
Abstract
Although there is broad consensus that the state psychiatric hospital population drastically declined over the past five decades, the destination and well-being of people with serious mental illness (SMI) have been in greater doubt. In this article, we examine the aftermath of the deinstitutionalization movement. We begin with a brief historical overview of the move away from state hospitals, followed by an examination of where people with SMI currently reside and receive treatment. Next, we review recent trends reflecting access to treatment and level of community integration among this population. Evidence suggests the current decentralized mental health care system has generally benefited middle-class individuals with less severe disorders; those with serious and persistent mental illness, with the greatest need, often fare the worst. We conclude with several questions warranting further attention, including how deinstitutionalization can be defined and how barriers to community integration may be addressed.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
It has been well-documented that the number of individuals in state psychiatric hospitals in the United States decreased dramatically over the past 50 years [1, 2]. The total number of residents in state hospitals peaked in 1955, with almost 559,000 inpatients, and fell to 47,000 in 2003. Though President John F. Kennedy called for a 50 % reduction in the number of state psychiatric patients in his address to Congress outlining the Community Mental Health Centers Act of 1963 [3], the depopulation of state hospitals would ultimately reflect a startling drop of more than 90 % [1, 4, 5••].
Societal shifts affecting de-hospitalization include a vast increase in the number of mental health professionals and community-based treatments since World War II, changing public perception and attitudes toward mental illness, and legal advocacy efforts related to psychiatric hospitalization [2, 6]. However, economic incentives to diversify psychiatric services may be the single most important factor shaping the currently decentralized mental health care system. Fundamental changes in the mental health system over the past 50 years have impacted where people with serious mental illness (SMI) currently reside and receive treatment, as well as shaping their overall quality of life since the depopulation of state hospitals [1, 2]. By examining recent trends related to mental health care spending, fragmentation and quality of mental health services, mental health disability rates, employment status, housing availability, and incarceration among this population, we seek insights into whether deinstitutionalization exists for the majority of people with SMI, and how the depopulation of state hospitals relates to present-day levels of community integration.
Historical Overview
The depopulation of state hospitals was precipitated by major societal forces that began to emerge in the 1950s. The post–World War II era gave rise to three such shifts: 1) in the wake of the Great Depression and the war, state hospitals were severely lacking in resources and subject to extreme understaffing and overcrowding; 2) the “combat neurosis” phenomenon of World War II led to high “psychiatric casualty rates” [6] and necessitated a large increase in efforts to train psychiatrists, clinical psychologists and other mental health professionals; and 3) World War II brought about an expansion of the federal government that ultimately led to the development of the National Institute of Mental Health in 1949 [7, 8]. Subsequent research into the etiology and treatment of SMI, along with the rapid expansion of clinically trained mental health professionals and the advent of psychiatric drug therapy, accelerated an outpatient model of community psychiatry that provided an alternative to lifelong institutionalization in state psychiatric hospitals.
With the use of the first psychiatric medication in 1954, chlorpromazine, mental health professionals began to view psychotic patients as manageable, and the notion of self-management among people with psychotic disorders began to grow [9–11, 12•]. While community-based mental health treatment expanded throughout the 1950s, increased awareness of the neglect and abuse of patients in state hospitals sparked social concern and catalyzed public protest during the 1960s [12•]. Accounts of conditions include descriptions of “naked humans herded like cattle” who were “stripped of every vestige of human decency” [13, 14]. New laws pertaining to the confinement and treatment of individuals with mental illness significantly increased the rate at which state psychiatric hospitals were depopulated. Informed by the civil liberties movement, advocates for the mentally ill challenged involuntary psychiatric commitment and succeeded in facilitating two key legal policies: 1) procedural due process with regard to involuntary commitment and 2) the establishment of minimally adequate standards of care. By the 1970s, the Supreme Court held, in O’Connor v. Donaldson, that an individual must present a danger to himself/herself and/or others to be constitutionally confined. Based on further rulings, the failure of state hospitals to meet judicially mandated standards of minimally required care led to the discharge of thousands of state psychiatric patients [10, 12•].
Shifting funding streams, such as the Community Mental Health Centers Act of 1963 and the advent of Medicaid and Medicare in 1965, further solidified the trend away from state hospitals. Through these programs, outpatient treatment was expanded and states gained financial incentives to move patients out of non–federally funded state hospitals into federally subsidized settings such as nursing homes and psychiatric wards of general hospitals [7, 11]. The growth of other social welfare programs during this period, such as Social Security Income (SSI), Social Security Disability Income (SSDI), and food stamps, also made direct benefits to people with SMI living in the community available. However, the Omnibus Budget Reconciliation Act of 1981 effectively ended direct federal funding of community-based mental health services, shifting treatment costs to individual states. This precipitated the rise of health maintenance organizations (HMOs) and private for-profit psychiatric hospitals in the 1980s and Managed Behavioral Health Organizations (MBHOs) throughout the 1990s [7, 15]. The impact of MBHOs on access to treatment, cost-shifting patterns, and community-based treatment options affecting individuals with SMI, discussed later in the review, continues today.
Where Are They Now?
While deinstitutionalization implies a definitive departure point of people with SMI from state hospitals, their destination has been more difficult to ascertain. Individuals with SMI are currently estimated at between 2.8 % and 7.2 % of the population [16] in the United States. Based on a comparison of data from several national sources, a comprehensive analysis of mental health care and the well-being of individuals with mental illness is offered in Better But Not Well: Mental Health Policy in the Unites States Since 1950 by Frank and Glied [1]. The authors estimate that of those with SMI, 15 % are noninstitutionalized, 7 % are in health care facilities, 5 % are in correctional facilities, 2 % are homeless, and the status of 71 % is unknown. Among the 15 % not institutionalized, nearly all were living with family (87 %), with the remaining in board-and-care facilities. Among those institutionalized in health care facilities, the population was distributed across “mental institutions” (2 %), nursing homes (3 %), and other health care facilities (2 %).
Building on the Frank and Glied [1] analysis with recent evidence described below, we provide an updated picture of where individuals with SMI can be found today. Tracking the whereabouts of people with SMI has proven to be a complex task for two major reasons. First, research in this area commonly focuses on the proportion of individuals in a specific setting who have SMI [17] rather than the total number of people with SMI in the population and where they reside. A downside of setting-specific prevalence rates is that the reader may come away without a scaled perception of how those with SMI are distributed in different living environments. To offer a balanced view, we thus seek to answer two central questions:
-
1.
Out of all people with SMI, how many are in specific settings? (Fig. 1)
Fig. 1 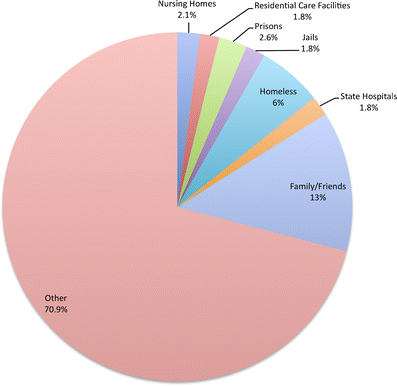
Proportion of the total number of people with serious mental illness (SMI) by setting. Percentages were calculated using prevalence rates reported and the 2008–2009 estimate of 10.4 million individuals with SMI (Data from Substance Abuse and Mental Health Services Administration, Center for Behavior Health Statistics and Quality. October 6, 2011. The NSDUH Report: State Estimates of Adult Mental Illness. Rockville, MD)
-
2.
In specific settings, how many people have SMI? (Fig. 2).
Fig. 2 
Number of people with serious mental illness (SMI) by setting. Raw numbers not found in the evidence reported were extrapolated using the 2008–2009 estimate of 10.4 million individuals with SMI (Data from Substance Abuse and Mental Health Services Administration, Center for Behavior Health Statistics and Quality. October 6, 2011. The NSDUH Report: State Estimates of Adult Mental Illness. Rockville, MD)


Second, determining precise estimates of where people with SMI reside and receive treatment is difficult due to considerable confusion in the literature, as evidenced by the following: 1) researchers often use the labels “mental illness” and “serious mental illness” interchangeably, without defining either label; 2) a limited number of settings have the necessary oversight to maintain reliable counts of individuals with SMI; and 3) researchers have not used uniform terminology when referring to various settings (e.g., residential care facilities [RCFs] may include a variety of facility types [such as board-and-care and group home]). Given these limitations, we present our best efforts to discern trends related to SMI in the context of nursing homes, correctional institutions, state psychiatric hospitals, residential care facilities, and on the streets.
Nursing Homes
According to the National Nursing Home Survey conducted by the Centers for Disease Control and Prevention [18], 1.5 million individuals reside in nursing homes. Given that the prevalence of SMI has been estimated at between 9 % and 20 % of all nursing home residents [19], we approximate that 217,500 individuals with SMI live in nursing home facilities. Among those with SMI, 6 % to 12 % were diagnosed with schizophrenia [20, 21] and 10 % to 44 % had significant depressive symptomatology [22•, 23]. In 2005, 19 % of the 996,311 new nursing home admissions were diagnosed with a mental illness other than dementia [22•]. In fact, the number of new admissions with a mental illness other than dementia was 50 % higher than those with dementia alone [22•]. The mass entry of people with mental illness into nursing homes is especially problematic because the quality of care is sometimes questionable [24], and those with SMI are more likely to be admitted to nursing homes with more deficiencies in overall and clinical care quality [25].
Residential Care Facilities
Distinct from nursing homes, RCFs provide nonmedical personal care and oversight for medication use [26]. Whereas nursing homes receive federal funding and are subject to greater oversight, residential facilities receive minimal funding; thus, no standardized federal definition for RCFs has been established [27]. RCFs have been variably termed “board-and-care homes, adult residential facilities, adult foster homes, community care homes, supervisory care homes, sheltered care facilities, continuing care facilities, transitional living facilities, and group homes,” among others [26]. After calculating a ratio of those with mental illness in residential facilities to nursing homes in California, Fleishman [26] extrapolated a national estimate of 157,956 people with mental illness in RCFs. We updated this figure based on SAMHSA’s report on the State Regulation of Residential Care Facilities for Adults with Mental Illness [27] and the recent National Survey of Residential Care Facilities [28]; these studies respectively provide an approximation of individuals with SMI who reside in RCFs that do and do not specialize in serving those admitted for a primary mental illness diagnosis. Extrapolating from the available data, we estimate that 183,789 individuals with SMI reside in RCFs, which is consistent with the Fleishman [26] assertion that his estimate likely represented an undercount of those with SMI in RCFs.
Correctional System
Although deinstitutionalization sought to release psychiatric patients from confinement, entrenchment in the correctional system has now become a stark reality for many with SMI. While estimates vary substantially across studies [29], the rates of SMI among prisoners are consistently higher than among those living in the community [30]. A recent study found three times more individuals with SMI in prisons and jails than in hospitals [31]. Also, the rates of SMI for those booked into jails are three to six times higher than in the general population [17], with similar findings observed in prisons [32]. Nearly 1 million individuals with SMI are booked into jail on an annual basis [33], and the number of people with SMI in prison was conservatively estimated at 150,000 in 2007 [29, 34]. Overall, epidemiologic evidence suggests that 15 % to 24 % of inmates have an SMI [35]. Furthermore, while just over one third of state prisons confirmed having protocols for the treatment and management of mental illness [36], one study found that 43 % of state prisoners with SMI had a release date within 12 months and still had not received mental health treatment [37]. Prisoners with SMI are subject to longer stays, have a lower likelihood of qualifying for community supervision, are more likely to have their parole revoked [38], and have higher rates of recidivism [29] than prisoners without SMI. Entrenchment, as opposed to involvement, often describes the status of individuals with SMI in the correctional system [39].
Homelessness
The issue of where those with SMI should be housed has brought attention to the rapid growth of the homeless population in the United States over the past several decades [40]. It is estimated that 636,017 adults are homeless on any given night in the United States [41], with as many as 2.15 million experiencing homelessness on an annual basis [42]; of these, 25 % to 33 % have an SMI [1, 43, 44]. Research suggests that 28 % of the sheltered homeless have an SMI [45], however, this estimate does not include people with SMI who may be among the 42 % of unsheltered homeless [46]. One study found that 36 % of those with mental illness discharged from a state hospital became homeless within 6 months [47]. Not surprisingly, homelessness has been identified as a risk factor for high utilization of psychiatric emergency services [48] and psychiatric rehospitalization [49].
The New State Hospital
Finally, there is recent growth in state psychiatric hospital admissions and residents for the first time in more than 50 years [5••, 50]. Based on state-level data gathered from the Center for Mental Health Services, Manderscheid and colleagues [5••] found a 21.1 % increase in the number of admissions to state psychiatric hospitals between 2002 and 2005, from 156,000 to 189,000 people—the first such increase since 1971. Additionally, there was a slight upturn in the number of total residents at year-end for the first time since 1955. Increased numbers of people with SMI within the criminal justice system may be driving much of the state hospital population increase [5••, 51–53]. For example, forensic patients can be committed to state hospitals when criminal courts question their competency or they have been found incompetent to stand trial [50]. Individuals nearing completion of their prison sentence who are deemed a continued threat to society may also be committed, along with individuals adjudicated as not guilty by reason of insanity. Many private psychiatric units are unwilling to admit people who appear difficult to discharge, such as those with past criminal histories [50], but state psychiatric hospitals have greater bed capacity and are designed to accept such patients.
Data from the National Association of State Mental Health Program Directors Research Institute [51] indicate that in 2004, 35 % of the 40,000 residents in 36 state hospitals were forensically involved mental health consumers. Some state hospitals report more than half of beds are occupied by patients with criminal justice involvement [52], and new construction of state hospitals dedicated solely to forensically linked patients is on the rise [53]. There is concern that the number of available beds is simply not enough for the prevailing need, particularly for those in the civil system who need psychiatric hospitalization [54]. Using California as an example, Lamb and Weinberger [54] noted that 90 % of the residents were forensic patients, with only 10 % of state hospital beds allocated for those in the civil system; this translates to less than 1.5 beds per 100,000 population. Highlighting the perceived deficiency in capacity, a recent report from the Treatment Advocacy Center [55] suggests an additional 96,000 beds are required to satisfy minimum treatment standards. Most state psychiatric hospitals are now accredited and have policies in place to protect the rights of their patients—a departure from the “shame of the states” of 60 years ago [56]. However, despite improved conditions, they seem to retain much of their original function, serving those that other institutions and programs cannot or will not serve, and segregating segments of the population perceived as deviant [50].
Finding the Right Label
Evidence reviewed here corroborates the notion that shifting individuals from a centralized institutional locus of care (i.e., the state hospital) to multiple and differentiated institutions and care facilities (e.g., nursing homes and prisons) does not represent a process of deinstitutionalization, but rather trans-institutionalization. Along these lines, Geller [2] used the term dehospitalization, which “seems more accurate for describing a phenomenon of transferring patients out of state hospitals because it implies no judgment about whether where they went could be considered an institution.” Though the large proportion of individuals with SMI who are homeless may be technically defined as “deinstitutionalized,” their living conditions and welfare raise obvious questions about the intent of the deinstitutionalization movement. Thus, we now turn our attention from where they are to how they are by looking at trends related to the intended goal of community integration upon which the “deinstitutionalization” movement was originally based.
How Are They Now? Recent Trends in Mental Health Care and Community Integration among People with Serious Mental Illness
Access, Utilization, and Cost of Mental Health Care
The fundamental reorganization of the mental health system over the past several decades has given rise to advances in many domains for people with mental illness [1]. The previously mentioned wide-ranging analysis of mental health care conducted by Frank and Glied [1] depicts steady progress in the lives of individuals with mental illness since President Kennedy’s original speech to Congress in 1963. For example, from 1950 to 2006, access to mental health treatment has steadily risen, the quality of care for major mental disorders continues to improve (especially in the area of pharmacotherapy), out-of-pocket costs for people with mental disorders have remained constant or declined, and housing and income status for people with mental illness have improved overall [1, 57••]. The advent of social welfare programs such as Medicare, Medicaid, SSI, and SSDI is identified as a major force shaping these improvements. However, aggregated trends reflecting overall improvements for people with mental illness may mask contrasting and adverse trends in mental health service access, delivery, financing, and well-being of people with severe and chronic mental illnesses such as schizophrenia. While the decentralization and diversification of psychiatric services has generally benefited middle-class individuals with less severe disorders, this shift has given rise to unforeseen problems and complexities that disproportionately affect more severely impaired segments of the mentally ill population [1, 58•]. In their most recent work, Glied and Frank [57••] analyzed trends in mental health financing, access to care, and well-being for people with mental illness, and conclude that despite consistent gains in these domains, “not all people with mental health problems have shared in these improvements.”
Recent trends in mental health spending and access to services reflect discrepancies between those with less severe disorders and those individuals with SMI. Mental health care spending on hospitalization and outpatient care has remained virtually constant from 1996 to 2006 [59] due to factors such as the adoption of MBHOs and reductions in the role of costly psychiatric inpatient care that have effectively controlled spending growth. Interestingly, though, the number of Americans receiving mental health treatment has increased by 50 % since 1977 [1]. Additionally, federal policymakers report sharp increases in mental health spending as a primary budgetary concern.
Frank and Glied [60] make sense of these contradictory trends by arguing that the apparent “flat” spending on mental health care over the past several decades “masks profound changes in the nature of mental health service delivery” within different categories of mental health care spending. For example, the rise of MBHOs led to reduced co-payments and increased use of mental health services among individuals with less severe mental health disorders [59]. Since the late-1980s, prescription drug spending, particularly on antidepressants, has increased dramatically. Increased prescribing of psychotropic medications through primary health care has played a central role in raising the rate at which general physicians diagnose and treat mental health problems in the general population, yet access to care among those impaired by mental illness has declined. Among adults, the rate of a mental health diagnosis being recorded at a primary care visit increased 30 % between 1996 and 2006. In contrast, the number of contacts with a mental health professional among adults impaired by a mental illness dropped from 51 % to 44.6 % during the same period. The upsurge in treatment rates in primary care, in which individuals are likely to have less severe mental health conditions, in conjunction with declines in treatment among those who are functionally impaired may represent a pattern of excluding the most severely mentally ill from treatment while expanding care for those with less severe conditions [59]. The proportion of adults impaired by mental illness reporting difficulties accessing a mental health professional was in excess of 30 % in 2002, and continues to rise.
While managed care has successfully contained overall mental health care costs by limiting spending on outpatient and inpatient care and shifting treatment costs to drugs, this pattern does not support the expansion of evidence-based rehabilitation treatments that are essential for people with SMI. Some researchers contend that the expansion of psychopharmacology has been at the expense of developing and funding a range of mental health treatment options, but even if such options were available, the lack of practitioners trained to provide evidence-based treatments likely would impede their rapid delivery [58•, 61].
Service Fragmentation and Community Integration for the Seriously Mentally Ill
Service fragmentation within the current mental health system, an unintended consequence of shifting funding streams and the diversification of mental health services, has also hindered community integration for people with SMI. Institutions and services aimed at subspecialties such as eating disorders, forensic psychiatry, and addictions, to name a few, have led to differentiated settings, treatment guidelines, and funding streams for services [58•]. Although there have been advances in expertise and treatment based on this pattern of specialization, “fragmentation of interests leads indirectly to fragmentation of services” [62]. The arrival of the Medicaid program, the largest single driver of current mental health care for people with SMI, is a primary example of mental health cost shifting affecting fragmented services. While this program has resulted in undeniable benefits for people with mental illness [1], the reliance on Medicaid to finance the majority of mental health services for this population has also dispersed responsibility for care to multiple federal, state, and local agencies [63].
Based on a survey of Medicaid directors in 50 states, Verdier and Barrett [64] found that Medicaid agencies have insufficient clinical input from mental health providers, while mental health agencies lack understanding of the regulatory and fiscal constraints pertaining to the Medicaid program. This “growing disconnect between what the mental health system views as ‘best practice’ and what the Medicaid program is able to cover” [64], in combination with an overall absence of cohesive national mental health care policies and leadership has led to significant gaps in care and a poorly coordinated network of institutions and services for people with SMI [58•, 63]. Concurrent social and demographic shifts since the depopulation of state psychiatric hospitals, such as growing divorce rates, increased geographical mobility, and a rapid rise in the number of women in the labor market, have simultaneously impinged on the capacity of families and informal networks to provide care for the seriously mentally ill within the community [58•, 65].
The resultant dependence of individuals with SMI on facilities such as nursing homes and residential treatment programs poses a significant challenge to the goal of community integration. Conditions such as understaffing, lack of stimulation, absence of evidence-based treatments, and social isolation are not uncommon in treatment and residential programs for people with SMI [66, 67•]. For example, studies indicate that few nursing homes provide psychiatric rehabilitation services of any kind [68], and barely more than one-third of nursing home residents receive a mental health visit over the course of a year [69]. In addition, a substantial segment of this population may have the functional capacity to live in less restrictive environments with proper treatment and financial resources [67•]. Aschbrenner and colleagues [67•] found that individuals with SMI tend to be younger and require less help with activities of daily living than those with other conditions in nursing homes, yet they are more likely to become long-stay residents. While it has been duly noted that some individuals with mental illness may have deficits that make them unsuitable for discharge from nursing homes [24], an alarming finding is that those with SMI, the most at-risk segment of the population with mental illness, are more likely to be admitted to nursing homes with greater deficiencies in care [25].
Importantly, Aschbrenner et al. [67•] cite ambiguity of Medicaid regulations and lack of coordination between state and federal entities in screening and evaluation as major factors in inappropriate placement of individuals with SMI in nursing homes, along with a lack of alternative community-based treatment and housing options. Unfortunately, the plight of many of those with SMI in nursing homes bears a striking resemblance to the inadequate atmospheres of the institutions they formerly inhabited.
Community Functioning and Quality of Life for the Seriously Mentally Ill
Recent evidence related to mental health disability rates, employment status, and housing availability for people with SMI also conveys an unfavorable view of quality of life and community integration for this population. Disability awards due to mental illness have been steadily rising over the past several decades [70•]. Between 1987 and 2005, the share of SSI’s adult caseload who were disabled due to a mental disorder increased from 24 % to approximately 36 %. Even more striking, the number of SSDI awards due to mental illness rose from 2 % in 1978 to almost 30 % in 2005, though this growth largely reflects growth in the overall program. Most recently, Mojtabai [71••] analyzed data from the National Health Interview Survey [72] and found that self-reported mental health disability increased from approximately 3.2 million people in 1997 to approximately 5.2 million people in 2009, while disability attributed to other chronic conditions did not change significantly. In addition, the author found that high rates of comorbid mental health and chronic medical conditions continue to rise. Conclusions based on these data are unclear because increased use of public income support programs is congruent with the goal of shifting away from the centralized state hospital system to independent living but also signifies continued functional impairment for individuals with mental illness. Furthermore, as Glied and Frank [57••] noted, improved living conditions that may have been achieved based on greater receipt of public benefits was likely offset by reduced access to affordable housing.
Evidence that 70 % of people diagnosed with a severe mental illness identify work as a primary goal while fewer than 15 % are employed [73] indicates that unemployment and resultant poverty are among the most substantial problems facing people with SMI today [62]. Unemployment and losses in productivity have been estimated at costing up to 32.4 billion dollars per year in the United States and comprise half of all schizophrenia-related costs [74]. Factors contributing to increasing use of psychiatric disability benefits and lack of successful employment for people with SMI are unclear, though insufficient access to supported employment may be one important contributor [62, 75]. While supported employment has shown superior outcomes compared with other vocational approaches [76], employment supports are not covered by Medicaid [62], hindering widespread availability of the intervention. Also, loss in disability benefits resulting from gainful employment serves as a disincentive to work for many people with SMI [62, 75]. Lastly, shifts in labor markets from manufacturing to service-oriented jobs requiring social skills that are often deficient among people with SMI may exacerbate poor employment outcomes [70•].
Poor employment status, poverty, and lack of affordable housing are highly intertwined barriers to independent living for people with SMI. Because the majority of this population relies on SSI and SSDI as their primary source of income [1, 77], poverty rates are extremely elevated. This widespread poverty has resulted in a phenomenon in which “people with SMI are priced out of the housing marketplace” [62]. As of 2006, the average rent for a modest one-bedroom apartment in the United States was estimated to cost 114 % of the average monthly SSI payment [62, 77]. Although Frank and Glied [1] identify the Section 8 housing subsidy program as a significant factor improving quality of life for people with mental illness, access to low-income housing has become increasingly difficult. Federal funds dedicated to low-income housing have decreased dramatically over the past three decades, while Section 8 housing has remained relatively constant [62, 77]. It is estimated that more than three times as many applicants qualify for low-income housing than receive it [78]. Hogan [62] suggests that the housing predicament is too immense to remedy with the development of specialized mental health housing alone and cannot be solved without federal leadership.
Recent evidence suggests that the health status of the severely mentally ill in the community is seriously compromised. People living with SMI in the United States die on average 25 years earlier than those in the general population largely due to preventable medical conditions and suboptimal medical care [79]. Studies have found higher incidence of many physical disorders among people with SMI, such as diabetes [80, 81], obesity [79], high cholesterol or dyslipidemia [82], metabolic and cardiovascular problems [83, 84], and cancer [85]. When combined with an SMI, physical illness can lead to other health conditions [86] and to a lower quality of life compared to both those in the general population and individuals with mental illness alone [87, 88]. These negative health consequences can affect other recovery goals such as housing, vocational training, and education [89].
Lastly, increased involvement in the criminal justice system has led to a vicious cycle of shrinking social capital impeding community integration among this population. Not only are people with SMI overrepresented in the criminal justice system, they often have longer incarcerations and maintain tenuous relationships with probation and parole officers [39]. Recent evidence also suggests higher rates of homelessness and general medical problems among people with SMI who have a history of incarceration [90]. Mentally ill ex-prisoners experience greater social isolation upon reentry from prisons and jails and often return to more limited social networks [91]. This population tends to reside in impoverished communities with high unemployment rates, high crime rates, fewer educational opportunities, and unstable housing [92, 93]. Open drug selling and high police presence in these communities often results in targeted drug arrests [93, 94]. These conditions contribute to increased recidivism rates among people with SMI, further undermining community tenure and the development of social resources [39]. Moreover, these stressors are compounded by a number of less visible punishments that restrict housing, parenting, voting, jury duty, political involvement, and medical assistance for all ex-prisoners [95, 96]. Despite recent attempts at the federal level to address the over-incarceration of this population, there is little proof that programmatic and policy shifts have had significant impacts on the number of people with SMI incarcerated [39].
Directions for Future Research and Mental Health Policy
Fifty years after the move away from state hospitals, several key questions regarding the concept and policies surrounding deinstitutionalization remain:
-
Are people with SMI deinstitutionalized? The evidence reviewed here, including the high proportion of people with SMI incarcerated and living in facilities that may be considered institutional, such as nursing homes, indicates the term deinstitutionalized may not apply to large segments of this population. However, a definitive answer to this question requires a clear and consistent definition of what comprises deinstitutionalized living. Currently, there are no agreed upon standards regarding what size facility, type of environment, and quality of care constitute “institutionalization.” Furthermore, the standardization and precise use of terminology for specific settings and how “serious mental illness” is defined in existing research is needed to accurately assess where people with SMI are residing and whether they can be considered deinstitutionalized.
-
Deinstitutionalization—or should the question be community integration? An implicit assumption of the deinstitutionalization movement is that moving out of state hospitals would result in fuller participation in community life. If an individual with SMI lives within the community and is socially isolated, physically ill, and impoverished, does this represent successful deinstitutionalization? Given that the vast majority of people with SMI lack employment, social relationships [97], involvement in community activities [98], and adequate medical care [79], it seems that deinstitutionalization and community integration represent distinct processes and constructs. Focusing on factors that may facilitate community integration as opposed to changing the locus of care may be important moving forward.
-
How can we address fragmentation of services that impede community integration? As previously mentioned, the current mental health care system is largely shaped by its greatest single funder, Medicaid. This has led to the administration of services by an entity that may not understand the nuances and complexities of mental illness and the determinants of community integration [99•]. The “medical home” concept developed for primary health care is one model aimed at addressing this fragmentation of interests and services. This approach entails consumers developing a relationship with a primary clinician who coordinates care with a range of rehabilitation and service providers, thereby creating a locus of care that is accessible, comprehensive, and coordinated.
-
Is institutionalized care necessary for some within the SMI spectrum? The majority of scholars and researchers examining the ramifications of de-hospitalization have alluded to the notion that inadequate funding of community-based services to replace long-term inpatient care has undermined successful community integration of people with SMI [5••]. Though insufficient availability of evidence-based treatments for SMI is the norm [61], some researchers have wondered whether it is also the case that subgroups within the SMI spectrum may require greater levels of structure, supervision, and institutionalized care regardless of other available treatment options [66]. Further research is needed to identify who may benefit from community-based services and under what conditions fuller community integration can be achieved.
-
Is the fundamental problem that the poor get poorer, and get poor services? If the intent of deinstitutionalization can be characterized as social inclusion rather than living in more diverse community-near institutions, then the shortcomings of this movement may be largely examined as an outgrowth of concentrated socioeconomic disadvantage among people with SMI. The reality is that this group is among the poorest in the United States [1]. Broad social and economic policy interventions, many of which are alluded to in this review, such as the creation of affordable housing, access to effective vocational rehabilitation, and employment without threat of losing public assistance benefits, are required to correct structural inequities that keep people with SMI from becoming active participants and stakeholders within the community. In concert with socioeconomic policies, greater access to mental health providers and evidence-based practices that are disproportionately lacking for people with SMI is needed.
Conclusions
While access to mental health care and the well-being of individuals with mental illness continues to improve overall, the shift from long-term psychiatric care in large and isolated state hospitals to a more diversified short-term outpatient care model may primarily benefit those with less severe mental health conditions. Current evidence suggests that those who are capable of maintaining a job, family, and other social resources while making use of mental health services are likely to gain benefit from the current system of mental health financing and treatment options [58•]. In contrast, those with more severe and chronic mental illnesses, with the greatest need, often fare the worst. Overall, evidence suggests that a high prevalence of functional impairment, unemployment, poverty, and isolation characterizes present-day life for most individuals with chronic and severe mental illness [58•, 71••, 73]. Following deinstitutionalization, individuals with SMI were discharged and seemingly scattered about, ending up everywhere and nowhere. Where are they now? While the answer to the question is not always easy to find, at least asking the question implies that someone is looking, and we need to be asking both where they are and how they are.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Frank R, Glied S. Better but not well: mental health policy in the United States since 1950. Baltimore: Johns Hopkins University Press; 2006.
Geller J. The last half-century of psychiatric services as reflected in psychiatric services. Psychiatr Serv. 2000;51(1):41–67.
Gronfein W. Incentives and intentions in mental health policy: a comparison of Medicaid and community mental health programs. J Heal Soc Behav. 1985;3:192–206.
Witkin M, Atay J, Manderscheid R. Trends in state and county mental hospitals in the US from 1970 to 1992. Psychiatr Serv. 1996;47:1079–81.
•• Manderscheid R, Atay J, Crider R. Changing trends in state psychiatric hospital use from 2002 to 2005. Psychiatr Serv. 2009;60(1):29–33. This recent article documents important trends related to increases in the state psychiatric hospital population and identifies relevant factors related to this increase (e.g., forensic admissions).
Scull A. Psychiatry and the social sciences, 1940–2009. Hist Polit Econ. 2010;42 suppl 1:25–52.
Accordino M, Porter D, Morse T. Deinstitutionalization of persons with severe mental illness: context and consequences. J Rehabil. 2001;67(2):16–21.
Ray C, Finley J. Did CMHC’s fail or succeed? analysis of the expectations and outcomes of the community mental health movement. Admin Pol Ment Health. 1994;21:283–93.
Gronfein W. Psychotropic drugs and the origins of deinstitutionalization. Soc Probl. 1985;32(5):437–54.
Torrey F. Out of the shadows: confronting America’s mental illness crisis. Oxford: Wiley; 1997.
Rochefort D. From poorhouses to homelessness. Westport: Greenwood Publishing Group, Inc; 1997.
• Harcourt B. Reducing mass incarceration: lessons from the deinstitutionalization of mental hospitals in the 1960s. John M.Olin Law and Economics Working Paper No. 542 (2nd Series) and Public Law and Legal Theory Working Paper No. 335. Chicago: The University of Chicago Law School; 2011. This paper makes important observations regarding the relationship between incarceration trends and the depopulation of state hospitals.
Deutsch A. The shame of the states. New York: Harcourt, Brace; 1948.
Halpern J. The myths of deinstitutionalization: policies for the mentally disabled. Boulder: Westview; 1980.
Breakey W. The rise and fall of the state hospital. In: Breakey WR, editor. Integrated mental health services. New York: Oxford University Press; 1996.
Lora A, Bezzi R, Erlicher A. Estimating the prevalence of severe mental illness in mental health services in Lombardy (Italy). Community Ment Health J. 2007;43(4):341–57.
Steadman HJ, Osher FC, Robbins PC, Case B, Samuels S. Prevalence of serious mental illness among jail inmates. Psychiatr Serv. 2009;60:761–5.
Jones AL, Dwyer LL, Bercovitz AR, Strahan GW. The national nursing home survey: 2004 overview. National Center for Health Statistics. Vital Health Stat. 2009;13(167).
Linkins KW, Lucca AM, Housman M, Smith SA. Use of PASRR programs to assess serious mental illness and service access in nursing homes. Psychiatr Serv. 2006;57:325–32.
Mechanic D, McAlpine D. Use of nursing homes in the care of persons with severe mental illness: 1985–1995. Psychiatr Serv. 2000;51:354–8.
McCarthy JF, Blow FC, Kales HC. Disruptive behaviors in veterans affairs nursing home residents: how different are residents with serious mental illness? J Am Geriatr Soc. 2004;52:2031–8.
• Fullerton C, McGuire T, Feng Z, Mor V, Grabowski D. Trends in mental health admissions to nursing homes. Psychiatr Serv. 2009;60(7):965–71. The authors document important trends related to increasing admissions of people with mental illness into nursing homes.
Burrows AB, Satlin A, Salzman C, Nobel K, Lipsitz LA. Depression in a long-term care facility: clinical features and discordance between nursing assessment and patient interviews. J Am Geriatr Soc. 1995;43:1118–22.
Grabowski DC, Aschbrenner KA, Rome VF, Bartels SJ. Review: quality of mental health care for nursing home residents: a literature review. Med Care Res Rev. 2010;67:627–56.
Li Y, Cai X, Cram P. Are patients with serious mental illness more likely to be admitted to nursing homes with more deficiencies in care? Med Care. 2011;49(4):397–405.
Fleishman M. The problem: how many patients live in residential care facilities? Psychiatr Serv. 2004;55(6):620–2.
Ireys H, Achman L, Takyi A. State regulation of residential facilities for adults with mental illness. DHHS Pub. No. (SMA) 06–4166. Rockville: Center for Mental Health Services, Substance Abuse and Mental Health Services Administration; 2006.
National Survey of Residential Care Facilities (NSRCF) (2010) Data dictionary. resident public-use file (Revised 2/2/12). www.cdc.gov/nchs/nsrcf/nsrcf_questionnaires.htm. Accessed February 2012.
Baillargeon J, Hoge SK, Penn JV. Addressing the challenge of community reentry among released inmates with serious mental illness. Am J Community Psychol. 2010;46:361–75.
Brink J. Epidemiology of mental illness in a correctional system. Curr Opin Psychiatr. 2005;18:536–41.
Torrey EF, Kennard AD, Eslinger D, Lamb R, Pavle J. More mentally ill persons are in jails and prisons than hospitals: a survey of the states. Treatment Advocacy Center and National Sheriffs’ Association. 2010;May:1–18.
James DJ, Glaze LE. Mental health problems of prison and jail inmates. Bureau of Justice Statistics Special Report (Publication No. NCJ 213600). Washington: U.S. Department of Justice; 2006.
Morrissey JP, Cuddeback GS, Cuellar AE, Steadman HJ. The role of Medicaid enrollment and outpatient service use in jail recidivism among persons with severe mental illness. Psychiatr Serv. 2007;58:794–801.
West HC, Sabol WJ. Prisoners in 2007. Bureau of Justice Statistics Bulletin (Publication No. NCJ 224280). Washington: U.S. Department of Justice; 2008.
National Commission on Correctional Health Care. The health status of soon-to-be-released inmates: a report to congress. Chicago: National Commission on Correctional Health Care; 2002.
Hornung CA, Anno BJ, Greifinger RB, Gadre S. The health status of soon-to-be-released inmates: a report to congress, vol. 2. Chicago: National Commission on Correctional Health Care; 2002. p. 1–11.
Beck AJ. State and federal prisoners returning to the community: findings from the Bureau of Justice Statistics. Paper presented at the First Reentry Courts Initiative Cluster Meeting, Washington, DC; April, 2000. bjs.ojp.usdoj.gov/content/pub/pdf/sfprc.pdf. Accessed February 2012.
Prins SJ, Draper L. Improving outcomes for people with mental illnesses under community corrections supervision: a guide to research-informed policy and practice. New York: Council of State Governments Justice Center; 2009.
Prins SJ. Does transinstitutionalization explain the overrepresentation of people with serious mental illnesses in the criminal justice system? Community Ment Health J. 2011;47:716–22.
Goldman HH, Morrissey JP. The alchemy of mental health policy: homelessness and the fourth cycle of reform. Am J Public Health. 1985;75:727–31.
The 2011 Point-in-Time Estimates of Homelessness.
National Law Center on Homelessness and Poverty. Homelessness in the United States and the Human Right to Housing; 2004.
Drake RE, Osher FC, Wallach MA. Homelessness and dual diagnosis. Am Psychol. 1991;46(11):1149–58.
Folsom DP, Hawthorne W, Lindamer L, et al. Prevalence and risk factors for homelessness and utilization of mental health services among 10,340 patients with serious mental illness in a large public mental health system. Am J Psychiatry. 2005;162:370–6.
US Department of Housing and Urban Development, Office of Community Planning and Development. The third annual homeless assessment report to congress. Washington: US Department of Housing and Urban Development, Office of Community Planning and Development; 2008.
U.S. Department of Housing and Urban Development. The 2008 annual homeless assessment report to Congress. Washington, DC: U.S. Department of Housing and Urban Development. Retrieved from http://www.helpingthepoor.org/homeless-help/homeless-statistics-now-quarterly-by-hud-2008-homelessness-report;2009.
Belcher JR. On becoming homeless: a study of chronically mentally ill persons. J Community Psychol. 1989;17:173–85.
Pasic J, Russo J, Roy-Byrne P. High utilizers of psychiatric emergency services. Psychiatr Serv. 2005;56(6):678–84.
Irmiter C, McCarthy JF, Barry KL, Soliman S, Blow FC. Reinstitutionalization following psychiatric discharge among VA patients with serious mental illness: a national longitudinal study. Psychiatr Q. 2007;78:279–86.
Fisher W, Geller J, Pandiani J. The changing role of the state psychiatric hospital. Heal Aff. 2009;28(3):676–84.
State Forensic Mental Health Services: 2004, State Profile Highlights, Alexandria, Va., National Association of State Mental Health Program Directors Research Institute, 2005.
Schmelling S. The person and prison, mental illness discussion highlights needs for change. NIH record 59(15), July 2007. Available at nihrecord.od.nih.gov/newsletters/2007/07272007.
Lutterman T. Trends in SMHA mental health services. Presented at the National Grantee Conference on the Mental Health Block Grant and Data, Leading Change in Mental Health Systems, Washington DC, May 20–22;2008.
Lamb HR, Weinberger LE. Meeting the needs of those persons with serious mental illness who are most likely to become criminalized. J Am Acad Psychiatr Law. 2011;39:549–54.
Torrey EF, Entsminger K, Geller J, Stanley J, Jaffe DJ. The shortage of public hospital beds for mentally ill persons: a report of the Treatment Advocacy Center. Arlington: Treatment Advocacy Center; 2008.
Geller J, et al. The rights of state hospital patients: from state hospitals to their alternatives. Admin Pol Ment Health. 1998;25(4):387–401.
•• Glied S, Frank R. Better but not best: recent trends in the well-being of the mentally ill. Heal Aff. 2009;28(3):637–47. This recent article provides important analyses that demonstrate disparities in well-being and mental health care access between those with less severe mental health conditions and those with mental health impairments.
• Novella E. Mental health care in the aftermath of deinstitutionalization: a retrospective and prospective view. Ment Health Care Anal. 2010;18:222–38. This review provides a comprehensive overview of significant changes in the mental health field since deinstitutionalization.
Frank R, Goldman H, McGuire T. Trends in mental health cost growth: an expanded role for management? Heal Aff. 2009;28(3):649–59.
Frank R, Glied S. Changes in mental health financing since 1971: implications for policymakers and patients. Heal Aff. 2006;25(3):601–13.
Druss B. The changing face of U.S. mental health care. Am J Psychiatry. 2010;167(12):1419–21.
Hogan M. Transforming mental health care: realities, priorities, and prospects. Psychiatr Clin N Am. 2008;31(1):1–9.
Sederer L. Mental health policy and services 5 years after the President’s Commission Report: an interview with Michael F. Hogan. Psychiatr Serv. 2008;59(11):1242–4.
Verdier J, Barrett A. How Medicaid agencies administer mental health services: results from a 50-state survey. Psychiatr Serv. 2008;59(10):1203–6.
Engelhardt H. Long-term care: the family, post-modernity and conflicting moral life-worlds. J Med Philos. 2007;32:519–32.
Salinsky E, Loftis C. Shrinking inpatient psychiatric capacity: cause for celebration or concern? National Health Policy Form, Issue Brief No. 823;2007.
• Aschbrenner K, Grabowski D, Cai S, Bartels S, Mor V. Nursing home admissions and long-stay conversions among persons with and without serious mental illness. J Aging Soc Pol. 2011;23:286–304. The authors highlight deficiencies in care provided in nursing homes for people with SMI.
Bartels S, Moak G, Dums A. Models of mental health services in nursing homes: a review of the literature. Psychiatr Serv. 2002;53(11):1390–6.
Shea D, Russo P, Smyer M. Use of mental health services by persons with a mental illness in nursing facilities: initial impacts of OBRA 87. J Aging Health. 2000;12(4):560–78.
• Danziger S, Frank R, Meara E. Mental illness, work, and income support programs. Am J Psychiatry. 2009;166(4):398–404. This article provides up-to-date information on the use of income support programs for people with SMI.
•• Mojtabai R. National trends in mental health disability, 1997–2009. Am J Public Health. 2011;101(11):2156–63. In this review of mental health disability trends, the author uses recent data to highlight the need for improved access to mental health care services for those impaired by mental illness.
Pleis J, Lucas J, Ward B. Summary health statistics for US adults: National Health Interview Survey, 2008. Vital Health Stat. 2009;10(242):1–157.
Leff J, Warner R. Social inclusion of people with mental illness. Cambridge: Cambridge University Press; 2006.
Wu EQ, Birnbaum HG, Shi L, et al. The economic burden of schizophrenia in the United States in 2002. J Clin Psychiatr. 2005;66:1122–9.
Drake RE, Bond GR. The future of supported employment for people with severe mental illness. Psychiatr Rehabil J. 2008;31:367–76.
Bond G. Supported employment: evidence for evidence-based practice. Psychiatr Rehabil J. 2004;27:345–59.
Newman S, Goldman H. Housing policy for persons with severe mental illness. Pol Stud J. 2009;37(2):299–324.
Braconi F. 2001. Comments to the millennial housing commission. Govinfo.library.unt.edu/mhc/hearings/testimony/chpc.doc. January 19, 2012.
Parks, Svendsen, Singer, & Foti, 2006.
Dickerson F, Brown C, Daumit G, Lijuan F, Goldberg R, Wohlheiter K, Dixon L. Health status of individuals with serious mental illness. Schizophr Bull. 2006;32(3):584–9.
Lester H, Tritter J, Sorohan H. Providing primary care for people with serious mental illness: a focus group study. Br Med J. 2005;330:1122–8.
Dalmau A, Bergman B, Brismar B. Somatic morbidity in schizophrenia—a case control study. Publ Health. 1997;111:393–7.
Brunero S, Lamont S. Health behaviour beliefs and physical health risk factors for cardiovascular disease in an outpatient sample of consumers with a severe mental illness: a cross-sectional survey. Int J Nurs. 2010;47:753–60.
Deakin B, Ferrier N, Holt R, et al. The physical health challenges in patients with severe mental illness: cardiovascular and metabolic risks. J Psychopharmacol. 2010;24 suppl 1:1–8.
Brown V. Untreated physical health problems among women diagnosed with serious mental illness. JAMWA. 1998;53(4):159–60.
Dickerson F, Goldberg R, Brown C, et al. Diabetes knowledge among persons with serious mental illness and type 2 diabetes. Psychosomatics. 2005;46(418–424):418.
Desai M, Rosenheck R, Druss B, Perlin J. Mental disorders and quality of diabetes care in the veterans health administration. Am J Psychiatry. 2002;159:1584–90.
Dickerson F, Brown C, Goldberg R, Kreyenbuhl J, Wohlheiter K, Dixon L. Quality of life in individuals with serious mental illness and type 2 diabetes. Psychosomatics. 2008;49:109–14.
Bazelon Center for Mental Health Law. Get it together. How to integrate physical and mental health care for people with serious mental disorders. Washington, DC;2004.
Cuddeback GS, Scheyett A, Pettus-Davis C, Morrissey JP. General medical problems of incarcerated persons with severe and persistent mental illness: a population-based study. Psychiatr Serv. 2010;61(1):45–9.
Wolff N, Draine J. Dynamics of social capital of prisoners and community reentry: ties that bind? J Correct Healthc. 2004;17(4):457–90.
Frank R, McGuire TG. Mental health treatment and criminal justice outcomes (NBER Working Paper 15858). Cambridge: National Bureau of Economic Research; 2010.
Lurigio AJ. Examining prevailing beliefs about people with serious mental illness in the criminal justice system. Fed Probat. 2011;75(1):11–8.
Petersilia J. When prisoners come home: parole and prisoner reentry. Oxford: Oxford University Press; 2003.
Travis J. Invisible punishment: an instrument of social exclusion. In: Mauer M, Chesney-Lind M, editors. Invisible punishment: the collateral consequences of mass imprisonment. New York: The New; 2002. p. 15–36.
Uggen C, Manza J, Behrens A. ‘Less than the average citizen’: stigma, role transition and the civic reintegration of convicted felons. In: Maruna S, Immarigeon R, editors. After crime and punishment: pathways to offender reintegration (261293). Portland: Willan Publishing; 2004.
Kurzban S, Davis L, Brekke J. Vocational, social, and cognitive rehabilitation for individuals diagnosed with schizophrenia: a review of recent research and trends. Curr Psychiatr Rep. 2010;12(4):345.
Yanos P, Moos R. Determinants of functioning and wellbeing among individuals with schizophrenia: an integrated model. Clin Psychol Rev. 2007;27:58–77.
• Smith T, Sederer L. A new kind of homelessness for individuals with serious mental illness? the need for a “mental health home”. Psychiatr Serv. 2009;60(4):528–33. This article describes an important model to address fragmentation in the current mental health care system: the “mental health home” concept.
Disclosure
No potential conflicts of interest relevant to this article were reported.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Davis, L., Fulginiti, A., Kriegel, L. et al. Deinstitutionalization? Where Have All the People Gone?. Curr Psychiatry Rep 14, 259–269 (2012). https://doi.org/10.1007/s11920-012-0271-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11920-012-0271-1