
Abstract
Purpose
The aim of this study was to assess the diagnostic value of catecholamines and their O-methylated metabolites in vitreous humor samples in identifying antemortem cold exposure and fatal hypothermia in the forensic casework.
Methods
A total of 80 autopsy cases (40 hypothermia fatalities and 40 cases in which hypothermia as the main or contributory cause of death was excluded) were selected for this study. Catecholamines and their O-methylated metabolites were measured in urine and vitreous humor samples collected at autopsy.
Results
Urine catecholamine and their O-methylated metabolite concentrations were significantly higher in hypothermia-related deaths. On the other hand, measurements in vitreous humor samples did not reveal statistically significant differences between hypothermia-related deaths and controls.
Conclusions
Globally considered, our findings seem to suggest that, contrary to urine catecholamines and their O-methylated metabolites, vitreous levels of these compounds appear to be of limited value in characterizing human antemortem stress reactions due to cold exposure and can hardly be used in the forensic setting to support the diagnosis of hypothermia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Reactions to stressful situations, such as exposure to cold temperatures, are characterized by enhanced catecholamine (adrenaline/epinephrine, noradrenaline/norepinephrine, and dopamine) secretion. Once released into blood circulation, these compounds undergo complex metabolism mediated by diverse tissue enzymes in various combinations. They are then excreted in urine in free and conjugated forms [1–5].
Metadrenaline/metanephrine, normetadrenaline/normetanephrine, and 3-methoxytyramine are produced by O-methylation of catecholamines. Further metabolism occurs by deamination or sulfate conjugation. Like the parent molecules, these O-methylated metabolites are excreted in urine [6].
A significant increase in urinary catecholamine and metanephrine levels has been reported in hypothermia fatalities. Hence, their determination has been recommended in forensic pathology routine to support the diagnosis of hypothermia [1, 7].
Unfortunately, urine unavailability for postmortem biochemical investigations may render the possibility of diagnosing hypothermia-related deaths challenging. Urine can be lost during antemortem agony and thus be absent at autopsy for collection and further analysis. In addition, renal failure with anuria may occur in terminal hypothermia [8, 9]. These situations are further exacerbated by the intrinsic difficulties of identifying fatal exposure to cold resulting from the variable presence of supportive macroscopic and microscopic findings at autopsy and histology. Consequently, there is a need to find alternative biological fluids should urine prove unavailable during postmortem investigations.
In the study herein described, concentrations of catecholamines and their O-methylated metabolites were measured in urine and vitreous humor samples collected during autopsy in a series of hypothermia fatalities and control cases that underwent medicolegal investigations. The aim of our analyses was to characterize catecholamine and their O-methylated metabolite profiles in vitreous humor samples and therefore evaluate their diagnostic potential in identifying hypothermia fatalities in the forensic setting.
Materials and methods
Study design and study populations
The present study was performed in 2013–2015. A total of 80 autopsy cases (41 males and 39 females) with a mean age of 44.5 years (range 21–69) were selected. Two study groups were prospectively formed, the first consisting of 40 hypothermia fatalities and the second consisting of 40 cases in which hypothermia as the main or contributory cause of death was excluded.
In order to collect a sufficient number of hypothermia-related death cases, 3 medico-legal centers in 3 different European countries were involved in the study. Both study groups were prospectively selected during the study period.
Inclusion criteria for the hypothermia group were:
-
circumstantial elements suggesting antemortem exposure to cold,
-
macroscopic and microscopic findings consistent with the hypothesis of hypothermia-related deaths (hemorrhagic spots of the gastric mucosa, frost erythema over the extensor surfaces of the large joints, synovial membrane hemorrhages and bloody discoloration of synovial fluid, generally observed in about 35–75 % of cases),
-
postmortem biochemical investigation results supporting the diagnosis of cold-related stress (increases in blood acetone/beta-hydroxybutyrate levels, increased blood cortisol and free fatty acid concentrations, and increased urine free cortisol values),
-
the availability of both urine and vitreous humor during autopsy,
-
exclusion of other causes of death based on all postmortem investigation findings.
All cases included in the hypothermia group occurred on dry land, originated from forensic practice, and underwent medicolegal autopsies as requested by local inquiring authorities. Postmortem intervals (defined as time elapsed between body discovery and specimen collection) ranged from 4 to 72 h. All individuals died without having undergone cardiopulmonary resuscitation, hospital admission, or catecholamine administration. No adrenaline was administered in the eyes during investigations at the death scene. Cases suspected of carrying primary ocular diseases or ocular traumas were excluded. According to medical records, none of these subjects had a previous history of renal failure or impaired renal function.
Non hypothermia-related deaths (control cases) included:
-
20 cases of death characterized by short agony. This was defined as a period of a few seconds up to a few minutes (10 cases of death involving individuals who had suddenly died in the presence of witnesses without acute coronary thrombosis/acute myocardial infarction at autopsy and 10 cases of thoracic trauma due to traffic accidents),
-
20 cases of death characterized by long agony. This was defined as a period lasting from several minutes up to hours (10 cases of severe thoracic and/or abdominal trauma due to traffic accidents and 10 cases of death involving individuals with acute coronary thrombosis and acute myocardial infarction at autopsy).
As in the hypothermia group, all these individuals died without hospital admission or catecholamine administration. No adrenaline was administered in the eyes during investigations at the death scene. Cases suspected of carrying primary ocular diseases or ocular traumas were excluded. According to medical records, none of these subjects had a previous history of renal failure or impaired renal function. Postmortem intervals (defined as time elapsed between body discovery and specimen collection) ranged from 6 to 68 h.
Inclusion criteria consisted of:
-
exclusion of hypothermia as the main or contributory cause of death,
-
the availability of both urine and vitreous humor during autopsy.
Postmortem investigations and sample collection
Complete, conventional medicolegal autopsies, histology, toxicology, and biochemical investigations were performed in all cases. Autopsies were jointly performed by two forensic pathologists (at least one board-certified) as in accordance with both local standards and international guidelines for medicolegal cases. Conventional histology included hematoxylin-eosin (HE) staining of brain, heart, lung, liver, and kidney samples. Histology of the kidney confirmed the absence of significant renal disease in the selected cases. Postmortem biochemical analyses were performed as part of the medicolegal investigations.
Undiluted vitreous humor samples (between 1 and 3 ml) were obtained by aspiration using a sterile needle and syringe. Right and left vitreous samples were collected through a scleral puncture at the lateral canthus, aspirated from the center of each eye, pooled in the same syringe and mixed together. All samples were immediately frozen after collection and kept frozen until analysis. Frozen vitreous humor samples were subsequently dispatched in dry ice from each medicolegal center and transported to the laboratory for analysis.
Urine samples (between 5 and 10 ml) were collected by bladder aspiration using a sterile needle and syringe during postmortem examination. Based on the results of former investigations, urine was collected in preservative-free tubes without acidification [1]. All samples were frozen after collection and kept frozen until analysis. As with the vitreous samples, frozen urine samples were subsequently dispatched in dry ice from each medicolegal center and transported to the laboratory for analysis.
Laboratory assays
Catecholamines (epinephrine, norepinephrine, and dopamine), metanephrines (metanephrine and normetanephrine), and 3-methoxytyramine were analyzed in urine and vitreous humor samples using high-performance liquid chromatography (HPLC) with amperometric detection, as previously described [10].
The measured values in urine were related to creatinine concentrations in urine and were expressed in nmol/mmol creatinine. Clinical reference intervals of metanephrines and catecholamines in urine were obtained from clinical literature [11, 12]. Cutoff levels discriminating hypothermia-related deaths and control cases were chosen according to the results of former investigations (adrenaline/epinephrine: 40 nmol/mmol creatinine; metadrenaline/metanephrine: 95 nmol/mmol creatinine).
Measured concentrations in vitreous humor were expressed in nmol/l. Cutoff levels discriminating hypothermia-related deaths and control cases were not preliminarily identified.
Urine creatinine was determined (Jaffé method, rate-blanked and compensated) by Roche standard methods on the Roche Modular P system (Roche Diagnostics GmbH, Mannheim, Germany). Creatinine levels in urine were expressed in mmol/l.
Statistical analysis
Data were analyzed using GraphPad Prism software 6.0 (published by GraphPad Software, Inc., La Jolla, CA, USA) as a statistical unit. Concentrations of catecholamines and their O-methylated metabolites in urine and vitreous humor in hypothermia-related deaths and control cases (and within control cases) were compared nonparametrically by the Mann–Whitney U test. p values less than 0.05 were considered statistically significant.
The relationship between catecholamine and their O-methylated metabolite concentrations in urine and vitreous in hypothermia fatalities and control cases was also explored.
Results
Tables 1, 2, and 3 summarize the main results obtained in all studied groups in urine and vitreous samples.
As expected, urine catecholamine, metanephrine, and 3-methoxytyramine concentrations were significantly higher in hypothermia-related deaths compared to those in the control group. In the latter, absolute values for adrenaline, noradrenaline, dopamine, metanephrine, normetanephrine, and 3-methoxytyramine failed to show significant differences relating to the cause of death.
Analysis of the results obtained from catecholamine, metanephrine, and 3-methoxytyramine measurements in vitreous humor did not reveal statistically significant differences between hypothermia-related deaths and control individuals. In the latter, absolute values for adrenaline, noradrenaline, dopamine, metanephrine, normetanephrine, and 3-methoxytyramine failed to show significant differences relating to the cause of death.
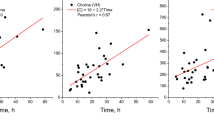
Lastly, no increase in vitreous catecholamine, metanephrine, or 3-methoxytyramine concentrations was observed in relation to their urinary levels in either of the studied groups.
Globally considered, these results seem to suggest that, contrary to urine catecholamines and their O-methylated metabolites in situations of cold-related stress and death, vitreous levels of these compounds in suspected hypothermia cases are of scarce diagnostic value and can hardly be used in the forensic setting to support de diagnosis of hypothermia.
Discussion
Catecholamines (dopamine, norepinephrine, and epinephrine) constitute a class of chemical neurotransmitters and hormones that occupy key positions in the regulation of physiological processes as well as in the development of neurological, psychiatric, endocrine, and cardiovascular diseases [13].
The term metanephrines describes two catecholamine metabolites: normetanephrine (the O-methylated metabolite of norepinephrine) and metanephrine (the O-methylated metabolite of epinephrine). The corresponding O-methylated metabolite of dopamine (3-methoxytyramine) is not generally considered a metanephrine. The catechol-O-methyl-transferase catalyzes the O-methylation of the 3-hydroxyl group of dopamine, norepinephrine, and epinephrine [14].
The term urinary “total” metanephrines was coined to describe both normetanephrine and metanephrine measured together as a single concentration by early spectrophotometry assays. These have been superseded by HPLC assays that allow separate measurements of normetanephrine and metanephrine, termed “fractionated” metanephrines [15].
Catecholamines and metanephrines are present in plasma and urine in free (unconjugated) and sulfate-conjugated forms. In humans, sulfate-conjugates are formed from free amines by the action of a specific sulfotranferase isoenzyme, monoamine-preferring sulfotranferase (SUTL1A3). This enzyme is located in high concentrations in the gastrointestinal tract, the source of most sulfate-conjugated catecholamines produced in the body. The sulfate conjugation of metanephrines gives rise to hydrosoluble metabolites, considered as end point products eventually eliminated in urine [14–16].
Free (unconjugated) metanephrines are cleared from the blood circulation rapidly and then further metabolized by monoamine oxidase (with subsequent vanillylmandelic acid formation) or monoamine-preferring sulfotransferase (with subsequent sulfate-conjugated metanephrine formation). As metabolic end-products, sulfate-conjugated metanephrines are cleared from the circulation slowly, with clearance depending almost entirely on elimination by the kidney (and, consequently, with increased plasma concentrations in patients with renal failure). In contrast, circulatory clearance of free metanephrines is influenced by the kidney to a lesser extent, with plasma concentrations of these analytes less importantly affected by impaired renal function [6, 15].
It is known that reactions to stressful situations of various natures are characterized by enhanced secretion of catecholamines. Prolonged exposure to cold leading to death is the most typical situation of forensic interest characterized by intense stress reaction and subsequent sympatico-adrenal activation, the latter responsible for increases in catecholamine levels in blood and, consequently, in urine [1, 7, 17]. Moreover, the conclusions of a recent study appeared to indicate that the hypothesis of antemortem cold exposure, intense stress reaction, and hypothermia-related death would be supported by increases of both catecholamines and their O-methylated metabolites in urine [1].
Catecholamine measurements in biological samples collected at autopsy (postmortem serum from peripheral and cardiac blood, vitreous humor and urine as well as pericardial and cerebrospinal fluids) in causes of death other than hypothermia fatalities have been occasionally carried out in the forensic setting. It has been speculated that the concomitant determination of catecholamine levels in different postmortem specimens could help semi-quantify stress intensity and the role of stress reactions in the pathogenesis of death. In addition, it has been postulated that high noradrenaline levels in cerebrospinal fluid or vitreous humor would be especially indicative of antemortem protracted stress [18–23].
Specifically concerning catecholamine determination in vitreous humor samples collected at autopsy, Wilke et al. [20] performed a study involving 98 medicolegal cases with various causes of death and agonal phase durations. They observed that the measured adrenaline and noradrenaline values in vitreous humor exclusively allowed cases that had documented catecholamine administration during cardiopulmonary resuscitation to be distinctively identified from other investigated cases (those with short or long agonal periods without catecholamine administration during cardiopulmonary resuscitation). These authors concluded that their own findings were not in agreement with those reported by Kernbach-Wighton et al. [24], who had measured significantly different adrenaline/noradrenaline ratios in vitreous humor depending on the cause of death and agony duration.
As far as vitreous catecholamine values in situations of cold-related stress are concerned, forensic literature in this field is quite limited at present.
Lapinlampi and Hirvonen [8] measured noradrenaline, adrenaline, and dopamine concentrations in vitreous humor and urine samples collected from 5 groups of animals (adult guinea pigs) with different causes of death and corpse storage conditions before sample collection (death following cold exposure without subsequent postmortem autolysis, death following cold exposure with subsequent postmortem autolysis, sudden death and immediate animal freezing, sudden death and immediate animal storage in warm conditions, sudden death and immediate sample collection without animal storage whatsoever).
According to their results, the highest vitreous noradrenaline concentrations were found in the two groups of animals that had cold exposure (with and without autolysis), with higher levels in the group that had cold exposure followed by autolysis. Nevertheless, differences between cold exposure with autolysis and cold exposure without autolysis were not statistically significant, nor were those between cold exposure without autolysis and autolysis alone. This suggested the effect of autolysis (individually considered) on vitreous noradrenaline levels likely due to diffusion of noradrenaline during storage from the nerve endings in the retina. Analogously, the highest vitreous adrenaline values were found in the two groups of animals that had cold exposure (with and without autolysis), with higher levels in the group that had cold exposure followed by autolysis [8].
Though Lapinlampi and Hirvonen [8] indicated that the autolysis effect was not observed with adrenaline concentrations in vitreous humor, statistically significant differences can be noticed when comparing sudden death and autolysis to sudden death and immediate freezing (p = 0.0139) as well as when comparing sudden death and autolysis to sudden death and immediate sampling (p = 0.0336). The authors emphasized that postmortem autolysis did not appear to significantly influence adrenaline and noradrenaline concentrations in urine. Hence, they concluded that urine samples would be preferred as primary evidence in hypothermia fatalities and recommended careful interpretation of vitreous noradrenaline levels due to the possible effects of autolysis on analyte diffusion [8].
The results of our investigations do not seem to confirm those by Lapinlampi and Hirvonen [8] in laboratory animals exposed to cold, and did not show increased vitreous catecholamine levels in situations of cold-related stress responses.
The limitations of our study must be acknowledged. The most important is the relatively small number of studied cases, which may limit the accuracy of our research. However, precise selection criteria were applied during the recruitment process in all studied groups and subgroups in order to minimize heterogeneity in the study populations. Prospective investigations, including a greater number of subjects, are therefore needed to confirm or invalidate our findings.
Key points
-
1.
Increases in catecholamines and their O-methylated metabolites in urine collected at autopsy may support the diagnosis of hypothermia fatalities.
-
2.
Catecholamine determination in vitreous humor samples in causes of death other than hypothermia has been very rarely performed in the forensic setting.
-
3.
Postmortem autolysis appears to be responsible for increases in vitreous noradrenaline levels in laboratory animals with various causes of death and corpse storage conditions.
-
4.
Vitreous catecholamine and their O-methylated metabolite concentrations appear to be of limited value in characterizing human antemortem stress reactions due to cold exposure.
References
Palmiere C, Teresiński G, Hejna P, Mangin P, Grouzmann E. Diagnostic performance of urinary metanephrines for the postmortem diagnosis of hypothermia. Forensic Sci Med Pathol. 2014;10:518–25.
Goldstein DS, Eisenhofer G, Kopin IJ. Sources and significance of plasma levels of catechols and their metabolites in humans. J Pharmacol Exp Ther. 2003;305:800–11.
Nohta H, Mitsui A, Umegae Y, Ohkura Y. Determination of free and total catecholamines in human urine by HPLC with fluorescence detection. Biomed Chromatogr. 1987;2:9–12.
Grouzmann E, Lamine F. Determination of catecholamines in plasma and urine. Best Pract Res Clin Endocrinol Metab. 2013;27:713–23.
Jeyaraman K, Natarajan V, Thomas N, Jacob PM, Nair A, Shanthly N, et al. The role of urinary fractionated metanephrines in the diagnosis of phaeochromocytoma. Indian J Med Res. 2013;137:316–23.
Eisenhofer G, Huysmans F, Pacal K, Walther MM, Sweep FC, Lenders JW. Plasma metanephrines in renal failure. Kidney Int. 2005;67:668–77.
Pakanen L, Kortelainen ML, Särkioja T, Porvari K. Increased adrenaline to noradrenaline ratio is a superior indicator of antemortem hypothermia compared with separate catecholamine concentrations. J Forensic Sci. 2011;56:1213–8.
Lapinlampi TO, Hirvonen JI. Catecholamines in the vitreous fluid and urine of guinea pigs dying of cold and the effect of postmortem freezing and autolysis. J Forensic Sci. 1986;31:1357–65.
Teresiński G, Buszewicz G, Madro R. The influence of ethanol on the level of ketone bodies in hypothermia. Forensic Sci Int. 2002;127:88–96.
Grouzmann E, Fathi M, Gillet M, de Torrenté A, Cavadas C, Brunner H, Buclin T. Disappearance rate of catecholamines, total metanephrines, and neuropeptide Y from the plasma of patients after resection of pheochromocytoma. Clin Chem. 2001;47:1075–82.
Grouzmann E, Drouard-Troalen L, Baudin E, Plouin PF, Muller B, Grand D, et al. Diagnostic accuracy of free and total metanephrines in plasma and fractionated metanephrines in urine of patients with pheochromocytoma. Eur J Endocrinol. 2010;162:951–60.
Pussard E, Neveux M, Guineno N. Reference intervals for urinary catecholamines and metabolites from birth to adulthood. Clin Biochem. 2009;42:536–9.
Eisenhofer G, Kopin IJ, Goldstein DS. Catecholamine metabolism: a contemporary view with implications for physiology and medicine. Pharmacol Rev. 2004;56:331–49.
Glauser M, Metrailler M, Gerber-Lemaire S, Centeno C, Seghezzi C, Dunand M, et al. Enzyme and acid deconjugation of plasma sulfated metanephrines. Clin Chim Acta. 2014;430:125–8.
Eisenhofer G. Free or total metanephrines for diagnosis of pheochromocytoma: what is the difference? Clin Chem. 2001;47:988–9.
Eisenhofer G, Lenders JW. Pacak. Biochemical diagnosis of pheochromocytoma. Front Horm Res. 2004;31:76–106.
Hirvonen J, Huttunen P. Increased urinary concentration of catecholamines in hypothermia deaths. J Forensic Sci. 1982;27:264–71.
Ishikawa T, Inamori-Kawamoto O, Quan L, Michiue T, Chen JH, Wang Q, et al. Postmortem urinary catecholamine levels with regard to the cause of death. Leg Med (Tokyo). 2014;16:344–9.
Tormey WP, Carney M, FitzGerald RJ. Catecholamines in urine after death. Forensic Sci Int. 1999;103:67–71.
Wilke N, Janssen H, Fahrenhorst C, Hecker H, Manns MP, Brabant EG, et al. Postmortem determination of concentrations of stress hormones in various body fluids - is there a dependency between adrenaline/noradrenaline quotient, cause of death and agony time. Int J Legal Med. 2007;121:385–94.
Kernbach-Wighton G. Diagnostic problems with functional cause of death: analytical approaches and procedures. Leg Med (Tokyo). 2009;11(Suppl 1):S31–5.
Zhu BL, Ishikawa T, Michiue T, Li DR, Zhao D, Quan L, et al. Postmortem serum catecholamine levels in relation to the cause of death. Forensic Sci Int. 2007;173:122–9.
Ishikawa T, Quan L, Michiue T, Kawamoto O, Wang Q, Chen JH, et al. Postmortem catecholamine levels in pericardial and cerebrospinal fluids with regard to the cause of death in medicolegal autopsy. Forensic Sci Int. 2013;228:52–60.
Kernbach-Wighton G, Sprung R, Saternus K-S. Zum Katecholaminspeigel bei Unterkühlung. 11 Frühjahrstatung der Deutschen Gesellshaft für Rechtsmedizin, Region Nord, 31 May–1 June 2002. Potsdam Rechtsmed. 2003;1:44–45.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hervet, T., Teresiński, G., Hejna, P. et al. Catecholamines and their O-methylated metabolites in vitreous humor in hypothermia cases. Forensic Sci Med Pathol 12, 163–169 (2016). https://doi.org/10.1007/s12024-016-9764-2
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12024-016-9764-2