
Abstract
Objective
To investigate positioning error analysis of the Fraxion localization system in the intracranial stereotactic radiotherapy of tumors.
Methods
64 patients were divided into two groups: a control group (36 patients with the standard thermoplastic mask) and a model group (28 patients with the Fraxion localization system). 3D images of the treated position were obtained by cone-beam computed tomography (CBCT). Positioning errors were obtained by, respectively, registering these two sets of CBCT images to planning CT images, using a 6°-freedom robotic patient positioning system (HexaPOD Evo RT System). The changes in positioning errors with the Fraxion localization system and with the standard thermoplastic mask were analyzed.
Results
CBCT scan results of the model group showed that the mean of linear error of three directions [superior-inferior (SI), lateral (LAT), and anterior–posterior (AP)] was 0.710 ± 0.676 mm, 0.817 ± 0.687 mm, and 0.710 ± 0.685 mm, respectively. The corresponding PTV was 1.23 mm, 1.26 mm, and 1.36 mm. The differences between the 3D images and the planned CT images were significant (p < 0.001).
Conclusion
The Fraxion radiotherapy system can not only improve the positioning accuracy and reduce positioning errors but also narrow the PTV margin and reduce the radiated volume of normal tissue.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Stereotactic radiotherapy (SRT) is a new technique that can accurately target and cut tumors [1]. It is comprised of two parts, i.e., the equipment and the software. It has been proven to be an effective and safe technique to treat brain metastases [1].
Nevertheless, accurate localization is an important guarantee for the accuracy of stereotactic radiotherapy, and no system is perfect enough to achieve 100% accuracy, even SRT [2]. In stereotactic radiotherapy treatment, a high dose of radiation is delivered to a small target volume within the brain in single or several fractions, normally up to five [3]. It requires high accuracy and precision in patient positioning as well as in delivered dose calculation, to locate the target properly and achieve a high‐gradient dose distribution, reducing the dosage of normal structures [4]. As we all know, inaccurate localization may cause the target area to be missed, and the high-dose area may be transferred to a dangerous organ area, causing serious sequelae and complications [4,5,6]. Therefore, although the accuracy of SRT is relatively higher than other techniques, a more accurate location is required and is crucial for SRT.
The conventional fixation for stereotactic radiosurgery (SRS) treatments is invasive because it is fixed to the skull using fixation screws [7]. Fraxion (Elekta, A.B., Stockholm, Sweden) is the commercial name of the repositioning head frame system designed to overcome the drawbacks of conventional invasive fixation for linac‐based SRS and SRT treatments. This repositioning system is based on the design of the Elekta Extend™ System for Leksell Gamma Knife™ (Elekta, A.B., Stockholm, Sweden), which has been described previously in the literature [8, 9]. The mean interpatient 3D setup error of linac-based SRT was 0.8 mm, and the mean 3D positioning displacement of PFX-SRT in stereotactic coordinates was 2.0 mm [8]. A radial repositioning error of < 1 mm has been achieved [9].
The purpose of this study is to analyze the positioning accuracy of the Fraxion system in the clinical application of brain metastases patients treated by SRT. For this reason, we compared the localization accuracy of the Fraxion system and the standard thermoplastic mask (Klarity, R461ST, Guangzhou, China) system.
Materials and methods
General information of the patients
64 patients with intracranial malignancies from the Affiliated Huaian No. 1 People's Hospital of Nanjing Medical University were selected for this study (from January 2017 to December 2018). Among them, 36 glioma patients (24 males and 12 females, 29–78 years old) who were treated with a thermoplastic mask, were selected as the control group, in which the conventional fractional dose was 200 cGy, and the frequency of treatment was 30 times per patient. 28 patients (17 males and 11 females, 33–71 years old) who were treated with the Fraxion radiotherapy system were selected as the model group in which the therapeutic dose was 400–800 cGy, and the frequency of treatment was 4–10 times per patient.
Position fixation method and CT scans
In the current study, a Versa HD linear accelerator (Elekta, Atlanta, GA, USA), a computer tomography (CT) simulator (PHILIPS Brilliance Big Bore CT), and a Monoca 5.1.1 Treatment planning system (Elekta, Atlanta, GA, USA) were used.
The Fraxion system basically consists of a patient control unit (PCU), and a Fraxion frame with a headrest and front piece. It also includes a unique vacuum mouthpiece and head vacuum cushion which fits into two holes on the bottom of the headrest to achieve accurate and comfortable patient immobilization, which, when combined with partial or full head thermoplastic masks, ensures patient immobilization and positioning accuracy. The PCU provides the necessary vacuum for securing the mouthpiece to the patient's maxilla, thus securely immobilizing the patient. In addition, the PCU is used to form the vacuum cushion. As shown in Fig. 1a, (1) is a bed adapter that can be rotated forward and backward (2° degrees of freedom) for accurate localization, (2) is a dental pad fixation, (3) is a thermoplastic film mask, and (4) is a vacuum pad. Figure 1b is a frame attached to the bed adapter.

The primary components of the Fraxion localization system. a (1) is a bed adapter that can be rotated forward and backward (2° degrees of freedom) for accurate localization, (2) is a dental pad fixation, (3) is a thermoplastic film mask, (4) is a vacuum pad; b a frame attached to the bed adapter
Patients in the model group were placed in a supine position and fixed with a thermoplastic mask and a vacuum pad, while patients in the control group were placed in a supine position and fixed with a standard thermoplastic mask. CT simulation positioning (scanning layer thickness 1 mm) was performed on both groups of patients. Subsequently, the scanned CT images were transmitted to the Monoca radiotherapy planning system and merged with the magnetic resonance images. After sketching the target area and designing the treatment plans, the CT images of the target area were transmitted to the X-ray volume image (XVI) system of the linear accelerator, serving as reference images for registration with the CBCT images.
Data collection
XVI images were obtained through the kV class CBCT of the Versa HD linear accelerator. Patients in the model group were treated with CBCT scans before each treatment for a total of 169 CBCT scans. Patients in the control group were treated with CBCT scans every week before treatment for a total of 169 CBCT scans. After online calibration, the CT images scanned by CBCT and the reference CT images were registered with the gray registration method and underwent a manual fine adjustment to obtain the bony marks and best overlaps of target tumors in the sagittal, coronal and transverse positions. Once applied, the final images and shifts were recorded in the MOSAIQ record and verification system (Elekta Inc, Atlanta, GA, USA).
Statistical methods
Population random (σ) and systematic (Σ) errors were calculated as the mean of the individual random errors and the SD of the individual systematic errors, respectively. The data in this paper were expressed as the mean ± SD. All statistical analyses were performed with SPSS 22.0 statistical software. Differences between groups were determined using the t test and considered at a value of p < 0.05. For calculating the planning tumor volume (PTV), Van Herk’s (2.5 Σ + 0.7 σ) margins calculation was selected [10].
Results
Results of the CBCT scans of all patients
All patients, respectively, received a CBCT scan to acquire two sets of CBCT images, CBCT1 and CBCT2. The positioning errors were obtained by, respectively, registering these two sets of CBCT images to the planning CT images. As shown in Table 1, the positioning errors of the two groups in the three directions are in the respective error ranges. And the range of displacement vector (\(T = \sqrt {X^{2} + Y^{2} + Z^{2} }\)) of the control group and the model group were 1–6 mm and 0–3 mm, respectively.
Analysis of the CBCT scan registration results
The changes in positioning errors between the control group and the model group are shown in Table 2. The positioning errors in the model group in the three directions significantly decreased compared with the standard thermoplastic mask group (p < 0.001), suggesting that the new Fraxion localization system could be fixed better.
Analysis of the PTV margins
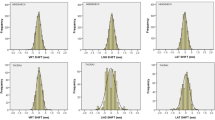
As shown in Table 3 and Fig. 2, the systematic errors and random errors are both reduced significantly compared with the standard thermoplastic mask group (p < 0.001). Accordingly, the PTV margins also significantly decreased compared with the standard thermoplastic mask group (p < 0.001).

Distribution of the planning tumor volume (PTV) margins (mm) in the three directions. Compared with the control group, **P < 0.001
Discussion
In recent years, the incidence of tumors has been increasing year after year. Radiotherapy is one of the main ways to treat tumors. However, in the course of radiotherapy, patients' positioning might change to some extent, leading to the missed exposure of the target area or a large amount of dose deviation to a dangerous area [11,12,13,14]. Although we can use immobilization devices for patient positioning, such as a thermoplastic mask, errors during radiotherapy are inevitable. Thus, monitoring and correcting these errors is very important. At present, the most effective method to reduce error is image-guided radiotherapy. For tumor patients receiving stereotactic radiotherapy, enhancing the accuracy and repeatability of positioning could effectively improve the clinical treatment effect and reduce the incidence of adverse events.
Gamma knife radiosurgery is a single-fraction treatment modality, but the Elekta Extend™ System can expand the range of indications for gamma knife so that patients can benefit from multi- or serial multi-session techniques. The relocatable eXtend frame can provide non-invasive head fixation while maintaining high accuracy, high dose, and the steep gradients associated with GKRS. Astreinidou reported that a rotation error with an average value of at least 1° would not affect the 95% prescription dose [15]. They reported that random translational deviations of 2 mm and rotational deviations of 1° did not affect the CTV (primary) volume receiving 95% of the prescribed dose (V(95)), regardless of the PTV margin used, and there was an additional reduction of 1% when rotational deviations were included. The same effect was observed for the CTV (elective) ipsilateral side. Therefore, they concluded that margins to account for random setup uncertainties should be 1.5 mm and 3.0 mm in the case of sigma = 2 mm and sigma = 4 mm, respectively, for the CTV (primary). In this project, the average of the rotation error of the two fixed methods was less than 1°, so CBCT was chosen to analyze the positioning errors of the two localization systems. In the current study, after registering CBCT images with planning CT images, we found that the positioning errors of the Fraxion group were markedly reduced compared with the standard thermoplastic mask device.
Additionally, we found that the mean values and standard deviations of the Fraxion group were all significantly decreased in the three directions. Besides, we found that the systematic errors and random errors were notably reduced in the Fraxion group. Accordingly, the PTV margins had an expected decrease, which was important for protecting normal tissue. Meanwhile, the reason why the results of PTV in our study were slightly increased as compared with the reports of Majella Russo [16] might be the lack of dental pads in this the Fraxion fixture device. All these findings indicate that the application of the Fraxion radiotherapy system for the fixed position of tumor patients could satisfy the curative precision and repeatability of the target area of radiotherapy and guarantee therapy safety.
Conclusion
The Fraxion radiotherapy system is an important clinical application with very low positioning errors and increasing fractional radiotherapy dose. Thus, it can protect normal functional tissue of the brain and improve the accuracy of radiotherapy.
References
Jeong WJ, Park JH, Lee EJ, Kim JH, Kim CJ, Cho YH. Efficacy and safety of fractionated stereotactic radiosurgery for large brain metastases. J Korean Neurosurg Soc. 2015;58:217–24.
Boman E, Kapanen M, Laaksomaa M, Mäenpää H, Hyödynmaa S, Kellokumpu-Lehtinen PL. Treatment accuracy without rotational setup corrections in intracranial SRT. J Appl Clin Med Phys. 2016;17(4):86–94.
Jin H, Keeling VP, Ali I, Ahmad S. Dosimetric effects of positioning shifts using 6D-frameless stereotactic Brainlab system in hypofractionated intracranial radiotherapy. J Appl Clin Med Phys. 2016;17(1):102–11.
Seravalli E, van Haaren PM, van der Toorn PP, Hurkmans CW. A comprehensive evaluation of treatment accuracy, including end-to-end tests and clinical data, applied to intracranial stereotactic radiotherapy. Radiother Oncol. 2015;116(1):131–8.
Tanaka Y, Oita M, Inomata S, Fuse T, Akino Y, Shimomura K. Impact of patient positioning uncertainty in noncoplanar intracranial stereotactic radiotherapy. J Appl Clin Med Phys. 2020;21(2):89–97.
Russo M, Owen R, Bernard A, Moutrie V, Foote M. Evaluation of accuracy and reproducibility of a relocatable maxillary fixation system for fractionated intracranial stereotactic radiation therapy. J Med Radiat Sci. 2016;63(1):41–7.
Morimoto CY, Mayer MN, Sidhu N, Bloomfield R, Waldner CL. Residual setup error in the canine intracranial region after megavoltage, kilovoltage, or cone-beam computed tomographic image guidance for radiation therapy. Vet Comp Oncol. 2020;18(2):199–205.
Berndt A, van Prooijen M, Guillot M. COMP report: CPQR technical quality control guidelines for Gamma Knife radiosurgery. J Appl Clin Med Phys. 2018;19(5):365–7.
Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand. 1951;102:312–9.
Ruschin M, Nayebi N, Carlsson P, Brown K, Tamerou M, Li W, Laperriere N, Sahgal A, Cho YB, Ménard C, Jaffray D. Performance of a novel repositioning head frame for gamma knife perfexion and image-guided linac-based intracranial stereotactic radiotherapy. Int J Radiat Oncol Biol Phys. 2010;78:306–13.
Sayer FT, Sherman JH, Yen CP, Schlesinger DJ, Kersh R, Sheehan JP. Initial experience with the eXtend System: a relocatable frame system for multiple-session Gamma Knife radiosurgery. World Neurosurg. 2011;75:665–72.
van Herk M. Errors and margins in radiotherapy. Semin Radiat Oncol. 2004;14(1):52–64.
Zollner B, Heinz C, Pitzler S, Manapov F, Kantz S, Rottler MC, Niyazi M, Ganswindt U, Belka C, Ballhausen H. Stereoscopic X-ray imaging, cone beam CT, and couch positioning in stereotactic radiotherapy of intracranial tumors: preliminary results from a cross-modality pilot installation. Radiat Oncol. 2016;11(1):158.
Wang ZY, Zeng ZL, Tan JW. Electron portal imaging device for the correction of set-up error in intensity-modulated radiotherapy for nasopharyngeal carcinoma and its application. Chin J Med Phys. 2017;34(9):887–92.
Astreinidou E, Bel A, Raaijmakers CP, Terhaard CH, Lagendijk JJ. Adequate margins for random setup uncertainties in head-and-neck IMRT. Int J Radiat Oncol Biol Phys. 2005;61(3):938–44.
Russo M, Owen R, Bernard A, Moutrie V, Foote M. Evaluation of accuracy and reproducibility of a relocatable maxillary fixation system for fractionated intracranial stereotactic radiation therapy. J Med Radiat Sci. 2016;63:41–7.
Acknowledgements
We wish to thank all the members in our department for their discussion on this project. Revision E. Fraxion™ User Manual. Medical Intelligence Medizintechnik GmbH. Schwabmünchen. Germany 2013.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to report.
Ethical approval
The current study has been approved by the Ethical Committee of our hospital.
Informed consent
All subjects signed written informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
He, DC., Zhu, ZJ., Zhang, XY. et al. Positioning error analysis of the fraxion localization system in the intracranial stereotactic radiotherapy of tumors. Clin Transl Oncol 23, 43–47 (2021). https://doi.org/10.1007/s12094-020-02382-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12094-020-02382-y