
Abstract
In recent years, ion mobility spectrometry is increasingly in demand for new applications especially on biological samples (cells, bacteria, fungi), in medicine (diagnosis, therapy and medication control e.g. from breath analyses), for food quality control, safety monitoring and characterisation or process control in chemical and pharmaceutical industry. For this purpose instruments based on gas phase separation of ions in weak electric fields were developed at ISAS–Institute for Analytical Sciences, focussing on the particular challenges such as humid and rather complex samples, specific sampling procedures adapted to the application, fast pre-separation techniques like multi-capillary columns and suitable data processing including data bases for relevant analytes and automatic characterisation of IMS-chromatograms. Feasibility studies were carried out successfully for biological and medical purpose at ISAS, including the detection of bacteria, fungi and metabolites of cells and in human breath. For all those samples characteristic pattern of analytes were found and could be used for the identification of cell lines, fungi and bacteria as well as of numerous diseases. Furthermore, the quantification of those analytes could be used to obtain information about the state of the process or person (e.g. growth of cultures, development of diseases, level of medication, grade of cancer). Those examples shall demonstrate the potential of ion mobility spectrometry for the selected applications. However, a general and reliable data bases of reference analytes is required in the near future to enable an exploitation of the metabolic pathways and to confirm the relevance of the detected signals for the investigated topic.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The metabolites of any kind of organism are increasingly subject of investigations as they are a carrier of information about the state of the organism itself, about influences of the environment on the organism and about synergistic effects as well [1–3]. Such organisms can be cells, bacteria or fungi but also human beings. Their metabolites carry information about the surrounding environment, individual nutrition and growth and also about deterioration of the organism like diseases or contamination with bacteria or fungi. Therefore, the metabolites detected could be used for identification and growth control of cell, bacteria or fungi cultures, for bio-process control when micro organisms are involved but also as marker for medical diagnosis and for description of the metabolic status of a patient in general [4–6].
The detection of metabolites in blood or urine is presently based on a variety of mass spectrometric (MS) methods in combination with different separation techniques. Nuclear magnetic resonance has also been described in this area (NMR) and this approach also requires pre-treatment of the samples [7–9]. Comparatively few investigations have been published related to breath analyses or the analysis of the headspace of bacteria, fungi or cell cultures. All of these studies require pre-concentration of the metabolitic analytes [10–13], and as such they are expensive and time consuming. The need for faster systems without compromising sensitivity is self-evident and the set of exemplar studies described in this paper seeks to demonstrate how ion mobility spectrometry coupled to multi-capillary chromatography is a candidate technology that requires serious consideration.
Ion mobility spectrometry is well known as a method for the detection of gas phase analytes first applied for the detection of chemical warfare agents in military use and civil protection [14]. Only few investigations were published on other applications such as biological samples [15–18]. At ISAS–Institute for Analytical Sciences, Dortmund, Germany, ion mobility spectrometry with fast pre-separation techniques was applied for the sensitive detection (lower ppbv down to pptv range) of metabolites in human breath [19, 20] but also for process control and food quality and safety [21–24]. By help of representative examples, the potential of the method for the identification and quantification of metabolic markers of bacteria, cells, fungi and in human breath—including diagnosis, therapy and medication control—will be illustrated.
Experimental
The ion mobility spectrometers (IMS) applied in the present studies were developed and built at ISAS and are described in detail elsewhere [25–27]. A radioactive source (63Ni, 550 MBq) was used to ionise the gas available in the ionisation chamber (synthetic air) thus forming the so-called reactant ions [14, 25]. If an analyte is introduced into the ionisation chamber of an ion mobility spectrometer, the reactant ions transfer their charge e.g. by proton transfer to the analyte molecules. In a weak electric field, the ions start to move towards the detector, a Faraday-plate. In the opposite direction, a so-called drift gas flow is applied which avoids the diffusion of neutral analyte ions into the drift region. Furthermore, the analyte ions collide with the drift gas molecules, thus reducing their drift velocity. The collision rate depends on their size, shape and charge. Therefore, they are—in the ideal case—totally separated when they reach the detector and different ions can be detected after a characteristic drift time which can be used for identification of the analyte. In addition, the signal area can be used for quantification using a calibration carried out earlier for each particular analyte considered. The drift time depends on the ambient conditions and therefore is standardised to temperature and pressure of the drift gas which leads to the so-called reduced ion mobility K o in cm2 V−1 s−1. The experimental parameters of the IMS for all the present studies are summarised in Table 1.
If complex mixtures are subject of IMS analyses, like some hundreds of different metabolites which can be found in human breath samples, the reduced ion mobility alone might not be sufficient for identification of the analytes in the mixture. Several analytes may have the same or almost the same mobility. Therefore, multi-capillary columns (MCC OV-5, Sibertech, Novosibirsk, Russia) were applied for rapid pre-separation. These columns consist of ∼1,000 glass capillaries and enable a high sample flow (150 ml/min) and a rapid separation (∼500 s for 20 cm capillary length operated at 30 °C constant temperature). To avoid contamination of the instrument if the analyte is injected continuously, the sample was introduced into a sample loop of 10 ml volume. Only the volume of the sample loop was injected via a six-way-valve into the MCC.
In addition, the use of MCC avoids negative influence especially when humid samples are analysed. If humidity enters the ionisation region together with the analyte, clustering of the analyte ions with water molecules takes place, thus making identification complicated or even impossible. Using MCC for pre-separation, water molecules and analyte ions enter the ionisation region in the ideal case totally separated and no negative influence can be observed even up to 100% relative humidity [23].
The retention time of the analytes in the MCC gives additional information for the identification of analytes in a complex mixture [20]. The complete information of a 63Ni-MCC-IMS—ion current vs. ion mobility and retention time—is the so-called topographic plot or IMS-chromatogram.
For the detection of the metabolites of cells and bacteria, the headspace of the particular cultures was introduced into the sample loop. For breath analyses, the subjects used a mouth peace to breathe through the sample loop. Before each breath analyses, room air was analysed to avoid misinterpretation if signals from room air were detected in breath too. Furthermore, clean humid air was analysed before each sample to avoid contamination influences on the sample analyses.
Results and discussion
Cells
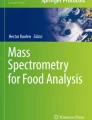
As a first step towards early diagnosis of lung cancer, the metabolites of a cancer cell line were detected in the headspace of a cell culture by the 63Ni-MCC-IMS as described above and compared to the analyses of the medium alone and a non-cancer cell line as well. Figure 1 shows the IMS-chromatogram (ion mobility vs. retention time) of such an analyses—dark colours represent high IMS signal. It was found, that at least two detected metabolites could be identified as characteristic for the cancer cell line—they are marked by a circle in Fig. 1. The next step will be to carry out analyses of the breath of numerous lung cancer patients in various states of lung cancer to identify the relevant metabolites in breath and to optimise the method for a sensitive and early detection [19].

63Ni-MCC-IMS topographic plot of the headspace of a cancer cell line. Some signals were found to be volatiles from the medium or from a non-cancer cell line but at least two metabolites are identified as characteristic for the cancer cell line and are indicated by circles
Bacteria and fungi
The 63Ni-MCC-IMS was used to analyse the headspace of cultures of bacteria and fungi growing on Columbia agar. The IMS chromatograms then were evaluated to identify typical peak pattern for several bacteria and fungi considering the peaks of the volatiles detected from the agar plate alone. The position of the peaks identified in the IMS-chromatogram for Pseudomonas aeroginosa as an example for bacteria and Candida albicans as an example for fungi are shown in Fig. 2. The detected five signals of the bacteria respectively the four signals of the fungi should enable their identification in the breath of an affected patient and the can be used for a pathogen specific diagnosis. In general, characteristic peak pattern of micro-organisms can not only be used for medical purpose but also for the identification of microbial contamination in bio-processes [22, 24, 26].

Characteristic peak pattern detected from 63Ni-MCC-IMS analyses of the headspace of cultures of a bacteria (Pseudomonas aeroginosa) and a fungi (Candida albicans) on Columbia agar
Human breath and diagnosis: healthy subjects
With its characteristics, ion mobility spectrometry should be optimally capable for breath analyses. Obviously, the analyses always have to be compared to analyses of the inhaled room air and of a typical healthy subject before any conclusion on the metabolic state of the patient can be drawn. For the 63Ni-MCC-IMS analyses, the subjects in general were asked to avoid eating, drinking and smoking at least 2 h before the analyses. The topographic plot of a breath analysis of a healthy subject is shown in Fig. 3 as an example. There are only few peaks, all at retention times <5 s which were identified as ammonia, ethanol and acetone by comparison with IMS measurements of reference analytes—natural metabolites which can be found always in human breath. Those peaks are indicated in the drift time spectra at 3 s retention time in Fig. 3.

Topographic plot of the 63Ni-MCC-IMS analyses of the breath of a healthy subject and the spectrum of the same analyses at 3 s retention time. Major signals and the reactant ion peak (RIP) are indicated
Human breath and diagnosis: diabetes
Acetone is well known as a marker for diabetes mellitus and can be identified by comparison with IMS data obtained from the measurement of reference analytes. The signal area as a measure for the concentration of an analyte was determined for the acetone peak of breath analyses of a healthy control group and compared to those of three diabetes mellitus patients in various metabolic states. It was found, that the acetone concentration is significantly higher in the breath of diabetes mellitus patients compared to healthy subjects (see Fig. 4). Further steps will be to validate those results with a higher number of patients and to investigate the diurnal variation of the acetone concentration and the correlation to the blood sugar content. However, the results obtained augur a possible application of IMS as a useful and non-invasive tool for rapid point-of-care diagnostics or for the use of the diabetes mellitus patients at home for control of the metabolic state, in particular the blood sugar content.

Signal area of the acetone peak detected with 63Ni-MCC-IMS in the breath of 30 healthy subjects and three diabetes mellitus patients under varying metabolic conditions
Human breath and diagnosis: sarcoidosis
While diabetes mellitus with the well known marker acetone is an obvious example for the use of IMS as diagnostic tool, most recently characteristic peak pattern could be identified for various diseases [19, 20]. This was done by breath analyses of numerous patients and comparison of the related topographic plots to those of room air and of the breath of healthy patients. Because of the huge amount of data obtained from such investigations, presently statistical tools are being developed to automate peak detection and comparison to data bases containing peak pattern for various diseases. However, those tools as well as the data bases are still under development [19, 28].
An example for such disease characteristic peak pattern is shown in Fig. 5 for sarcoidosis. Three significant peaks were found in the breath of sarcoidosis patients exclusively and were compared successfully to traditional diagnostic tools as used by health professionals. Presently investigations are carried out to identify the responsible analytes which then could be used to explore disease related metabolic processes in detail. Furthermore, the number of patients investigated up to now need to be increased for validation of the findings.

Characteristic peak pattern as detected from the topographic plot of a 63Ni-MCC-IMS analysis of the breath of a patient diseased with sarcoidosis. The peaks characteristic for sarcoidosis are indicated by rectangles
Human breath and diagnosis: lung cancer
A data set of the breath analyses of 36 patients suffering from lung cancer and a control group of 56 healthy subjects was investigated. The huge amount of data (approximately 1,000,000 values per analyses) was reduced considering the signals in relevant peak areas only and by calculating a so-called discriminant value, a statistical tool described in detail elsewhere [28, 29]. By this procedure it was possible to differentiate the healthy subjects from the lung cancer patients with an error of less than 5% (see Fig. 6). Presently further investigations are carried out in the frame of clinical studies to extend the investigations on patients in various states of cancer to enable an early diagnosis of lung cancer, thus increasing the chance of healing significantly.

Discriminant values calculated from the peak pattern in topographic plots of 63Ni-MCC-IMS breath analyses of 36 lung cancer patients and a healthy control group of 54 subjects. A classification and differentiation of these two groups was obtained with an error <5%
Human breath and therapy control: angina lateralis
As disease characteristic peaks can be identified and quantified, it is obvious that the applied method should also be suitable for control of a therapy. If a disease relevant peak can be identified, the signal area of this peak should be related to the state of the disease. Figure 7a shows the topographic plot of a breath analysis of a patient with angina lateralis before any medication was applied—the relevant peak is indicated by a rectangle. Figure 7b shows the drift time spectra at the peak maximum retention time (56 s) and at 24, 48 and 72 h after application of an antibiotic. Figure 7c finally shows the signal area of this obviously declining peak which follows an exponential decrease. By help of such an investigation, the duration as well the success of a therapy applied to a specific disease can be controlled with a rapid and non-invasive method.

63Ni-MCC-IMS topographic plot of a breath analyses of a patient diseased with angina lateralis before medication (a), drift time spectra of the relevant peak during medication (b) and signal area of the peak during medication (c)
Human breath and medication control
Beside the response of a disease (and the related metabolites) some drugs also produce characteristic metabolites which then could be used for control of the level of medication. The exemplar drift time spectra in Fig. 8a shows the three peaks of the metabolites in breath caused by a psychopharmacological medicament. The peaks signal area was determined from breath analyses carried out in steps of approximately 1/2 h for a period of 9.5 h starting 1 h before the application of the medicament. The related peaks increase with a delay of 2 h after the medication and reach a constant level after a steep increase at around 4 h. Therefore, MCC-IMS can also be used as a non-invasive tool for the control of the level of medication

63Ni-MCC-IMS spectra of breath analyses during medication with a psychopharmacological medicament (a) and quantification of the three relevant peaks before and during medication (b)
Conclusions
Ion mobility spectrometers equipped with 63Ni as beta radiation source for ionisation and with additional fast pre-separation by multi-capillary columns (approximately 500 s for a complete separation) were applied for various biological and medical purposes. The headspace of cell, bacteria and fungi cultures was analysed and characteristic peak pattern related to characteristic metabolites could be identified and quantified in sufficient sensitivity. The method enables an identification as well as a statement about the state of the subject of investigation and e.g. the differentiation of cancer and non-cancer cells or different bacteria respectively fungi.
Human breath was a further subject of investigation. It could be demonstrated that ion mobility spectrometry is a promising rapid and non-invasive tool for medical applications such early diagnosis, therapy and medication control. Presently, clinical studies are carried out for further validation of the results, development of data bases for peak pattern for various diseases, for different cell lines and for various bacteria and fungi. Another focus of further investigations will be on the identification of the related analytes. Furthermore, the conversion into commercially available instrumentation for clinical or point-of-care applications is envisaged.
However, the identification of the detected signals found to be significant for the different samples under investigation is required as soon as possible. Therefore a standardised and reliable data bases of reference analytes (retention time and ion mobility) is essential. Presently such a data bases is not commonly available, but is actually under construction at ISAS. Such a data bases will help to exploit the metabolic processes involved and will enable the confirmation of the relevance of the detected signals, then no longer only from statistical evaluation.
References
Kell DB (2006) Systems biology, metabolic modelling and metabolomics in drug discovery and development. Drug Discov Today 11(23–24):1085–1092
Schnackenberg LK, Beger RD (2006) Monitoring the health to disease continuum with global metabolic profiling and systems biology. Pharmacogenomics 7(7):1077–1086
Rochfort S (2005) Metabolomics reviewed: a new “Omics” platform technology for systems biology and implications for natural products research. J Nat Prod 68(12):1813–1820
Smedsgaard J, Nielsen J (2005) Metabolite profiling of fungi and yeast: from phenotype to metabolome by MS and informatics. J Exp Bot 56(410):273–286
Griffin JL, Kauppinen RA (2007) Tumour metabolomics in animal models of human cancer. J Proteome Res 6(2):498–505
de Bruijn I, de Kock MJD, Yang M, de Waard P, van Beek TA, Raaijmakers JM (2007) Genome-based discovery, structure prediction and functional analysis of cyclic lipopeptide antibiotics in Pseudomonas species. Mol Microbiol 63(2):417–428
Lenz EM, Wilson ID (2007) Analytical strategies in metabonomics. J Proteome Res 6(2):443–458
Hodavance MS, Ralston SL, Pelczer I (2007) Beyond blood sugar: the potential of NMR-based metabonomics for type 2 human diabetes, and the horse as a possible model. Anal Bioanal Chem 387(2):533–537
Thevis M, Schanzer W (2007) Mass spectrometry in sports drug testing: structure characterization and analytical assays. Mass Spectrom Rev 26(1):79–107
Libardoni M, Stevens PT, Waite JH, Sacks R (2006) Analysis of human breath samples with a multi-bed sorption trap and comprehensive two-dimensional gas chromatography (GC × GC). J Chromatogr B Analyt Technol Biomed Life Sci 842(1):13–21
Ma W, Liu XY, Pawliszyn J (2006) Analysis of human breath with micro extraction techniques and continuous monitoring of carbon dioxide concentration. Anal Bioanal Chem 385(8):1398–1408
Cho SM, Kim YJ, Heo GS, Shin SM (2006) Two-step preconcentration for analysis of exhaled gas of human breath with electronic nose. Sens Actuators B Chem 117(1):50–57
Wood WL, Higbee DJ, Gooldy M, Glogowski S, Fitzpatrick R, Karalus RJ, Wood TD, Mangino DJ (2006) Analysis of volatile bacterial metabolites by gas chromatography-mass spectrometry. Spectroscopy 21:20–25
Eiceman GA, Karpas Z (2005) Ion mobility spectrometry. CRC, London, UK
Schmidt H, Tadjimukhamedov F, Douglas KM, Prasad S, Smith GB, Eiceman GA (2006) Quantitative assessment and optimization of parameters for pyrolysis of bacteria with gas chromatographic analysis. J Anal Appl Pyrol 76:161–168
Prasad S, Schmidt H, Lampen P, Wang M, Guth R, Rao JV, Smith GB, Eiceman GA (2006) Analysis of bacterial strains with pyrolysis-gas chromatography/differential mobility spectrometry. Analyst 131(11):1216–1225
Tang XT, Bruce JE, Hill HH (2006) Characterizing electrospray ionization using atmospheric pressure ion mobility spectrometry. Anal Chem 78(22):7751–7760
Hill HH, Asbury CH, Wu GR, Matz LM, Ichiye T (2002) Charge location on gas phase peptides. Int J Mass Spectrom 219(1):23–37
Baumbach JI, Westhoff M (2006) Ion mobility spectrometry to detect lung cancer and airway infections. Spectrosc Eur 18(6):22–27
Ruzsanyi V, Baumbach JI, Sielemann S, Litterst P, Westhoff M, Freitag L (2005) Detection of human metabolites using multi-capillary columns coupled to ion mobility spectrometers. J Chromatogr A 1084(1):2145–2151
Baumbach JI (2006) Process analysis using ion mobility spectrometry. Anal Bioanal Chem 384:1059–1070
Vautz W, Baumbach JI, Jung J (2006) Beer fermentation control using ion mobility spectrometry. J Inst Brew 112(2):157–164
Vautz W, Sielemann S, Baumbach JI (2004) Determination of terpenes in humid ambient air using ultraviolet ion mobility spectrometry. Anal Chim Acta 513:393–399
Vautz W, Zimmermann D, Hartmann M, Baumbach JI, Nolte J, Jung J (2006) Ion mobility spectrometry for food quality and safety. Food Addit Contam 23(11):1064–1073
Baumbach JI, Eiceman GA (1999) Ion mobility spectrometry: arriving on-site and moving beyond a low profile. Appl Spectrosc 53(9):338A–355A
Ruzsanyi V, Baumbach JI, Eiceman GA (2003) Detection of the mold markers using ion mobility spectrometry. Int J Ion Mobil Spectrom 6(2):53–57
Soppart O, Baumbach JI (2000) Comparison of electric fields within drift tubes for ion mobility spectrometry. Meas Sci Technol 11:1473–1479
Bader S, Urfer W, Baumbach JI (2007) Reduction of Ion Mobility Spectrometry data by clustering characteristic peak structures. J Chemom 20(3–4):128–135
Bader S, Urfer W, Baumbach JI (2005) Processing ion mobility spectrometry data to characterize group differences in a multiple class comparison. Int J Ion Mobil Spectrom 8:1–4
Acknowledgement
The financial support of the Bundesministerium für Bildung und Forschung and the Ministerium für Wissenschaft und Forschung des Landes Nordrhein-Westfalen is gratefully acknowledged. The co-operation with the Lung Hospital in Hemer, Germany, in particular Dr. Lutz Freitag, Dr. Michael Westhoff and Dr. Patrick Litterst and the participation of all the healthy subjects and patients was essential for the breath analyses investigations. The bacteria and fungi investigations were carried out at the Hygiene-Institut in Iserlohn, Germany. The dedicated work of Luzia Seifert and Susanne Krois, both technicians at ISAS, was indispensable for the success of the investigations as well as the support of Dunja Zimmermann and Michéle Hartmann during the work with the cell lines and of Dr. Jürgen Nolte and Rita Fobbe for the identification of unknown analytes using mass spectrometry. Last but not least, the contributions of Sabine Bader related to data processing and evaluation potentiated the interpretation of the numerous and complex data sets.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vautz, W., Baumbach, J.I. Exemplar application of multi-capillary column ion mobility spectrometry for biological and medical purpose. Int. J. Ion Mobil. Spec. 11, 35–41 (2008). https://doi.org/10.1007/s12127-008-0007-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12127-008-0007-4