
Abstract
Purpose
Congenital nasal obstruction can be a significant cause of respiratory distress in the newborn, given that they are considered to be obligate nasal breathers. Several different causes have been described, which can be broadly classified as anatomical/malformative, non-tumoral masses and cysts, benign and malignant neoplasia, inflammatory/infectious, traumatic/iatrogenic, and miscellaneous. The purpose of this review is to provide updated and useful clinical information for teams involved in neonatal care, especially in a hospital setting.
Methods
A review of the available literature was performed. Studies were sourced from PubMed with searching of relevant headings and sub-headings and cross-referencing.
Results
The most common etiology is inflammatory, which can have different precipitating factors or be idiopathic, a condition known as neonatal rhinitis. On the other hand, some less frequent but nonetheless relevant conditions causing severe nasal obstruction include choanal atresia, midnasal stenosis, and pyriform aperture stenosis. Some cystic lesions, such as dacryocystoceles with intranasal mucocele, can also produce significant obstruction. Diagnosis usually requires a nasal endoscopy and in some cases imaging such as computed tomography. Management includes different medical and surgical strategies and will greatly depend on the etiology and the severity of symptoms.
Conclusion
Congenital nasal obstruction can be a significant cause of respiratory distress in the newborn. The wide spectrum of differential diagnoses requires a thorough knowledge of nasal anatomy, physiology, and pathology; as well as different management strategies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mild nasal congestion is a common finding in neonates, but fortunately clinically relevant nasal obstruction resulting in distress is infrequent. However, it is an important condition to recognize and treat, as newborns are generally considered to be obligate nasal breathers in the first months of life [1,2,3,4,5].
The neonatal pharynx is functionally separated in two compartments, allowing for breathing and swallowing simultaneously [4,5,6,7,8]; as the larynx lies on a more superior position, with the epiglottis reaching closer to the soft palate, creating a respiratory pathway from the nose to the larynx. Milk goes from the oral cavity through two lateral channels towards the piriform sinuses and into the esophagus [2, 4, 5, 8].
Nasal obstruction in the neonate can have multiple short- and long-term consequences, affecting not only breathing—even with potential life-threatening results—but also sucking, growth, and craniofacial development [3, 6, 7, 9]. Severity of symptoms will mainly depend on the degree of obstruction, with complete bilateral blockage causing evident distress, whereas partial, intermittent, and/or unilateral problems will produce milder symptoms, sometimes not diagnosed until later in life.
The aim of this article was to provide a diagnostic approach to nasal obstruction in newborns, describing the most frequent etiologies and their respective treatment strategies.
Assessment
History and physical examination
A thorough clinical history will consider familial genetic disorders and allergies; prenatal background including diseases of pregnancy, sexually-transmitted infections, teratogen exposure, ultrasound findings and other prenatally diagnosed conditions; and birth history including gestational age, method of delivery, trauma, Apgar score, and need of resuscitation maneuvers, among others.
Most clinical features revolve around two main areas, breathing and feeding. Signs related to breathing may include hyponasal cry, nasal stertor, snoring; and signs of increased respiratory effort such as tachypnea, nasal flaring, intercostal indrawing or apneas. A highly suggestive finding is cyclical cyanosis, which intermittently improves with crying as mouth-breathing occurs [1, 6, 7, 10, 11]. Feeding-related signs will include distress or cyanosis while feeding, frequent pauses, and aerophagia with abdominal distention. Failure to thrive is considered a sign of alarm [1, 7, 9].
Increased work of breathing needs to be accounted for and managed promptly, keeping in mind that cyanosis and lethargy can be signs of impending respiratory failure [6].
Physical examination will evaluate for facial asymmetries, deformities or midline defects. Anterior rhinoscopy is performed to assess for malformations, masses or secretions. Airflow can be detected below the nostrils by placing a mirror to look for misting, holding a strand of cotton wool to look for movement, or by auscultation. Some clinicians still attempt to pass a thin 5 or 6 F catheter through the nose into the oral cavity, to demonstrate its patency [6, 7].
Endoscopy
The next step to determine the location and etiology of the obstruction is to perform a nasal endoscopy, using a rigid or flexible scope. This is a simple, minimally invasive, low-risk procedure when performed by a properly trained specialist, which provides relevant information about the anatomy of the nasal cavities [1, 6, 7, 12]. Importantly, if a nasal mass is found, intracranial extension must be ruled out before attempting to obtain a biopsy sample.
Imaging
If clinical and endoscopic evaluation is not sufficient, computed tomography (CT) is the imaging modality of choice in the workup of most causes of neonatal nasal obstruction, as it provides excellent spatial resolution and bone detail. In some cases, it can be useful to perform a nasal toilet with application of topical vasoconstrictor drops 30 min before the exam. On the other hand, magnetic resonance imaging (MRI) provides a better definition of soft tissues and is mainly indicated in nasal masses when intracranial involvement needs to be ruled out [6, 12,13,14,15].
Swallowing assessment
Investigations for deglutition might be indicated in more severe cases, considering breathing–swallowing coordination status. These can include clinical swallowing tests, videofluoroscopy, and/or fiberoptic endoscopic evaluation of swallowing (FEES) [15].
Differential diagnosis
The main causes for nasal obstruction in the newborn can be classified into anatomical/malformative; non-tumoral masses and cysts; benign and malignant neoplasia; inflammatory/infectious; traumatic/iatrogenic; and miscellaneous (Table 1). Anatomical and tumoral etiologies will be often treated surgically, whereas the treatment of inflammatory conditions will be initially oriented to managing the factors precipitating mucosal edema.15 Below we will describe some of the most relevant etiologies, providing general guidelines on diagnosis and management.
Choanal atresia
The congenital obliteration of the posterior nasal aperture is a relatively infrequent condition, with an incidence of 1: 7000–8000 live newborns. It is more common in females and more often unilateral than bilateral [1, 13, 16,17,18,19,20]. Obstruction can be partial (stenosis) or complete (atresia), and can be classified as bony or mixed (membranous and bony), explaining 30–70% of cases, respectively [21, 22].
There are four theories about the pathogenesis of choanal atresia, none universally accepted: persistence of the buccopharyngeal membrane of the anterior foregut; persistence or abnormal localization of mesodermal tissue causing adhesions in the nasochoanal region; persistence of the nasobuccal membrane of Hochstetter; and abnormal migration of cells from the neural crest and mesoderm [19,20,21,22,23,24,25].
Up to 50% can be associated with other congenital anomalies, especially in bilateral cases [16, 18, 26]. One case series reported a second airway anomaly in 34% of cases, such as tracheomalacia, laryngomalacia or subglottic stenosis; and association to craniofacial anomalies in 21% of cases, including CHARGE, Treacher Collins, Pfeiffer and Apert syndromes [26]. Of these, the most frequent syndrome is CHARGE (an acronym for Coloboma, Heart defects, Atresia choanae, Retarded growth, Genital abnormalities and Ear abnormalities) [9, 18, 21]. Given the high rate of coexisting malformations, it is recommended that patients with choanal atresia are studied with echocardiogram, renal ultrasound, and ophthalmological and audiological evaluations [1, 13].
Clinical presentation will mainly depend on whether the obstruction is unilateral or bilateral, and if there are other congenital malformations. Unilateral atresia is characterized by unilateral nasal obstruction and rhinorrhea and is frequently diagnosed later in life, even into adulthood. Bilateral cases manifest early in the neonatal period with upper airway obstruction, respiratory distress, and intermittent cyanosis which deteriorates with feeding and improves when crying. Patients with other congenital anomalies can have complex airway problems, sometimes presenting with more severe and acute symptoms, which could even require a tracheostomy before definitive surgical treatment [1, 13, 19, 21, 27].
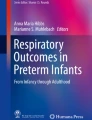
As discussed previously, nasal endoscopy and CT will confirm the diagnosis (Fig. 1), provide anatomical detail and rule out other nasal, skull base or nasopharyngeal anomalies. It is important to also search for temporal bone malformations, as semicircular canal abnormalities are commonly found in patients with CHARGE syndrome [9, 13].

Axial CT showing left-sided choanal atresia (red asterisk)
In bilateral cases, initial management includes securing an oral airway with a McGovern nipple, Guedel airway or orotracheal intubation if required, and orogastric tube feeding [18, 19]. These measures will help stabilize the newborn, allowing for proper assessment of other existing anomalies and surgical planning, which should be performed as soon if the condition of the patient allows it [9, 15]. In unilateral cases, diagnosis and, therefore, treatment are often delayed, but should be ideally resolved before the age of 5 years, to help manage persistent nasal secretion [9]. Definitive surgical treatment can be performed via transnasal puncture, endoscopic transnasal resection, or transpalatal resection.
Transnasal puncture with progressive dilatation is a less complex procedure that has been traditionally described. It has the benefit of easier work in a narrow space, such as the neonatal nasal fossa and although some authors consider it to have high recurrence rates, other studies have not shown significative differences compared to more complex or aggressive procedures [20, 21, 28], especially in atresia with a thin bony component. It has the potential risk of inadvertent damage to nearby structures such as the skull base. Transoral control using a 120° endoscope and the use of drills can help to improve safety and success rates.
Endoscopic transnasal repair allows direct visualization of the atresia and the ability to raise flaps to cover raw areas, aiming to reduce restenosis. It is technically more difficult because of a narrow surgical field, but has similar success rates and less complications than the transpalatal approach, so many authors consider it to be the method of choice [7, 21, 29].
Transpalatal repair is seldom used nowadays, as it is a more aggressive approach. It provides a better exposure at the expense of drilling part of the hard palate, carrying higher risks of postoperative complications such as fistula formation, velopharyngeal insufficiency or altering craniofacial development [19,20,21].
As all techniques carry a risk of postoperative restenosis, complementary use of stents or mitomycin C are sometimes advocated, although evidence of their effectiveness is controversial [19, 21, 29].
Pyriform aperture stenosis
The pyriform aperture is the narrowest part of the bony nasal airway; thus, even a small decrease on its cross-sectional area can determine significative increase in resistance and respiratory difficulties. Congenital stenosis is determined by overgrowth of the nasal process of the maxillary bone [1, 30]. It is an infrequent cause of neonatal nasal obstruction and its incidence is unknown [31]. This can be an isolated condition or can be part of a spectrum of midline anomalies and holoprosencephaly and sometimes associated with the presence of a single central mega-incisor tooth [32, 33].
Clinical presentation is similar to choanal atresia and can be suspected by a difficult intranasal examination because of a narrow anterior bony nasal aperture [32]. Diagnosis can be confirmed with a CT scan showing an aperture diameter < 11 mm (in a term neonate), measured at the level of the inferior turbinate in an axial plane [34]. If associated anomalies are suspected, investigations may include endocrine and electrolyte tests, and a brain MRI [6, 31].
After establishing a secure airway when needed, specific treatment will depend on symptom severity rather than size of the stenosis [30, 35]. Mild cases can be managed with topical treatment using saline solution, intranasal steroids and/or decongestants [1]. Surgical treatment involves enlarging the pyriform aperture through a sublabial approach and will be indicated in patients with poor response to medical treatment, persistent respiratory distress or failure to thrive [1, 11, 32]. This technique is safe, avoids visible scars and provides immediate results [36], although craniofacial dysmorphisms and neurological abnormalities can be associated with decreased outcomes [30]. Some surgeons will use postoperative stents for a few days, to prevent cicatricial stenosis [32, 35, 36].
Midnasal stenosis
Less commonly described condition characterized by bilateral narrowing of the middle part of the nasal fossae, secondary to an uneven growth of the lateral walls of the nose or an excessive infolding of the nasal septum [1, 14, 37]. It is often seen in children with midface hypoplasia such as in Apert or fetal alcohol syndrome [5, 37]. Clinical manifestations are similar to other causes of neonatal nasal obstruction. Nasal endoscopy will reveal a stenotic nasal fossa, past the pyriform aperture, that does not allow visualization of the middle turbinate [14, 37]. Diagnosis will be confirmed with a CT scan, showing a bony narrowing of the midpart of the nasal fossae.
Conservative management with saline drops is indicated in most cases, to allow midfacial growth to relieve the obstruction, usually around 6 months of age [1, 5]. Surgical treatment is reserved for patients with respiratory distress or failure to thrive and generally involves mechanical dilatations or endoscopic inferior turbinate lateralization [1, 14, 37]. The latter technique is safe and decreases the risk of mucosal injury. Some authors recommend a short-term period of postoperative stenting, with early removal aiming to avoid complications such as obstruction, migration, infection and pressure injuries, among others [14].
In severe cases, such as those associated with some craniosynostoses, an adequate nasal airway might not always be achieved, so upfront discussions about expectations with the family and close follow-ups are required. Sometimes, additional procedures—including a tracheostomy—might be necessary.
Dacryocystocele
The nasolacrimal duct allows drainage of tears from the medial canthus into the inferior meatus of the nasal cavity [1, 38]. Defective lacrimal drainage is frequent, affecting up to 20% of newborns, but often self-resolving before the first year of age [39]. However, when congenital distal obstruction at the level of Hasner’s valve is accompanied by a proximal obstruction, a cystic lesion, called dacryocystocele, can result [1, 38]. This is an uncommon and severe form of nasolacrimal duct obstruction, which is unilateral in 90% of cases and usually presents within the first days or weeks of life [40, 41].
On examination, a gray-blue mass inferior to the medial canthus can be noted, usually associated with epiphora or mucopurulent discharge. Manual compression does not show tear reflux, confirming a closed system [41] Secondary infection occurs in 25–50% of patients [40, 42, 43].
Anterior rhinoscopy must be performed to rule out association with an intranasal component, which can cause nasal obstruction in up to 20% [41, 42]. If bilateral, this can lead to severe respiratory distress in a newborn. As for imaging, CT can be used to confirm the diagnosis (Fig. 2a, b) [1, 41].

Congenital dacryocystocele with intranasal mucocele. a Axial CT showing a right-sided congenital dacryocystocele (red asterisk). b Coronal CT showing the intranasal mucocele (blue cross)
Conservative management includes nasal decongestants, warm compresses and massage and can be effective in up to 85% of cases within the first 3 weeks. In case of intranasal cyst, nasal obstruction or treatment failure, surgery is indicated [5, 41, 42]. Alternatives include duct probing and irrigation; endoscopic marsupialization and endoscopic intranasal dacryocystorhinostomy [38, 44] Intranasal components should receive endoscopic treatment [41], and marsupialization is often a straight-forward procedure.
Neonatal rhinitis and inferior turbinate hypertrophy
Rhinitis is the commonest cause of nasal obstruction in the newborn, clinically presenting with nasal obstruction, mucosal edema and mucous rhinorrhea, producing obstruction by itself or exacerbating another condition [6, 12]. Although symptoms are often mild and self-resolving, it can occasionally cause significant distress.
Neonatal rhinitis refers to an idiopathic condition, differentiating itself from other etiologies such as gastroesophageal reflux [6], cow’s milk protein allergy or hypothyroidism [12, 45]; infectious diseases like upper respiratory tract viruses, chlamydia or syphilis;1 or maternal causes like estrogen stimulus or medications including methyldopa, propranolol and tricyclic antidepressants [12, 46].
Examination will reveal mucosal edema, and imaging is often not required [5, 47] Initial management considers saline drops and suctioning [3, 5]. Although off-label, short-term use of topical decongestants and/or courses of intranasal steroids have been empirically used and described in the literature [47,48,49], and can help to stabilize more severe cases or to avoid aggressive procedures. On the other hand, some caution should be exerted with these medications, as newborns might be more susceptible to adverse effects [50].
It is not well defined if congenital inferior turbinate hypertrophy can be considered as part of neonatal rhinitis or if it constitutes a separate entity. Anyways, in case of treatment failure and severe ongoing obstruction, after ruling out other causes, there can be a role for surgery [51]. This could include intranasal dilatation, inferior turbinate lateralization or turbinoplasty. Temporary use of nasopharyngeal airway cannulas can also be considered.
Conclusions
Congenital nasal obstruction can be a significant cause of respiratory distress in the newborn. As such, it is important to accurately and promptly recognize, diagnose and treat these conditions. The wide spectrum of differential diagnoses requires a thorough knowledge of nasal anatomy, physiology and pathology; as well as different management strategies. There are some limitations to this review, as some of these conditions are relatively infrequent and not all treatment strategies are supported by good quality evidence. Further studies are required on the safety and efficacy of topical nasal treatments and coadjuvant measures such as postoperative mitomycin C and stenting.
References
Wyatt M (2018) Neonatal nasal obstruction. In: Watkinson JC, Clarke RW (eds). Scott-Brown’s Otorhinolaryngology and Head and Neck Surgery. 8th Ed. Boca Raton:CRC Press 2 251–9
Moss ML (1965) The veloepiglottic sphincter and obligate nose breathing in the neonate. J Pediatr 67(2):330–331
Leboulanger N (2016) Nasal obstruction in children. Eur Ann Otorhinolaryngol Head Neck Dis 133(3):183–186
Gaultier C, Denjean A (2008) Developmental Anatomy and Physiology of Respiratory System. In: Taussig LM, Landau LI (eds). Pediatric Respiratory Medicine. 2nd Ed. St Louis:Mosby, 15–35
Adil E, Huntley C, Choudhary A, Carr M (2012) Congenital nasal obstruction: clinical and radiologic review. Eur J Pediatr 171(4):641–650
Gnagi SH, Schraff SA (2013) Nasal obstruction in newborns. Pediatr Clin North Am 60(4):903–922
Rodríguez H, Cuestas G, Rodríguez M, Rodríguez J (2016) Algoritmo para el manejo de la obstrucción nasal en neonatos y lactantes. Arch Argent Pediatr 114(5):477–484
Dickison AE (1987) The normal and abnormal pediatric upper airway Recognition and management of obstruction. Clin Chest Med 8(4):583–596
Smith MM, Ishman SL (2018) Pediatric nasal obstruction. Otolaryngol Clin North Am 51(5):971–985
Manica D, Smith M, Schweiger C, Silva D, Kuhl G (2009) Nasal obstruction of the newborn: a differential diagnosis. Int Arch Otorhinolaryngol 13(3):340–345
Patel VA, Carr MM (2017) Congenital nasal obstruction in infants: a retrospective study and literature review. Int J Pediatr Otorhinolaryngol 99:78–84
Olnes SQ, Schwartz RH, Bahadori RS (2000) Diagnosis and management of the newborn and young infant who have nasal obstruction. Pediatr Rev 21(12):416–420
Rajan R, Tunkel DE (2018) Choanal atresia and other neonatal nasal anomalies. Clin Perinatol 45(4):751–767
Syed KA, Raja K, Kolethekkat AA, Varghese AM, Al Abri R, Kurien M (2016) Congenital midnasal stenosis: a novel technique for management. Int J Pediatr Otorhinolaryngol 87:117–120
Sohal M, Schoem SR (2016) Disorders of the neonatal nasal cavity: fundamentals for practice. Semin Fetal Neonatal Med 21(4):263–269
Myer CM, Cotton RT (1983) Nasal obstruction in the pediatric patient. Pediatrics 72(6):766–777
Carpenter RJ, Neel HB (1977) Correction of congenital choanal atresia in children and adults. Laryngoscope 87:1304–1311
Keller JL, Kacker A (2000) Choanal atresia, charge association, and congenital nasal stenosis. Otolaryngol Clin North Am 33(6):1343–1351
Ramsden JD, Campisi P, Forte V (2009) Choanal atresia and choanal stenosis. Otolaryngol Clin North Am 42(2):339–352
Hengerer AS, Brickman TM, Jeyakumar A (2008) Choanal atresia: Embryologic analysis and evolution of treatment, a 30-year experience. Laryngoscope 118(5):862–866
Kwong KM (2015) Current updates on choanal atresia. Front Pediatr 3(June):1–7
Brown OE, Pownell P, Manning SC (1996) Choanal atresia: a new anatomic classification and clinical management applications. Laryngoscope 106(1l):97–101
Flake CG, Ferguson CF (1964) Congenital choanal atresia in infants and children. Ann Otol Rhinol Laryngol 73:458–473
Stankiewicz JA (1990) The endoscopic repair of choanal atresia. Otolaryngol Head Neck Surg 103(6):931–937
Hengerer AS, Strome M (1982) Choanal atresia: a new embryologic theory and its influence on surgical management. Laryngoscope 92(8):913–921
Burrow TA, Saal HM, De Alarcon A, Martin LJ, Cotton RT, Hopkin RJ (2009) Characterization of congenital anomalies in individuals with choanal atresia. Arch Otolaryngol Head Neck Surg 135(6):543–547
Patel VA, Carr MM (2018) Transnasal repair of congenital choanal atresia. Oper Tech Otolaryngol Head Neck Surg 29(2):77–82
Al-khatib T, Haneef SH, Alhusaini OA et al (2019) Transnasal puncture technique vs endoscopic transnasal choanal atresia repair. J Otolaryngol ENT Res 11(2):124–127
Durmaz A, Tosun F, Yildirim N, Sahan M, Kivrakdal C, Gerek M (2008) Transnasal endoscopic repair of choanal atresia: results of 13 cases and meta-analysis. J Craniofac Surg 19(5):1270–1274
Gonik NJ, Cheng J, Lesser M, Shikowitz MJ, Smith LP (2015) Patient selection in congenital pyriform aperture stenosis repair - 14 year experience and systematic review of literature. Int J Pediatr Otorhinolaryngol 79(2):235–239
Castaño JE, Chi DH (2018) Pyriform aperture stenosis repair in infants. Oper Tech Otolaryngol Head Neck Surg 29(2):51–54
Lee WT, Koltai PJ (2003) Nasal deformity in neonates and young children. Pediatr Clin North Am 50(2):459–467
Shah GB, Ordemann A, Daram S, Roman E, Booth T, Johnson R et al (2019) Congenital nasal pyriform aperture stenosis: analysis of twenty cases at a single institution. Int J Pediatr Otorhinolaryngol 126:109608
Belden CJ, Mancuso AA, Schmalfuss IM (1999) CT features of congenital nasal piriform aperture stenosis: initial experience. Radiology 213(2):495–501
Lin KL, Lee KS, Yang CC, Hsieh LC, Su CH, Sun FJ (2016) The natural course of congenital nasal pyriform aperture stenosis. Laryngoscope 126(10):2399–2402
Sessena E, Leporati M, Brevi B, Oretti G, Ferri A (2009) Congenital nasal pyriform aperture stenosis: diagnosis and management. Ital J Pediatr 38:28
Raghavan U, Fuad F, Gibbin KP (2004) Congenital midnasal stenosis in an infant. Int J Pediatr Otorhinolaryngol 68(6):823–825
Patel VA, Landis ZC, Ely AL (2018) Endoscopic management of congenital dacryocystocele. Oper Tech Otolaryngol Head Neck Surg 29(2):55–60
Mac Ewen CJ, Young JDH (1991) Epiphora during the first year of life. Eye 5(5):596–600
Mansour AM, Cheng KP, Mumma JV, Stager DR, Harris GJ, Patrinely JR et al (1991) Congenital dacryocele: a collaborative review. Ophthalmology 98(11):1744–1751
Shashy RG, Durairaj V, Holmes JM, Hohberger GG, Thompson DM, Kasperbauer JL (2003) Congenital dacryocystocele associated with intranasal cysts: diagnosis and management. Laryngoscope 113(1):37–40
Davies R, Watkins WJ, Kotecha S, Watts P (2018) The presentation, clinical features, complications, and treatment of congenital dacryocystocele. Eye 32(3):522–526
Lee MJ, Park J, Kim N, Choung HK, Khwarg SI (2018) Conservative management of congenital dacryocystocele: resolution and complications. Can J Ophthalmol 54(4):421–425
Zhang Y, Fan Y, Fan J, Cui Y (2019) Selection of surgical intervention for congenital dacryocystocele. Eur J Ophthalmol 29(2):158–164
Najjar S (1962) Respiratory manifestations in infants with hypothyroidism. Arch Dis Child 37(196):603–605
Le Gras MD, Seifert B, Casiro O (1990) Neonatal nasal obstruction associated with methyldopa treatment during pregnancy. Am J Dis Child 144(2):143–144
Nathan CAO, Seid AB (1997) Neonatal rhinitis. Int J Pediatr Otorhinolaryngol 39(1):59–65
Harley EH (1991) Neonatal Rhinitis. Arch Otolaryngol Head Neck Surg 117(7):709
Tolley NS, Ford G, Commins D (1992) The management of neonatal rhinitis. Int J Pediatr Otorhinolaryngol 24(3):253–260
Gopalakrishnan S, Sodhi K (2016) Recurrent apnea in a neonate following intranasal oxymetazoline. Indian Pediatr 53(4):353
Kwok J, Leung MK, Koltai P (2007) Congenital inferior turbinate hypertrophy: an unusual cause of neonatal nasal obstruction. Int J Pediatr Otorhinolaryngol Extra 2:26–30
Acknowledgements
We would like to thank Mr. Graeme van der Meer, pediatric otolaryngologist at Starship Children’s Hospital (Auckland, New Zealand) for revising this article.
Funding
No funding was received for this article.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no potential conflicts of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Alvo, A., Villarroel, G. & Sedano, C. Neonatal nasal obstruction. Eur Arch Otorhinolaryngol 278, 3605–3611 (2021). https://doi.org/10.1007/s00405-020-06546-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-020-06546-y