
Abstract
Neonates are obligatory nasal breathers hence nasal obstruction is a very important symptom to be evaluated. Although causes can be trivial most of the time, they can be life-threatening in some. Respiratory distress immediately after birth, feeding difficulties, paradoxical cyanosis, and failure to thrive are the most evident symptoms, and determination of unilateral or bilateral involvement guides the rationale for elective or emergency intervention. This study aimed to evaluate the causes, presentation, and management of neonates with nasal obstruction. We collected the data of all the neonates evaluated for nasal obstruction at our hospital over the past 20 years from June 2003 to May 2023 and assessed the strategy of approach for diagnosis and management of those cases. In our study, the commonest cause for neonatal nasal obstruction was found to be choanal atresia and the rarest was iatrogenic. A variety of other causes were also reported. As neonatal nasal obstruction has a multitude of rare causes each carries a unique assessment and treatment plan. History taking and clinical examination are the most important parts of evaluation including endoscopic evaluation in an office-based setup. Imaging studies add to the evaluation of cases of anatomical obstructions and associated anomalies (syndromes). Early diagnosis and swift intervention can be life-saving. The need for follow-up visits and second-stage corrections should be emphasized in getting the best long-term results.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Neonatal nasal obstruction is a significant cause of respiratory distress as they are obligate nasal breathers for at least 6 weeks to 6 months of life [1]. This can have multiple short and long-term consequences, including breathing difficulty which can be life-threatening, suckling or feeding difficulty, growth issues leading to failure to thrive, and effects on craniofacial development causing cosmetic issues [2,3,4].
The causes can be classified as Congenital (choanal atresia, CNPAS, NLD cysts, midline nasal masses); Neoplastic (teratoma, haemangioma, hamartoma); Inflammatory (allergic, GERD); Infections (viral, bacterial); Traumatic/iatrogenic (birth injuries, instrumentation); Others (metabolic, maternal drug-induced). Association with CHARGE, Apert, Crouzon, Teacher-Collin syndromes, etc. is also documented. Workup includes assessment of severity, establishing a safe airway initially, detailed history, local and systemic examination (for other associated anomalies), endoscopic examination, imaging studies (for more precise knowledge of pathology), and appropriate, adequate & effective management plan [5].
This study aimed to analyze and describe the multitude of causes of neonatal nasal obstruction, modes of presentation, assessment methods, and management strategies adopted at our center over the past years.
Materials and Methods
It was a retrospective study conducted at a quaternary care referral institution in India. Data from all the neonates evaluated for nasal obstruction from June 2003 to May 2023 were analyzed. We included all newborns less than 28 days of life with a documented diagnosis of nasal obstruction by the ENT team. Babies with suspected nasal obstruction in which the cause could not be evaluated due to death or loss of follow-up were excluded from the study. The consent was taken from all the parents for images and video usage for educational purposes. Data was analyzed for etiology, clinical presentation, methods of examination, intervention performed, and complications.
Results & Discussion
A total of 63 cases were seen and the etiology is tabulated in Table 1. Also, the signs and symptoms at presentation ranging from stertor and feeding difficulties to external deformity and association with other anomalies have been tabulated according to the percentage of association. (Table 2). A total of 35% of cases were treated conservatively and the remaining underwent surgical correction. Details of each etiology have been discussed below.
Choanal Atresia (CA)
CA is characterized by congenital obstruction of the posterior nasal aperture, this condition is rare and has an incidence of 1: 7000–8000 live newborns. It is more common in females and more often unilateral [2, 6,7,8]. Obstruction can be partial (stenosis) or complete (atresia) and can be classified as bony or mixed (membranous and bony), explaining 30–70% of cases, respectively [9, 10]. Various theories that have been postulated for the occurrence of this condition [9, 11]: (1) Persistence of the buccopharyngeal membrane from the foregut. (2) Abnormal persistence of mesoderm forming adhesions in the naso-choanal region. (3) Abnormal persistence of the naso-buccal membrane of Hochstetter and (4) Misdirection of neural crest cell migration.
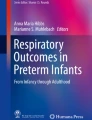
In our series, the diagnosis was confirmed by failure to pass a 6Fr catheter. Nasal endoscopy (Fig. 1) and radiology (Fig. 2) helped in planning the management.

Endoscopic images of–A Bony choanal atresia B Membranous choanal atresia

A Bilateral bony choanal atresia B Bilateral membranous choanal atresia C Mixed bony-membranous atresia
Out of 17 cases, 15 were bilateral and only 2 were unilateral. Bilateral cases presented with respiratory distress immediately after birth and cyclical cyanosis. The patients were stabilized in the NICU & then taken up for surgery. The mean time for surgical correction was 12 days (range-7–20 days) and then regular two weekly follow up with endoscopic evaluation to check the patency of posterior choanal space. Unilateral cases presented with stertor, stuffy nose, and feeding difficulties. Depending on the severity these patients were reassured and followed up, conservatively managed & operated at a later age.
Various approaches and techniques are available for choanal atresia repair. Urethral sounds or Hegars dilators are used to puncture the atretic plate blindly via the nostrils but this has a high restenosis rate [9] and specially not recommended in thick bony atresia or children with CHARGE syndrome [11]. Also, other complications of transnasal puncture include septal or turbinate injury, intranasal adhesion, CSF leakage, and meningitis from inadvertent fracture of the perpendicular plate and/or cribriform plate of ethmoids [12]. Transpalatal CA repair gives good exposure but is associated with complications of palatal flap breakdown, fistula, palatal dysfunction, and velopharyngeal insufficiency [9, 13]. The use of endoscopy for transnasal CA repair was demonstrated first by Stankiewicz [14]. After adequate nasal decongestion, a 2.7 mm Hopkins rigid endoscope is introduced into nose. A laterally based mucosal flap is raised and the bony part of the atretic plate is exposed. The thinnest section of the atresia, found at the junction of the hard palate and vomer below the posterior end of the middle turbinate, is the ideal point of entry into the nasopharynx. The posterior bony septum is also removed and a neounichoana is created [15] using the powered instrument. Laser has been used in endonasal surgery for more than 30 years [9]. Healy et al. first described the feasibility of using CO2 laser in the management of CA [16]. However, bony atresia > 1 mm thick is not amenable to laser ablation. With no significant advantage over conventional powered instruments and increased risk of fire, laser use is not accepted widely [17, 18].
We preferred to use the transnasal endoscopy and drill technique to remove the bony atretic plate of choana and drill as inferior and medial as possible to achieve a safe and good opening (Fig. 3). In our experience raising flaps was difficult with low birth weight babies and in bilateral cases and hence was not done whereas it was effectively possible in older age groups and unilateral cases which we took up for surgery.

Transnasal endoscopic drill technique for choanal atresia repair-A external view, B endoscopic view
After a few initial years of using a stent post-operatively to keep the patency and avoid restenosis, we encountered problems with using a stent-like columella necrosis, stent block, and difficulty breathing and difficulty while breastfeeding the baby as the stent caused breast injuries leading to lot of discomfort and also there was loss of the touch sensation between the baby’s nose and the breast due to which babies started refusing feeds or do not suckle efficiently. Hence we preferred not to use a stent and instead if required electively plan for a re-dilatation after 4 weeks. Several publications [19,20,21,22] and Cochrane review [23] report no difference in patency rates for patients who receive or do not receive stenting after surgery.
Some of the complications we saw post-operatively were due to the usage of drill and endoscope together in a small space causing alar injuries and alar stenosis which was noticed in 2 patients (Fig. 4) in the long term. We devised methods to avoid it by putting a sheath around the drill shaft (Fig. 5), and giving intermittent pauses while drilling.

A Alar injury, B Stenosis post choanal atresia repair by transnasal drill technique

Protection of drill shaft with plastic tubing
Congenital Nasal Pyriform Aperture Stenosis (CNPAS)
CNPAS is determined by bony overgrowth of the nasal process of the maxilla, it is an infrequent cause of neonatal nasal obstruction and its incidence is unknown [2, 6]. It is commonly associated with holoprosencephaly and other congenital midline anomalies such as hypertelorism, flat nasal bridge, a central mega incisor, and pituitary disorders [1]. The pyriform aperture is considered stenotic when the maximum transverse diameter of each aperture is less than or equal to 3 mm or when the pyriform aperture width is less than 8 mm [24].
Management depends on the degree of stenosis and mild cases can be managed with topical vasoconstrictor drops, nasal steroids, and humidification until further growth increases the size of the nasal airway. Surgical management includes a sublabial approach to expose the pyriform aperture and dilate by drilling the lateral and inferior margins.
In our series, 3 neonates presented with tachypnoea, increased work of breathing, nasal alar flaring, and feeding difficulties. Obstruction to the passage of the 5/6F catheter in the anterior inlet raised suspicion of pyriform aperture stenosis. Anterior rhinoscopy showed stenosis in the anterior part, radiology (Fig. 6) confirmed the diagnosis, and all 3 cases were managed conservatively and followed up.

A Axial view showing narrowing at pyriform aperture B Coronal view of CNPAS with development of single central incisor tooth
Nasolacrimal Duct Cysts
Caused by craniocaudal canalization defect of the lacrimal apparatus [25]. It is seen in more than 84% of newborns and in 2–4% of the cases, the obstruction becomes symptomatic of which 80% spontaneously resolve within 6 months [24]. It can present as a nasal mass either external or internal; below the medial canthus or in the inferior meatus. In the case of intranasal cysts, surgery is indicated [26, 27] and marsupialisation, duct probing, and stent placement are the other treatment options [28, 29].
In our series, 3 cases presented with asymptomatic nasal mass (unilateral), and 2 had nasal obstruction (bilateral). Interestingly, the mother noticed the lesion while breastfeeding as a pinkish mass in the nostril. Endoscopy confirmed the diagnosis (Fig. 7) and radiology taken in 1 case showed bilateral nasolacrimal duct obstruction (Fig. 8). Conservative management with lacrimal sac massage, hot compress, and saline nasal wash was done and followed up regularly. Spontaneous resolution occurred in all three.

Nasal endoscopy showing nasolacrimal duct cyst seen just below the inferior turbinate

Axial CT scan showing Bilateral nasolacrimal duct dilation and cysts
Nasal Hypoplasia/Developmental Anomalies
This form of skeletal dysplasias can be due to metabolic, karyotypic, teratogenic, or warfarin embryopathy [24, 30]. It can present with congenital absence of the nose, the spectrum of holoprosencephaly, hypoplasia of the maxilla, and an underdeveloped cartilaginous skeleton of the nose. Management is largely waiting for growth-dependent improvement and avoiding respiratory compromise during this period by temporary nasal stenting or in some cases tracheostomy is needed [31].
In our series of 4 cases 2 partial arrhinia and 1 bifid nostril [Fig. 9] were seen and managed conservatively with plastic surgery correction at a later age. 1 case of complete arrhinia was seen presenting with respiratory distress and cyanosis while feeding. A surgical opening of the right nasal aperture was done and the left was not operated on due to the risk of low skull base seen on the MRI [Fig. 10]. However, the baby died in the course of the hospital stay due to other co-morbid conditions.

A Partial arrhinia B Bifid nostril

A Complete bilateral arrhinia B MRI in complete arrhinia showing low skull base
Midline Fronto-Nasal Mass: Developmental Errors of Anterior Neuropore
Seen 1 in 20,000–40,000 births. It is caused by aberrant embryogenesis of the anterior neuropore with or without skull base defect and carries a risk of intracranial infection [5, 32]. Nasal endoscopy shows the extent of mass and MRI is the imaging of choice. Management is always surgical, and a team approach is necessary combined with neurosurgery, and plastic surgery for the best results.
Meningo-Encephalocele
Characterized by displaced intra-cranial contents through a bony defect in the skull base they contain brain and meninges [1]. They might present with meningitis or CSF leak. Complete resection and meticulous closure of the dural defect are very important. The approach can be endoscopic or combined craniotomy with endoscopic removal.
In our series, 2 cases were seen with clinical presentation of nasal obstruction. Anterior rhinoscopy and endoscopy showed a unilateral mass, varying with a cry (Fig. 11). MRI Imaging confirmed the diagnosis and with combined Neuro and ENT approach, surgical excision and repair of the skull base defect were done.

Nasal endoscopy showing meningoencephalocele
Glioma/Glial Heterotopia
These are isolated extracranial glial tissues that may or may not be connected to the brain by a fibrous stalk [5]. They can present as firm, non-pulsatile, non-compressible masses, not varying with a cry. 15% to 20% are associated with intracranial extension, hence a CT to assess for skull base defect is recommended [1]. Recurrence is seen in 4–10% [33].
In our experience, we had 2 cases, a 1-month-old male baby presenting with internal nasal pinkish firm mass, not varying in size with cry. Both CT and MRI were taken to look for skull base defect and intracranial connection, which was negative, and a combined approach (COMET- combined Microscopic and Endoscopic Technique) surgical excision was done. In this technique initially, microscope-assisted debulking of tissue will be done and later with endoscopic visualization attaching stalk is seen and excised. Follow up was uneventful.
Another 1-month-old male child presenting with feeding difficulties & noisy breathing was also operated and endoscopic resection was done. Histopathology showed mature glial cells with interwoven fibrovascular connective tissue which was consistent with heterotopic central nervous system tissue—Glial Heterotropia (Fig. 12). Minimally invasive endoscopic surgery has emerged as a mainstay for treatment now as angled endoscopes allow improved visualization of cribriform plates.

Nasal endoscopy showing glial heterotopia
Dermoid Cyst
Caused by faulty involution of a neuroectodermal tract through the anterior neuropore, pulling the skin internally leading to the formation of a pit, sinus tract, or cyst with mesodermal and ectodermal components [5]. Intracranial extension has a variable incidence, with 5–45% reported in the literature [34].
In our series, 4 cases were seen presenting with external nasal mass (Fig. 13), 2 with infection of which 1 had pus discharging sinus. Surgical excision and confirmation of diagnosis by histopathology were done.

A Infected dermoid cyst presenting on right nasal dorsum B Surgical removal of dermoid cyst C Dermoid cyst removed in toto
Tumors of Nasal Cavity
They can be benign or malignant with a reported prevalence in the range of 1.7–13.5 cases per 100,000 live births [35]. Teratomas, hamartomas, hemangiomas, neurofibromas are few of the differentials. Teratomas are germ cell tumors with components of 3 embryonic layers. 1 in 40,000 are seen in the head and neck region of which the most common is cervical teratoma followed by nasopharyngeal teratomas [36, 37].
In our study, 2 cases of nasopharyngeal teratoma were seen. A 10-day-old baby with a history of noisy breathing and cyanosis while crying, admitted to NICU was referred to us. A flexible laryngoscopy performed in the NICU showed a mass in the nasopharynx, firm to hard, going into the oropharynx. MRI showed a 1.5*1.7*2.4 cm mass attached to the soft palate (Fig. 14). The trans-nasal, trans-oral approach was adapted for removal and mass excised in toto (Fig. 15). The postoperative period was uneventful and histopathology showed mature teratoma. Another 5-day-old baby with a similar presentation showing a mass in the nasopharynx attached to the roof was resected trans-nasally and found to have glial tissue component along with mature adipocytes and epithelial clusters on histopathology, consistent with teratoma.

MRI imaging showing mass attached to the soft palate

Surgical removal of nasopharyngeal teratoma
Congenital Nasal Septal Deviation
Incidence is seen to be approximately 1% [1] and could be caused by intrauterine nasal compression or trauma during delivery. If significant obstruction is not relieved with conservative measures, then correction can be done by repositioning of septum under general anesthesia.
In our series, 10 cases with septal deviation were encountered and all were managed conservatively with reassurance, saline nasal drops, and topical steroids.
Patent Craniopharyngeal Canal
It is a rare corticated defect through the midline of the sphenoid bone from the sellar floor to the antero-superior nasopharyngeal roof. Prevalent in only 0.42% of the asymptomatic population, it is associated with CSF rhinorrhea, meningitis, rathke’s cleft cyst, infrasellar craniopharyngioma, holoprosencephaly, ectopic pituitary tissue, and other anomalies of skull base [38, 39].
In our case, a mass later identified as craniopharyngioma was seen extending into the nasal cavity and oropharynx (Fig. 16). It was resected completely with transoral & transnasal approach and the post-operative period was uneventful.

A Patent craniopharyngeal canal B Craniopharyngioma extending into the oropharynx
Neonatal Rhinitis
The most common cause of nasal obstruction in the newborn is clinically presenting with nasal obstruction, mucosal edema, and mucous rhinorrhoea [2, 5, 40].
Most commonly managed conservatively by saline drops/steroid drops/short course nasal decongestants, it is self-resolving. Most of them are managed by pediatricians, hence presentation to ENT is very variable. In our series, we had 11 cases, most of which were referred for long-standing rhinitis.
Iatrogenic Nasal Obstruction
Prolonged or inappropriate CPAP (Continuous positive airway pressure) usage; Inadvertent nasal suctioning; and Inappropriate nasal prongs in HFNC (High-flow nasal cannula) are the common causes of iatrogenic nasal obstruction in neonates. The literature review shows a wide spectrum of complications due to Nasal CPAP and upper airway aspirations [41,42,43]. Especially in preterm babies who have fragile skin, CPAP usage for long-term or inappropriate size or poor nursing care and infection control can lead to nasal complications. The spectrum of changes can range from nasal skin redness to skin erosion, ulceration, columellar or tip necrosis, synechiae nasal stenosis, or cosmetic deformity [42, 43]. Synechia formation between septum and turbinate can be seen and the child might have respiratory distress and feeding problems. In our series, 1 case of a baby on prolonged ventilator support and repeated failures in weaning from respiratory support was referred for ENT evaluation and was found to have synechiae which was released endoscopically. Another case of a 32-week-old baby born at 28 weeks presented in OPD with complaints of breathing difficulty and recurrent apnoea episodes. On examination, the baby had a nasal deformity and stenosis with very small anterior nares. History revealed that the baby had nasal tip necrosis after CPAP usage at birth which progressed to involve the whole nasal dorsum followed by fibrosis and stenosis of nasal structure (Fig. 17). The baby was planned for a nasal endoscopy evaluation and possible dilation of nares or choana but unfortunately baby had another episode of apnoea and died.

Nasal dorsum necrosis and stenosis post-CPAP usage in a 28 weeks baby
Conclusion
Choanal atresia is usually treated through a trans-nasal endoscopic approach and may not need stenting. Instead, a repeat endoscopy and dilation are preferred in case of restenosis; Pyriform aperture stenosis can be observed, but severe cases may require surgery. The evaluation of an infant with suspected encephalocele, glioma, or dermoid will require imaging with both computed tomography and MRI. Rare tumors and external developmental deformities need a tailored approach. Inflammatory/benign obstructive pathologies can be managed conservatively. Iatrogenic causes are better to be prevented with proper nursing care. Early diagnosis and swift intervention can be lifesaving and the need for regular follow-up and second-stage corrections ensure the best long-term results. Excellent pre-operative and post-operative supportive care by the NICU team plays a very important role in the prognosis of neonates with nasal obstruction. It is truly a challenging experience to deal with neonatal nasal obstruction and this field needs a lot of research and consensus in bringing out the best management strategies.
References
Valdez TA, Ainsworth T (2012) Neonatal nasal obstruction. American Academy of Pediatrics, pp 109–123
Alvo A, Villarroel G, Sedano C (2021) Neonatal nasal obstruction. Eur Arch Oto-Rhino-Laryngol 278:3605–3611
Leboulanger N (2016) Nasal obstruction in children. Eur Ann Otorhinolaryngol Head Neck Dis 133(3):183–186
Smith MM, Ishman SL (2018) Pediatric nasal obstruction. Otolaryngol Clin North Am 51(5):971–985
Gnagi SH, Schraff SA (2013) Nasal obstruction in newborns. Pediatr Clin N Am 60:903–922
Wyatt M (2018) Neonatal nasal obstruction. In: Watkinson JC, Clarke RW (eds) Scott-Brown’s Otorhinolaryngology and Head and Neck Surgery, vol 2, 8th edn. CRC Press, Boca Raton, pp 251–259
Rajan R, Tunkel DE (2018) Choanal atresia and other neonatal nasal anomalies. Clin Perinatol 45(4):751–767
Myer CM, Cotton RT (1983) Nasal obstruction in the pediatric patient. Pediatrics 72(6):766–777
Kwong KM (2015) Current updates on choanal atresia. Front Pediatr 3:52
Brown OE, Pownell P, Manning SC (1996) Choanal atresia: a new anatomic classifcation and clinical management applications. Laryngoscope 106(1l):97–101
Hengerer AS, Brickman TM, Jeyakumar A (2008) Choanal atresia: embryologic analysis and evolution of treatment, a 30-year experience. Laryngoscope 118(5):862–866
Gujrathi CS, Daniel SJ, James AL, Forte V (2004) Management of bilateral choanal atresia in the neonate: an institutional review. Int J Pediatr Otorhinolaryngol 68(4):399–407
Stieve M, Kempf HG, Lenarz T (2009) Management of choanal atresia in cases of craniofacial malformation. J Maxillofac Oral Surg 8(1):52–54
Stankiewicz JA (1990) The endoscopic repair of choanal atresia. Otolaryngol Head Neck Surg 103(6):931–937
Ibrahim AA, Magdy EA, Hassab MH (2010) Endoscopic choanoplasty without stenting for congenital choanal atresia repair. Int J Pediatr Otorhinolaryngol 74(2):144–150
Healy GB, McGill T, Jako GJ, Strong MS, Vaughan CW (1978) Management of choanal atresia with the carbon dioxide laser. Ann Otol Rhinol Laryngol 87(5 Pt 1):658–662
Ramsden JD, Campisi P, Forte V (2009) Choanal atresia and choanal stenosis. Otolaryngol Clin North Am 42(2):339–352
Yuan HB, Poon KS, Chan KH, Lee TY, Lin CY (1993) Fatal gas embolism as a complication of Nd-YAG laser surgery during treatment of bilateral choanal stenosis. Int J Pediatr Otorhinolaryngol 27(2):193–199
Newman JR, Harmon P, Shirley WP, Hill JS, Woolley AL, Wiatrak BJ (2013) Operative management of choanal atresia. JAMA Otolaryngol Head Neck Surg 139(1):71–75
Van Den Abbeele T, Francois M, Narcy P (2002) Transnasal endoscopic treatment of choanal atresia without prolonged stenting. Arch Otolaryngol Head Neck Surg 128(8):936–940
Gosepath J, Santamaria VE, Lippert BM, Mann WJ (2007) Forty-one cases of congenital choanal atresia over 26 years—retrospective analysis of outcome and technique. Rhinology 45(2):158–163
Uzomefuna V, Glynn F, Al-Omari B, Hone S, Russell J (2012) Transnasal endoscopic repair of choanal atresia in a tertiary care centre: a review of outcomes. Int J Pediatr Otorhinolaryngol 76(5):613–617
Cedin AC, Atallah AN, Andriolo RB, Cruz OL, Pignatari SN (2012) Surgery for congenital choanal atresia. Cochrane Database Syst Rev 15(2):CD008993
Vanzieleghem BD, Lemmerling MM, Vermeersch HF, Govaert P, Dhooge I, Meire F, Mortier GR, Leroy J, Kunnen MF (2001) Imaging Studies in the Diagnostic Workup of Neonatal Nasal Obstruction. J Comput Assist Tomogr 25(4):540–549
Bossche VS, De Vos G, Lemmerling M (2017) CT in a neonate with nasal obstruction. J Belgian Soc Radiol 101(1):25. https://doi.org/10.5334/jbr-btr.1365
Shashy RG, Durairaj V, Holmes JM, Hohberger GG, Thompson DM, Kasperbauer JL (2003) Congenital dacryocystocele associated with intranasal cysts: diagnosis and management. Laryngoscope 113(1):37–40
Davies R, Watkins WJ, Kotecha S, Watts P (2018) The presentation, clinical features, complications, and treatment of congenital dacryocystocele. Eye 32(3):522–526
Patel VA, Landis ZC, Ely AL (2018) Endoscopic management of congenital dacryocystocele. Oper Tech Otolaryngol Head Neck Surg 29(2):55–60
Zhang Y, Fan Y, Fan J, Cui Y (2019) Selection of surgical intervention for congenital dacryocystocele. Eur J Ophthalmol 29(2):158–164
International Working Group on Constitutional Diseases of Bone. (1998) International nomenclature and classification of osteochondrodysplasias (1997). Am J Med Genet 79:376–82
Seguin JH, Baugh RF, McIntee RA (1993) Airway manifestations of chondrodysplasia punctata. Int J Pediatr Otorhinolaryngol 27:85–90
Hughes GB, Sharpino G, Hunt W, Tucker HM (1980) Management of the congenital midline nasal masses: a review. Head Neck Surg 2:222–233
Ajose-Popoola O, Lin HW, Silvera VM, Teot LA, Madsen JR, Meara JG, Rahbar R (2011) Nasal glioma: prenatal diagnosis and multidisciplinary surgical approach. Skull Base Rep 1(2):83–88
Zapata S, Kearns DB (2006) Nasal dermoids. Curr Opin Otolaryngol Head Neck Surg 14:406–411
Woodward PJ, Sohaey R, Kennedy A (2005) A comprehensive review of fetal tumors with pathologic correlation. Radiographics 25:215–242
Anand B, Raman EV, Rakshit SH (2019) Mature nasopharyngeal teratoma in a neonate: case report and a review of literature. Indian J Otolaryngol Head Neck Surg 71(Suppl 3):S1775–S1778
Kountakis SE, Minotti AM, Maillard A et al (1994) Teratomas of the head and neck. Am J Otolaryngol 15:292
Nanjaraj CP, Rajendrakumar NL, Manupratap N, Priyanka SV, Pradeep Kumar CN, Pradeep HN, Sanjay P, Billal S, Chandana V, Kavya BT A rare case of persistent hypophyseal canal with ectopic pituitary teratoma. https://www.eurorad.org/case/16584.
Arey L (1950) The craniopharyngeal canal reviewed and reinterpreted. Anat Record 106:1–16 ((PMID: 15404751))
Olnes SQ, Schwartz RH, Bahadori RS (2000) Diagnosis and management of the newborn and young infant who have nasal obstruction. Pediatr Rev 21(12):416–420
Aykanat A, Çelik HT, Günaydın RÖ, Yiğit Ş (2020) Iatrogenic nasal synechiae in a premature newborn. T J Pediatr 62:505–508
Pascual A, Wielenga JM (2023) Nasal pressure injuries among newborns caused by nasal CPAP: An incidence study. J Neonatal Nurs. https://doi.org/10.1016/j.jnn.2022.09.006
Jatana KR, Oplatek A, Stein M, Phillips G, Kang DR, Elmaraghy CA (2010) Effects of nasal continuous positive airway pressure and cannula use in the neonatal intensive care unit setting. Arch Otolaryngol Head Neck Surg 136(3):287–291
Funding
This research did not receive any specific Grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Study Concept & Design: EVR, DS, SK. Analysis & Interpretation of Data: SK, MK, DS. Drafting of the Manuscript: DS, SK. Critical revision of the manuscript for important intellectual content: EVR, DS, SK, GS. Literature Research & analysis: DS, GS, SK. Statistical Analysis: DS, SK, MK. Study Supervision: EVR, GS.
Corresponding author
Ethics declarations
Declarations
Ethical approval
Ethical committee approval for the study has been obtained.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Shivnani, D., Kobal, S., Kobal, M. et al. Neonatal Nasal Obstruction: A Comprehensive Analysis of Our 20 Years’ Experience. Indian J Otolaryngol Head Neck Surg 76, 2490–2501 (2024). https://doi.org/10.1007/s12070-024-04537-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12070-024-04537-7