
Abstract
Stress has been shown to impact significantly on mental and physical well-being, and a key moderator variable in the stress process is continuing to ruminate about emotional upset: rumination serves to prolong elevations in adrenaline and cortisol, resulting in sustained cardiovascular strain and immune compromise. However, inspection of rumination scales suggests a distinction between prospective and retrospective rumination, and their differential contribution to stress and its consequences have not been explored. The aim of the present paper was two-fold: to establish that the two components could reliably be extracted from a widely-used rumination index, and whether their effects on anxiety, depression and physical symptoms could be distinguished. A final study explored their differential effects on self-harming behaviour, where the impact of rumination has already been demonstrated. Results showed that prospective rumination is the better predictor of psychological and physical health. The deleterious effects of stress are primarily associated with chronic rather than acute stress, and in the interests of resolving definitional confusion, the term stress is used in this paper to describe chronic stress and substituting pressure for acute ‘stress’. The distinction provides a justification for defining stress as rumination, since ruminating about emotional upset serves to prolong physiological arousal (fight-or-flight) which would otherwise revert to resting levels.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The negative and often deleterious impact of stress on psychological and physical well-being is well established (see for example Goldberger and Breznitz 1993). The link between stress and illness is mediated primarily by the activation of the hypothalamic-pituitary-adrenal (h-p-a) axis, resulting in elevations in so-called ‘stress hormones’ such as adrenaline and cortisol. Conventionally described as ‘fight-or-flight’, this is an adaptive response, but only in the short term—sustained elevation in adrenaline exerts significant cardiovascular strain, with concomitant potential lesioning of arterial walls and the deposition of fatty plaques (atherosclerosis), while sustained elevations in cortisol compromises immune function by inhibiting production of leucocytes such as natural killer (NK) and T cells (Ahlgren et al. 2009; Yang and Glaser 2000).
There are, however, systematic individual differences in susceptibility to stress, as evidenced by the relatively low proportion of people subsequently diagnosed with post-traumatic stress following exposure to the same incident (Neria et al. 2008). This led to a search for factors that might be involved in moderating the impact of events. These included personality and coping strategies, but the evidence has been inconclusive, attributable in large measure to significant psychometric shortcomings in the assessment tools that have been developed. Coping questionnaires, for example, have been marred by unreliable item-selection procedures, a reliance on an eigenvalue-1 criterion to decide on structure (which invariably leads to the extraction of too many factors—see for example DeVellis 2003), and an absence of confirmatory factor analysis to endorse the obtained structure (Steed 1998; Stemmet et al. 2015).
Perhaps the strongest evidence for the moderating role of personality has come from research on emotional response styles, and emotional rumination in particular has offered unambiguous and replicated evidence for predicting a prolonged physiological stress response, as well as providing an explanatory mechanism for the psychological sequelae of stress (Roger and Najarian 1998; Nolen-Hoeksema and Morrow 1991; Nolen-Hoeksema et al. 1994). The negative effects of stress are primarily associated with chronic as opposed to acute stress, but chronicity is commonly defined in terms of exposure to unusual circumstances where there is no relief from demand, such as amongst those caring for relatives suffering from Alzheimer’s disease (Kiecolt-Glaser et al. 1995).
In more everyday environments demand is normally intermittent, allowing the opportunity for cardiovascular and immune function recovery. However, continuing to ruminate about emotional upsets in these circumstances leads to sustained elevations in adrenal hormone levels—habitual rumination has been shown to impact significantly on cardiovascular and adrenocortical systems following exposure to both laboratory and naturalistic stressors (see for example, Roger and Jamieson 1988; Roger and Najarian 1998; Thomsen et al. 2004).
The Emotion Control Questionnaire (ECQ—Roger and Nesshoever 1987; ECQ2—Roger and Najarian 1989) was developed in a study aimed at isolating personality moderators of the stress response, and included the earliest published rumination scale. The scale was initially entitled ‘rehearsal’, which implied a concern primarily with future events, but was renamed ‘rumination’ to include both retrospective as well as prospective preoccupations with emotional upset. The ECQ inventories included four scales, two of which, benign control and aggression control, were found to be significantly positively correlated and to form part of the extraversion constellation—benign control, for example, is strongly associated with measures of impulsiveness (Roger and Nesshoever 1987). The remaining scale, emotional inhibition, is orthogonal to rumination, and while it has been shown to mediate muscle-tension recovery in a speech preparation paradigm (Kaiser et al. 1995), subsequent studies using the ECQ have confirmed the preeminent role of rumination in a wide range of health-related contexts, including cardiovascular recovery from a laboratory stress manipulation, prolonged cortisol secretion following exposure to a naturalistic stressor, and increased post-partum analgesic demand (Nieland and Roger 1993; Roger and Jamieson 1988; Roger and Najarian 1998).
Since extraversion is not significantly implicated as a stress moderator (Jackson and Schneider 2014) the ECQ questionnaires were subsequently revised in the light of research findings to yield the Inhibition-Rumination Scale (I-RS—Roger et al. 2011), comprising the two orthogonal dimensions of emotional rumination and emotional inhibition. Both this and the earlier measures were developed using an unbiased scenario technique to generate the initial item pool (see for example Forbes and Roger 1999). Exploratory factor analysis was based on a scree plot to indicate how many factors to extract, and the obtained factor structures were endorsed by confirmatory factor analyses of the responses of independent samples (Roger et al. 2011).
The rumination scales from both the ECQ2 and the I-RS are acknowledged to include prospective and retrospective components, but there has been no attempt to date to explore any differential discriminative power between these two components. For example, in their review of anxiety disorders, Craske et al. (2009) note that one of the factors which distinguishes anxiety from depression is that anxiety is defined as an anticipatory fear response, while depression tends to be characterised by a memory bias towards negative events. The authors acknowledge that the distinction between anxiety and depression is not well understood, but in the light of these differences it might be expected that anxiety would be more strongly associated with prospective rumination, and depression with retrospective rumination.
The aim of the present paper was, firstly, to establish the validity of distinguishing factorially between retrospective and prospective rumination. There have been attempts to distinguish between past and future negative preoccupations by labelling the former rumination and the latter worry (for example, Nolen-Hoeksema et al. 2008), and the argument has been buttressed by claiming that even worry about past issues ‘usually’ has implications for effects on future behaviour. However, rumination is equally likely to be based on future concerns, and the case for making this distinction between worry and rumination is so hedged about with qualifiers like ‘usually’ and ‘often’ as to render it unconvincing. To ensure clarity over past and future ruminative orientations, this paper will consequently use retrospective for the former case and prospective for the latter.
Measures of psychological and physical health were included in the studies, and the second aim was to use these data to explore the differential role of retrospective and prospective rumination in relation to depression, anxiety, stress, and the physical symptoms associated with psychological distress. Two studies using independent samples are reported, the first comprising working adults in New Zealand. This sample was used to test whether the retrospective and prospective rumination factors could reliably be distinguished, and to test their differential effects on psychological and physical health. The second sample comprised undergraduate students attending university in London, England, many of whom had not yet entered working life. Having independent samples that differed in age and experience and that were drawn from different cultures (England and New Zealand) meant that the key findings from the first study could be explored in a wider context. Overall rumination scores have been shown to predict deliberate self-harming behaviour (Borrill et al. 2009), and the inclusion of data on self-harming for the participants in Study 2 also allowed these findings to be tested for retrospective and prospective dimensions of rumination. The respondents in the samples were predominantly female, and the analyses were confined to the data obtained from female respondents in both studies.
Study 1
Participants and Data Collection
The sample comprised voluntary working adult female participants recruited in New Zealand, 126 females with a mean age of 38.83 years (range 19–72 years; SD = 11.50). The sample comprised individuals from a wide range of occupations, including education, finance, customer services and local and central government, and participants were obtained primarily through the first author’s professional network. Reliable samples of working adults are notoriously difficult to recruit, and exclusion was restricted to cases where demographic information such as age had not been disclosed or, more importantly, where responses to the package of measures listed below were either incomplete or missing (although this involved fewer than 3% of the overall total).
The data were collected as part of a larger study which included the following self-reported measures of emotional style, coping, and psychological and physical health:
The Inhibition-Rumination Scale (I-RS—Roger et al. 2011) comprises emotional inhibition and emotional rumination, and only the 18-item rumination scale was used in this study. The scale uses a dichotomised true-false format and has been shown to be highly internally consistent (alpha = 0.84; Roger et al. 2011). The mean score for the participants in this study on I-RS rumination was 8.04 (SD = 5.23, range = 0–18).
The Depression, Anxiety and Stress Scales (DASS—Lovibond and Lovibond 1995) is a widely used 42-item self-report measure of depression, anxiety and stress, based on a 4-point Likert scale ranging from 0 = “Did not apply to me at all” to 3 = “Applied to me very much, or most of the time”. Alpha coefficients were high for all three scales (Depression = .91, Anxiety = .84, and Stress = .90), and Lovibond and Lovibond (1995) suggest that scores ranging from 0 to 78 be regarded as ‘normal’, 78–87 as ‘mild’, 87–95 as ‘moderate’, 95–98 as ‘severe’, and 98–100 as ‘extremely severe’ (Crawford and Henry 2003). Mean scores for the Study 1 participants on the DASS were 3.75 (SD = 3.79, range = 0–20) for depression, 3.10 (SD = 3.58, range = 0–19) for anxiety, and 6.27 (SD = 3.93, range = 0–19) for stress.
The Physical Symptoms Inventory (PSI—Spector and Jex 1998) assesses physical symptoms associated with psychological distress, with each of the 18 items in the scale assessing a discrete condition. Respondents are asked to indicate whether they have had no symptoms, had the symptom, or saw a doctor for it in the past 30 days. Totals for each of the latter two categories are summed to provide an index of total symptoms, and the mean total-symptoms score for the participants in Study 1 was 5.50 (SD = 3.12, range = 0–17).
The questionnaires formed part of a secure online package completed by participants, who were offered the opportunity to enter a NZ$100.00 prize voucher draw in order to increase participation in the larger study. Skewness indices of score distributions were <1.90 for all three measures, indicating that they were within the acceptable range (George and Mallery 2010).
Exploratory Factor Analysis
In order to establish whether retrospective and prospective components could be isolated from the I-RS rumination scale, the first step in the analysis was to subject the responses to the scale to exploratory factor analysis (EFA) using SPSS 21. The Kaiser-Meyer-Olkin (KMO: 0.900) measure of sampling adequacy and Bartlett’s Test of Sphericity (p < 0.001) indicated that the data were factorable (Brace et al. 2006), and the scree plot indicated a two-factor structure.
Principal Axis Factoring (PAF) rotated to a direct oblimin terminal solution indicated an unambiguous distinction between the two factors: all items loaded on either Factor 1 (11 items) or Factor 2 (7 items), with Factor 1 reflecting ruminating about the future and Factor 2 ruminating about the past. The two highest-loading items on Factor 1 were item 8 (.732), “For me, the future seems to be full of troubles and problems” and item 9 (.648), “I often feel as if I'm just waiting for something bad to happen”, and the corresponding items on Factor 2 were item 1 (.846), “I remember things that upset me or make me angry for a long time afterwards”, and item 3 (.720), “I get worked up just thinking about things that have upset me in the past”. Eigenvalues for the first two factors were 6.65 and 1.63, respectively, accounting for 46.01% of the cumulative variance.
Since the two factors are both assessing facets of rumination it was anticipated that they would be positively correlated, and although significant, the correlation between them (r = 0.629; p < 0.001) indicated a shared variance of 39.56%. The item loadings are summarised in Table 1.
Confirmatory Factor Analysis
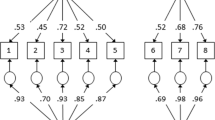
Confirmatory factor analysis (CFA) offers a robust test of the fit of the factor structure obtained from exploratory factor analysis (Brace et al. 2006; Brown 2006; DeVellis 2003). In the present study CFA was based on Amos 22, using the default setting of constraining one of the regression weights for each latent variable to 1.0. Latent variables were allowed to covary freely, and the robust Maximum Likelihood Estimation was used to estimate the fit of the model. The fit indices used to test the model in the present study were Chi-square (χ2: a smaller value is more favourable), the Comparative Fit Index (CFI: >0.90 is good; >0.95 is very good), the Tucker-Lewis Index (TLI: >0.90 is good; >0.95 is very good), and the Root Mean Square Error of Approximation (RMSEA: <0.08 is good; <0.05 is very good). The CFA for the sample clearly endorsed the 2-factor model (χ2 = 165.6, p = 0.033; CFI = 0.956; TLI = 0.950; and RMSEA = 0.043), although one statistical constraint on the findings is that EFA and CFA were conducted on the same sample. Ideally, an independent would be used to cross-validate a factor structure, which might have yielded a less corroborative fit for the CFA results in this study.
Multiple Regression Analysis
A matrix of correlations showed that both retrospective and prospective rumination correlated significantly with all four of the health indices, although the largest of the coefficients (0.625, between prospective rumination and depression) accounted for less than 40% of common variance. Tests for multicollinearity showed that Tolerance (all <0.610) and Variance Inflation Factors (VIF; all <1.66) statistics were acceptable for all coefficients, and to further explore which of the two facets of rumination was a stronger predictor of psychological and physical health, a regression analysis was performed using Factor 1 and Factor 2 from the IR-S as the predictor variables and depression, anxiety, stress and physical symptoms as criterion variables. The overall models were significant for depression (F (2,123) = 39.75, p < .001), anxiety (F (2,123) = 20.17, p < .001), stress (F (2,123) = 28.43; p < .001) and physical symptoms (F (2,123) = 13.67; p < .001), and in each case Factor 1 (ruminating about the future) proved to be the significant predictor. The results of the regression analyses are summarised in Table 2.
Study 2
The second study provided the opportunity to test whether the two-factor structure for rumination would replicate in a sample differing in age, cultural context and employment status, and whether the relationships established between the rumination dimensions and the anxiety, depression, stress indices would be comparable in the second sample. In addition, data were available for deliberate self-harm behaviour amongst the participants in the second sample. Previous studies have established a significant positive correlation between overall rumination and the tendency to self-harm (Borrill et al. 2009). Participants in Study 2 also completed the Deliberate Self-Harm Inventory(DSHI—Gratz 2001), which allowed a more refined test of the relationship by analysing the differential contribution to the effect from retrospective as compared to prospective rumination.
Participants and Data Collection
The 155 female participants (mean age = 19.93 years; SD = 4.05; Range: 18–43) were drawn from a first-year undergraduate student cohort from a university based in the United Kingdom and were offered course credits for taking part in the context of the university’s research participation scheme. The participants completed the same set of scales used in Study 1, except that the Physical Symptoms Inventory was replaced by the Deliberate Self-Harm Inventory (DSHI—Gratz 2001). Of the measures used in Study 1 the Physical Symptoms Inventory, although significantly implicated, showed the weakest relationship to rumination, and overall rumination significantly predicts self-harming behaviour (Borrill et al. 2009).
The DSHI (Gratz 2001) comprises 17 items assessing behaviourally-based self-harm. It is a self-report assessment asking participants to respond ‘yes/no’ to statements exploring the direct destruction of body tissue (Gratz 2001; Sansone and Sansone 2010). The scale has satisfactory internal consistency (alpha coefficient = .82), and re-test reliability over 2 to 4 week intervals was .68 (Gratz 2001). The frequency and severity of self-harm are also reported on the DSHI, and in a study by Gratz (2006), 37% of female psychology undergraduates reported at least one lifetime incident of self-harming. The participants in the present study were drawn from a variety of disciplines, and the corresponding figure of at least one lifetime incident of self-harming was 32.26%.
The mean DHSI score for the participants in the study was 6.58 (SD = 20.45, range = 0–148), and the mean score on I-RS rumination was 8.73 (SD = 4.14, range = 0–17). Mean scores for the three DASS subscales were 5.30 (SD = 4.32, range = 0–19) for depression, 4.57 (SD = 3.70, range = 0–17) for anxiety, and 6.98 (SD = 4.02, range = 0–19) for stress.
Factor Analysis
Exploratory factor analysis (EFA) was run on the data for the sample in Study 2, and again two factors emerged which were unambiguously concerned with prospective rumination and retrospective rumination. The results endorsed the structure that emerged in Study 1, though the factors were not identical: the prospective factor retained 7 of the 11 items extracted in Study 1, with two of the four excluded items (Item 15, “I never get so involved thinking about upsetting things that I am unable to feel positive about the future”, and Item 5, “I seldom get preoccupied with worries about my future”) failing to load on either factor and two (Item 18, “Any reminder about upsetting things brings all the emotion flooding back”, and Item 13, “I don’t let a lot of unimportant things irritate me”) migrating to retrospective rumination. The retrospective ruminations factors in the two studies included the same items except for item 16 (“I worry less about what might happen than most people I know”), which failed to load on either factor in Study 2. The highest-loading item on the prospective factors was the same one for both studies (item 8: “For me, the future seems to be full of troubles and problems”; .693), while the highest and second-highest ranking items on the retrospective factor in Study 1 (Item 1:“I remember things that upset me or make me angry for a long time afterwards”, and item 3:“I get worked up just thinking about things that have upset me in the past”) exchanged rankings on this factor in Study 2 (item 3: .850; item 1: .601) Eigenvalues for the prospective and retrospective factors in Study 2 were 4.486 and 1.762, respectively, accounting for 34.71% of the cumulative variance. The correlation between the two factors was similar to the corresponding coefficient for Study 1 (r = .546; p < 0.001), indicating a shared variance of 29.8%.
Multiple Regression Analysis
The regression analysis performed in Study 1 was repeated, using Factor 1 and Factor 2 from the IR-S as the predictor variables and depression, anxiety, and number of self-reported deliberate self-harm attempts as criterion variables. As was the case with the New Zealand working adult sample, the overall models were significant for depression (F (2,154) = 40.56, p < .001), anxiety (F (2,154) = 15.22, p < .001) and stress (F (2,154) = 24.40; p < .001), and the results were also significant for deliberate self-harm (F (2,154) = 14.74; p < .001). In each case Factor 1 (ruminating about the future) proved to be the significant predictor, and the results are summarised in Table 3.
Discussion and Conclusions
The tendency to ruminate about emotional upset has been shown to act as a significant moderator variable in the stress response. Indeed, the authors would argue that the defining feature of stress is rumination, since continuing to dwell on negative emotion has the effect of prolonging both the psychological experience and the accompanying physiological fight-or-flight response mediated by the h-p-a axis. However, what has not previously been explored is the distinction between retrospective and prospective components of rumination, which are apparent from an examination of the scale items. The first aim of the paper was to establish that there are discrete and discriminable components of rumination, which was demonstrated with exploratory factor analysis, and the unambiguous two-factor structure was endorsed by confirmatory factor analysis. The two factors do form part of a unified construct, but they share clearly discriminable components.
The second aim of the paper was to explore the differential effects of these retrospective and prospective components on psychological and physical well-being. Study 1 used a widely used and researched index of rumination taken from the Inhibition-Rumination Scale (I-RS—Roger et al. 2011), and the dependent variables were measures of depression, anxiety and stress from the Depression, Anxiety and Stress Scales (DASS—Lovibond and Lovibond 1995) and the Physical Symptoms Inventory (PSI—Spector and Jex 1998). Correlating the rumination factors with the outcome variables showed that both retrospective and prospective rumination were significantly associated with all four dependent variables, but refining the analysis using multiple regression showed that only ruminating about the future significantly predicted greater anxiety, depression, stress and physical symptoms. Study 2 extended the research by exploring the differential effects of past and future rumination using a sample that differed in age, experience and culture. The same measures were used as in Study 1, except that the physical symptoms inventory was replaced by a measure of self-harming behaviour. Self-harming has been shown to be predicted by overall rumination scores, and the regression analyses in Study 2 showed that self-harming was predicted by future rumination but not past rumination.
While the results from the two studies were clear-cut, there are a number of factors that might have biased the findings. The samples were relatively small and were exclusively female, so the question of whether the same results would emerge in male samples remains untested. As has been acknowledged, the exploratory and subsequent confirmatory factor analyses in Study 1 should ideally be based on separate independent samples. Study 2 allowed a further exploratory factor analysis of the rumination scale, and the migration of two items from the first factor to the second factor and the omission of two other items suggests that the endorsement of the structure by the confirmatory factor analysis in Study 1 might not be entirely reliable. The two factors that emerged in each of the studies had more similarities than differences, but further confirmatory factor analysis with a new sample in the future would provide further clarification for the structure. The dependent variables were obtained from self-report questionnaires rather than for example clinical diagnoses of depression and anxiety, and a related issue is that the reported effects for retrospective and prospective rumination might have been confounded by correlations between the measures of anxiety and depression. However, while they were significant they were nonetheless moderate, ranging from .474 (22.47% shared variance) to .601 (36.12% shared variance) across the samples.
Overall, it should be borne in mind that the paper was intended as an exploratory study, and despite some sampling and procedural limitations it does provide a clear indication of the importance of distinguishing between retrospective and prospective components of rumination. In the light of the established impact of overall rumination on a wide range of outcomes, the findings offer a significant and psychometrically grounded avenue for future research using the rumination construct.
References
Ahlgren, A. R., Cinthio, M., Steen, S., Persson, H. W., Sjöberg, T., & Lindstrom, K. (2009). Effects of adrenaline on longitudinal arterial wall movements and resulting intramural shear strain: A first report. Clinical Physiology and Functional Imaging, 29, 353–359.
Borrill, J., Fox, P., Flynn, M., & Roger, D. (2009). Students who self-harm: Coping style, rumination and alexithymia. Counselling Psychology Quarterly, 22(4), 361–372.
Brace, N., Kemp, R., & Snelgar, R. (2006). SPSS for psychologists (3rd ed.). Hampshire: Palgrave MacMillan.
Brown, T. A. (2006). Confirmatory factor analysis for applied research. New York: The Guilford Press.
Craske, M. G., Rauch, S. L., Ursano, R., Prenoveau, T., Pine, D. S., & Zinbarg, R. F. (2009). What is an anxiety disorder? Depression and Anxiety, 26, 1066–1085.
Crawford, J. R., & Henry, J. D. (2003). The Depression Anxiety Stress Scales (DASS): Normative data and latent structure in a large non-clinical sample. British Journal of Clinical Psychology, 42, 111–131.
DeVellis, R. F. (2003). Scale development: Theory and applications (2nd ed.). London: Sage Publications Ltd.
Forbes, A., & Roger, D. (1999). Stress, social support and fear of disclosure. British Journal of Health Psychology, 4, 165–179.
George, D., & Mallery, M. (2010). Using SPSS for Windows step by step: A simple guide and reference. Boston: Allyn & Bacon.
Goldberger, L., & Breznitz, S. (1993). Handbook of stress: Theoretical and clinical aspects. NY: Simon & Schuster, The Free Press.
Gratz, K. L. (2001). Measurement of deliberate self-harm: Preliminary data on the Deliberate Self-Harm Inventory. Journal of Psychopathology and Behavioural Assessment, 23(4), 253–263.
Gratz, K. L. (2006). Risk factors for deliberate self-harm among female college students: The role and interaction of childhood maltreatment, emotional inexpressivity and affect intensity/reactivity. American Journal of Orthopsychiatry, 76, 238–250.
Jackson, S., & Schneider, T. S. (2014). Extraversion and stress. In A. D. Haddock & A. P. Rutkowski (Eds.), Psychology of extraversion. NY: Nova Science Publications.
Kaiser, J., Hinton, J. W., Krohne, H. W., Stewart, R., & Burton, R. (1995). Coping dispositions and physiological recovery from a speech preparation stressor. Personality and Individual Differences, 9, 1–11.
Kiecolt-Glaser, J. K., Marucha, P. T., Malarkey, W. B., Mercado, A. M., & Glaser, R. (1995). Slowing of wound healing by psychological stress. Lancet, 346, 1194–1196.
Lovibond, S. H., & Lovibond, P. F. (1995). Manual, for the depression anxiety stress scales. Sydney: Psychology Foundation.
Neria, Y., Nandi, A., & Galea, S. (2008). Post traumatic stress disorder following disasters: A systematic review. Psychological Medicine, 38, 467–480.
Nieland, M., & Roger, D. (1993). Emotion control and analgesia in labour. Personality and Individual Differences, 14, 841–844.
Nolen-Hoeksema, S., & Morrow, J. (1991). A prospective study of depression and distress following a natural disaster: The 1989 Loma Prieta earthquake. Journal of Personality and Social Psychology, 61, 105–121.
Nolen-Hoeksema, S., Parker, L., & Larson, J. (1994). Ruminative coping with depressed mood following loss. Journal of Personality and Social Psychology, 67(1), 92–104.
Nolen-Hoeksema, S., Wisco, B. E., & Lyubomirsky, S. (2008). Rethinking rumination. Perspectives on Psychological Science, 3(5), 400–424.
Roger, D., & Jamieson, J. (1988). Individual differences in delayed heart-rate recovery following stress: The role of extraversion, neuroticism and emotional control. Personality and Individual Differences, 9, 721–726.
Roger, D., & Najarian, B. (1989). The construction and validation of a new scale for measuring emotional control. Personality and Individual Differences, 10, 845–853.
Roger, D., & Najarian, B. (1998). The relationship between emotional rumination and cortisol secretion under stress. Personality and Individual Differences, 24, 531–538.
Roger, D., & Nesshoever, W. (1987). The construction and preliminary validation of a scale for measuring emotional control. Personality and Individual Differences, 8, 527–534.
Roger, D., Guarino de Scremin, L., Borrill, J., & Forbes, A. (2011). Rumination, inhibition and stress: The construction of a new scale for assessing emotional style. Current Psychology, 30, 234–244.
Sansone, R. A., & Sansone, L. A. (2010). Measuring self-harm behavior with the Self-Harm Inventory. Psychiatry, 7(4), 16–19.
Spector, P. E., & Jex, S. M. (1998). Development of four self-report measures of job stressors and strain: Interpersonal conflict at work scale, organizational constraints scale, quantitative workload inventory, and physical symptoms inventory. Journal of Occupational Health Psychology, 3, 356–367.
Steed, L. G. (1998). A critique of coping scales. Australian Psychologist, 33(3), 193–202.
Stemmet, L., Roger, D., Kuntz, J., & Borrill, J. (2015). General and specific avoidance: The development and concurrent validation of a new measure of avoidance coping. European Journal of Psychological Assessment, 31(3), 222–230.
Thomsen, D. K., Mehlsen, M. Y., Hokland, M., Viidik, A., Olesen, F., Avlund, K., Munk, K., & Zachariae, R. (2004). Negative thoughts and health: Associations among rumination, immunity, and health care utilization in a young and elderly sample. Psychosomatic Medicine, 66, 363–371.
Yang, E. V., & Glaser, R. (2000). Stress-induced immunomodulation: Impact on immune defences against infectious disease. Biomedical Pharmacotherapy, 54, 245–250.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval was obtained from the relevant Research Ethics Committees for the samples and no external funding was received for the research.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The Authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Stemmet, L., Roger, D., Kuntz, J. et al. Ruminating about the past or ruminating about the future—which has the bigger impact on health? An exploratory study. Curr Psychol 39, 593–599 (2020). https://doi.org/10.1007/s12144-018-9781-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-018-9781-2