p < .001, ηp2 = 0.72, and multiple comparisons showed a significant increase in self-reported stress levels from pre-task to post-task scores (p < .001), suggesting that the mental arithmetic task induced psychological stress. To avoid overall Type I errors, the Bonferroni method was used for multiple comparisons.
Neuroticism and psychological response
As shown in Table 2, there were no statistically significant associations between neuroticism and self-reported stress levels of reactivity and recovery. i.e., no significant association was observed between neuroticism and subjective stress responses elicited by the stressor.
Neuroticism and physiological reactivity
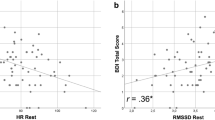
In Table 2, the unadjusted correlation analysis indicated that neuroticism exhibited a negative association with HF reactivity. Conversely, it demonstrated a positive correlation with LF, LF/HF ratio, and HR reactivity.
Results of the hierarchical multiple linear regression model controlling for age and baseline measurements, indicated that neuroticism significantly negatively predicted HF reactivity, β = -0.02, p < .001, ΔR2 = 0.34, test power = 0.87. Neuroticism positively predicted HR reactivity, β = 1.51, p < .001, ΔR2 = 0.59, test power = 0.98, LF reactivity, β = 0.04, p = .05, ΔR2 = 0.11, test power = 0.51, and LF/HF reactivity, β = 0.05, p < .001, ΔR2 = 0.82, test power = 0.98(see Table 3).
All significant associations between neuroticism and physiological reactivity remained statistically significant following Benjamini- Hochberg corrections.
Neuroticism and physiological recovery
In unadjusted correlational analyses, it was observed that neuroticism exhibited a significant negative association with HF recovery, and a positive association with LF, LF/HF ratio, and HR recovery (see Table 2).
In adjusted analyses, neuroticism remained a significant negative predictor of HF recovery, β = -0.01, p < .001, ΔR2 = 0.49, test power = 0.98. However, it positively predicted greater recovery on measures of HR, β = 0.29, p = .049, ΔR2 = 0.02, test power = 0.53, LF, β = 0.11,p < .001, ΔR2 = 0.24, test power = 0.95, and LF/HF, β = 0.03, p = .035, ΔR2 = 0.01, test power = 0.58 (see Table 4).
Follow-up analyses using a Benjamini-Hochberg correction indicated that all significant associations remained statistically significan.
Discussion
The study investigated the relationship between neuroticism and acute psychological stress response through physiological and psychological measurements. It was found that neuroticism could predict the the physiological response patterns triggered by acute psychological stress. High neuroticism was significantly associated with an increase in the LF component, a higher LF/HF ratio, and greater change in HR, while showing a negative correlation with both the stress reactivity and recovery of the HF component. This suggested that under stress, individuals with high neuroticism exhibited stronger activation of the sympathetic nervous system and diminished parasympathetic nervous system inhibition. Following the cessation of stress, these individuals were found to exhibit slower recovery rates in sympathetic nervous activity, maintaining comparatively elevated activation levels, and parasympathetic nervous activity, persisting at comparatively reduced activity levels. However, in this study, neuroticism was not significantly associated with subjective emotional stress experience.
The majority of studies to date have found that individuals with higher levels of neuroticism exhibit a reduced sympathetic nervous activation in response to acute stress, characterized by blunted cardiovascular reactivity (Bibbey et al., 2013; Hughes et al., 2011; Xin et al., 2017). In contrast, the current study suggests that individuals with high levels of neuroticism are associated with a greater sympathetic nervous activation response and a decrease in vagal tone, as evidenced by an increased HR reactivity. This is in line with previous research that focused on the aspects of neuroticism related to autonomic stress responses. Consistently, these studies indicated that the aspects of high neuroticism were associated with greater cardiovascular reactivity under stress conditions (Grewen et al., 2004; Movius & Allen, 2005; Schwerdtfeger & Gerteis, 2013; Vella & Friedman, 2007). Furthermore, while previous studies have shown that neuroticism negatively predicts subjective stress (Xin et al., 2017; Cheng et al., 1990), the current study failed to replicate that result. One potential explanation may relate to variability in the stress measurement tasks used in the different studies. Neuroticism has been found to be associated with blunted cardiovascular responses in several studies using social tasks to induce stress (van der Veen et al., 2016). By comparison, earlier studies using cognitive tasks to induce stress showed neuroticism to be associated with a greater magnitude of change in physiological indices (Cheng et al., 1990). In essence, when confronted with adverse psychosocial or physiological stimuli, both overly intense and insufficient stress responses are non-adaptive and indicative of a diminished state of homeostasis. Moreover, the persistent escalation of this unstable physiological burden is a crucial pathological contributor to the development of psychosomatic disorders (Kassim et al., 2015; McEwen, 2000).
Psychophysiological recovery is considered one of the key factors in preventing stress from negatively impacting mental and physical health. Inadequate recovery or prolonged stress responses increase non-steady-state load, thereby affecting overall health. stress in predicting the development of cardiovascular diseases (Hutchinson & Ruiz, 2011; Pieper & Brosschot, 2005). Previous research on the effects of neuroticism on stress response recovery has shown that individuals with high levels of neuroticism demonstrate worse cardiovascular recovery in stressful situations (Anderson et al., 2005; Chida & Hamer, 2009; Hutchinson & Ruiz, 2011; Pieper & Brosschot, 2005). The current study indicates that during stress recovery, individuals with high neuroticism continue to exhibit high levels of sympathetic nervous system activity and low levels of vagal tone. These findings suggest that individuals with high neuroticism find it more difficult to return to a physiological state of calm after stress has dissipated. Over time, this pattern of physiological response may increase the risk of cardiovascular diseases (Dyavanapalli, 2020; Hayano & Yuda, 2021).
The current study has some limitations. First, given the exploratory nature of our study, neuroticism has been able to significantly predict both the reactivity and recovery to physiological stress even with a relatively small sample size, achieving a moderate or higher statistical power. This may suggest that the actual effect is substantial, allowing for significant effects to be detected even in the context of a limited sample size. Therefore, it is imperative to include a larger and more comprehensive sample in subsequent studies to verify the stability and generality of these findings. Second, this study used a sample of college students who are likely to have different experiences and abilities than those who do not attend college. However, these group differences may be less important in studies that focus on basic human processes such as personality and emotions (Schneider et al., 2012). Finally, because the experiments were conducted in a laboratory, the findings may be limited to that situation and may not be representative of stress experienced in everyday life. However, a recent study suggests that reactivity in the laboratory can predict reactivity to stressors in real life (Johnston et al., 2008).
Conclusion
In conclusion, this study aimed to explore the relationship between neuroticism and stress reactivity and recovery. Our findings suggest that neuroticism can predict physiological stress reactivity and recovery caused by acute psychological stress. This study did not find a significant correlation between neuroticism and subjective emotional stress experience, which may imply an inconsistency between the physiological responses and subjective feelings of individuals with high neuroticism under psychological stress. These findings may indicate that individuals with high levels of neuroticism have a nonadaptive physiologic response pattern to acute psychological stress, which can lead to adverse health outcomes. These findings may suggest that individuals with neuroticism, characterized as a stress-prone personality trait, exhibit a maladaptive physiological response to acute psychological stress, marked by an impaired ability to maintain the body’s dynamic equilibrium. Specifically, they might experience heightened physiological reactions and exhibit delayed recovery post-stress, potentially jeopardizing their health. This study explores the link between neuroticism and acute psychological stress, shedding light on the physiological and psychological pathways affecting health outcomes. These insights could offer guidance for tailored psychological interventions. For instance, proactive measures can address these maladaptive responses, aiming to bolster physiological stress regulation and consequently improve overall well-being. Practically, monitoring tools capturing heartbeat and pulse intervals could be beneficial for keeping a check on those with pronounced neuroticism traits, thereby aiding in mental health upkeep. Furthermore, in terms of public health strategies and health education, these findings may help enhance public awareness of the psychological and physiological health needs of individuals with high neuroticism.
Data availability
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
References
Akiskal, H. S., Kilzieh, N., Maser, J. D., Clayton, P. J., Schettler, P. J., Shea, M. T., Endicott, J., Scheftner, W., Hirschfeld, R. M. A., & Keller, M. B. (2006). The distinct temperament profiles of bipolar I, bipolar II and unipolar patients. Journal of Affective Disorders, 92(1), 19–33. https://doi.org/10.1016/j.jad.2005.12.033
Anderson, J. C., Linden, W., & Habra, M. E. (2005). The importance of examining blood pressure reactivity and recovery in anger provocation research. International Journal of Psychophysiology, 57(3), 159–163. https://doi.org/10.1016/j.ijpsycho.2004.12.011
Aubert, A., Seps, B., & Beckers, F. (2003). Heart rate variability in athletes. Sports Medicine (Auckland N Z), 33, 889–919. https://doi.org/10.2165/00007256-200333120-00003
Batty, G. D., McIntosh, A. M., Russ, T. C., Deary, I. J., & Gale, C. R. (2016). Psychological distress, neuroticism, and cause-specific mortality: Early prospective evidence from UK Biobank. Journal of Epidemiology and Community Health, 70(11), 1136–1139. https://doi.org/10.1136/jech-2016-207267
Benjamin, L. S. (1967). Facts and artifacts in using analysis of covariance to undo the law of initial values. Psychophysiology, 4(2), 187–206. https://doi.org/10.1111/j.1469-8986.1967.tb02757.x
Berardelli, I., Serafini, G., Cortese, N., Fiaschè, F., O’Connor, R. C., & Pompili, M. (2020). The involvement of hypothalamus-pituitary-adrenal (HPA) Axis in suicide risk. Brain Sciences, 10(9). https://doi.org/10.3390/brainsci10090653
Bibbey, A., Carroll, D., Roseboom, T. J., Phillips, A. C., & de Rooij, S. R. (2013). Personality and physiological reactions to acute psychological stress. International Journal of Psychophysiology, 90(1), 28–36. https://doi.org/10.1016/j.ijpsycho.2012.10.018
Brosschot, J. F., Gerin, W., & Thayer, J. F. (2006). The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. Journal of Psychosomatic Research, 60(2), 113–124. https://doi.org/10.1016/j.jpsychores.2005.06.074
Brumbaugh, C. C., Kothuri, R., Marci, C., Siefert, C., & Pfaff, D. D. (2013). Physiological correlates of the big 5: Autonomic responses to video presentations. Applied Psychophysiology and Biofeedback, 38(4), 293–301. https://doi.org/10.1007/s10484-013-9234-5
Cheng, S., Tang, C., & Li, X. (1990). Effects of personality type on stress response (section of laboratory stressor). Acta Psychologica Sinica, 22(4), 79–86.
Chida, Y., & Hamer, M. (2009). Chronic psychosocial factors and Acute physiological responses to Laboratory-Induced stress in healthy populations: A quantitative review of 30 years of investigations. Psychological Bulletin, 135, 793. https://doi.org/10.1037/a0016852
Costa, P. T., & McCrae, R. R. (1992). Four ways five factors are basic. Personality and Individual Differences, 13(6), 653–665. https://doi.org/10.1016/0191-8869(92)90236-I
de Rooij, S. R. (2013). Blunted cardiovascular and cortisol reactivity to acute psychological stress: A summary of results from the Dutch famine birth cohort study. International Journal of Psychophysiology, 90(1), 21–27. https://doi.org/10.1016/j.ijpsycho.2012.09.011
Dedovic, K., Renwick, R., Mahani, N. K., Engert, V., Lupien, S. J., & Pruessner, J. C. (2005). The Montreal imaging stress Task: Using functional imaging to investigate the effects of perceiving and processing psychosocial stress in the human brain. Journal of Psychiatry & Neuroscience, 30(5), 319–325.
Digman, J. M. (1997). Higher-order factors of the big five. Journal of Personality and Social Psychology, 73(6), 1246–1256. https://doi.org/10.1037//0022-3514.73.6.1246
Dyavanapalli, J. (2020). Novel approaches to restore parasympathetic activity to the heart in cardiorespiratory diseases. American Journal of Physiology-Heart and Circulatory Physiology, 319(6), H1153–H1161. https://doi.org/10.1152/ajpheart.00398.2020
Foley, P., & Kirschbaum, C. (2010). Human hypothalamus-pituitary-adrenal axis responses to acute psychosocial stress in laboratory settings. Neuroscience and Biobehavioral Reviews, 35(1), 91–96. https://doi.org/10.1016/j.neubiorev.2010.01.010
Görgens-Ekermans, G., & Brand, T. (2012). Emotional intelligence as a moderator in the stress-burnout relationship: A questionnaire study on nurses. Journal of Clinical Nursing, 21(15–16), 2275–2285. https://doi.org/10.1111/j.1365-2702.2012.04171.x
Grewen, K. M., Girdler, S. S., Hinderliter, A., & Light, K. C. (2004). Depressive symptoms are related to higher ambulatory blood pressure in people with a family history of hypertension. Psychosomatic Medicine, 66(1), 9–16. https://doi.org/10.1097/01.psy.0000106881.60228.16
Hayano, J., & Yuda, E. (2021). Assessment of autonomic function by long-term heart rate variability: Beyond the classical framework of LF and HF measurements. Journal of Physiological Anthropology, 40(1), 21. https://doi.org/10.1186/s40101-021-00272-y
Hill, W. D., Weiss, A., Liewald, D. C., Davies, G., Porteous, D. J., Hayward, C., McIntosh, A. M., Gale, C. R., & Deary, I. J. (2020). Genetic contributions to two special factors of neuroticism are associated with affluence, higher intelligence, better health, and longer life. Molecular Psychiatry, 25(11), 3034–3052. https://doi.org/10.1038/s41380-019-0387-3
Hughes, B. M., Howard, S., James, J. E., & Higgins, N. M. (2011). Individual differences in adaptation of cardiovascular responses to stress. Biological Psychology, 86(2), 129–136. https://doi.org/10.1016/j.biopsycho.2010.03.015
Hutchinson, J. G., & Ruiz, J. M. (2011). Neuroticism and cardiovascular response in women: Evidence of effects on blood pressure recovery. Journal of Personality, 79(2), 277–302. https://doi.org/10.1111/j.1467-6494.2010.00679.x
Ireland, M. E., & Mehl, M. R. (2014). Natural language use as a marker of personality. In The Oxford Handbook of Language and Social Psychology (pp.201–218). https://doi.org/10.1093/oxfordhb/9780199838639.013.034
Jezova, D., Makatsori, A., Duncko, R., Moncek, F., & Jakubek, M. (2004). High trait anxiety in healthy subjects is associated with low neuroendocrine activity during psychosocial stress. Progress in Neuro-Psychopharmacology & Biological Psychiatry, 28(8), 1331–1336. https://doi.org/10.1016/j.pnpbp.2004.08.005
Johnston, D. W., Tuomisto, M. T., & Patching, G. R. (2008). The relationship between cardiac reactivity in the laboratory and in real life. Health Psychology, 27(1), 34–42. https://doi.org/10.1037/0278-6133.27.1.34
Jokela, M., Pulkki-Råback, L., Elovainio, M., & Kivimäki, M. (2014). Personality traits as risk factors for stroke and coronary heart disease mortality: Pooled analysis of three cohort studies. Journal of Behavioral Medicine, 37(5), 881–889. https://doi.org/10.1007/s10865-013-9548-z
Kaiser, J., Beauvale, A., & Bener, J. (1997). The evoked cardiac response as a function of cognitive load differs between subjects separated on the main personality dimensions. Personality and Individual Differences, 22(2), 241–248. https://doi.org/10.1016/S0191-8869(96)00188-2
Kassim, A. A., Payne, A. B., Rodeghier, M., Macklin, E. A., Strunk, R. C., & DeBaun, M. R. (2015). Low forced expiratory volume is associated with earlier death in sickle cell anemia. Blood, 126(13), 1544–1550. https://doi.org/10.1182/blood-2015-05-644435
Kennedy, D. K., & Hughes, B. M. (2004). The optimism-neuroticism question: An evaluation based on Cardiovascular Reactivity in Female College Students. The Psychological Record, 54(3), 373–386. https://doi.org/10.1007/BF03395480
Li, C., Zheng, S., Lu, S., Zhang, Y., & Liu, Z. (2020). The relation between the neuroticism of big five personality and heart rate variability: A correlation study. Studies of Psychology and Behavior, 18(2), 275–280. https://psybeh.tjnu.edu.cn/EN/Y2020/V18/I2/275
Linden, W., Earle, T. L., Gerin, W., & Christenfeld, N. (1997). Physiological stress reactivity and recovery: Conceptual siblings separated at birth? Journal of Psychosomatic Research, 42(2), 117–135. https://doi.org/10.1016/s0022-3999(96)00240-1
Llabre, M. M., Spitzer, S. B., Saab, P. G., Ironson, G. H., & Schneiderman, N. (1991). The reliability and specificity of delta versus residualized change as measures of cardiovascular reactivity to behavioral challenges. Psychophysiology, 28(6), 701–711. https://doi.org/10.1111/j.1469-8986.1991.tb01017.x
Malik, M., Bigger, J. T., Camm, A. J., Kleiger, R. E., Malliani, A., Moss, A. J., & Schwartz, P. J. (1996). Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. European Heart Journal, 17(3), 354–381. https://doi.org/10.1093/oxfordjournals.eurheartj.a014868
Malouff, J. M., Thorsteinsson, E. B., Rooke, S. E., & Schutte, N. S. (2007). Alcohol involvement and the five-factor model of personality: A meta-analysis. Journal of Drug Education, 37, 277–294. https://doi.org/10.1002/abio.370040210
McCrae, R. R., & Costa, P. T. Jr. (2003). Personality in adulthood: A five-factor theory perspective. Guilford Press. https://doi.org/10.4324/9780203428412. 2nd ed.
McEwen, B. S. (2000). The neurobiology of stress: From serendipity to clinical relevance. Brain Research, 886(1), 172–189. https://doi.org/10.1016/S0006-8993(00)02950-4
McEwen, B. S. (2007). Physiology and neurobiology of stress and adaptation: Central role of the brain. Physiological Reviews, 87(3), 873–904. https://doi.org/10.1152/physrev.00041.2006
Movius, H. L., & Allen, J. J. (2005). Cardiac vagal tone, defensiveness, and motivational style. Biological Psychology, 68(2), 147–162. https://doi.org/10.1016/j.biopsycho.2004.03.019
Norris, C. J., Larsen, J. T., & Cacioppo, J. T. (2007). Neuroticism is associated with larger and more prolonged electrodermal responses to emotionally evocative pictures. Psychophysiology, 44, 823–826. https://doi.org/10.1111/j.1469-8986.2007.00551.x
Pieper, S., & Brosschot, J. F. (2005). Prolonged stress-related cardiovascular activation: Is there any? Annals of Behavioral Medicine, 30(2), 91–103. https://doi.org/10.1207/s15324796abm3002_1
Potter, J. F., Watson, R. D., Skan, W., & Beevers, D. G. (1986). The pressor and metabolic effects of alcohol in normotensive subjects. Hypertension, 8(7), 625–631. https://doi.org/10.1161/01.hyp.8.7.625
Pruessner, J. C., Dedovic, K., Khalili-Mahani, N., Engert, V., Pruessner, M., Buss, C., Renwick, R., Dagher, A., Meaney, M. J., & Lupien, S. (2008). Deactivation of the limbic system during acute psychosocial stress: Evidence from positron emission tomography and functional magnetic resonance imaging studies. Biological Psychiatry, 63(2), 234–240. https://doi.org/10.1016/j.biopsych.2007.04.041
Puig-Perez, S., Villada, C., Pulopulos, M. M., Hidalgo, V., & Salvador, A. (2016). How are neuroticism and depression related to the psychophysiological stress response to acute stress in healthy older people? Physiology & Behavior, 156, 128–136. https://doi.org/10.1016/j.physbeh.2016.01.015
Qi, M., Gao, H., Guan, L., Liu, G., & Yang, J. (2016). Subjective stress, salivary cortisol, and electrophysiological responses to psychological stress. Frontiers in Psychology, 7, 229. https://doi.org/10.3389/fpsyg.2016.00229
Sapolsky, R. M. (1994). Individual differences and the stress response. Seminars in Neuroscience, 6(4), 261–269. https://doi.org/10.1006/smns.1994.1033
Saulsman, L. M., & Page, A. C. (2004). The five-factor model and personality disorder empirical literature: A meta-analytic review. Clinical Psychology Review, 23(8), 1055–1085. https://doi.org/10.1016/j.cpr.2002.09.001
Schneider, T. R. (2004). The role of neuroticism on psychological and physiological stress responses. Journal of Experimental Social Psychology, 40(6), 795–804. https://doi.org/10.1016/j.jesp.2004.04.005
Schneider, T. R., Rench, T. A., Lyons, J. B., & Riffle, R. R. (2012). The influence of neuroticism, extraversion and openness on stress responses. Stress and Health, 28(2), 102–110. https://doi.org/10.1002/smi.1409
Schwerdtfeger, A. R., & Gerteis, A. K. (2013). Is the blunted blood pressure reactivity in dysphoric individuals related to attenuated behavioral approach? International Journal of Psychophysiology, 90(1), 58–65. https://doi.org/10.1016/j.ijpsycho.2013.01.015
Serafini, G., Adavastro, G., Canepa, G., Capobianco, L., Conigliaro, C., Pittaluga, F., Murri, M. B., Valchera, A., De Berardis, D., Pompili, M., Lindqvist, D., Brundin, L., & Amore, M. (2017). Abnormalities in Kynurenine Pathway Metabolism in Treatment-Resistant Depression and Suicidality: A systematic review. Cns & Neurological Disorders-Drug Targets, 16(4), 440–453. https://doi.org/10.2174/1871527316666170413110605
Shipley, B. A., Weiss, A., Der, G., Taylor, M. D., & Deary, I. J. (2007). Neuroticism, Extraversion, and Mortality in the UK Health and Lifestyle Survey: A 21-Year prospective cohort study. Psychosomatic Medicine, 69(9), 923–931. https://doi.org/10.1097/PSY.0b013e31815abf83
Somers, V. K., Conway, J., Coats, A., Isea, J., & Sleight, P. (1991). Postexercise hypotension is not sustained in normal and hypertensive humans. Hypertension, 18(2), 211–215. https://doi.org/10.1161/01.hyp.18.2.211
Stoyanov, Z., Boncheva, I., Nikolova, P., & Ivanova, M. (2013). Neuroticism and vascular response to mental load. WebmedCentral Physiology, 4(1), WMC003951. https://doi.org/10.9754/journal.wmc.2013.003951
Sun, Y., Zhang, H., Wang, B., Chen, C., Chen, Y., Chen, Y., Xia, F., Tan, X., Zhang, J., Li, Q., Qi, L., Lu, Y., & Wang, N. (2022). Joint exposure to positive affect, life satisfaction, broad depression, and neuroticism and risk of cardiovascular diseases: A prospective cohort study. Atherosclerosis, 359, 44–51. https://doi.org/10.1016/j.atherosclerosis.2022.08.007
Tafet, G. E., & Nemeroff, C. B. (2016). The links between stress and depression: Psychoneuroendocrinological, genetic, and environmental interactions. Journal of Neuropsychiatry and Clinical Neurosciences, 28(2), 77–88. https://doi.org/10.1176/appi.neuropsych.15030053
Thayer, J. F., & Lane, R. D. (2007). The role of vagal function in the risk for cardiovascular disease and mortality. Biological Psychology, 74(2), 224–242. https://doi.org/10.1016/j.biopsycho.2005.11.013
van der Veen, F. M., van der Molen, M. J., van der Molen, M. W., & Franken, I. H. (2016). Thumbs up or thumbs down? Effects of neuroticism and depressive symptoms on psychophysiological responses to social evaluation in healthy students. Cognitive Affective & Behavioral Neuroscience, 16(5), 836–847. https://doi.org/10.3758/s13415-016-0435-2
Vella, E. J., & Friedman, B. H. (2007). Autonomic characteristics of defensive hostility: Reactivity and recovery to active and passive stressors. International Journal of Psychophysiology, 66(2), 95–101. https://doi.org/10.1016/j.ijpsycho.2007.03.014
Verschoor, E., & Markus, C. R. (2011). Affective and neuroendocrine stress reactivity to an academic examination: Influence of the 5-HTTLPR genotype and trait neuroticism. Biological Psychology, 87(3), 439–449. https://doi.org/10.1016/j.biopsycho.2011.06.001
Wang, M., Dai, X., & Yao, S. (2011). Preliminary development of the Chinese big five personality inventory III: Establishment and psychometric test of the brief version. Chinese Journal of Clinical Psychology, 19(04), 454–457. https://doi.org/10.16128/j.cnki.1005-3611.2011.04.004
Williams, P. G., Rau, H. K., Cribbet, M. R., & Gunn, H. E. (2009). Openness to experience and stress regulation. Journal of Research in Personality, 43(5), 777–784. https://doi.org/10.1016/j.jrp.2009.06.003
Wirtz, P. H., Elsenbruch, S., Emini, L., Rüdisüli, K., Groessbauer, S., & Ehlert, U. (2007). Perfectionism and the cortisol response to psychosocial stress in men. Psychosomatic Medicine, 69(3), 249–255. https://doi.org/10.1097/PSY.0b013e318042589e
Xin, Y., Wu, J., Yao, Z., Guan, Q., Aleman, A., & Luo, Y. (2017). The relationship between personality and the response to acute psychological stress. Scientific Reports. https://doi.org/10.1038/s41598-017-17053-2. 7.
Yang, J., Qi, M., Guan, L., Hou, Y., & Yang, Y. (2012). The time course of psychological stress as revealed by event-related potentials. Neuroscience Letters, 530(1), 1–6. https://doi.org/10.1016/j.neulet.2012.09.042
Zhang, W., Yan, K., Lu, Y., Zhang, D., Hong, J., Yuan, L., & Zhang, Y. (2007). The effect of different psychological stressors on responses of sympathetic and parasympathetic nervous systems. Acta Psychologica Sinica, 39(2), 285–291.
Acknowledgements
The authors would like to thank all participants for their generous insight.
Funding
This work was supported by grants from the Project Everest Research Fund for Military Medicine at the Air Force Medical University (grant number 2020ZFB011), Air Force Medical University “Rapid Response” Project (2023KXKT060) and Shaanxi Province Key Research and Development Program (2024SF-YBXM-063).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Mengxin Yin, Huaihuai Yu, Mingxuan Zou, Yuqing He and Xiucha Wang. The first draft of the manuscript was written by Mengxin Yin and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yin, M., Yu, H., Zou, M. et al. The relationship between neuroticism and the acute psychological stress response: Evidence from the autonomic nervous system. Curr Psychol 43, 20153–20164 (2024). https://doi.org/10.1007/s12144-024-05813-z
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-024-05813-z