
Abstract
Background
This study aims to investigate the efficacy and safety of glibenclamide treatment in patients with acute aneurysmal subarachnoid hemorrhage (aSAH).
Methods
The randomized controlled trial was conducted from October 2021 to May 2023 at two university-affiliated hospitals in Beijing, China. The study included patients with aSAH within 48 h of onset, of whom were divided into the intervention group and the control group according to the random number table method. Patients in the intervention group received glibenclamide tablet 3.75 mg/day for 7 days. The primary end points were the levels of serum neuron-specific enolase (NSE) and soluble protein 100B (S100B) between the two groups. Secondary end points included evaluating changes in the midline shift and the gray matter–white matter ratio, as well as assessing the modified Rankin Scale scores during follow-up. The trial was registered at ClinicalTrials.gov (identifier NCT05137678).
Results
A total of 111 study participants completed the study. The median age was 55 years, and 52% were women. The mean admission Glasgow Coma Scale was 10, and 58% of the Hunt-Hess grades were no less than grade III. The baseline characteristics of the two groups were similar. On days 3 and 7, there were no statistically significant differences observed in serum NSE and S100B levels between the two groups (P > 0.05). The computer tomography (CT) values of gray matter and white matter in the basal ganglia were low on admission, indicating early brain edema. However, there were no significant differences found in midline shift and gray matter–white matter ratio (P > 0.05) between the two groups. More than half of the patients had a beneficial outcome (modified Rankin Scale scores 0–2), and there were no statistically significant differences between the two groups. The incidence of hypoglycemia in the two groups were 4% and 9%, respectively (P = 0.439).
Conclusions
Treating patients with early aSAH with oral glibenclamide did not decrease levels of serum NSE and S100B and did not improve the poor 90-day neurological outcome. In the intervention group, there was a visible decreasing trend in cases of delayed cerebral ischemia, but no statistically significant difference was observed. The incidence of hypoglycemia did not differ significantly between the two groups.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Stroke is a large group of life-threatening diseases of the central nervous system. According to the China Stroke Statistics 2019, approximately 1.57 million people died of stroke in 2018 [1]. Subarachnoid hemorrhage (SAH), particularly aneurysm SAH (aSAH), is a specific subtype of stroke and is associated with high disability and mortality, accounting for approximately 5% of all strokes [2]. This disease primarily affects young individuals, with an average age of 55 years [3, 4], leading to a significant economic burden on both patients and society [5]. In recent decades, advancements in aneurysms treatment and the widespread use of nimodipine therapy have contributed to improved survival rates [1, 6, 7].
Retrospective studies of patients with diabetes with stroke show improved outcomes in patients who are continued on sulfonylureas after stroke onset [8]. Both preclinical and clinical studies have demonstrated its effectiveness in alleviating cerebral edema following intracranial hemorrhage and ischemic stroke [9,10,11,12,13]. The mechanism involves the blocking of the sulfonylurea receptor 1-transient receptor potential melastatin 4 channel (TRPM4), a nonselective cation channel discovered to be transcriptionally upregulated by all cell types in the neurovascular unit following ischemia [14, 15]. This channel opens in response to adenosine triphosphate depletion, allowing the influx of sodium and water, which leads to cytotoxic edema and subsequent vasogenic edema [16, 17]. In addition, glibenclamide has shown benefits in maintaining vascular endothelial integrity during cell injury, reducing edema, and inhibiting neuronal cell death caused by elevated intracranial pressure (ICP) [18, 19].
The upregulation of TRPM4 has been confirmed in SAH [20]. Early cerebral edema, which contributes to elevated ICP, appears to be associated with ion channel dysfunction and subsequent cellular swelling [21]. Recent studies highlighted the importance of managing early brain injury characterized by diffuse brain edema within 72 h of aSAH onset [22]. Hence, we hypothesized that glibenclamide may have neuroprotective effects in individuals with acute aSAH. Previous studies on ischemic stroke have already used oral glibenclamide [23, 24]. Additionally, the intravenous form of glibenclamide has not yet been clinically approved in China. Therefore, this study selected oral glibenclamide as the trial drug.
Methods
Study Design
The study was a multicenter, prospective, randomized, controlled, open-label, blinded end point clinical trial, conducted simultaneously in Beijing Tiantan Hospital and Beijing Tongren Hospital, affiliated with Capital Medical University. Its objective was to assess the potential of glibenclamide in reducing early brain injury following aSAH. All procedures in this study strictly adhered to the recommendations of Good Clinical Practice guidelines and the Declaration of Helsinki. Participants or their legally authorized representatives provided written consent before entering the study.
Study Objects
Inclusion criteria: Radiological evidence of aSAH (confirmed by CT/CTA/MRI/MRA/DSA) within 48 h of onset, age 18 to 74 years (the older population tended to have lower tolerance to hypoglycemia).
Exclusion criteria: (1) patients who were previously diagnosed with aneurysms and have a history of stroke, epilepsy, neurodegenerative diseases such as Parkinson’s disease, dementia, cerebrovascular diseases, motor neuron diseases, traumatic brain injury, schizophrenia, or depression were excluded. Exclusion criteria were based on previously published data, indicating that levels of some brain-specific biomarkers may be elevated in these diseases [25]; (2) being allergic to sulfonamides or glibenclamide tablets and having taken sulfonylurea within 30 days before the trial; (3) having severe craniocerebral injury such as cerebral hernia or Hunt-Hess grade of V occurred at admission; (4) having severe renal disease, severe liver disorder, coagulation abnormalities, or malignant tumor; (5) having blood sugar levels below 4 mmol/L after aSAH or a history of hypoglycemia; and (6) being pregnant or lactating. The details of inclusion and exclusion criteria are shown in Supplementary Table 1.
Randomization and Masking
Study participants were randomly assigned in a 1:1 ratio to either the glibenclamide group or the control group using a Web-based randomization process. The randomization sequence was computer generated. It was prepared by a doctor skilled in statistics who was not involved in the rest of the study. The grouping results were unmasked to participants and researchers, except for those who assessed the outcome and conducted the analysis. All imaging evaluations were conducted by investigators who were masked to clinical variables, interventions, and functional outcomes. One investigator, who was unaware of the allocation and intervention, assessed the functional outcomes at day 90. The statistical analysis was conducted by an independent doctor, who was also masked.
Intervention
Study participants assigned to the intervention group were prescribed glibenclamide tablets (Tianjin Pacific Pharmaceutical Co., Ltd., China; each tablet 2.5 mg) at a dosage of 1.25 mg three times daily, along with standard care, for 7 consecutive days after enrollment. The glibenclamide was orally taken within 30 min before three meals. For patients with enteral nutrition, glibenclamide was given at regular time points (08:00, 12:00, and 16:00) through a nasogastric feeding tube. The control group received neither glibenclamide tablets nor placebo. Both groups in the trial were prescribed with standard care following guidelines [26,27,28]. Surgical clipping or endovascular coiling was determined by a team of neurosurgeons and interventional neuroradiologists based on medical indications, such as the results of the complete blood count, size and location of the aneurysm, and the neurological status of the patient. In patients with symptomatic hydrocephalus, external continuous ventricular drainage with of the cerebrospinal fluid was first implanted.
Clinical Evaluation
Demographic data, medical history, and baseline clinical parameters were collected after admission. This included information on gender, age at diagnosis, risk factors (such as hypertension, cigarette, alcohol, diabetes mellitus, and dyslipidemia), familial history, and details related to aneurysms, such as number, location, size, and treatment, from each patient. The patient’s clinical status at the ICU was assessed using the Acute Physiology and Chronic Health Evaluation II score. Brain CT, liver and kidney function, and coagulation indexes were measured at baseline, on the third day, and on the seventh day.
The modified Fisher score and the SAH early brain edema score (SEBES) were conducted according to the brain CT at enrolled. SEBES is a CT-based, semiquantitative assessment method for brain edema [29]. This scoring system evaluates four areas of sulci disappearance in specific brain tissue planes in each hemisphere, focusing on the basal ganglia and centrum semiovale. Patients with a high SEBES on admission, particularly a score of 3–4, often exhibit more severe disease severity, increased risk of delayed cerebral ischemia (DCI), and poorer functional outcomes. However, it is important to note that this scoring method primarily focuses on severe cases of edema and may not fully capture the entire spectrum of early brain injury. Furthermore, its effectiveness has not been validated in large-scale clinical studies.
Initial neurological conditions of the patients were assessed using the World Federation of Neurosurgical Societies SAH grading scale, and the severity of aSAH was classified using the Hunt-Hess scale. Glasgow Coma Scale was used to assess the disturbance of consciousness in study participants. All of the above were performed by intensive care unit physicians. The modified Rankin Scale (mRS) was assessed on the 90th day to evaluate the degree of study participants’ neurological recovery. If an ICP monitoring device was placed, the recorded values include ICP. The relevant information was collected and recorded in the case report form. There are four key evaluation time points in this trial: baseline (T0), third day (T1), seventh day (T2), and 90th day (T3) after admission (Supplementary Table 2).
Serum Neuron-Specific Enolase and Soluble Protein 100B Levels
Blood samples were collected from each patient on admission (T0), as well as on T1 and T2. A 3-mL blood sample was drawn from an intravenous catheter and injected into a tube with no anticoagulation. Subsequently, each blood sample was centrifuged at 3000 rpm for 5 min. The resulting supernatant was then aliquoted and stored at − 80 °C until assayed. The concentrations of serum neuron-specific enolase (NSE) and soluble protein 100B (S100B) were detected using the Roche automatic chemiluminescence immunoassay analyzer known as Cobas e801. This analyzer uses the method recommended by the American Clinical Standards Institute documents. All tests were conducted by qualified professionals in a qualified laboratory using the electrochemiluminescence immunoassay method. The reagents used for the measurements were manufactured by Roche Diagnostics GmbH (Mannheim, Germany). Specifically, the NSE detection kit was used for NSE measurement, whereas the S100 detection kit was employed for S100B measurement.
Brain CT Scan
The study participants underwent CT scans to measure midline shift and gray matter–white matter ratio (GWR) at T0, T1, and T2. Middle shift refers to the vertical distance, measured in millimeters, between a line structure (typically the septum pellucidum) and the line that indicates the midline. The ideal midline method commonly used in routine radiology practice was used to measure the midline shift in this study. The gray–white matter density ratio was measured at the level of the basal ganglia in this study. A circular region with a diameter of 20 mm2 was selected in the gray matter region of the head of the caudate nucleus, and the average Hounsfiled Unit (HU) in this region (HU1) was measured. Similarly, a circular region with a diameter of 20 mm2 was chosen in the white matter region of the posterior limb of the internal capsule, and its average HU (HU2) was determined. The gray–white matter density ratio was then calculated as HU1/HU2. The diagnosis of hydrocephalus and cerebral infarction was confirmed through a formal diagnostic report provided by the radiology department. An investigator, trained by a radiologist and unaware of the clinical outcome, was tasked with measuring midline shift and the gray-to-white matter density ratio.
DCI is defined as the development of focal or global neurological deficits, including motor limb weakness, aphasia, hemineglect, and/or hemianopia, or a decline in the Glasgow Coma Scale by ≥ 2 points, which lasts or fluctuates for at least 1 h [30]. Furthermore, the presence of new cerebral infarcts on neuroimaging, without explanation from other clinical, radiological, or laboratory abnormalities, is also considered a manifestation of DCI. This is in line with the definition of DCI, as described in the article by Vergouwen et al. [30], which emphasizes the importance of excluding other potential causes of neurological decline, such as infection or metabolic disturbances.
Adverse Events
Hypoglycemia
Glibenclamide has been widely used in clinical practice for many years. Its primary side effect is hypoglycemia, with an incidence of 14% [31]. The study protocol of glibenclamide 3.75 mg daily dosage (the dosage used in this study) has been verified by researchers and found to be well tolerated [11]. Peripheral blood sugar (BS) was checked by a glucometer (Abbott) every 2 h within the first 12 h of glibenclamide administration and followed by every 4 h within the first 48 h. Thereafter, the frequency of BS test was determined by the attending doctor. If a tendency toward hypoglycemia is identified, participants will provide with a 5% to 10% glucose solution. The standard for hypoglycemia in patients with diabetes is BS set at ≤ 3.9 mmol/L according to the Chinese guidelines for the prevention and treatment of type 2 diabetes mellitus (2020 edition), whereas for patients without diabetes, it is set at ≤ 2.8 mmol/L.
Other Adverse and Severe Adverse Events
Other common adverse reactions may include the following: (1) diarrhea, nausea, vomiting, headache, stomach pain, or discomfort; (2) rash (although this is a rare side effect); and (3) rare and serious cases such as jaundice, liver function damage, bone marrow suppression, granulocytopenia (characterized by sore throat, fever, and infection), and thrombocytopenia (characterized by bleeding and purpura). In the event of a severe adverse event or accident, it is the responsibility of the clinical investigator to promptly inform the study supervisor. He will then decide whether to modify or terminate the study. All adverse events will be meticulously recorded on the case report form.
Study End Points
The levels of S100B can measure astrocytic damage and blood–brain barrier dysfunction, whereas NSE is served as a marker for neuronal cell injury [25, 32]. The combination of the two can detect early brain injury. Therefore, the primary end point of this study was the difference in serum NSE and S100B levels with or without glibenclamide. Secondary end points included changes in midline shift and GWR, as well as the mRS score during follow-up. We also documented complications associated with aSAH, such as rebleeding, hydrocephalus, and cerebral infarction (confirmed by CT imaging). To assess the safety of glibenclamide in patients with aSAH, we compared the 90-day survival rate and episodes of hypoglycemia.
Statistical Analysis
Continuous variables were shown as means and standard deviations (SDs) or medians and interquartile ranges (IQRs) after assessing for normality. Categorical variables were reported as numbers and percentages. The difference between patients with and without glibenclamide were compared by the χ2 test or Fisher’s exact test for categorical variables and the nonparametric Mann–Whitney U-test for continuous variables. All analyses were completed using R software (version 4.1.2, R Foundation for Statistical Computing). A two-sided P value of < 0.05 was considered statistically significant.
Sample Size
The primary end points of this study were two biomarkers of neurological injury. Of the two, S100B is rarely used in cases of SAH, so the sample size is calculated only based on the data of NSE. Changes in NSE activity are closely correlated with nerve injury. Previous studies have shown that the mean value of NSE on the third day after aSAH is 21 ng/ml, with an SD of approximately 3 ng/ml. In the group with a good prognosis, the NSE on the third day is approximately 19 ng/ml, with an SD of 3 ng/ml [33]. According to the two-sided test, significance was 0.05, the number of the two groups was equal, and the power was 90%, the sample size was calculated to be 98. Assuming 10% loss to follow-up, the total sample size was expected to be 110.
Results
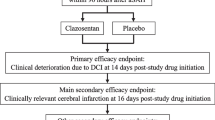
The enrollment period for this study was from October 2021 to May 2023, with the final follow-up conducted in August 2023. A total of 120 consecutive patients who meet inclusion criteria were included. They were all confirmed to have aSAH with radiological imaging. During the study, four patients withdrew from the trial because of hypoglycemia; five patients did not complete the follow-up or data acquisition. The final analysis included 111 patients, with 57 in the experimental group and 54 in the control group. Figure 1 illustrates the screening process. The median age of the participants was 55 years, and 52% were women. The mean admission Glasgow Coma Scale score was 10, and 58% of the Hunt-Hess grades were no less than III. Among study participants with ICP monitoring, elevated ICP was first detected within 48 h after aSAH in 97% of patients, and the highest ICP was ≥ 20 mm Hg in only 17% of patients. 53% of the highest ICP occurred within 48 h after aSAH, and 37% occurred around 72 h after aSAH. Most patients (85%) were treated with mannitol, but measurable intracranial hypertension was uncommon. There were no significant differences in demographic and neurological characteristics between the two groups. Table 1 provides a summary of patient baseline characteristics.

Patient selection algorithm. aSAH, aneurysmal subarachnoid hemorrhage, BS, blood sugar, CT, computed tomography, GCS, Glasgow Coma Scale, NSE, neuron-specific enolase, S100B, soluble protein 100B, mRS, Modified Rankin Scale, T0, baseline, T1, third day, T2, seventh day, T3, 90th day
Serum NSE and S100B
A comparison of outcomes between the two groups is shown in Table 2. The median serum NSE levels in the glibenclamide group were 7.37 (5.26, 11.4) ng/ml before administration, 6.11 (4.93, 10.4) ng/ml on the third day of administration, and 7.24 (5.07, 11.2) ng/ml on the seventh day of administration. In contrast, the values in the control group were 7.84 (5.04, 11.36) ng/ml before administration, 6.27 (3.71, 11.1) ng/ml on the third day of administration, and 8.15 (5.85, 12.34) ng/ml on the seventh day of administration. The serum NSE levels of patients in the glibenclamide group were similar to those in the control group, but no statistically significant difference was found (P = 0.399). A similar result was obtained in the measurements of S100B. The levels of S100B and NSE did not show a significant difference in patients with and without glibenclamide. The change trend of the experimental group and the control group is illustrated in Fig. 2.

The change trend of biomarkers in the glibenclamide group and the control group. D1, baseline, D3, third day, D7, seventh day, NSE, neuron-specific enolase, S100B, soluble protein 100B
Midline Shift and GWR
The midline shift occurred in 14 patients (25%) in the intervention group and 12 patients (22%) in the control group. There was no significant difference in the value of midline shift between the two groups at the three time points (P > 0.05). Under normal conditions, gray matter is denser than white matter on unenhanced CT, with CT values ranging from 32 to 40 HU for gray matter and about 25 to 32 HU for white matter. It was observed that the HU values of both gray matter and white matter were low at T0 than other time points, indicating the presence of early brain edema. This finding is consistent with the theory that diffuse brain edema occurs in the early stage of SAH. There was no significant difference in GWR between the two groups at T0 and T2 (P > 0.05). Statistical analysis revealed a significant difference in GWR between the two groups at T1 (P = 0.006), but because both of the median GWRs in the two groups were 1.3, we considered this statistical difference to be of no practical clinical significance.
mRS at 90 Days
The modified Rankin score at the 90-day visit was as Fig. 3 in both the intervention and control groups, and 30 patients had a good outcome, accounting for 53% and 56%, respectively. There was no significant difference between the two groups (P = 0.681). Therefore, it can be observed that glibenclamide has little effect on improving neurological outcome, which is consistent with the findings of Glibenclamide in aneurysmatic subarachnoid hemorrhage (GASH) [18].

Distribution of mRS scores in the glibenclamide group and the control group at 90 days. mRS, Modified Rankin Scale
Complications and Adverse Events
As shown in Table 2, the BS of patients remained stable throughout the study period, with a median value ranging from 6.4 to 8.25 mmol/L. On the third day of administration, the BS of intervention group experienced a slightly decrease (P = 0.075). No symptomatic hypoglycemic episode was observed in either group. Hypoglycemia was reported in two patients (4%) of control group and in five patients (9%) of intervention group (two received nasal feeding and three took oral feeding). Three patients in the intervention group returned to normal BS after receiving a high concentration glucose solution and completed the trial. The remaining four individuals withdrew from the trial with the approval of the study supervisor.
Common adverse outcome events were showed in Table 3. There were eight patients with bleeding and 23 patients with hydrocephalus, but no statistically significant difference was found between the intervention and control groups (P > 0.05). Forty-two patients developed DCI, 18 patients in the intervention group and 24 patients in the control group (P = 0.23). Data show that more than 60% of patients who develop DCI have a SEBES score of 3 or greater upon admission. This result indicated that patients with high-level SEBES at admission had a higher risk of DCI, which aligns with the findings of other studies [29]. By the 90th day of follow-up, a total of nine patients died (four in the intervention group and five in the control group). The 90-day survival was no significant difference in the two groups (P = 0.933).
Transaminases were elevated in about one third of the patients (intervention group of 26 patients, control group 20 patients). It was related to the characteristics of the disease itself and the use of antiepileptic drug, such as Valproate or Levetiracetam. The liver function all improved after discontinuation of the drugs and liver-protective therapy. No instances of liver failure or other serious complications were observed. Furthermore, there were no significant cases of bone marrow suppression. Table 3 provides a detailed overview of the complications and adverse events during the study period. The use of glibenclamide did not show any statistical differences in adverse events. Importantly, no serious adverse events were reported throughout the study.
Discussion
SAH is the third most common type of stroke after cerebral infarction and cerebral hemorrhage. When an aneurysm ruptures, blood enters the subarachnoid space, leading to a significant increase in ICP. This process results in global cerebral ischemia and secondary brain edema, known as early brain injury. During this process, brain cells (neurons and glial cells) are damaged due to inflammatory infiltration, vasospasm, ischemia, hypoxia, and the release of toxic substances. As a result, proteins from these cells are released into the cerebrospinal fluid and blood, allowing for the detection of biomarkers indicating brain cell damage. Glibenclamide, a specific inhibitor of the sulfonylurea receptor 1-transient receptor potential melastatin 4 channel, has been shown to effectively reduce brain edema. This study aimed to evaluate the effectiveness and safety of glibenclamide in patients with aSAH. However, no significant difference was found in primary endpoint between the control and intervention group.
There is more water content in gray matter than in white matter following the brain injury that results in edema [34]. Cerebral edema reduces the attenuation of gray matter on unenhanced CT scans and results in a loss of distinction between gray and white matter [35]. Research in aSAH has shown that GWR > 1.34 predicted good recovery in female patients with 82.3% sensitivity and 80% specificity, and GWR > 1.36 predicted go od recovery in male patients with 80% sensitivity and 95% specificity [36]. Regarding cerebral edema, the HU values of the gray matter in the head of the caudate nucleus and the white matter in the posterior limb of the internal capsule in the basal ganglia plane of the brain CT were mostly within the normal range for both groups. It is worth noting that the HU values of the gray matter and white matter were initially low, which indicated the presence of early brain edema. These findings supported the existence of global cerebral edema in the early stages of aSAH. Not many patients had midline shifts and there was no significant difference between the two groups. More than half of the patients in both groups had a favorable outcome (mRS 0–2), and there was no statistically significant difference between the groups. Following analysis was conducted to compare these negative results with other relevant studies.
Large hemispheric infarction is usually accompanied by progressive brain edema. The cases targeted by early studies, such as Glyburide Advantage in Malignant Edema and Stroke (GAMES), were those with large hemispheric infarction, and the effect of reducing cerebral edema can be observed at doses of glibenclamide lower than the hypoglycemic dose. Glyburide Advantage in Malignant Edema and Stroke, and the drug used is RP-1127 (Glyburide for Injection) (GAMES-RP) was a multicenter randomized controlled clinical trial conducted at 18 centers in the United States involving 86 study participants. The results indicated no significant impact on the primary end point event analysis (avoidance of decompressive craniectomy and mRS score of 0–4). However, a noteworthy reduction in midline shift was observed, with the glibenclamide group showing a measurement of 4.6 mm compared to 8.5 mm in the placebo group (P = 0.0006). The dosage used in that study was similar to that of our study, but it employed an intravenous glibenclamide. Injectable glibenclamide is not approved for clinical use in many countries, leading to an increasing number of studies focusing on oral glibenclamide. The GASH study conducted by Costa et al. [18] in Sao Paulo included 78 patients with aSAH within 96 h of onset. Among them, 38 patients in the intervention group received 5 mg glibenclamide tablets once daily for 21 days. The findings indicated that there were no significant differences in the mRS score, mortality rate, and incidence of DCI between the two groups. It is worth noting that the treatment window in the GASH study was twice as long as in our study. Despite advancing the initiation of treatment to within 48 h of onset, our study still yielded similar negative results.
From the above analysis, it can be found that the insufficient dose of glibenclamide tablets is likely to be an important reason for the effect of the trial. The conventional dosage of glibenclamide is 5 to 10 mg daily (equivalent to 2 to 4 tablets). Because glibenclamide becomes concentrated in the lesion due to the upregulation of receptors within the central nervous system and the destruction of the blood–brain barrier following strokes [37], a lower dose of glibenclamide was used in previous studies to avoid inducing hypoglycemia. Oral glibenclamide tablets, compared with intravenous administration, has the problem of absorption in the digestive tract. Another factor to the negative outcome could be the limited discrimination of endpoint indicators, such as serum biomarkers and mRS scores.
In conclusion, this study is a large, prospective, randomized, controlled clinical trial that investigates the neuroprotective effect of glyburide. The trial includes a shorter time window, earlier intervention, and multidimensional evaluation, incorporating biomarkers, imaging, and neurological scores. However, it is important to note that the number of patients in our study is still very small. Our findings suggest a lower incidence of DCI in the glibenclamide intervention group, although statistical significance was not reached. Further studies with larger sample sizes are necessary to confirm the efficacy of glibenclamide in reducing brain edema and improving functional prognosis in the treatment of aSAH.
Conclusions
Oral administration of glibenclamide in patients with early aSAH did not result in a significant decrease in serum NSE and S100B levels, and it did not significantly improve the poor neurological outcome at 90 days. Additionally, in the intervention group, there was a visible decreasing trend in cases of late-onset cerebral ischemia, but no statistically significant difference was observed. Furthermore, no cases of oral hypoglycemia were reported after glibenclamide administration. It is important to note that this study had limitations in terms of the number of patients and the duration of observation. Therefore, further studies with larger sample sizes and longer observation times are needed to validate the efficacy of glibenclamide in patients with aSAH.
References
Wang YJ, Li ZX, Gu HQ, et al. China Stroke Statistics 2019: A Report From the National Center for Healthcare Quality Management in Neurological Diseases, China National Clinical Research Center for Neurological Diseases, the Chinese Stroke Association, National Center for Chronic and Non-communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention and Institute for Global Neuroscience and Stroke Collaborations. Stroke Vasc Neurol. 2020;5(3):211–39.
Etminan N, Chang HS, Hackenberg K, et al. Worldwide incidence of aneurysmal subarachnoid hemorrhage according to region, time period, blood pressure, and smoking prevalence in the population: a systematic review and meta-analysis. JAMA Neurol. 2019;76(5):588–97.
Tu WJ, Zhao Z, Yin P, et al. Estimated burden of stroke in China in 2020. JAMA Netw Open. 2023;6(3): e231455.
English SW. Long-term outcome and economic burden of aneurysmal subarachnoid hemorrhage: are we only seeing the tip of the iceberg? Neurocrit Care. 2020;33(1):37–8.
Autio AH, Paavola J, Tervonen J, et al. Clinical condition of 120 patients alive at 3 years after poor-grade aneurysmal subarachnoid hemorrhage. Acta Neurochir (Wien). 2021;163(4):1153–66.
Claassen J, Park S. Spontaneous subarachnoid haemorrhage. Lancet. 2022;400(10355):846–62.
Neifert SN, Chapman EK, Martini ML, et al. Aneurysmal subarachnoid hemorrhage: the last decade. Transl Stroke Res. 2021;12(3):428–46.
Chang JJ, Khorchid Y, Kerro A, et al. Sulfonylurea drug pretreatment and functional outcome in diabetic patients with acute intracerebral hemorrhage. J Neurol Sci. 2017;381:182–7.
Eisenberg HM, Shenton ME, Pasternak O, et al. Magnetic resonance imaging pilot study of intravenous glyburide in traumatic brain injury. J Neurotrauma. 2020;37(1):185–93.
Kimberly WT, Bevers MB, von Kummer R, et al. Effect of IV glyburide on adjudicated edema endpoints in the GAMES-RP trial. Neurology. 2018;91(23):e2163–9.
Zhao J, Song C, Li D, et al. Efficacy and safety of glibenclamide therapy after intracerebral haemorrhage (GATE-ICH): a multicentre, prospective, randomised, controlled, open-label, blinded-endpoint, phase 2 clinical trial. EClinicalMedicine. 2022;53:101666.
Wali B, Ishrat T, Atif F, Hua F, Stein DG, Sayeed I. Glibenclamide administration attenuates infarct volume, hemispheric swelling, and functional impairments following permanent focal cerebral ischemia in rats. Stroke Res Treat. 2012;2012:460909.
Xu ZM, Yuan F, Liu YL, Ding J, Tian HL. Glibenclamide attenuates blood-brain barrier disruption in adult mice after traumatic brain injury. J Neurotrauma. 2017;34(4):925–33.
Kurland DB, Gerzanich V, Karimy JK, et al. The Sur1-Trpm4 channel regulates NOS2 transcription in TLR4-activated microglia. J Neuroinflammation. 2016;13(1):130.
Jha RM, Desai SM, Zusman BE, et al. Downstream TRPM4 polymorphisms are associated with intracranial hypertension and statistically interact with ABCC8 polymorphisms in a prospective cohort of severe traumatic brain injury. J Neurotrauma. 2019;36(11):1804–17.
Jha RM, Puccio AM, Chou SHY, et al. Sulfonylurea receptor-1: a novel biomarker for cerebral edema in severe traumatic brain injury. Crit Care Med. 2017;45(3):e255–64.
Stokum JA, Kwon MS, Woo SK, et al. SUR1-TRPM4 and AQP4 form a heteromultimeric complex that amplifies ion/water osmotic coupling and drives astrocyte swelling. Glia. 2018;66(1):108–25.
da Costa BBS, Windlin IC, Koterba E, et al. Glibenclamide in aneurysmatic subarachnoid hemorrhage (GASH): study protocol for a randomized controlled trial. Trials. 2019;20(1):413.
Vorasayan P, Bevers MB, Beslow LA, et al. Intravenous glibenclamide reduces lesional water uptake in large hemispheric infarction. Stroke. 2019;50(11):3021–7.
Mehta RI, Tosun C, Ivanova S, et al. Sur1-Trpm4 cation channel expression in human cerebral infarcts. J Neuropathol Exp Neurol. 2015;74(8):835–49.
Hayman EG, Wessell A, Gerzanich V, Sheth KN, Simard JM. Mechanisms of global cerebral edema formation in aneurysmal subarachnoid hemorrhage. Neurocrit Care. 2017;26(2):301–10.
Lauzier DC, Jayaraman K, Yuan JY, et al. Early brain injury after subarachnoid hemorrhage: incidence and mechanisms. Stroke. 2023;54(5):1426–40.
Huang K, Hu Y, Wu Y, et al. Exploratory analysis of oral glibenclamide in acute ischemic stroke. Acta Neurol Scand. 2019;140(3):212–8.
Khalili H, Derakhshan N, Niakan A, et al. Effects of oral glibenclamide on brain contusion volume and functional outcome of patients with moderate and severe traumatic brain injuries: a randomized double-blind placebo-controlled clinical trial. World Neurosurg. 2017;101:130–6.
Savarraj J, Park ES, Colpo GD, et al. Brain injury, endothelial injury and inflammatory markers are elevated and express sex-specific alterations after COVID-19. J Neuroinflammation. 2021;18(1):277.
Connolly ES Jr, Rabinstein AA, Carhuapoma JR, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2012;43(6):1711–37.
Dong Y, Guo ZN, Li Q, et al. Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of spontaneous subarachnoid haemorrhage. Stroke Vasc Neurol. 2019;4(4):176–81.
Hoh BL, Ko NU, Amin-Hanjani S, et al. 2023 Guideline for the management of patients with aneurysmal subarachnoid hemorrhage: a guideline from the American Heart Association/American Stroke Association. Stroke. 2023;54(7):e314-E370.
Ahn SH, Savarraj JP, Pervez M, et al. The subarachnoid hemorrhage early brain edema score predicts delayed cerebral ischemia and clinical outcomes. Neurosurgery. 2018;83(1):137–45.
Vergouwen MD, Vermeulen M, van Gijn J, et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: proposal of a multidisciplinary research group. Stroke. 2010;41(10):2391–5.
Draeger KE, Wernicke-Panten K, Lomp HJ, Schuler E, Rosskamp R. Long-term treatment of type 2 diabetic patients with the new oral antidiabetic agent glimepiride (Amaryl): a double-blind comparison with glibenclamide. Horm Metab Res. 1996;28(9):419–25.
Yun GS, In YN, Kang C, et al. Development of a strategy for assessing blood-brain barrier disruption using serum S100 calcium-binding protein B and neuron-specific enolase in early stage of neuroemergencies: a preliminary study. Medicine (Baltimore). 2022;101(28):e29644.
Quintard H, Leduc S, Ferrari P, Petit I, Ichai C. Early and persistent high level of PS 100beta is associated with increased poor neurological outcome in patients with SAH: is there a PS 100beta threshold for SAH prognosis? Crit Care. 2016;20:33.
Ali A, Tanirgan G, Sabanci PA, et al. Relation of gray-white matter ratio with long-term cognitive functions and quality of life in patients with mild to moderate aneurysmal subarachnoid hemorrhage: a prospective observational study. Acta Neurochir. 2017;160(1):181–9.
Gentsch A, Storm C, Leithner C, et al. Outcome prediction in patients after cardiac arrest: a simplified method for determination of gray-white matter ratio in cranial computed tomography. Clin Neuroradiol. 2014;25(1):49–54.
Ali A, Bitir B, Abdullah T, et al. Gray-to-white matter ratio predicts long-term recovery potential of patients with aneurysmal subarachnoid hemorrhage. Neurosurg Rev. 2018;43(1):195–202.
Szeto V, Chen N-H, Sun H-S, Feng Z-P. The role of KATP channels in cerebral ischemic stroke and diabetes. Acta Pharmacol Sin. 2018;39(5):683–94.
Acknowledgements
The study was conducted in a challenging health care environment during the COVID-19 pandemic. All members of our research group would like to extend our most sincere thanks to the doctors and nurses in the intensive care unit and neurosurgery department of Tiantan and Tongren Hospitals for their support and help to our work.
Funding
This work was supported by the Yangfan Project for Key medical Programs from the Hospital Authority of Beijing (Grant number ZYLX202109, Grant recipient: Shi G).
Author information
Authors and Affiliations
Contributions
Professor Guangzhi Shi and Rongli Yang were the principal investigators of this project, and they were also the corresponding authors. Professor Guangqiang Chen and Professor Shangfeng Zhao were the independent oversight of the study, who made decisions over reporting of serious adverse events and continuation of the study. Professor Guangzhi Shi and Professor Tong Li managed the intensive care units of two research centers, Tiantan Hospital and Tongren Hospital, respectively. Qing Lin and Dawei Zhou participated in the conception of the study and the design of the experimental scheme. Honglin Wen was responsible for the laboratory testing of NSE and soluble protein 100B. Huixian Yu was the follow-up visitor and was responsible for the follow-up of all study participants. Kai Gao was responsible for the generation of the random number table and the statistical analysis of the findings. The remaining authors were responsible for the treatment, collection of specimens and clinical observation of the study participants. Each author has approved the submitted version (and any substantially modified version that involves the author's contribution to the study); and has agreed both to be personally accountable for the author’s gifts and to ensure that questions related to the accuracy or integrity of any part of the work.
Corresponding author
Ethics declarations
Conflicts of Interest
No conflicts of interest were reported for this study.
Ethical Approval/Informed Consent
The research protocol of this experiment and the informed consent of the study participants have been approved by the Ethics Committee of Tiantan Hospital Affiliated with Capital Medical University of China (Ethics review number KY 2021-087-01). Researchers explain the study plan in detail to all patients or their legal representatives and obtain written informed consent. Before they agree to participate in the trial and sign the informed consent form, information will be provided, including the natural history, treatment procedures, risks, possible consequences, and costs of subarachnoid hemorrhage. At any stage of the study, each patient has the right to request a withdrawal. Trial results will be disseminated via publications, conference presentations, and the media. During the study, the patient’s name was replaced by a number to protect the patient’s privacy. Copies of the study participant’s code catalog, informed consent forms, case report forms, and relevant diagnostic test data, as well as drug handling records, are kept for 2 years after the termination of the clinical trial. Entered electronic data are kept for life.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lin, Q., Zhou, D., Ma, J. et al. Efficacy and Safety of Early Treatment with Glibenclamide in Patients with Aneurysmal Subarachnoid Hemorrhage: A Randomized Controlled Trial. Neurocrit Care (2024). https://doi.org/10.1007/s12028-024-01999-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s12028-024-01999-z