
Abstract
Purpose of Review
Pediatric low-grade gliomas (pLGGs) often result in significant long-term morbidities despite high overall survival rates. This review aims to consolidate the current understanding of pLGG biology and molecular features and provide an overview of current and emerging treatment strategies.
Recent Findings
Surgical resection remains a primary treatment modality, supplemented by chemotherapy and radiotherapy in specific cases. However, recent advances have elucidated the molecular underpinnings of pLGGs, revealing key genetic abnormalities such as BRAF fusions and mutations and the involvement of the RAS/MAPK and mTOR pathways. Novel targeted therapies, including MEK, BRAF and pan-RAF inhibitors, have shown promise in clinical trials, demonstrating significant efficacy and manageable toxicity.
Summary
Understanding of pLGGs has significantly improved, leading to more personalized treatment approaches. Targeted therapies have emerged as effective alternatives, potentially reducing long-term toxicities. Future research should focus on optimizing therapy sequences, understanding long-term impacts, and ensuring global accessibility to advanced treatments.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Pediatric low-grade gliomas (pLGGs) represent the most prevalent primary brain tumor in children, constituting approximately 25–30% of all brain and spinal cord tumors [1].These tumors are highly heterogeneous and classified by the World Health Organization (WHO) histopathological system as grade 1 or 2 tumors of the central nervous system, boasting a 10-year overall survival (OS) of 90–95% [2]. While most cases emerge sporadically from various brain regions, including the cerebellum, cerebral cortex, brainstem, spinal cord, hypothalamus, optic chiasm, or optic nerves, around 20% of cases occur in patients with the genetic predisposition syndrome neurofibromatosis type 1 (NF1), often manifesting as optic pathway tumors [3]. Despite their benign, slow-growing nature and excellent OS, pLGGs entail significant long-term morbidity, stemming from both the tumor itself and treatment-related effects. These morbidities encompass neurosensory, motor, and visual deficits, as well as cognitive and endocrine complications. Often following a protracted disease course with multiple recurrences, patients may undergo several lines of treatment over many years, resulting in cumulative treatment burden. This presents management challenges, necessitating a delicate balance between disease control, treatment toxicity, and preservation of neurodevelopmental, visual, and endocrine function. Consequently, the focus of future therapies is shifting towards enhancing the quality of survival and mitigating long-term treatment sequelae.
Recent years have witnessed remarkable progress in unraveling the molecular biology of pLGGs, offering promising prospects for novel targeted therapeutic approaches. However, it remains uncertain whether conventional management strategies can be supplanted by less toxic therapies or if new agents will prove efficacious following treatment failure. This review aims to encapsulate our current comprehension of the biology and molecular classification of pLGGs, delineate their clinical implications, and furnish an overview of contemporary management strategies, emerging agents, and ongoing trials in pediatric and adolescent pLGG patients.
Histopathology and Molecular Classification:
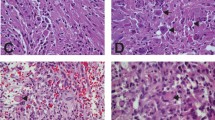
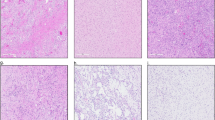
pLGGs typically exhibit glial or mixed glial-neuronal morphology and are predominantly categorized as WHO grade 1 or 2 tumors, historically including entities such as pilocytic astrocytoma, pilomyxoid astrocytoma, subependymal giant cell astrocytoma, pleomorphic xanthoastrocytoma, and various mixed low-grade glial-neuronal tumors. However, the classification based solely on histopathology fails to capture the molecular heterogeneity of pLGGs. Collaborative studies worldwide have elucidated genomic alterations in gliomas across ages, grades, and histologies [4,5,6]. The 2021 WHO Classification of Tumors of the Central Nervous System (CNS5) integrates molecular and histological diagnoses, unveiling new tumor types and subtypes in pediatric patients and underscoring the distinction between pediatric-type and adult-type diffuse gliomas due to their disparate molecular and clinical profiles[7]. The majority of pLGGs harbor genetic abnormalities linked to aberrant intracellular signalling via the RAS/mitogen-activated protein kinase (RAS/MAPK) pathway, including the KIAA1549::BRAF fusion, the BRAF V600E mutation, neurofibromin 1 mutations, and less common alterations in fibroblast growth factor receptor 1 (FGFR1), FGFR2, NTRK, MYB, or MYBL1 genes[4, 8]. In contrast to adult gliomas, pediatric-type diffuse gliomas usually lack IDH1/2 mutations and 1p/19q co-deletion but frequently exhibit alterations in BRAF, FGFR1, MYB, or MYBL1 genes[2]. These distinct molecular profiles inform pLGG treatment planning, with clinical trials stratifying patients based on "targetable" BRAF mutations and fusions.
Treatment Strategies
Surgical Treatment
Surgical resection remains the cornerstone of PLGG management. The primary goal of surgery is to achieve maximal safe resection of the tumor. However, the definition of "maximal safe resection" varies depending on factors such as tumor location and the risk of neurological injury[9]. For patients who underwent a gross total resection (GTR), 10-year PFS exceeds 85%, whereas it is less than 50% for patients with remaining tumor. Complete surgical resection, particularly for hemispheric or cerebellar lesions [10, 11]. In selected cases, minimally invasive surgical techniques such as endoscopic or laser interstitial thermal therapy (LITT) may be utilized for tumor resection, particularly for small, deep-seated lesions or tumors in eloquent areas where traditional open surgery carries higher risks[12]. Partial resections for mechanical decompression or biopsy are usually performed when lesions are closer to vital structures that preclude total resection (e.g., optic pathway, hypothalamus, and pituitary). As targeted therapies are increasingly available, tissue sampling has become recommended for patients except for children with NF1 and an optic pathway tumors. Understanding a patient's tumor biology helps identify new targeted therapies that defer or avoid the toxicity associated with chemotherapy and radiation.
Radiation Therapy
Radiation therapy, once a standard treatment, is now reserved for only specific cases due to long-term complications, including increased risk of second malignancies, strokes and cognitive deficits [13]. Its use is limited to patients where complete surgical resection is not feasible, and there is no response to other treatment options. Advancements in radiation planning, such as proton radiotherapy, aim to maintain tumor control while reducing toxicity [14]. Merchant et al. (2022) reviewed the use of proton beam therapy (PBT) in children with PLGGs. Proton beam therapy was associated with a 75% disease control rate at 2 years and significantly fewer neurocognitive side effects compared to conventional radiotherapy.
Chemotherapy
Chemotherapy plays a pivotal role in the treatment of patients, especially with unresectable tumous, patients with NF1 and patients with metastatic disease [8]. Overall response rates of up to 50–60% and 5-year PFS 39–53% have been reported with chemotherapy regimens in most series [13]. Vincristine and carboplatin combinations or monotherapy with vinblastine remain the most common chemotherapy regimens for pLGG treatment at many centers worldwide.
Gnekow et al. evaluated the efficacy of the SIOP-LGG 2004 protocol, which uses vincristine and monthly carboplatin, in treating children with PLGGs. The 5-year PFS was 46% and and OS was 89% [14]. Toxicity was manageable, with most side effects being hematological. Bouffet et al. assessed the use of vinblastine as a single-agent therapy for children with recurrent or refractory PLGGs. The results indicated that vinblastine is an effective and well-tolerated treatment option. Five-year overall survival was 93.2% ± 3.8%, and 5-year progression-free survival was 42.3% ± 7.2%. Toxicity was manageable and mostly hematological [15]. Other regimens used more infrequently include single-agent carboplatin, TPCV combination (thioguanine, procarbazine, CCNU and vincristine), the cisplatin and etoposide regimen or single-agent vinorelbine. Outcomes vary, with some patients experiencing favorable responses, particularly NF1 patients, while others – in particular children < 1 year old, those with diencepha-ic syndrome and/or disseminated disease – face continued disease progression despite therapy. The overall response rates reported between 35 to 86%, and 5-year PFS between 37 to 52% with these treatment protocols[16,17,18,19].
Up to 60% of pLGG cases progress after conventional chemotherapy, necessitating novel therapeutic approaches. Targeted therapies focusing on common genetic aberrations in the RAS/MAPK pathway have emerged as promising options, aiming to disrupt tumor growth [4].
Molecular Characterization and Targeted Therapies
The identification of alterations of genes in RAS/MAPK and mTOR signalling pathways has been a significant advancement in the understanding of PLGGs. The targetable points on these pathways are shown in Fig. 1. Current targeted therapies for pLGG involve MEK inhibitors, BRAF inhibitors, pan-RAF inhibitors, and mTOR inhibitors. Active clinical trials are summarized in Table 1 and Table 2.

RAS/MAPK Pathway-mTOR Pathway, targetable points
MEK Inhibitors
MEK inhibitors target the downstream effectors of the MAPK pathway and have shown promise in treating PLGGs, particularly those with BRAF fusions. Fangusaro et al. investigated the use of selumetinib in children with recurrent or refractory PLGGs. The results demonstrated durable responses and manageable toxicity profiles, suggesting that selumetinib could be an effective treatment for this patient population. The study reported a two-year PFS of 78 ± 8.5%, and the most common toxicities were grade1/2 CPK elevation, anemia, diarrhea, headache, nausea/emesis, fatigue, AST and ALT increase, hypoalbuminemia, and rash [20]. The preliminary results of an ongoing multicenter phase II trial of trametinib in patients with progressive/refractory pLGG showed a PFS at 12 months of 79.9% [21]. Significant clinical benefits were observed, including tumor shrinkage and disease stabilization. The treatment was well-tolerated, with manageable side effects. Other MEK inhibitors like cobimetinib, and binimetinib are also under investigation, showing potential in refractory/recurrent pLGG [5, 6]. A recent study aimed to evaluate the efficacy of MEK162 (binimetinib) in children with progressive or recurrent low-grade glioma and to validate its target. It was a multi-institutional phase II study. Among 38 evaluable patients, the overall response rate was 34% (13/38), with 3 complete responses and 10 partial responses. Stable disease was noted in 18 patients (47%), and 7 patients (18%) had progressive disease. The 2-year progression-free survival was 47.5% (95% CI 30.6–62.4). The study validated the target of MEK162 in low-grade glioma, demonstrating that higher levels of phosphorylated ERK correlated with response to therapy. The study concluded that MEK162 showed promising efficacy in children with progressive or recurrent low-grade glioma, with manageable toxicity [22].
BRAF Inhibitors
Recent studies have demonstrated the efficacy of BRAF inhibitors, such as vemurafenib and dabrafenib, in treating BRAF-mutant PLGGs. Vemurafenib has shown to have promising anti-tumor activity in recurrent BRAF V600E-positive brain tumors with manageable toxicity in a phase 1 study[23]. A phase 2 study is ongoing (NCT01748149). Hargrave et al., in a phase I/II trial, assessed the safety and efficacy of vemurafenib in pediatric patients with BRAF V600E-mutant recurrent or refractory PLGGs. The trial showed a 56% overall response rate, with 22% achieving complete response and 34% partial response, along with acceptable safety and tolerability. The study demonstrated favorable response rates and manageable toxicity, supporting the use of vemurafenib in this patient population [24]. Bouffet et al.aimed to evaluate the efficacy of dabrafenib plus trametinib in pediatric patients with glioma harboring BRAF V600 mutations. The combination of dabrafenib plus trametinib was compared to standard chemotherapy with vincristine and carboplatin in treatment naïve patients with low grade glioma associated with a BRAF V600 mutation, This trial showed a significant benefit favoring targeted treatment with a one year progression free survival rate of 67% versus 26% for the chemotherapy arm. The overall response rate (ORR, CR + PR) was 47%, verus 11% in the chemotherapy arm%. The overall clinical benefit rate (CR + PR + SD) was 86%, indicating a strong response to the treatment in the study population [25].
Pan-RAF inhibitors
Tovorafenib (DAY101) is a new targeted therapy being investigated for its efficacy in treating PLGGs with BRAF alterations. It is an oral pan-RAF brain penetrant inhibitor that has shown promise in clinical trials. The drug is administered orally, once a week, and there is a sprinkle formulation for young children.
PNOC014 study aimed to evaluate the safety, tolerability, and preliminary efficacy of tovorafenib in children LGGs and other tumors activated by the RAS/RAF/MEK/ERK pathway. The study found tovorafenib to be well-tolerated with manageable side effects. Preliminary efficacy data showed promising responses in children with LGGs and other pathway-activated tumors. The overall response rate (ORR) was approximately 42%, indicating a significant proportion of patients experienced tumor shrinkage or stabilization [26]. The FIREFLY-1 trial aimed to assess the efficacy and safety of tovorafenib in children with relapsed or refractory pediatric low-grade glioma (pLGG). Tovorafenib demonstrated significant clinical activity in treating relapsed/refractory pLGG. The study reported a high overall response rate (ORR, including CR + PR + MR) of approximately 64%, with many patients showing substantial tumor reduction. Durable disease control was observed, with many responses lasting over 12 months. The trial outcomes were considered highly significant, leading to increased interest in tovorafenib for pLGG treatment and FDA approval on April 23, 2024 for patients 6 months of age and older with relapsed or refractory pediatric low-grade glioma (LGG) harboring a BRAF fusion or rearrangement, or BRAF V600 mutation. [27]. The The LOGGIC/FIREFLY-2 trial aims to compare the efficacy and safety of tovorafenib versus standard chemotherapy in pediatric patients with newly diagnosed low-grade glioma (LGG) harboring an activating RAF alteration. The study is designed to determine if tovorafenib could provide superior outcomes compared to traditional chemotherapy. Tovorafenib may represent a more effective and better-tolerated treatment option for this group of patients, highlighting its potential as a promising therapeutic agent for pLGGs [28].
mTOR Pathway Inhibitors
The mTOR pathway is another critical signaling pathway implicated in the pathogenesis of PLGGs. Inhibitors targeting this pathway, such as everolimus, have been explored as potential therapies. Ullrich et al., aimed to assess the efficacy of continuous daily oral everolimus in treating recurrent, radiographic-progressive NF1-associated pediatric low-grade glioma. The study found that everolimus was well-tolerated, with manageable toxicities. However, the overall response rate was low, with only 2 out of 35 patients (5.7%) achieving an objective response. Median PFS was 11.3 months. Everolimus showed limited efficacy in this patient population, with a low response rate [29].
Wright et al., investigated the efficacy of continuous oral daily everolimus in treating recurrent, radiographically progressive pediatric low-grade glioma. Everolimus was well-tolerated, with manageable toxicities. However, the overall response rate was also low, with only 2 out of 27 patients (7.4%) achieving a partial response. The median PFS was 10.5 months. Everolimus showed limited efficacy in this patient population, with a low response rate [30].
Haas-Kogan et al., evaluated the efficacy of everolimus in children with recurrent or progressive low-grade glioma. Everolimus demonstrated limited efficacy, with only 2 out of 45 patients (4.4%) achieving a partial response. The disease control rate at 6 months was 31.1%. The median PFS was 6.1 months. Everolimus showed modest activity in this patient population, with a low response rate and short PFS [31].
Overall, these studies suggest that everolimus has limited efficacy in treating pLGGs, with low response rates and modest progression-free survival benefits. Clinical trials are ongoing studying the combination of MEK and mTOR inhibitors for recurrent pLGG (NCT04485559/PNOC021).
Controversial Discoveries and Hypotheses
Despite significant progress, several controversies and unresolved questions remain. One area of debate is the optimal sequencing and combination of therapies, particularly in the context of targeted treatments. The optimal duration of treatment remains to be defined, as rebound and early progression have been described, particularly after discontinuation for BRAF inhibitor [32]. Additionally, the long-term impact of these novel therapies on the developing brain is not fully understood.
Controversial Hypothesis:
Ongoing Debate: There is ongoing debate regarding the potential long-term neurocognitive effects of targeted therapies and immunotherapies in pediatric patients. While these treatments offer significant benefits in terms of tumor control, their impact on brain development and function requires further investigation.
Personal Observations and Future Directions
From our observations and review of the recent literature, it is evident that the treatment landscape for PLGGs is rapidly evolving. The integration of molecular diagnostics has revolutionized the approach to therapy, enabling more personalized and targeted treatment strategies. However, the translation of these advancements into routine clinical practice remains a challenge, particularly in resource-limited settings.
Future Research Focuses:
Long-term Outcomes: Investigating the long-term neurocognitive and psychosocial outcomes of children treated with targeted therapies.
Combination Therapies: Exploring the optimal sequencing, duration and combination of targeted therapies and conventional treatments.
Biomarker Development: Identifying biomarkers that can predict response to therapy and guide treatment decisions.
Global Access: Ensuring that advancements in PLGG treatment are accessible to children worldwide, regardless of geographic or socioeconomic barriers.
Conclusion
Significant strides have been made in the treatment of pediatric low-grade gliomas over the past few years. Advances in molecular characterization, targeted therapies, and surgical techniques have improved the management and outcomes of these tumors. However, ongoing research and collaboration are essential to address the remaining challenges and controversies in the field. By continuing to build on these advancements, we aim to achieve even better outcomes for children with PLGGs.
By focusing on these advancements, we can continue to improve the outcomes and quality of life for children with PLGGs and ensure that they receive the most effective and least harmful treatments available.
Data Availability
No datasets were generated or analysed during the current study.
References
Ostrom QT, Cioffi G, Gittleman H, Patil N, Waite K, Kruchko C, Barnholtz-Sloan JS. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2012–2016. Neuro Oncol. 2019;21(Suppl 5):v1–100. https://doi.org/10.1093/neuonc/noz150.
Louis DN, Perry A, Wesseling P, Brat DJ, Cree IA, Figarella-Branger D, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary. Neuro Oncol. 2021;23(8):1231–51. https://doi.org/10.1093/neuonc/noab106.
de Blank P, Bandopadhayay P, Haas-Kogan D, Fouladi M, Fangusaro J. Management of pediatric low-grade glioma. Curr Opin Pediatr. 2019;31(1):21–7. https://doi.org/10.1097/MOP.0000000000000717.
Ryall S, Tabori U, Hawkins C. Pediatric low-grade glioma in the era of molecular diagnostics. Acta Neuropathol Commun. 2020;8(1):30. https://doi.org/10.1186/s40478-020-00902-z.
Weller M, Wen PY, Chang SM, Dirven L, Lim M, Monje M, Reifenberger G. Glioma Nat Rev Dis Primers. 2024;10(1):33. https://doi.org/10.1038/s41572-024-00516-y.
Rousseau J, Bennett J, Lim-Fat MJ. Brain Tumors in Adolescents and Young Adults: A Review. Semin Neurol. 2023;43(6):909–28. https://doi.org/10.1055/s-0043-1776775.
Bale TA, Rosenblum MK. The 2021 WHO Classification of Tumors of the Central Nervous System: An update on pediatric low-grade gliomas and glioneuronal tumors. Brain Pathol. 2022;32(4): e13060. https://doi.org/10.1111/bpa.13060.
Haizel-Cobbina J, Thakkar R, Richard K, Du L, Levine A, Bennett J, et al. Clinical and molecular features of disseminated pediatric low-grade glioma and glioneuronal tumors: a systematic review and survival analysis. Neurooncol Adv. 2022;4(1):vdac122. https://doi.org/10.1093/noajnl/vdac122.
Samples DC, Mulcahy Levy JM, Hankinson TC. Neurosurgery for Optic Pathway Glioma: Optimizing Multidisciplinary Management. Front Surg. 2022;9:884250. https://doi.org/10.3389/fsurg.2022.884250.
Wisoff JH, Sanford RA, Heier LA, Sposto R, Burger PC, Yates AJ, et al. Primary neurosurgery for pediatric low-grade gliomas: a prospective multi-institutional study from the Children's Oncology Group. Neurosurgery. 2011;68(6):1548–54; discussion 54–5. https://doi.org/10.1227/NEU.0b013e318214a66e
Manoharan N, Liu KX, Mueller S, Haas-Kogan DA, Bandopadhayay P. Pediatric low-grade glioma: Targeted therapeutics and clinical trials in the molecular era. Neoplasia. 2023;36:100857. https://doi.org/10.1016/j.neo.2022.100857.
Strauss I, Gabay S, Roth J. Laser interstitial thermal therapy (LITT) for pediatric low-grade glioma-case presentations and lessons learned. Childs Nerv Syst. 2024https://doi.org/10.1007/s00381-024-06419-3
Lassaletta A, Zapotocky M, Bouffet E. Chemotherapy in pediatric low-grade gliomas (PLGG). Childs Nerv Syst. 2024https://doi.org/10.1007/s00381-024-06458-w
Gnekow AK, Walker DA, Kandels D, Picton S, Giorgio P, Grill J, et al. A European randomised controlled trial of the addition of etoposide to standard vincristine and carboplatin induction as part of an 18-month treatment programme for childhood (</=16 years) low grade glioma - A final report. Eur J Cancer. 2017;81:206–25. https://doi.org/10.1016/j.ejca.2017.04.019.
Bouffet E, Jakacki R, Goldman S, Hargrave D, Hawkins C, Shroff M, et al. Phase II study of weekly vinblastine in recurrent or refractory pediatric low-grade glioma. J Clin Oncol. 2012;30(12):1358–63. https://doi.org/10.1200/JCO.2011.34.5843.
Ater JL, Zhou T, Holmes E, Mazewski CM, Booth TN, Freyer DR, et al. Randomized study of two chemotherapy regimens for treatment of low-grade glioma in young children: a report from the Children’s Oncology Group. J Clin Oncol. 2012;30(21):2641–7. https://doi.org/10.1200/JCO.2011.36.6054.
Cappellano AM, Petrilli AS, da Silva NS, Silva FA, Paiva PM, Cavalheiro S, Bouffet E. Single agent vinorelbine in pediatric patients with progressive optic pathway glioma. J Neurooncol. 2015;121(2):405–12. https://doi.org/10.1007/s11060-014-1652-6.
Massimino M, Spreafico F, Cefalo G, Riccardi R, Tesoro-Tess JD, Gandola L, et al. High response rate to cisplatin/etoposide regimen in childhood low-grade glioma. J Clin Oncol. 2002;20(20):4209–16. https://doi.org/10.1200/JCO.2002.08.087.
Dodgshun AJ, SantaCruz N, Hwang J, Ramkissoon SH, Malkin H, Bergthold G, et al. Disseminated glioneuronal tumors occurring in childhood: treatment outcomes and BRAF alterations including V600E mutation. J Neurooncol. 2016;128(2):293–302. https://doi.org/10.1007/s11060-016-2109-x.
Fangusaro J, Onar-Thomas A, Poussaint TY, Wu S, Ligon AH, Lindeman N, et al. A phase II trial of selumetinib in children with recurrent optic pathway and hypothalamic low-grade glioma without NF1: a Pediatric Brain Tumor Consortium study. Neuro Oncol. 2021;23(10):1777–88. https://doi.org/10.1093/neuonc/noab047.
Perreault S, Larouche V, Tabori U, Hawkins C, Lippé S, Ellezam B, et al. SYST-04. TRAM-01: a phase 2 study of trametinib for patients with pediatric glioma with activation of the mapk/erk pathway. Neuro-Oncology Advances. 2021;3(Supplement_4):9. https://doi.org/10.1093/noajnl/vdab112.032
Robison N, Pauly J, Malvar J, Gardner S, Allen J, Margol A, et al. LTBK-04. Late breaking abstract: MEK162 (binimetinib) in children with progressive or recurrent low-grade glioma: a multi-institutional phase II and target validation study. Neuro-Oncology. 2022;24(Supplement_1):i191-i2. https://doi.org/10.1093/neuonc/noac079.716
Nicolaides T, Nazemi KJ, Crawford J, Kilburn L, Minturn J, Gajjar A, et al. Phase I study of vemurafenib in children with recurrent or progressive BRAF(V600E) mutant brain tumors: pacific pediatric neuro-oncology consortium study (PNOC-002). Oncotarget. 2020;11(21):1942–52. https://doi.org/10.18632/oncotarget.27600.
Hargrave DR, Bouffet E, Tabori U, Broniscer A, Cohen KJ, Hansford JR, et al. Efficacy and Safety of Dabrafenib in Pediatric Patients with BRAF V600 Mutation-Positive Relapsed or Refractory Low-Grade Glioma: Results from a Phase I/IIa Study. Clin Cancer Res. 2019;25(24):7303–11. https://doi.org/10.1158/1078-0432.CCR-19-2177.
Bouffet E, Hansford JR, Garre ML, Hara J, Plant-Fox A, Aerts I, et al. Dabrafenib plus Trametinib in Pediatric Glioma with BRAF V600 Mutations. N Engl J Med. 2023;389(12):1108–20. https://doi.org/10.1056/NEJMoa2303815.
Wright K, Kline C, Abdelbaki M, Ebb D, Sayour E, Elster J, et al. CTNI-53. PNOC014: phase ib study results of day101(TOVORAFENIB) for children with low-grade gliomas (LGGS) and other RAS/RAF/MEK/ERK pathway-activated Tumors. Neuro-Oncol. 2022;24(Supplement_7):vii84-vii. https://doi.org/10.1093/neuonc/noac209.318.
Kilburn LB, Khuong-Quang DA, Hansford JR, Landi D, van der Lugt J, Leary SES, et al. The type II RAF inhibitor tovorafenib in relapsed/refractory pediatric low-grade glioma: the phase 2 FIREFLY-1 trial. Nat Med. 2024;30(1):207–17. https://doi.org/10.1038/s41591-023-02668-y.
van Tilburg CM, Kilburn LB, Perreault S, Schmidt R, Azizi AA, Cruz-Martinez O, et al. LOGGIC/FIREFLY-2: a phase 3, randomized trial of tovorafenib vs. chemotherapy in pediatric and young adult patients with newly diagnosed low-grade glioma harboring an activating RAF alteration. BMC Cancer. 2024;24(1):147. https://doi.org/10.1186/s12885-024-11820-x.
Ullrich NJ, Prabhu SP, Reddy AT, Fisher MJ, Packer R, Goldman S, et al. A phase II study of continuous oral mTOR inhibitor everolimus for recurrent, radiographic-progressive neurofibromatosis type 1-associated pediatric low-grade glioma: a Neurofibromatosis Clinical Trials Consortium study. Neuro Oncol. 2020;22(10):1527–35. https://doi.org/10.1093/neuonc/noaa071.
Wright KD, Yao X, London WB, Kao PC, Gore L, Hunger S, et al. A POETIC Phase II study of continuous oral everolimus in recurrent, radiographically progressive pediatric low-grade glioma. Pediatr Blood Cancer. 2021;68(2):e28787. https://doi.org/10.1002/pbc.28787.
Haas-Kogan DA, Aboian MS, Minturn JE, Leary SES, Abdelbaki MS, Goldman S, et al. Everolimus for Children With Recurrent or Progressive Low-Grade Glioma: Results From the Phase II PNOC001 Trial. J Clin Oncol. 2024;42(4):441–51. https://doi.org/10.1200/JCO.23.01838.
Nobre L, Zapotocky M, Ramaswamy V, Ryall S, Bennett J, Alderete D, et al. Outcomes of BRAF V600E Pediatric Gliomas Treated With Targeted BRAF Inhibition. JCO Precis Oncol. 2020;4. https://doi.org/10.1200/PO.19.00298.
Author information
Authors and Affiliations
Contributions
I.Y.B. and E.B wrote the main manuscript text, prepared the figure and tables.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Yaman Bajin, I., Bouffet, E. Advances in the Treatment of Pediatric Low-Grade Gliomas. Curr Neurol Neurosci Rep (2024). https://doi.org/10.1007/s11910-024-01369-4
Accepted:
Published:
DOI: https://doi.org/10.1007/s11910-024-01369-4