
Abstract
Thiopurine methyltransferase (TPMT) gene polymorphism regulates thiopurine therapeutic efficacy and toxicity. The aim of this study was to determine the influence of TPMT gene polymorphism in Egyptian children with acute lymphoblastic leukaemia (ALL). Sixty-four patients with ALL, T lineage (27%) and pre-B phenotype (73%), who were treated with BFM 90 or CCG 1991 standard risk protocol, and who also experienced myleosuppresion toxicity and required interruption and/or modification of thiopurine chemotherapy were recruited over a year period. Thirty-two patients were on maintenance and another 32 completed their chemotherapy. Seventy healthy age-matched and sex-matched children served as controls. They were subjected to clinical assessment, haematological panel investigations and TPMT gene polymorphism for G238C, G460A and A719G alleles assessment using PCR followed by RFLP analysis. Although none of the studied patients had the mutant TPMT variant alleles, myelosuppression toxicity in the form of different degree of neutropenia was detected in all patients. As a result of myelosuppression toxicity, most of the patients needed 6-MP dose modification either once (53.1%), twice (15.6%), or \(\ge \) thrice (25.1%) during their maintenance course and 96.9% of the patients required to stop 6-MP for less than a week (62.5%), up to 2 weeks (28.1%), or \(> 2\) weeks (6.3%). Patients also developed infection who mostly (71%) needed hospitalization. None of the studied G238C, G460A and A719G TPMT variant alleles were detected. Infections and febrile neutropenia were common causes of 6-PM dose modification and interruption.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Polymorphisms in key genes were involved in drug transport, metabolism, or targeting have been responsible for the variable response to drugs. Further, pharmacogenetic variants can influence response and toxicity of therapy in children with acute lymphoblastic leukaemia (ALL) (Davies et al. 2008). The best-studied example is the gene thiopurine methyltransferase (TPMT) that modifies metabolism of 6-mercaptopurine (6-MP) (Evans et al. 2001), which is a purine antimetabolite widely used in the treatment of ALL, especially in maintenance therapy (Pui and Evans 2006).
The TPMT is a cytoplasmic enzyme that catalyzes the S-methylation of thiopurine drugs, such as 6-MP and 6-thioguanine to inactive metabolites. The human TPMT gene exhibits genetic polymorphism and its activity shows wide interindividual differences because of a common genetic polymorphism that tend to be expressed stably within a given population and typically inherited as autosomal codominant or autosomal recessive traits (Krynetski and Evans 1998; Samochatova et al. 2009).
Variation in TPMT activity regulates toxicity and therapeutic efficacy of thiopurine drugs (McLeod et al. 1994; Krynetski et al. 1996; Yates et al. 1997). Polymorphisms that reduce the activity of TPMT are an important contributor to adverse reactions to conventional doses of thiopurines (Samochatova et al. 2009). Patients with a homozygous deficiency of TPMT, who are treated with thiopurine derivatives at a standard therapeutic oral dosage, 6-thioguanine nucleotides will accumulate, usually within 4–6 weeks, to toxic concentrations. They may experience profound, long-lasting cytopenia, infectious complications, prolonged interruption of their maintenance treatment, and consequently risk of treatment failure (Fujita and Sasaki 2007). Consequently, they could be treated at a reduced dosage of thiopurines without decreasing the cytostatic effect or reducing the likelihood of survival (Relling et al. 1999).
Current genotyping methods allele-specific polymerase chain reaction (PCR) allow the detection of variant TPMT genotypes with more than 95% accuracy and can be used for the molecular diagnosis of TPMT deficiency or heterozygosity (Schaeffeler et al. 2004). Accordingly, TPMT genotyping prior to mercaptopurine therapy has a significant clinical impact on dosage optimization of this drug (Schaeffeler et al. 2004). Four variant TPMT alleles have been identified (TPMT*2, TPMT*3A, TPMT*3B and TPMT*3C) and account for around 80% of Caucasians with low or intermediate TPMT activity (Otterness et al. 1997). We aimed to determine the frequency of these common gene polymorphisms in Egyptian children with ALL and its correlation with chemotherapy response and toxicity. This consequently may provide a stronger scientific basis to identify patients who are at high risk for developing toxicity based on each patient’s genetic constitution that could be used to individualize drug treatment.
Subjects and methods
The present study recruited 64 patients of 150 ALL patients who were attending haematology/oncology clinic, Children’s Hospital, Ain Shams University over a year period. The inclusion criteria were patients with ALL, whose initial diagnosis was based on peripheral blood and bone marrow examination, and immunophenotyping with all markers evaluated by direct immunofluorescence, and cytochemical staining with myeloperoxidase. The recruited patients who were treated with standard risk BFM 90 or CCG 1991, should have had experienced myleosuppresion toxicity in the form of neutropenia and infections, and required interruption and/or modification of thiopurine chemotherapy.
Seventy clinically healthy age-matched and sex-matched children were recruited as controls, they were presented with acute illness to our outpatients’ clinic of Ain Shams University Children’s Hospital. Their ages ranged from two to 15 years and they had no personal or family history suggestive of leukaemia.
The study was approved by The Ethical Committee of the Pediatric Department, Faculty of Medicine, Ain Shams University. Informed consent was obtained from the patients or their legal guardians to participate in the study.
All the studied ALL patients were subjected to detailed history and clinical examination stressing on patient’s demographic data including age at diagnosis and sex; and presenting symptoms and signs of leukaemia such as fever, purpura and organomegaly, stage of therapy, duration of therapy. Further, fillies were revised for history of viral hepatitis and liver function tests, ALT and AST were recorded.
Adverse events during treatment that suggest myleosuppression were recorded, these included infections whether or not necessitate hospital admission and fever that defined as body temperature between 38.1 and \(40.0{^{\circ }}\hbox {C}\) with or without neutropenia. Decrease absolute neutrophil count (ANC) that were categorized into mild \({<} 1500 - {>}1000\), moderate \({<}1000 - {>} 500\), and severe \({<}500\) (Hann et al. 1997) were recorded, where complete blood count (CBC) was done according to hospital protocol every month or as otherwise when clinically indicated.
During the course of therapy, 6-MP dose modification and interruption were recorded. On both protocols, BFM 90 and CCG 1991 and during maintenance therapy patients received daily doses of oral 6-MP (\(75\,\hbox {mg}/\hbox {m}^{2}\)) and dosage were adjusted only in maintenance therapy to keep ANC between 750 per \(\mu \hbox {L}\) and 1500 per \(\mu \hbox {L}\) and platelet count >75,000 per \(\mu \hbox {L}\), the dose of 6-MP was not adjusted on the bases of TPMT genotype.
TPMT gene polymorphism was detected by PCR with subsequent amplification and restriction fragment length polymorphism (RFLP) analysis. Genomic DNA was extracted from blood specimens using (QIAamp DNA Blood Mini Kit, Qiagen, UK). Amplification of extracted DNA was done at exons 5, 7 and 10 to detect the G238C (TPMT*2), G460A (TPMT*3B), and A719G (TPMT*3C) allelic variation at the TPMT locus, respectively. TPMT*3A is a combination of mutations at two sites (G460A and A719G). The primers used for PCR were as follows (Yates et al. 1997; Ameway et al. 1999): G238C wild specific sense, \(5'\)-GTA TGA TTT TAT GCA GGT TTG-\(3'\); G238C mutant specific sense, \(5'\)-GTA TGA TTT TAT GCA GGT TTC-\(3'\); G238C common antisense, \(5'\)-TAA ATA GGA ACC ATC GGA CAC-\(3'\); G460A sense, \(5'\)-AGG CAG CTA GGG AAA AAG AAA GGT G-\(3'\); G460A antisense, \(5'\)-CAA GCC TTA TAG CCT TAC ACC CAG G-\(3'\); A719G sense, \(5'\)-GAG ACA GAG TTT CAC CAT CTT GG-\(3'\); A719G antisense, \(5'\)-CAG GCT TTA GCA TAA TTT TCA ATT CCT C-\(3'\).
For the G238C polymorphism, the DNA fragment can be amplified using a G238C wild specific sense primer in addition to a G238C common antisense primer in the wild-type allele (TPMT*1), while it can be amplified using a G238C mutant specific sense primer in the TPMT*2 allele. For the G460A polymorphism, MwoI digestion produces 443 and 251 bp fragments in the wild-type allele (TPMT*1) and an uncleaved 694-bp fragment in the TPMT*3B allele. For the A719G polymorphism, AccI digestion produces an uncleaved 373-bp fragment in the wild-type allele (TPMT*1) and 283 and 90 bp fragments in the TPMT*3C allele. The amplified digested PCR products were analysed by electrophoresis in 2% gel stained with ethidium bromide and visualized by ultraviolet transilluminator.
Statistical analysis
Data were analysed by computer using the statistical program SPSS for windows ver. 13. The mean, standard deviation (SD), median and IQ range were presented for descriptive analysis. Groups were compared using Mann–Whitney test in case of nonparametric data, in addition, chi square \(({\chi }^{2})\) test was used for comparison of categorical data. P values less than 0.05 were considered a cut off level for statistical significance.

(a) Electrophoresis patterns for G460A and A719G alleles at TPMT locus analysed by PCR-RFLP-based assays and allele-specific PCR. ‘Wild type TPMT*3B and wild type TPMT*3C’. (b) Electrophoresis patterns for G238C alleles at TPMT locus analysed by PCR-RFLP-based assays and allele-specific PCR. ‘Wild-type TPMT*2’.
Results
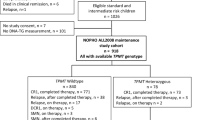
Sixty-four patients of 150 ALL patients who were attending pediatric hematology/oncology clinic over a year period were recruited. The recruited patients were 40 males (62.5%) and 24 females (37.5%). Their ages ranged from two to 15 years with a mean value \(6.16 \pm 3.16\) years. Their ALL diagnosis was based on the initial haematological workup, 26.9% were found to have T lineage immunophenotype and 73.1% had a pre-B phenotype, all the study population showed remission and none of them experience relapse. Thirty-two patients were still receiving their maintenance chemotherapy and the other 32 patients completed their chemotherapy since 6 months to 2 years. The presenting clinical manifestation were lymphadenopathy (75%), pallor (72%), purpura (62%), fever (59%), and joint pain (22%).
Complications during the course of chemotherapy that may suggestive of mercaptopurine side effects in form of myelosuppression and liver toxicity are illustrated in table 1. Fifty per cent of those who had fever also had accompanied ANC less than 500 per \(\mu \hbox {L}\) (febrile neutropenia), that required hospitalization. Eighteen patients (28.1%) of those developed infection during the course of therapy, having mild clinical illness that did not required hospitalization. Forty-six patients had elevated liver enzyme, 20 of whom had elevated liver enzymes more than 200 IU/L and had a history of positive viral hepatitis.
During the course of chemotherapy, most of patients (81.2%) need 6-PM dose modification either once or more and 96.9% of patients required to stop 6-MP for days and sometimes weeks as shown in table 2.
Those four patients, who need a high frequency of dose modification (four times), also required to interrupt the therapy for more than two weeks. Two females and two males did not tolerate the full dose of 6-MP and had experienced frequent severe myelosuppression when taken in full dose, and accordingly they continued their chemotherapy with a lower dose. Two of whom continued with 50% of the original dose and the other two continued with 75%.
Among 64 patients and 70 controls (288 examined allies), neither the studied leukaemic patients nor the controls had the mutant TPMT variant alleles in either homozygous or heterozygous form. Figure 1a illustrates electrophoresis patterns for G238C alleles at TPMT locus analysed by PCR-RFLP-based assays and allele-specific PCR. It is positive for wild-type TPMT*2, and it yields after digestion fragment of 254 bp at exon 5. In addition, figure 1b illustrates the electrophoresis patterns for G460A (TPMT*3B) and A719G (TPMT*3C) alleles at TPMT locus. It is positive for wild-type TPMT*3B and it yields after digestion fragments of 267 and 98 bp at exon 7. Moreover, it is positive for wild-type TPMT*3C, and it yields an uncleaved fragment of 293 bp at exon 10. The TPMT allele’s frequencies distribution in the study population and different countries and population are illustrated in table 3.
Discussion
6-Mercaptopurine (6MP), a commonly used treatment of childhood ALL, is a prodrug with no intrinsic anticancer activity, requires activation by hypoxanthine-guanine phosphoribosyl transferase (HGPRT) (Hamdy et al. 2003) with intracellular conversion to thioguanine nucleotides (TGNs) and subsequent incorporation into DNA as one mechanism of its antiproliferative effects (Stork et al. 2010). Alternatively, 6MP is methylated by TPMT to inactive metabolites (Evans et al. 2001). Patients with low erythrocyte TPMT activity developed severe and potentially fatal myelosuppression by the increased accumulation of intracellular TGNs when treated with standard doses of 6MP (McLeod et al. 1993; Ando et al. 2001). Patients heterozygous for TPMT mutations have intermediate activity while those homozygous for the mutation have low activity (Evans et al. 2001).
More than 20 variant alleles of TPMT could cause decreased enzymatic activity (Samochatova et al. 2009). The common polymorphisms reported as follow: a G to C mutation at codon 80 (G238C; Ala to Pro), a G to A mutation at codon 154 (G460A; Ala to Thr), and a A to G mutation at codon 240 (A719G; Tyr to Cys). Five allelotypes have been shown: TPMT*1 (wild type), TPMT*2 (G238C), TPMT*3A (G460A and A719G), TPMT*3B (G460A) and TPMT*3C (A719G) (Otterness et al. 1997; Weinshilboum et al. 1999; Kumagai et al. 2001). TPMT*3C is the most prevalent mutant allele in African populations and represents 86% of the TPMT variant allele in the Egyptian population (Hamdy et al. 2003).
The present work was designed to study frequency distribution of the most common variant alleles of TPMT (TPMT*2, TPMT*3A, TPMT*3B and TPMT*3C) in the Egyptian children with acute lymphoblastic leukaemia who presented with clinical manifestation suggested myelosuppression toxicity, and required interruption or modification of 6-PM therapy. Among the 64 patients and the 70 controls, neither the studied leukaemic patients nor the controls had the TPMT mutant variant alleles in either homozygous or heterozygous form, and this may be due to the small numbers of alleles examined (288 alleles) or that we have other types of TPMT variant alleles in our population. Similarly, a recent published Egyptian study, included 40 ALL children and 40 controls, reported that no homozygous mutant TPMT genotypes were detected for these four common alleles, neither the cases nor the controls had TPMT*2 and TPMT*3B genotypes, and only one patients was heterozygous TPMT*3A (El-Kaffash et al. 2014). Moreover, a Palestine study detected no TPMT*2, TPMT*3B or TPMT*3C alleles and only one of 56 patients was found to be heterozygous for the TPMT*3A allele (Ayesh et al. 2013).
Dramatic ethnic variations of TPMT enzyme activity have been shown in the frequency distributions of both the phenotype and genotype in the previous population studies, particularly between Asian and Caucasians (Black et al. 1998). TPMT*C, but no other variant alleles were found in Chinese, West African, Kenyan or Japanese populations (Ameway et al. 1999; Collie-Duguid et al. 1999; McLeod et al. 1999; Hiratsuka et al. 2000; Ando et al. 2001). In contrast, TPMT*3A is most common in Caucasian and Southwest Asian populations (De la Moureyre et al. 1998a, b; Collie-Duguid et al. 1999). Healthy Caucasian populations demonstrate a tri-modal distribution of TPMT activity, with \(89\pm 94\%\) of the healthy having a high activity, \(6\pm 11\%\) having an intermediate activity, and \({\sim }0.3\%\) having a low activity (Ando et al. 2001). Considering the importance of TPMT mutations on azathioprine toxicity (Black et al. 1998; Stolk et al. 1998; Kumagai et al. 2001), investigation of TPMT polymorphisms with consideration of ethnic differences before administration of 6-MP may provide clinically useful information.
The absence of any allelic variation responsible for the low TPMT activity in the studied leukaemic patients in either homozygous or heterozygous form, together with fact that TPMT*3C mutant allele is previously detected in the Egyptian population (Hamdy et al. 2003), and also that patients experienced signs of myelosuppression toxicity during the course of chemotherapy and 6-PM dose modification and interruption would suggest the existence of additional factors other than the studied TPMT genetic variations in the development of 6-PM cytotoxicity. These factors could be other polymorphic alleles in TPMT gene as we used PCR-RFLP-based assays, which may not detect other SNPs, scattered throughout the TMPT gene and may be the use of complete gene sequencing can overcome this limitation (Lee et al. 2012), or factors other than TPMT polymorphisms may be responsible for the development of toxicity. The folate pathway is crucial for the uptake of 6-MP. RFC1 (SLC29A1) is responsible for the transport of 6-MP across red blood cell membranes and its function influences intracellular distribution of 6-MP. A few researchers have investigated the contribution of folate pathway genetic polymorphisms in 6-MP mediated haematological toxicity (Dorababu et al. 2012). In conclusion none of the studied G238C, G460A and A719G TPMT variant alleles were detected. Infections and febrile neutropenia were common causes of 6-PM dose modification and interruption.
References
Ameway M. M., Collie-Duguid E. S. R., Powrie R. H., Ofori-Adjei D. and Mcleod H. L. 1999 Thiopurine S-methyltransferase alleles in British and Ghanaian populations. Hum. Mol. Genet. 8, 367–370.
Ando M., Ando Y., Hasegawa Y., Sekido Y., Shimokata K. and Horibe K. 2001 Short communication: Genetic polymorphisms of thiopurine S-methyltransferase and 6-mercaptopurine toxicity in Japanese children with acute lymphoblastic leukaemia. Pharmacogenetics 11, 269–273.
Ayesh B. M., Harb W. M. and Abed A. A. 2013 Thiopurine methyltransferase genotyping in Palestinian childhood acute lymphoblastic leukemia patients. BMC Hematol. 13, 3.
Black A. J., McLeod H. L., Capell H. A., Powrie R. H., Matowe L. K., Pritchard S. C. et al. 1998 Thiopurine methyltransferase genotype predicts therapy-limiting severe toxicity from azathioprine. Ann. Intern. Med. 129, 716–718.
Collie-Duguid E. S. R., Pritchard S. C., Powrie R. H., Sludden J., Collier D. A., Li T. and McLeod H. L.1999 The frequency and distribution of thiopurine methyltransferase alleles in Caucasian and Asian populations. Pharmacogenetics 9, 37–42.
Davies S. M., Borowitz M. J., Rosner G. L., Ritz K., Devidas M., Winick N. et al. 2008 Pharmacogenetics of minimal residual disease response in children with B-precursor acute lymphoblastic leukemia: a report from the Children’s Oncology Group. Blood 111, 2984–2990.
De la Moureyre C. S. V., Debuysere H., Mastain B., Vinner E., Marez D., Lo Guidice J. M. et al. 1998a Genotypic and phenotypic analysis of the polymorphic thiopurine S-methyltransferase gene (TPMT) in a European population. Br. J. Pharmacol. 125, 879–887.
De la Moureyre C. S. V., Debuysere H., Sabbagh N., Marez D., Vinner E., Chevalier E. D. et al. 1998b Detection of known and new mutations in the thiopurine S-methyltransferase gene by single-strand conformation polymorphism analysis. Hum. Mutat. 12, 177–185.
Dorababu P., Naushad S. M., Linga V. G., Gundeti S., Nagesh N., Kutala V. K. et al. 2012 Genetics variants of thiopurine and folate metabolic pathways determine 6-MP-mediated hematological toxicity in childhood ALL. Pharmacogenomics 13, 1001–1008.
El-Kaffash D. M. N. E., Abou Elfotouh Hassab H. M., AbouZeid A. A., Abd El Moaty Elneily D. and Shaaban I. O. A. 2014 Analysis of thiopurine S methyltransferase genotype in children with acute lymphoblastic leukemia by strip hybridization. JMSCR 2, 1740–1750.
Evans W. E., Hon Y. Y., Bomgaars L., Coutre S., Holdsworth M., Janco R. et al. 2001 Preponderance of thiopurine S-methyltransferase deficiency and heterozygosity among patients intolerant to mercaptopurine or azathioprine. J. Clin. Oncol. 19, 2293–2301.
Fujita K. and Sasaki Y. 2007 Pharmacogenomics in drug-metabolizing enzymes catalyzing anticancer drugs for personalized cancer chemotherapy. Curr. Drug Metab. 8, 554–562.
Hamdy S. I., Hiratsuka M., Narahara K., Endo N., El-Enany M., Moursi N. et al. 2003 Genotype and allele frequencies of TPMT, NAT2, GST, SULT1A1 and MDR-1 in the Egyptian population. Br. J. Clin. Pharmacol. 55, 560–569.
Hann I., Viscoli C., Paesmans M., Gaya H. and Glauser M. A. 1997 Comparison of outcome from febrile neutropenic episodes in children compared with adults: results from four EORTC studies. International Antimicrobial Therapy Cooperative Group (IATCG) of the European Organization for Research and Treatment of Cancer (EORTC). Br. J. Haematol. 99, 580–588.
Hiratsuka M., Inoue T., Omori F., Agatsuma, Y. and Mizugaki M. 2000 Genetic analysis of thiopurine methyltransferase polymorphism in a Japanese population. Mutat. Res. 448, 91–95.
Krynetski E. Y. and Evans W. E. 1998 Pharmacogenetics of cancer therapy: getting personal. Am. J. Hum. Genet. 63, 11–16.
Krynetski E. Y., Tai H. L., Yates C. R., Fessing M. Y., Loennechen T., Schuetz J. D. et al. 1996 Genetic polymorphism of thiopurine S-methyltransferase: clinical importance and molecular mechanisms. Pharmacogenetics 6, 279–290.
Kumagai K., Hiyama K., Ishioka S., Sato H., Yamanishi Y., McLeod H. L. et al. 2001 Allelotype frequency of the thiopurine methyltransferase (TPMT) gene in Japanese. Pharmacogenetics 11, 275–278.
Lee C. K., Loh T. P., Wong S. T., Lee H. K., Huan P. T., Chiu L. L. and Koay E. S. 2012 Detection of a novel single nucleotide polymorphism of the human thiopurine s-methyltransferase gene in a Chinese individual. Drug Metab. Pharmacokinet. 27, 559–561.
McLeod H. L., Miller D. R. and Evans W. E. 1993 Azathioprine-inducedmyelosuppression in thiopurinemethyl-transferase deficient heart transplant recipient. Lancet 341, 1151.
McLeod H. L., Lin J. S., Scott E. P., Pui C. H. and Evans W. E. 1994 Thiopurine methyltransferase activity in American white subjects and black subjects. Clin. Pharmacol. Ther. 55, 15–20.
McLeod H. L., Pritchard S. C., Githang’a J., Indalo A., Ameyaw M. M., Powrie R. H. et al. 1999 Ethnic differences in thiopurine methyltransferase pharmacogenetics: evidence for allele specificity in Caucasian and Kenyan individuals. Pharmacogenetics 9, 773–776.
Otterness D., Szumlanski C., Lennard L., Klemetsdal B., Aarbakke J., Park-Hah J. O. et al. 1997 Human thiopurine methyl transferase pharmacogenetics: gene sequence polymorphisms. Clin. Pharmacol. Ther. 62, 60–73.
Pui C. H. and Evans W. E. 2006 Treatment of acute lymphoblastic leukemia. N. Engl. J. Med. 354, 166–178.
Relling M. V., Hancock M. L., Boyett J. M., Pui C. H. and Evans W. E. 1999 Prognostic importance of 6-mercaptopurine dose intensity in acute lymphoblastic leukemia. Blood 93, 2817–2828.
Samochatova E. V., Chupova N. V., Rudneva A., Makarova O., Nasedkina T. V., Fedorova O. E. et al. 2009 TPMT genetic variations in populations of the Russian Federation. Pediatr. Blood Cancer 52, 203–208.
Schaeffeler E., Fischer C., Brockmeier D., Wernet D., Moerike K., Eichelbaum M. et al. 2004 Comprehensive analysis of thiopurine S-methyltransferase phenotype-genotype correlation in a large population of German-Caucasians and identification of novel TPMT variants. Pharmacogenetics 14, 395–396.
Stolk J. N., Boerbooms A. M., de Abreu R. A., de Koning D. G., van Beusekom H. J., Muller W. H. et al. 1998 Reduced thiopurine methyltransferase activity and development of side effects of azathioprine treatment in patients with rheumatoid arthritis. Arthritis Rheum. 41, 1858–1866.
Stork L. C., Matloub Y., Broxson E., Mei L. A., Yanofsky R., Sather H. et al. 2010 Clinical trials and observations. Oral 6-mercaptopurine versus oral 6-thioguanine and veno-occlusive disease in children with standard-risk acute lymphoblastic leukemia: report of the Children’s Oncology Group CCG-1952 clinical trial. Blood 115, 2740–2748.
Weinshilboum R. M., Otterness D. M. and Szumlanski C. L. 1999 Methylation pharmacogenetics: catechol O-methyltransferase, thiopurine methyltransferase, and histamine N-methyltransferase. Annu. Rev. Pharmacol. Toxicol. 39, 19–52.
Yates C. R., Krynetski E. Y., Loennechen T., Fessing M. Y., Tai H. L., Pui C. H. et al. 1997 Molecular diagnosis of thiopurine S-methyltransferase deficiency: genetic basis for azathioprine and mercaptopurine intolerance. Ann. Intern. Med. 126, 608–614.
Author information
Authors and Affiliations
Corresponding author
Additional information
Corresponding editor: Shantanu Sengupta
Rights and permissions
About this article

Cite this article
Tantawy, A.A.G., Ebeid, F.S.E., Adly, A.A.M. et al. Influence of thiopurine methyltransferase gene polymorphism on Egyptian children with acute lymphoblastic leukaemia. J Genet 96, 905–910 (2017). https://doi.org/10.1007/s12041-017-0853-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12041-017-0853-0