
Abstract
Purpose of Review
Metabolic syndrome (MetS) is a cluster of cardiovascular disease risk factors that are related to several adverse health outcomes, including poor cognitive function. This review seeks to summarize and critically review select recent findings on the association between MetS and cognition.
Recent Findings
MetS was associated with lower domain-specific and global cognitive function in most cross-sectional studies, but findings from longitudinal studies are not consistent. The associations varied depending on age, sex, cognitive test, genetic susceptibility, and the duration of follow-up in prospective studies. MetS was associated with a higher risk of mild cognitive impairment (MCI) and progression from MCI to dementia, particularly vascular dementia. Among MetS components, high blood pressure, high waist circumference, and hyperglycemia were the strongest predictors of cognitive function.
Summary
MetS is associated with higher risk of cognitive impairment. Research is needed on how preventing or treating MetS affects cognition.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Dementia, the most extreme form of cognitive impairment, is defined as a loss of mental abilities combined with impairments in the ability to perform basic activities of daily living. It is estimated that roughly 11% of Americans aged 65 years and older have Alzheimer’s disease (AD) or a related dementia [1]. While non-modifiable risk factors, such as age and genetic susceptibility, are primary drivers of the risk of cognitive impairment and dementia [2], identifying modifiable risk factors for dementia is important because it provides an opportunity for intervention and prevention. In particular, there has been increasing interest on how the aggregation of risk factors affects the risk of cognitive impairment. The metabolic syndrome (MetS) is one of the most commonly used definitions of aggregation of risk factors.
MetS refers to a cluster of cardiometabolic conditions with shared pathophysiology that together have been shown to increase the risk of cardiovascular disease (CVD), stroke, and type 2 diabetes (T2D) [3]. MetS has been operationalized in many ways [4]. The World Health Organization (WHO) first defined MetS in 1998, with insulin resistance being at the center of the WHO definition. Without evidence of insulin resistance, a diagnosis of MetS cannot be made even with the presence of the other criteria which are: waist/hip ratio > 0.90 for men, > 0.85 for women; or BMI > 30 kg/m2 triglyceride ≥ 150 mg/dl or HDL-C: < 35 mg/dl for men, < 39 mg/dl for women, blood pressure ≥ 140/90 mmHg, microalbuminuria [4]. The most widely used definition of MetS was operationalized by the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III) and later updated by the American Heart Association (AHA) and the National Heart Lung and Blood Institute (NHLBI) in 2005 [5]. This definition combined previous concepts to provide simple criteria that can be readily measured and easily applied in both clinical and epidemiological settings [4]. In this definition, MetS requires the presence of three or more of the following conditions:
-
1.
Central or abdominal obesity measured by waist circumference (men: > 40 inches, women: > 35 inches)
-
2.
High triglycerides ≥ 150 mg per deciliter (mg/dL) or if taking a medication for high triglycerides.
-
3.
Low HDL cholesterol (men < 40 mg/dL, women < 50 mg/dL) or if taking a medication for low HDL cholesterol.
-
4.
High blood pressure ≥ 130/85 mm of mercury (mm Hg) or if taking a medication for high blood pressure.
-
5.
High fasting glucose ≥ 100 mg/dL, or if taking a medication for high blood glucose.
Epidemiology and Prevalence of MetS
Data from the National Health and Nutrition Examination Survey (NHANES) conducted between 1988 and 2012 estimated the prevalence of the MetS to be nearly 34% among US adults [6]. The prevalence of MetS is often difficult to ascertain due to the secular trends in increasing obesity and incidence of T2D and because of differences in MetS criteria and adiposity thresholds applied across various studies. The prevalence of MetS also differs by age, sex, and race. It has been reported that the prevalence of MetS is higher among older (35–64 years old) compared to younger (20–34 years old) adults and among Mexican Americans compared to non-Hispanic Whites [7]. MetS is also higher in non-Hispanic white men compared to non-Hispanic black men and in non-Hispanic black women compared to non-Hispanic white women [6]. Differences in the prevalence of MetS have also been observed by socioeconomic status and education subgroups [6].
Important Concepts of Cognitive Function
The American Psychological Association (APA) defines cognition as “all forms of knowing and awareness, such as perceiving, conceiving, remembering, reasoning, judging, imagining, and problem solving” [8]. Major cognitive processes (or domains) that are often measured by neuropsychological tests include: memory (encoding, storing, and retrieving information), learning (acquiring and integrating new information), language (understanding and expressing thoughts), visual-spatial skills (processing a visual stimulus and understanding the spatial relationship between objects), and executive function (mental processes that leads to a goal-driven action). Standardized and validated neuropsychological tests are often used to assess performance in a single cognitive domain or across multiple cognitive domains. Impairments in cognition may be present if an individual has difficulty in operating and performing in one or more cognitive domains compared to the expected performance for an individual’s age and level of education [9]. Cognitive impairment can range from mild to severe. Mild cognitive impairment (MCI) represents an intermediate phase between normal cognitive functioning and clinical dementia. The primary distinction between MCI and dementia is the loss of independence in functional abilities, such as basic activities of daily living, among individuals with dementia [10]. MCI is often subdivided into amnestic MCI (aMCI) and non-amnestic (naMCI). In aMCI, memory is impaired while in naMCI, memory is preserved and domains other than memory are impaired [10,11,12]. Both aMCI and naMCI can progress to dementia [10, 12].
Search Strategy
We used PubMed as the main database for our literature search with a focus on observational studies published in the past 5 years through March 9th, 2021. We searched both original and relevant review articles. We used the search term “metabolic syndrome” paired with; cognition, cognitive, dementia in the abstract/title of each article or as a Medical Subject Headings (MeSH) term. An article was selected if it investigates MetS as a construct and any measure of cognitive function as an outcome in Humans. Studies examining only individual components of MetS were not included. A separate search was performed for MetS and biomarkers of Alzheimer’s disease and other dementias using the search term “metabolic syndrome” paired with amyloid, tau, cerebrovascular disease and neurodegeneration. Reference lists of included studies and relevant review articles were reviewed to identify additional studies.
MetS and Cognitive Performance
A summary of select recent studies that examined the association of MetS with cognitive performance using individual neuropsychological tests or cognitive domain scores are detailed in Table 1.
Most recent cross-sectional studies reported an inverse association between the presence of MetS and lower global and domain-specific cognitive performance [13–24]. The reported association in most of the studies differed depending on the type of neuropsychological test used with some neuropsychological tests being more sensitive than others [15, 16, 18, 19]. Lower performance across multiple cognitive domains was reported among those with MetS compared with those without MetS, including memory [13, 15, 17, 20], executive function [13–15, 19, 20], attention/speed [13, 16, 18], and global cognition [13, 20].
Age and sex are other important factors to take into consideration that can influence the association between MetS and cognitive function. Studies among both middle-aged [15, 17] and older adults [16, 18, 21] reported a lower cognition among individuals who have MetS. Age, however, can be a modifier in this association. González et al. [20] reported that the association of MetS with cognition was stronger among middle-aged as compared to older adults, particularly in tests of verbal memory. The observation of weaker association between MetS and cognition in older adults was also previously described in longitudinal cohorts [25, 26]. Differences in the magnitude and strength of associations between MetS and cognition when comparing studies conducted in mid-life as compared to late-life may be due to several factors including survival bias [25], differential validity of measures of the MetS components across the lifespan, and the fact that some MetS components change with age. For example, triglyceride levels and waist circumference may be lower among older adults as a result of inadequate nutrition and sarcopenia, which has its own adverse health consequences [25, 27].
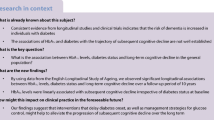
Longitudinal studies are critical to establishing temporality in the associations between MetS and cognitive function. There have been several recent reports on the longitudinal associations of MetS with cognition, but the results are inconsistent [13, 27, 28, 29•, 30•, 31]. The Women’s Health across Nation (SWAN) study reported that the presence of MetS in midlife was associated with a 24% accelerated decline in perceptual speed over 10 years [29•]. In the Singapore Longitudinal Aging Study (SLAS), there was a trend of cognitive decline in memory/learning, executive function, processing speed, attention/working memory, and global cognition related to the presence of MetS among late-middle aged adults over 4.5-year follow-up but the results did not reach statistical significance [13]. In contrast to the SWAN study, the European Male Aging Study (EMAS) reported no significant cognitive decline in those with MetS compared with those without MetS over a mean of 4.4 years [28]. EMAS, however, reported hyperglycemia, a component of the MetS, as the primary predictor of cognitive decline in tests of processing speed and visual-spatial abilities [28]. The discrepant results between these studies may be due to the characteristics of the study population or follow-up time. EMAS included a representative cohort of healthy European men, while the SWAN study included a cohort of US women traversing menopause. It is also possible that these discrepant results reflect sex differences in the association between MetS and cognitive function [32, 33], with the associations being stronger in women compared to men, as reported in some studies [34, 35].
A key large prospective study from the Framingham Offspring Study illustrates additional factors that may influence the association between MetS and cognitive function [30•]. Spanning midlife to late life, the authors reported that baseline MetS was not associated with change in cognitive function in the overall sample. However, results were different after conducting a stratified analysis by APOE-ε4 carrier status and dementia status. Specifically, baseline MetS was associated with lower cognitive function among non-demented vs. demented and APOE-ε4 non-carriers vs. APOE-ε4 carriers. Furthermore, participants with evidence of a more rapid rate of cognitive decline were more likely to have MetS compared to those who had a slower rate of cognitive decline [30•]. Finally, the study reported that both mid-life (at age 50) and late-life (at age 70) MetS were both associated with poor cognitive function; however, mid-life MetS was associated with more affected cognitive domains compared to late-life; memory, global cognition, processing speed/executive function were all affected at mid-life while memory was not affected at late-life [30•]. In addition to midlife and late life, the negative impact of MetS on cognition may extend to adolescents as well. Poor performance of reading, attention, working memory [22], executive function, and cognitive flexibility [19], were all reported in studies among adolescents. It should be noted however that there are only few studies published on Mets and cognition among adolescents and more studies are needed in order to assess these associations.
Severity of MetS, quantified as the overall number of MetS components present, was also related to lower cognition in some studies [13, 17, 21]. In some studies, the number of MetS components present appeared to be more strongly associated with lower cognitive function than the presence/absence of MetS [13]. Among the MetS components, hyperglycemia, high blood pressure, and high waist circumference were the component measures that were mostly strongly associated with cognitive performance [19, 21, 22, 28].
Fewer studies reported no association between the presence vs. absence of MetS and cognitive performance [28, 36–38]. A lack of an association in these studies could be due to common use of less sensitive global cognition screening tools, such as the Montreal Cognitive Assessment (MoCA) or the Mini Mental Status Exam (MMSE), rather than standardized and validated neuropsychological tests. These tests are more commonly used as dementia screening tools and are therefore not able to detect subtle changes in cognition that can be present before cognitive impairment is clinically present [37, 38]. Heterogenous results may also be due to the characteristics of the study population, covariates included in multivariate models, and different criteria used to define MetS.
MetS and Cognitive Impairment Syndromes (MCI, Dementia)
A summary of select recent studies that examined MetS and cognitive impairment syndromes are detailed in Table 2.
Relatively few recent studies have examined the association of MetS with MCI [39, 40•, 41, 42]. The Singapore Longitudinal Ageing Study Cohort (SLAS) reported that MetS was associated with an increased risk of incident MCI [40•]. Similar results were reported in a cross-sectional study by Wang and colleagues [39]. Similarly, fewer studies have examined the association of MetS with MCI subtypes (aMCI vs naMCI). Bae and colleagues [43] reported that MetS was associated naMCI but not with aMCI; however, the study was limited by a small aMCI sample size [43]. Some studies however reported no association between MetS and MCI. As with cognitive function as an outcome, factors such as the study population [42], study design, and definition of MetS used [41] may play a role in the differences across studies. For example, Martinez et al. reported no association between MetS and cognitive impairment among older high socioeconomic status participants, suggesting the importance of socioeconomic factor when it comes to the association between MetS and cognitive impairment [42].
On the other hand, many recent studies reported that MetS is related to an increased risk of progression from MCI to dementia [44, 45]. In the SLAS study, MetS was associated with an increased risk of progression from MCI to dementia [40•]. While the SLAS study did not specify dementia subtypes, Lee, and colleagues reported an increased risk of all dementia types including both Alzheimer’s disease (AD) and vascular dementia (VD) [46]. Reports also exist of only VD [44] or only AD dementia [47] when both dementia types are compared to each other. It is more plausible, however, that MetS is more prevalent in VD than it is in AD dementia given that cardiovascular risk factors such high blood pressure, hyperglycemia and dyslipidemia are individual risk factors of VD which is primarily due to micro- and macrovascular disease such as small and large strokes [44, 46].
Among subjects with MetS, there may be differences in dementia progression depending on whether their MetS status improved or worsened. Fan et al. reported that there is a higher risk of dementia in patients with worsened MetS compared to those with improved MetS [48•]. Likewise, improvement in MetS status can result in reduced risk of dementia [46, 48•]. Categories of persistent, worsened and improved were defined by using changes of MetS diagnosis at different screening points. Fan and colleagues used 2 screenings that are 5 years apart where persistent MetS was defined as a diagnosis of Mets at the two screenings points; Worsened Mets as no MetS at the first screening and MetS at the second screening; and Improved MetS as MetS diagnosis at the first screening and no MetS at the second screening [48•]. These findings suggest that interventions that modify the trajectory of MetS may reduce the risk of dementia.
MetS and Biomarkers of Alzheimer’s Disease and Other Dementias
Advances in in-vivo brain imaging, cerebral spinal fluid (CSF) and blood biomarkers have led researchers to use in vivo biomarkers to define AD. The current research framework from the National Institute on Aging and Alzheimer’s Association (NIA-AA) suggests a biologic definition of AD that focuses on amyloid (Aβ), tau, and neurodegeneration as constructs regardless of cognitive impairment [49]. According to the NIA-AA, evidence of brain Aβ by biomarkers defines AD pathologic change and the AD continuum [49], making Aβ the primary construct of AD. There is a dearth of studies that have examined the association between MetS as a construct and biomarkers of AD and the associations in these studies are inconsistent [50]. Most studies report no association between MetS and AD neuropathology [51, 52]. In the Baltimore Longitudinal Study of Aging (BLSA), Gomez and colleagues [51] reported an association between MetS and accelerated Aβ deposition on amyloid Positron Emission Tomography (PET), only among Aβ positive participants, suggesting that pre-existing amyloid pathology is required in order to have an accelerating effect of MetS on further Aβ deposition. As such, subjects with no significant Aβ deposition at baseline may not be affected by MetS. Therefore, MetS could be an important factor in the progression of AD pathology but not necessarily the initiation of Aβ accumulation [51]. Similar to MetS, conflicting results are reported in regard to components of MetS. Some studies reported no association between Aβ on PET imaging and dyslipidemia [52, 53], high blood pressure [52, 54, 55] and waist circumference/obesity [52, 56]. On post-mortem neuropathology, Crane and colleagues reported no associations between glucose levels and Braak neurofibrillary tangles (representing tau) or neuritic plaque (representing Aβ plaques) [57]. Others however did report positive associations between Aβ on PET imaging, high blood pressure [51], and hyperglycemia [58]. Using CSF biomarkers of Aβ and tau, Nägga et al. reported a positive association between higher levels of triglycerides in midlife and higher CSF Aβ42 and Aβ42/p-tau ratio 20 years later [59]. Inconsistent results between MetS and AD pathology may be due to the few studies with the abilities to examine this association or potentially a result of the heterogeneity between studies in terms of demographics, specifically the age of AD biomarker measurement [50]. More longitudinal studies are needed in order to assess temporality between MetS and AD biomarkers [50].
Several studies have investigated and reported an association between MetS and biomarkers of CVD, an important factor in the clinical manifestation of AD [60, 61]. CVD and MetS are two interlinked conditions [62]. In fact, one of the feared complications of MetS along with cardiovascular disease is stroke, which is the most common manifestation of CVD [63, 64]. Stroke is a well-known cause of neurologic deficits, cognitive impairment and dementia [65, 66]. MetS is also associated with subclinical manifestations of CVD, including microinfarcts, microbleeds and white matter lesions [63]. These small silent brain insults are usually incidentally found in neuroimaging and a large body of literature do correlate these lesions with cognitive decline and dementia [63, 67, 68]. Among the MetS components, impaired glycemia, high blood pressure, and obesity were most often examined and were associated with cerebrovascular disease measured using magnetic resonance imaging (i.e., higher prevalence of microinfarcts and microbleeds) and worse brain microstructural integrity measured using diffusion tensor imaging (i.e., lower fractional anisotropy suggesting adverse alterations in white matter connectivity) [67].
Conclusion
MetS is an important risk factor for cognitive dysfunction. However, as discussed in the present review, many factors play a role in this association and account for some of the discrepancies observed in the literature. More longitudinal studies are needed to assess causality between MetS and cognitive dysfunction. When examining cognitive function, ideally these studies should use a battery of neuropsychological tests that tap into multiple cognitive domains instead of relying on a single test or on cognitive screening tools. More studies are also needed to assess which MCI subtype is more related to MetS. Similarly, more studies are needed to assess the association between AD biomarkers and MetS. Furthermore, among MetS components: high blood pressure, high waist circumference and hyperglycemia were among the strongest predictors of cognitive function. It should be noted however that our focus in this review was studies that examined MetS as a construct and we discuss MetS components according to findings from these studies.
Finally, there have been several clinical trials that target individual components of MetS such as blood pressure [69, 70], glycemic control [71], or lipid control [72, 73]. An intervention study that targets all MetS components is potentially not feasible due to cost. Most MetS components however are associated with excess weight (blood pressure, glucose, and lipid levels) [74], and therefore may show reductions in response to a weight loss intervention and have downstream impacts on cognitive outcomes [75, 76].
Based on this review, data suggest that MetS is associated with cognitive impairment. Further research is needed on how preventing or treating MetS across the life course will impact downstream cognitive outcomes.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Alzheimer’s disease facts and figures. Alzheimers Dement. 2021;17(3):327–406. https://doi.org/10.1002/alz.12328.
Karr JE, Graham RB, Hofer SM, Muniz-Terrera G. When does cognitive decline begin? A systematic review of change point studies on accelerated decline in cognitive and neurological outcomes preceding mild cognitive impairment, dementia, and death. Psychol Aging. 2018;33(2):195–218. https://doi.org/10.1037/pag0000236.
Rochlani Y, Pothineni NV, Kovelamudi S, Mehta JL. Metabolic syndrome: pathophysiology, management, and modulation by natural compounds. Ther Adv Cardiovasc Dis. 2017;11(8):215–25. https://doi.org/10.1177/1753944717711379.
Huang PL. A comprehensive definition for metabolic syndrome. Dis Model Mech. 2009;2(5–6):231–7. https://doi.org/10.1242/dmm.001180.
Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112(17):2735–52.
Moore JX, Chaudhary N, Akinyemiju T. Metabolic syndrome prevalence by race/ethnicity and sex in the United States, National Health and Nutrition Examination Survey, 1988–2012. Prev Chronic Dis. 2017;14:E24. https://doi.org/10.5888/pcd14.160287.
Park Y-W, Zhu S, Palaniappan L, Heshka S, Carnethon MR, Heymsfield SB. The metabolic syndrome: prevalence and associated risk factor findings in the US population from the Third National Health and Nutrition Examination Survey, 1988–1994. Arch Intern Med. 2003;163(4):427–36. https://doi.org/10.1001/archinte.163.4.427.
Asssociation AP. Cognition. 2021. https://dictionary.apa.org/cognition.
McCollum L, Karlawish J. Cognitive impairment evaluation and management. Med Clin North Am. 2020;104(5):807–25. https://doi.org/10.1016/j.mcna.2020.06.007.
Petersen RC, Caracciolo B, Brayne C, Gauthier S, Jelic V, Fratiglioni L. Mild cognitive impairment: a concept in evolution. J Intern Med. 2014;275(3):214–28. https://doi.org/10.1111/joim.12190.
Duong S, Patel T, Chang F. Dementia: what pharmacists need to know. Can Pharm J (Ott). 2017;150(2):118–29. https://doi.org/10.1177/1715163517690745.
Petersen RC. Mild cognitive impairment. Continuum (Minneap Minn). 2016;22(2 Dementia):404–18. https://doi.org/10.1212/CON.0000000000000313.
Przybycien-Gaweda PM, Gwee X, Gao Q, Chua DQL, Fam J, Ng TP. Metabolic syndrome and cognition: follow-up study of Chinese over-55-year-olds. Dement Geriatr Cogn Disord. 2020;49(2):129–37. https://doi.org/10.1159/000509124.
Lai MMY, Ames DJ, Cox KL, Ellis KA, Sharman MJR, Hepworth G, et al. Association between cognitive function and clustered cardiovascular risk of metabolic syndrome in older adults at risk of cognitive decline. J Nutr Health Aging. 2020;24(3):300–4. https://doi.org/10.1007/s12603-020-1333-4.
Foret JT, Oleson S, Hickson B, Valek S, Tanaka H, Haley AP. Metabolic syndrome and cognitive function in midlife. Arch Clin Neuropsychol. 2020. https://doi.org/10.1093/arclin/acaa112.
Buyo M, Takahashi S, Iwahara A, Tsuji T, Yamada S, Hattori S, et al. Metabolic syndrome and cognitive function: cross-sectional study on community-dwelling non-demented older adults in Japan. J Nutr Health Aging. 2020;24(8):878–82. https://doi.org/10.1007/s12603-020-1412-6.
Bahchevanov KM, Dzhambov AM, Chompalov KA, Massaldjieva RI, Atanassova PA, Mitkov MD. Contribution of components of metabolic syndrome to cognitive performance in middle-aged adults. Arch Clin Neuropsychol. 2020. https://doi.org/10.1093/arclin/acaa081.
Wooten T, Ferland T, Poole V, Milberg W, McGlinchey R, DeGutis J, et al. Metabolic risk in older adults is associated with impaired sustained attention. Neuropsychology. 2019;33(7):947–55. https://doi.org/10.1037/neu0000554.
Mangone A, Yates KF, Sweat V, Joseph A, Convit A. Cognitive functions among predominantly minority urban adolescents with metabolic syndrome. Appl Neuropsychol Child. 2018;7(2):157–63. https://doi.org/10.1080/21622965.2017.1284662.
González HM, Tarraf W, Vásquez P, Sanderlin AH, Rosenberg NI, Davis S, et al. Metabolic syndrome and neurocognition among diverse middle-aged and older Hispanics/Latinos: HCHS/SOL results. Diabetes Care. 2018;41(7):1501–9. https://doi.org/10.2337/dc17-1896.
Tsai CK, Kao TW, Lee JT, Wu CJ, Hueng DY, Liang CS, et al. Increased risk of cognitive impairment in patients with components of metabolic syndrome. Medicine (Baltimore). 2016;95(36): e4791. https://doi.org/10.1097/md.0000000000004791.
Rubens M, Ramamoorthy V, Saxena A, George F, Shehadeh N, Attonito J, et al. Relationship between metabolic syndrome and cognitive abilities in U.S. adolescents. Metab Syndr Relat Disord. 2016;14(8):397–403. https://doi.org/10.1089/met.2016.0015.
Wang JY, Zhang L, Liu J, Yang W, Ma LN. Metabolic syndrome, ApoE genotype, and cognitive dysfunction in an elderly population: a single-center, case-control study. World J Clin Cases. 2021;9(5):1005–15. https://doi.org/10.12998/wjcc.v9.i5.1005.
Mehra A, Suri V, Kumari S, Avasthi A, Grover S. Association of mild cognitive impairment and metabolic syndrome in patients with hypertension. Asian J Psychiatr. 2020;53: 102185. https://doi.org/10.1016/j.ajp.2020.102185.
Harrison SL, Stephan Bc Fau - Siervo M, Siervo M Fau - Granic A, Granic A Fau - Davies K, Davies K Fau - Wesnes KA, Wesnes Ka Fau - Kirkwood TBL et al. Is there an association between metabolic syndrome and cognitive function in very old adults? The Newcastle 85+ Study. 2015(1532–5415 (Electronic)).
Assuncao N, Sudo FK, Drummond C, de Felice FG, Mattos P. Metabolic syndrome and cognitive decline in the elderly: a systematic review. PLoS ONE. 2018;13(3): e0194990. https://doi.org/10.1371/journal.pone.0194990.
Viscogliosi G, Chiriac IM, Andreozzi P, Ettorre E. The metabolic syndrome predicts longitudinal changes in clock drawing test performance in older nondemented hypertensive individuals. Am J Geriatr Psychiatry. 2016;24(5):359–63. https://doi.org/10.1016/j.jagp.2015.09.001.
Overman MJ, Pendleton N, O’Neill TW, Bartfai G, Casanueva FF, Forti G, et al. Glycemia but not the metabolic syndrome is associated with cognitive decline: findings from the European Male Ageing Study. Am J Geriatr Psychiatry. 2017;25(6):662–71. https://doi.org/10.1016/j.jagp.2017.02.004.
• Kazlauskaite R, Janssen I, Wilson RS, Appelhans BM, Evans DA, Arvanitakis Z, et al. Is midlife metabolic syndrome associated with cognitive function change? The Study of Women’s Health Across the Nation. J Clin Endocrinol Metab. 2020;105(4):e1093–105. https://doi.org/10.1210/clinem/dgaa067. This is a large multi-racial/ethnic population study with a long follow-up period and multiple assessments.
• Bangen KJ, Armstrong NM, Au R, Gross AL. Metabolic syndrome and cognitive trajectories in the Framingham Offspring Study. J Alzheimers Dis. 2019;71(3):931–43. https://doi.org/10.3233/jad-190261. This is a large population study with a large age range (40 to 80+) and a long follow-up, 41 years for metabolic risk factors and 13 years with cognitive asseseemnts
Viscogliosi G, Donfrancesco C, Palmieri L, Giampaoli S. The metabolic syndrome and 10-year cognitive and functional decline in very old men. A population-based study Arch Gerontol Geriatr. 2017;70:62–6. https://doi.org/10.1016/j.archger.2016.12.008.
Foong HF, Hamid TA, Ibrahim R, Haron SA, Shahar S. Chronic condition as a mediator between metabolic syndrome and cognition among community-dwelling older adults: The moderating role of sex. Geriatr Gerontol Int. 2017;17(11):1914–20. https://doi.org/10.1111/ggi.12993.
Kim YH, Kim NH, Jung MH, Kim HJ. Sex differences in metabolic risk indicator of dementia in an elderly urban Korean population: a community-based cross-sectional study. Geriatr Gerontol Int. 2017;17(11):2136–42. https://doi.org/10.1111/ggi.13049.
Vanhanen M, Koivisto K, Moilanen L, Helkala EL, Hänninen T, Soininen H, et al. Association of metabolic syndrome with Alzheimer disease. Neurology. 2006;67(5):843. https://doi.org/10.1212/01.wnl.0000234037.91185.99.
Schuur M, Henneman P, van Swieten JC, Zillikens MC, de Koning I, Janssens AC, et al. Insulin-resistance and metabolic syndrome are related to executive function in women in a large family-based study. Eur J Epidemiol. 2010;25(8):561–8. https://doi.org/10.1007/s10654-010-9476-y.
Sweat V, Yates KF, Migliaccio R, Convit A. Obese adolescents show reduced cognitive processing speed compared with healthy weight peers. Child Obes. 2017;13(3):190–6. https://doi.org/10.1089/chi.2016.0255.
Del Brutto OH, Mera RM, Zambrano M. Metabolic syndrome correlates poorly with cognitive performance in stroke-free community-dwelling older adults: a population-based, cross-sectional study in rural Ecuador. Aging Clin Exp Res. 2016;28(2):321–5. https://doi.org/10.1007/s40520-015-0404-6.
Chen B, Jin X, Guo R, Chen Z, Hou X, Gao F, et al. Metabolic syndrome and cognitive performance among Chinese ≥50 years: a cross-sectional study with 3988 participants. Metab Syndr Relat Disord. 2016;14(4):222–7. https://doi.org/10.1089/met.2015.0094.
Wang X, Ji L, Tang Z, Ding G, Chen X, Lv J, et al. The association of metabolic syndrome and cognitive impairment in Jidong of China: a cross-sectional study. BMC Endocr Disord. 2021;21(1):40. https://doi.org/10.1186/s12902-021-00705-w.
• Ng TP, Feng L, Nyunt MS, Feng L, Gao Q, Lim ML, et al. Metabolic syndrome and the risk of mild cognitive impairment and progression to dementia: follow-up of the Singapore Longitudinal Ageing Study Cohort. JAMA Neurol. 2016;73(4):456–63. https://doi.org/10.1001/jamaneurol.2015.4899. This a large population, prospective study that examined the association between metabolic syndrome and the risk of MCI as well as the risk of progression from MCI to dementia in cognitvely normal middle-aged adults.
Feinkohl I, Janke J, Hadzidiakos D, Slooter A, Winterer G, Spies C, et al. Associations of the metabolic syndrome and its components with cognitive impairment in older adults. BMC Geriatr. 2019;19(1):77. https://doi.org/10.1186/s12877-019-1073-7.
Martinez-Miller EE, Kohl HW 3rd, Barlow CE, Willis BL, DeFina LF. Metabolic syndrome and cognitive impairment among high socioeconomic, nondemented older US adults. J Am Geriatr Soc. 2019;67(7):1437–43. https://doi.org/10.1111/jgs.15836.
Bae S, Shimada H, Lee S, Makizako H, Lee S, Harada K, et al. The relationships between components of metabolic syndrome and mild cognitive impairment subtypes: a cross-sectional study of Japanese older adults. J Alzheimers Dis. 2017;60(3):913–21. https://doi.org/10.3233/jad-161230.
Atti AR, Valente S, Iodice A, Caramella I, Ferrari B, Albert U, et al. Metabolic syndrome, mild cognitive impairment, and dementia: a meta-analysis of longitudinal studies. Am J Geriatr Psychiatry. 2019;27(6):625–37. https://doi.org/10.1016/j.jagp.2019.01.214.
Pal K, Mukadam N, Petersen I, Cooper C. Mild cognitive impairment and progression to dementia in people with diabetes, prediabetes and metabolic syndrome: a systematic review and meta-analysis. Soc Psychiatry Psychiatr Epidemiol. 2018;53(11):1149–60. https://doi.org/10.1007/s00127-018-1581-3.
Lee JE, Shin DW, Han K, Kim D, Yoo JE, Lee J, et al. Changes in metabolic syndrome status and risk of dementia. J Clin Med. 2020;9(1). https://doi.org/10.3390/jcm9010122.
Kim YJ, Kim SM, Jeong DH, Lee SK, Ahn ME, Ryu OH. Associations between metabolic syndrome and type of dementia: analysis based on the National Health Insurance Service database of Gangwon province in South Korea. Diabetol Metab Syndr. 2021;13(1):4. https://doi.org/10.1186/s13098-020-00620-5.
• Fan YC, Chou CC, You SL, Sun CA, Chen CJ, Bai CH. Impact of worsened metabolic syndrome on the risk of dementia: a nationwide cohort study. J Am Heart Assoc. 2017;6(9). https://doi.org/10.1161/jaha.116.004749. This is the first study to examine causal associations between changes in metabolic syndrome status and the risk of dementia.
Jack CR Jr, Bennett DA, Blennow K, Carrillo MC, Dunn B, Haeberlein SB, et al. NIA-AA Research Framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dement. 2018;14(4):535–62. https://doi.org/10.1016/j.jalz.2018.02.018.
Luchsinger JA, Zetterberg H. Tracking the potential involvement of metabolic disease in Alzheimer’s disease-Biomarkers and beyond. Int Rev Neurobiol. 2020;154:51–77. https://doi.org/10.1016/bs.irn.2020.03.014.
Gomez G, Beason-Held LL, Bilgel M, An Y, Wong DF, Studenski S, et al. Metabolic syndrome and amyloid accumulation in the aging brain. J Alzheimers Dis. 2018;65(2):629–39. https://doi.org/10.3233/jad-180297.
Palta P, Rippon B, Tahmi M, Sherwood G, Soto L, Ceballos F, et al. Metabolic syndrome and its components in relation to in vivo brain amyloid and neurodegeneration in late middle age. Neurobiol Aging. 2021;97:89–96. https://doi.org/10.1016/j.neurobiolaging.2020.09.023.
Bennett EE, Gianattasio KZ, Hughes TM, Mosley TH, Wong DF, Gottesman RF, et al. The association between midlife lipid levels and late-life brain amyloid deposition. Neurobiol Aging. 2020;In press.
Lane CA, Barnes J, Nicholas JM, Sudre CH, Cash DM, Parker TD, et al. Associations between blood pressure across adulthood and late-life brain structure and pathology in the neuroscience substudy of the 1946 British birth cohort (Insight 46): an epidemiological study. Lancet Neurol. 2019;18(10):942–52. https://doi.org/10.1016/S1474-4422(19)30228-5.
Gottesman RF, Schneider ALC, Zhou Y, Coresh J, Green E, Gupta N, et al. Association between midlife vascular risk factors and estimated brain amyloid deposition. JAMA. 2017;317(14):1443–50. https://doi.org/10.1001/jama.2017.3090.
Vemuri P, Knopman DS, Lesnick TG, Przybelski SA, Mielke MM, Graff-Radford J, et al. Evaluation of amyloid protective factors and Alzheimer disease neurodegeneration protective factors in elderly individuals. JAMA Neurol. 2017;74(6):718–26. https://doi.org/10.1001/jamaneurol.2017.0244.
Crane PK, Walker RL, Sonnen J, Gibbons LE, Melrose R, Hassenstab J, et al. Glucose levels during life and neuropathologic findings at autopsy among people never treated for diabetes. Neurobiol Aging. 2016;48:72–82. https://doi.org/10.1016/j.neurobiolaging.2016.07.021.
Morris JK, Vidoni ED, Wilkins HM, Archer AE, Burns NC, Karcher RT, et al. Impaired fasting glucose is associated with increased regional cerebral amyloid. Neurobiol Aging. 2016;44:138–42. https://doi.org/10.1016/j.neurobiolaging.2016.04.017.
Nägga K, Gustavsson A-M, Stomrud E, Lindqvist D, van Westen D, Blennow K, et al. Increased midlife triglycerides predict brain β-amyloid and tau pathology 20 years later. Neurology. 2018;90(1):e73–81. https://doi.org/10.1212/WNL.0000000000004749.
Santos CY, Snyder PJ, Wu W-C, Zhang M, Echeverria A, Alber J. Pathophysiologic relationship between Alzheimer’s disease, cerebrovascular disease, and cardiovascular risk: a review and synthesis. Alzheimer’s & dementia (Amsterdam, Netherlands). 2017;7:69–87. https://doi.org/10.1016/j.dadm.2017.01.005.
Iadecola C, Gottesman RF. Cerebrovascular alterations in Alzheimer disease. Circ Res. 2018;123(4):406–8. https://doi.org/10.1161/CIRCRESAHA.118.313400.
Jabir NR, Firoz CK, Khan MS, Zaidi SK, Ashraf GM, Shakil S, et al. Potential linkage between cerebrovascular diseases and metabolic syndrome. Curr Drug Metab. 2017;18(1):62–8. https://doi.org/10.2174/1389200217666160810155055.
Portegies MLP, Koudstaal PJ, Ikram MA. Chapter 14-Cerebrovascular disease. In: Aminoff MJ, Boller F, Swaab DF, editors. Handbook of clinical neurology. Elsevier; 2016. p. 239–61.
Roever L, Resende ES, Diniz ALD, Penha-Silva N, O'Connell JL, Gomes PFS, et al. Metabolic syndrome and risk of stroke: protocol for an update systematic review and meta-analysis. Medicine. 2018;97(15):e9862-e. https://doi.org/10.1097/MD.0000000000009862.
Tang EY, Amiesimaka O, Harrison SL, Green E, Price C, Robinson L, et al. Longitudinal effect of stroke on cognition: a systematic review. J Am Heart Assoc. 2018;7(2). https://doi.org/10.1161/jaha.117.006443.
Mijajlović MD, Pavlović A, Brainin M, Heiss WD, Quinn TJ, Ihle-Hansen HB, et al. Post-stroke dementia-a comprehensive review. BMC Med. 2017;15(1):11. https://doi.org/10.1186/s12916-017-0779-7.
Alfaro FJ, Gavrieli A, Saade-Lemus P, Lioutas VA, Upadhyay J, Novak V. White matter microstructure and cognitive decline in metabolic syndrome: a review of diffusion tensor imaging. Metabolism. 2018;78:52–68. https://doi.org/10.1016/j.metabol.2017.08.009.
Teng Z, Dong Y, Zhang D, An J, Lv P. Cerebral small vessel disease and post-stroke cognitive impairment. Int J Neurosci. 2017;127(9):824–30. https://doi.org/10.1080/00207454.2016.1261291.
Group TSMIftSR. Effect of intensive vs standard blood pressure control on probable dementia: a randomized clinical trial. JAMA. 2019;321(6):553–61. https://doi.org/10.1001/jama.2018.21442.
Gupta A, Perdomo S, Billinger S, Beddhu S, Burns J, Gronseth G. Treatment of hypertension reduces cognitive decline in older adults: a systematic review and meta-analysis. BMJ Open. 2020;10(11): e038971. https://doi.org/10.1136/bmjopen-2020-038971.
Tang X, Cardoso MA, Yang J, Zhou J-B, Simó R. Impact of intensive glucose control on brain health: meta-analysis of cumulative data from 16,584 patients with type 2 diabetes mellitus. Diabetes Therapy. 2021;12(3):765–79. https://doi.org/10.1007/s13300-021-01009-x.
Giugliano RP, Mach F, Zavitz K, Kurtz C, Schneider J, Wang H, et al. Design and rationale of the EBBINGHAUS trial: a phase 3, double-blind, placebo-controlled, multicenter study to assess the effect of evolocumab on cognitive function in patients with clinically evident cardiovascular disease and receiving statin background lipid-lowering therapy-a cognitive study of patients enrolled in the FOURIER trial. Clin Cardiol. 2017;40(2):59–65. https://doi.org/10.1002/clc.22678.
Sano M, Bell KL, Galasko D, Galvin JE, Thomas RG, van Dyck CH, et al. A randomized, double-blind, placebo-controlled trial of simvastatin to treat Alzheimer disease. Neurology. 2011;77(6):556–63. https://doi.org/10.1212/WNL.0b013e318228bf11.
Phelan S, Wadden TA, Berkowitz RI, Sarwer DB, Womble LG, Cato RK, et al. Impact of weight loss on the metabolic syndrome. Int J Obes. 2007;31(9):1442–8. https://doi.org/10.1038/sj.ijo.0803606.
Veronese N, Facchini S, Stubbs B, Luchini C, Solmi M, Manzato E, et al. Weight loss is associated with improvements in cognitive function among overweight and obese people: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2017;72:87–94. https://doi.org/10.1016/j.neubiorev.2016.11.017.
Espeland MA, Carmichael O, Hayden K, Neiberg RH, Newman AB, Keller JN, et al. Long-term impact of weight loss intervention on changes in cognitive function: exploratory analyses from the Action for Health in Diabetes Randomized Controlled Clinical Trial. J Gerontol A Biol Sci Med Sci. 2018;73(4):484–91. https://doi.org/10.1093/gerona/glx165.
Lee JY, Han K, Han E, Kim G, Cho H, Kim KJ, et al. Risk of incident dementia according to metabolic health and obesity status in late life: a population-based cohort study. J Clin Endocrinol Metab. 2019;104(7):2942–52. https://doi.org/10.1210/jc.2018-01491.
Funding
Priya Palta has received grant funding from the National Institutes of Health. José A. Luchsinger reports the following grants: K24AG045334, RF1AG051556, R01AG050440, R01AG058571, R01AG058969, and R01AG055299.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
JA Luchsinger receives a stipend from Wolters Kluwer, N.V. as Editor-in-Chief of the journal Alzheimer’s Disease and Associated Disorders, receives royalties from Springer for the book Diabetes and the Brain, and has served as a paid consultant to vTv therapeutics, Inc., Recruitment Partners, and NYU Langone. The other authors have no other conflicts of interests to declare.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Psychological Aspects of Cardiovascular Diseases
Rights and permissions
About this article

Cite this article
Tahmi, M., Palta, P. & Luchsinger, J.A. Metabolic Syndrome and Cognitive Function. Curr Cardiol Rep 23, 180 (2021). https://doi.org/10.1007/s11886-021-01615-y
Accepted:
Published:
DOI: https://doi.org/10.1007/s11886-021-01615-y