
Abstract
Observations available for patients with acute heart failure (HF) show conflicting results, and the prognostic role of anaemia ascertained on hospital admission is not well defined. We investigated the database of the Italian Survey on Acute Heart Failure (IS-AHF) to analyze prevalence, factors associated with and the prognostic role of anaemia (defined as haemoglobin < 12 g/dl) in patients hospitalized for acute HF with either depressed or preserved (>40%) ejection fraction (EF). The median haemoglobin level of the 2,318 patients considered in this analysis was 13 g/dl (inter-quartile range 11.5–14.3). The prevalence of anaemia was 31%. Patients who had anaemia were older, more frequently female gender, hospitalized for a chronic destabilized HF, had higher prevalence of preserved EF, hyponatremia, elevated troponin and other comorbidities (including diabetes, peripheral artery disease, chronic renal failure) than those who did not have anaemia. During the hospital stay, they were treated with higher doses of diuretics, and more frequently required mechanical ventilation and ultrafiltration, and less frequently received ACEi/ARB, aldosterone blockers and beta-blockers at hospital discharge. In-hospital mortality was 12.1 and 5.3% in patients with and without anaemia, respectively (p < 0.0001). In the multivariable analysis, anaemia was a significant independent predictor of in-hospital mortality apart from age, low systolic blood pressure, impaired renal function, elevated troponin assay, the non use of beta-blocker and the requirement of inotropic drug. In conclusion, anaemia diagnosed at hospital admission for acute HF is a frequent comorbidity with meaningful implications on the clinical management and prognosis both in patients with reduced and preserved EF.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In spite of the substantial improvements in evidence-based therapy on heart failure (HF) that has occurred in the past few decades [1], hospitalizations for acute HF exhibit a relentless increase [2], and since HF prevalence increases with age [3], such a trend will presumptively proceed as result of the ageing of western societies. The management of HF in elderly people is usually complicated by the frequent coexistence of other clinical conditions [4], and among them, anaemia is increasingly recognized as a frequent comorbidity with relevant clinical implications [5, 6]. On the other hand, in patients with acute HF, conflicting data exist on the prognostic role of anaemia, which has never been clearly defined [7–9].
The aims of this study were to analyse (1) the prevalence of anaemia in a population of patients admitted for acute HF, (2) the clinical, demographic variables correlated with anaemia, (3) whether anaemia is an independent predictor of in-hospital mortality, and (4) whether anaemia has a similar prognostic role in patients with either depressed or preserved EF.
Methods
We investigated the database of the Italian Survey on Acute Heart Failure (IS-AHF), whose protocol and results are reported elsewhere [10]. Briefly, IS-AHF is a nationwide, prospective, observational study conducted from March 1, 2004 to May 31, 2004 that aimed to analyze the clinical aspects, the prognosis and the therapeutic approaches of all the consecutive patients admitted for acute HF in 206 Italian Cardiology Centres with Intensive Coronary Care Units. The enrolling Centres were well representative of the geographic distribution and level of technology of the network of the Italian hospitals.
Study population
IS-AHF was a strictly observational study designed to evaluate the current practice of management of AHF patients admitted to cardiology centres. Out of the 2,807 consecutive patients admitted with a diagnosis of acute HF in the IS-AHF database, for the purpose of the present study, we excluded the patients who reported any history of neoplasia or gastro-enteric disease (413 patients), as well as those with unavailable data on the haemoglobin level at hospital entry (76 patients). Therefore, the analyzed cohort in the present study consists of 2,318 subjects. Local Institutional Review Boards were notified of the study according to national rules.
Baseline information on demographics, medical history and prior medication were gathered at the time of hospital admission, whereas data on physical examination and selected biochemical variables, were checked out at hospital entry. Left ventricular ejection fraction (LVEF) was collected during hospitalization, as well as the use of pharmacological treatments and procedures (mechanical ventilation and ultrafiltration) aimed to manage respiratory failure and refractory congestion. We registered the length of stay, and the in-hospital mortality, and reported the drugs prescribed at hospital discharge.
Statistics
Categorical variables are presented as frequencies and percentages. The duration of in-hospital stay, the dose and the duration of furosemide administration are presented as the median value (and inter-quartile ranges, IQR). Other continuous variables are presented as their means with standard deviations. Univariate associations between baseline characteristics, main diagnostic procedures, pharmacological/non-pharmacological treatments and all-cause, in-hospital mortality were tested. Categorical variables were compared by the chi-square test and continuous variables by the t test or the Mann–Whitney U Test. Age, gender, presenting clinical profile, type of HF (de novo/worsening) and all the variables significantly associated at the unadjusted analysis with all-cause mortality, among which anaemia, were included in a multivariable analysis (logistic model) with the aim of identifying the independent predictors of all-cause in-hospital mortality. The linearity of the continuous variables was tested by piecewise polynomials (the restricted cubic spline), and we particularly estimated the relationship between in-hospital mortality and different haemoglobin levels. Receiver Operating Characteristic (ROC) analysis was used to assess the best cut-off of haemoglobin level in order to identify patients with a poorer prognosis. For categorization, “anaemia” was defined when values of haemoglobin level were below the prognostic cut-off value.
A multiple imputation technique was therefore used to avoid the loss of the information in those subjects with some missing variables. According to this procedure, five complete data sets were obtained using the MICE package [11] and five full data analyses were completed. Finally, the results were pooled using the method of Barnard and Rubin [12]. A p value < 0.05 was considered statistically significant. All tests were two-sided. Analyses were performed with SAS system software (SAS Institute Inc, Cary, NC, USA) and the R Development Core Team (R Foundation for Statistical Computing, Vienna, Italy).
Results
The distribution of haemoglobin level on hospital admission is shown in Fig. 1. The mean haemoglobin level in the whole cohort was 12.9 ± 2.1 g/dl (median: 13 g/dl; IQR: 11.5–14.3 g/dl). The cut-off point value of haemoglobin with the best specificity and sensitivity in predicting adverse outcome (ROC analysis) was 12 g/dl (Fig. 2). This value identified “anaemia,” which was a common condition affecting 719 out of 2,318 pts (prevalence 31%). The demographic, clinical characteristics and laboratory data of the whole cohort of the 2,318 patients are reported in Table 1. The anaemic HF patients in contrast to those with higher haemoglobin levels, were significantly older, of female gender, and with significantly higher prevalence of other comorbidities like diabetes, peripheral artery disease, or chronic renal failure. In contrast to HF patients with normal haemoglobin levels, they were hospitalized, characteristically, for a “chronic” destabilized illness, with more hospital admissions for HF in the previous year, and finally, they showed a slight but significantly higher prevalence of subjects with a normal or mildly impaired LVEF. Patient with low haemoglobin level, indeed, were more frequently on therapy with Angiotensin Converting Enzyme inhibitor (ACEi) or Angiotensin Receptor Blocker (ARB), diuretics, Anti-Aldosterone Agents (AAA), Anticoagulant or Antiplatelets drugs.

Distribution of haemoglobin level at hospital admission in the 2,318 patients enrolled in the study

ROC curve for anaemia. Area under the curve is shown. The cut-off point identifying the subgroup of patients with an adverse outcome was 12 g/dl (area under the curve 0.617)
At hospital admission, patients with low haemoglobin levels revealed some slight but significant differences from those not anaemic in clinical signs (Table 1). They showed an inferior prevalence of overweight/obese subjects (BMI > 25 kg/m2), presented lower blood pressure values, and showed more evidence of peripheral venous congestion than those with normal haemoglobin levels. There were also some significant differences in laboratory values in anaemic patients with respect to those with normal haemoglobin level: they had a great incidence of hyponatremia and an elevated level of troponin at hospital admission; furthermore, the anaemic HF patients presented higher values of azotemia, creatininemia and lower serum bilirubin levels.
In-hospital treatment and outcome
Table 2 reports how acute HF patients with/without anaemia were managed during the in-hospital phase: anaemic patients received higher doses of loop diuretics for a longer period of time, and more frequently needed the support of inotropic drugs. Patients with anaemia, furthermore, required more frequent mechanical ventilation, and presented a twofold risk in the development of acute renal failure, or to receive ultrafiltration.
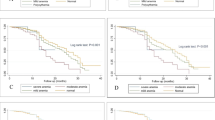
As shown in Fig. 3, there is an inverse relationship between the risk of death during hospital stay and haemoglobin level that seems “almost linear”. The patient with low haemoglobin concentration presents significantly higher in-hospital mortality for all-causes. In these patients, the cause of death was cardiac in 92 (sudden death in 32%, pump failure in 68%), vascular in 2% and non-cardiovascular in 6% of cases. In patients without anaemia, the cause of death was cardiac in 88% (sudden death in 39%, pump failure in 61%), vascular in 5% and non-cardiovascular in 7% of cases (p = 0.6). Death for acute myocardial infarction occurred in 14 patients with anaemia (1.9%) and in 10 without anaemia (0.6%, p = ns). By considering separately the subgroups with preserved (> 40%) and reduced (≤ 40%) LVEF the in-hospital all cause mortality was higher in the latter than in the former, but the presence of anaemia significantly increases the risk of death in both groups, by roughly doubling the in-hospital mortality (Fig. 4). Also the length of hospitalization, is significantly longer in patients with anaemia. At hospital discharge, patients with anaemia less frequently received a treatment with ACEI/ARB, AAA and beta-blockers.

Estimated relation between risk of in hospital death for the different haemoglobin levels. Log odds plot with 95% confidence intervals

All-cause in-hospital mortality by anaemia and EF levels (on 2,137 patients with EF measured)
Multivariable analysis
A haemoglobin level below 12 g/dl is confirmed to be a strong independent predictor of in-hospital mortality (odds ratio: 1.61, 95% confidence interval: 1.10–2.35, p = 0.013) apart from age, low systolic blood pressure, impaired renal function (expressed as high serum azotemia), evidence of myocardial damage, as suggested by elevated troponin levels, and use of inotropic drugs (Table 3).
Discussion
A low level of haemoglobin is frequently observed in patients with HF, and its prevalence depends on several variables: the severity of HF, the diagnostic criteria to define the anaemia, the selection of the patients enrolled and the setting of the study [4, 5]. Furthermore, because of marked fluid retention, above all in destabilized HF, a “pseudo anaemia” state may occur from hemodilution and extracellular blood volume expansion [13–15]. Nevertheless in HF, a “true” anaemia may occur, with a relevant prognostic role, owing to an intense derangement of erythropoiesis as is well documented as a result mainly of a blunted production or resistance state to erythropoietin, and an impaired iron metabolism [4, 5, 16, 17]. The studies performed in the community on patients with acute heart failure [7–9, 18–20] report a prevalence ranging from 44 to 62%. In our series, we confirm the high prevalence of anaemia in patients hospitalized for acute HF (31%). Such results differ largely from those reported by randomized clinical trials and observational studies on stable and younger patients with chronic HF [4, 5, 21–23]. The higher prevalence of anaemia reported in other series [OPTIMIZE-HF Registry (50%) [8] and Silva single-centre series (45%) [9], in which the definition of anaemia was based on the same cut-off of haemoglobin level may be the consequence of the inclusion in such studies of HF patients with gastrointestinal disease or cancer, clinical conditions with a high prevalence of anaemia, excluded in our cohort. Furthermore, our patients were Caucasian, and presented at a younger age and with less compromised renal function, relevant determinants of anaemia [18, 24, 25].
In our study, as in the OPTIMIZE Registry [8], a low haemoglobin level at hospital admission is significantly associated with a longer length of in-hospital stay, and independently predicts a greater in hospital all-cause mortality. Such observations, also reported in other large unselected cohorts of patients with acute HF [7, 8], underscore that a low haemoglobin level at hospital entry, below 12 g/dl in our case, is a powerful marker of adverse outcomes during hospital stay. The prognostic importance of a low haemoglobin level is not coloured by the HF aetiology, and furthermore is not alleviated by the presence of a preserved or mildly impaired systolic function. Our findings are consistent with previous studies [8, 26–29], and have relevant clinical implications. HF with preserved systolic function, indeed, is a clinical entity not well defined with a prognosis that is still controversial [30]. Findings from a large in-hospital study [31] underline the relevance of comorbidities in defining the prognosis of HF with preserved systolic function. Our study confirms that anaemia is a relevant prognostic marker in such a subset of HF patients. In our study, the relationship between the blood haemoglobin level and the risk of in hospital death is “almost” linear. This actually may be related to several components including less comorbidities associated with depressed erythrocytes production or shorter survival, better nutrition and nutrients absorption, less hemodilution that implies less systemic circulatory load and lower neurohormonal activation. Overall, in spite of a similar acute clinical presentation, this may suggest a less severe clinical status and HF stage in non-anemic patients. However, in our population, the magnitude of patients with haemoglobin levels above 16 g/dl was very low, and this situation could influence the right side of the relationship which could be actually “U” shaped, a trend already described in other series and justified by the potential disadvantageous effect of high blood viscosity in patients with HF.
It is well known that patients with HF and a low level of haemoglobin present more frequently with significant renal dysfunction [5, 7–9, 18, 24, 25, 32, 33]. This also is the case in our cohort. Further, patients with a haemoglobin level below 12 g/dl receive more intensive diuretic therapy, and more often develop acute renal failure. Besides enhancing a marked fluid retention and consequently hemodilution, when renal dysfunction coexists with HF (the so called “cardiorenal” syndrome), the interaction between heart and kidney broadens the activity of biologic mediators (the sympathetic nervous system, the renin–angiotensin–aldosteron system, nitric oxide and reactive oxygen species, chronic inflammatory states) [34–36] with induction of positive feedback loops and the amplification of a progressive dysfunction of both systems. In such a context, anaemia is a common and essential feature of the cardiorenal syndrome [35] that may play a critical role in the maintenance or even the progression of the syndrome [35–37], and the evolution toward the failure of both cardiac and renal systems. Acute HF is a leading cause of hospital acquired renal failure [36, 38], and, in such a context, anaemia further reducing oxygen delivery to a hypo perfused kidney may facilitate the progression of a worsened renal function to overt acute renal failure [36, 39, 40].
At hospital discharge, patients with anaemia less frequently receive evidence-based therapies, such as RAAS blockers, beta-blockers, AAA recommended for the therapy of HF. Our data confirm the results reported elsewhere [8]. There may be quite a few reasons why patients with anaemia are more likely to receive less than optimal discharge care. HF patients with low haemoglobin present more frequently renal dysfunction and diabetes, and show a significantly lower systolic blood pressure at hospital entry. However, we cannot rule out that fatigue, a common symptom of anaemia, may be a potential reason for failure to prescribe drugs such as ACEi/ARB and beta-blockers.
Limitations of the study
The present study has several limitations that must be taken in account. This report is a strictly observational survey, and many unmeasured variables may have been present that might influence the results. The haemoglobin level was obtained as a single measure at hospital admission, therefore, we cannot clarify and quantify the changes in haemoglobin to verify how many patients were affected with transitory anaemia or hemodilution. For a better stratification of HF patients with anaemia, we have excluded those with a history of gastrointestinal disease and history of cancer, however we do not have any information about aetiology and specific treatments of anaemia particularly with respect to blood transfusion, iron supplements and erythropoietin receptor stimulating agents. In regards to drug therapy, we cannot ascertain contraindications or intolerance to drugs recommended as evidence-based by guidelines. Furthermore, no comorbidity or severity index was used to adjust analyses. Our statistical approach provided for using all the variables significantly associated at the unadjusted analysis with all-cause mortality, among which anaemia, in a multivariable logistic model. Finally, it is important to underline that more than half of patients hospitalized for acute HF are managed by internal medicine wards in Italy; thus, present results do not necessarily apply to other populations with acute HF that could have been differently selected.
Conclusions
Our study underscores that anaemia is a frequent comorbidity in acute HF with relevant clinical implications, independent of the presence and degree of left ventricular systolic dysfunction, older age and lower systolic blood pressure. Prevalence of this prognostically adverse condition is high even in the community populations (such as ours), and in cohorts of patients without gastrointestinal disease or cancer, two frequent causes of non-cardiogenic anaemia that are frequent in HF patients, but were excluded in our investigation. Recent specific therapeutic approaches [41, 42] encourage to plan ad hoc studies assessing whether the pharmacological correction of anaemia can be associated with an improved outcome of patients with HF and low haemoglobin levels.
Reference
Jessup M, Brozena S (2003) Heart failure. N Engl J Med 348:2007–2018
Fang J, Mensah GA, Croft JB, Keenan NL (2008) Heart failure-related hospitalization in the US, 1979 to 2004. J Am Coll Cardiol 52:428–434
Bleumink GS, Knetsch AM, Sturkenboom MC, Straus SM, Hofman A, Deckers JW et al (2004) Quantifying the heart failure epidemic: prevalence, incidence rate, lifetime risk and prognosis of heart failure. The Rotterdam Study. Eur Heart J 25:1614–1619
Braunstein JB, Anderson GF, Gerstenblith G, Weller W, Niefeld M, Herbert R et al (2003) Noncardiac comorbidity increases preventable hospitalizations and mortality among Medicare beneficiaries with chronic heart failure. J Am Coll Cardiol 42:1226–1233
Groenveld HF, Januzzi JL, Damman K, van Wijngaarden J, Hillege HL, van Veldhuisen DJ et al (2008) Anemia and mortality in heart failure patients a systematic review and meta-analysis. J Am Coll Cardiol 52:818–827
Tang YD, Katz SD (2006) Anemia in chronic heart failure: prevalence, etiology, clinical correlates, and treatment options. Circulation 113:2454–2461
Kosiborod M, Curtis JP, Wang Y, Smith GL, Masoudi FA, Foody JM et al (2005) Anemia and outcomes in patients with heart failure: a study from the National Heart Care Project. Arch Intern Med 165:2237–2244
Young JB, Abraham WT, Albert NM, GattisStough W, Gheorghiade M, OPTIMIZE-HF Greenberg BH Investigators and Coordinators et al (2008) Relation of low hemoglobin and anemia to morbidity and mortality in patients hospitalized with heart failure (insight from the OPTIMIZE-HF registry). Am J Cardiol 101:223–230
Silva RP, Barbosa PH, Kimura OS, Sobrinho CR, Sousa Neto JD, Silva FA et al (2007) Prevalance of anemia and its association with cardio-renal syndrome. Int J Cardiol 120:232–236
Tavazzi L, Maggioni AP, Lucci D, Cacciatore G, Ansalone G, Oliva F, Porcu M, Italian survey on Acute Heart Failure Investigators (2006) Nationwide survey on acute heart failure in cardiology ward services in Italy. Eur Heart J 27:1207–1215
Van Buuren S, Oudshoorn CGM. MICE: Multivariate Imputation by Chained Equations. R package version 1.14. Available at: http://web.inter.nl.net/users/S.van.Buuren/mi/hmtl/mice.htm
Barnard J, Rubin DB (1999) Small sample degrees of freedom with multiple imputation. Biometrika 86:955–984
Adlbrecht C, Kommata S, Hülsmann M, Szekeres T, Bieglmayer C, Strunk G et al (2008) Chronic heart failure leads to an expanded plasma volume and pseudoanaemia, but does not lead to a reduction in the body’s red cell volume. Eur Heart J 29:2343–2350
Westenbrink BD, Visser FW, Voors AA, Smilde TD, Lipsic E, Navis G et al (2007) Anaemia in chronic heart failure is not only related to impaired renal perfusion and blunted erythropoietin production, but to fluid retention as well. Eur Heart J 28:166–171
Androne AS, Katz SD, Lund L, LaManca J, Hudaihed A, Hryniewicz K et al (2003) Hemodilution is common in patients with advanced heart failure. Circulation 107:226–229
Opasich C, Cazzola M, Scelsi L, De Feo S, Bosimini E, Lagioia R et al (2005) Blunted erythropoietin production and defective iron supply for erythropoiesis as major causes of anaemia in patients with chronic heart failure. Eur Heart J 26:2232–2237
van der Meer P, Lok DJ, Januzzi JL, de la Porte PW, Lipsic E, van Wijngaarden J et al (2008) Adequacy of endogenous erythropoietin levels and mortality in anaemic heart failure patients. Eur Heart J 29:1510–1515
Go AS, Yang J, Ackerson LM, Lepper K, Robbins S, Massie BM et al (2006) Hemoglobin level, chronic kidney disease, and the risks of death and hospitalization in adults with chronic heart failure: the Anemia in Chronic Heart Failure: Outcomes and Resource Utilization (ANCHOR) Study. Circulation 113:2713–2723
Culleton BF, Manns BJ, Zhang J, Tonelli M, Klarenbach S, Hemmelgarn BR (2006) Impact of anemia on hospitalization and mortality in older adults. Blood 107:3841–3846
Baggish AL, van Kimmenade R, Bayes-Genis A, Davis M, Lainchbury JG, Frampton C et al (2007) Hemoglobin and N-terminal pro-brain natriuretic peptide: Independent and synergistic predictors of mortality in patients with acute heart failure Results from the International Collaborative of NT-proBNP (ICON) Study. Clin Chim Acta 381:145–150
Maggioni AP, Opasich C, Anand I, Barlera S, Carbonieri E, Gonzini L, Tavazzi L, Latini R, Cohn J (2005) Anemia in patients with heart failure: prevalence and prognostic role in a controlled trial and in clinical practice. J Card Fail 11:91–98
Tang WH, Tong W, Jain A, Francis GS, Harris CM, Young JB (2008) Evaluation and long-term prognosis of new-onset, transient, and persistent anemia in ambulatory patients with chronic heart failure. J Am Coll Cardiol 51:569–576
Komajda M, Anker SD, Charlesworth A, Okonko D, Metra M, Di Lenarda A et al (2006) The impact of new onset anaemia on morbidity and mortality in chronic heart failure: results from COMET. Eur Heart J 27:1440–1446
Astor BC, Muntner P, Levin A, Eustace JA, Coresh J (2002) Association of kidney function with anemia: the Third National Health and Nutrition Examination Survey (1988–1994). Arch Intern Med 162:1401–1408
McFarlane SI, Chen SC, Whaley-Connell AT, Sowers JR, Vassalotti JA, Salifu MO et al, Kidney Early Evaluation Program Investigators (2008) Prevalence and associations of anemia of CKD: Kidney Early Evaluation Program (KEEP) and National Health and Nutrition Examination Survey (NHANES) 1999–2004. Am J Kidney Dis 51(4 Suppl 2):S46–S55
Latado AL, Passos LC, Darzé ES, Lopes AA (2006) Comparison of the effect of anemia on in-hospital mortality in patients with versus without preserved left ventricular ejection fraction. Am J Cardiol 98:1631–1634
Felker GM, Shaw LK, Stough WG, O’Connor CM (2006) Anemia in patients with heart failure and preserved systolic function. Am Heart J 151:457–462
Dunlay SM, Weston SA, Redfield MM, Killian JM, Roger VL (2008) Anemia and heart failure: a community study. Am J Med 121:726–732
O’Meara E, Clayton T, McEntegart MB, McMurray JJ, Lang CC, Roger SD, CHARM Committees, Investigators et al (2006) Clinical correlates and consequences of anemia in a broad spectrum of patients with heart failure: results of the Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) Program. Circulation 113:986–994
Chatterjee K, Massie B (2007) Systolic and diastolic heart failure: differences and similarities. J Card Fail 13:569–576
Yancy CW, Lopatin M, Stevenson LW, De Marco T, Fonarow GC, ADHERE Scientific Advisory Committee and Investigators (2006) Clinical presentation, management, and in-hospital outcomes of patients admitted with acute decompensated heart failure with preserved systolic function: a report from the Acute Decompensated Heart Failure National Registry (ADHERE) Database. J Am Coll Cardiol 47:76–84
Tarantini L, Cioffi G, Gonzini L, Oliva F, Lucci D, Di Tano G, Maggioni AP, Tavazzi L, on behalf of the Italian Acute Heart Failure Survey (2010) Evolution of renal function during and after an episode of cardiac decompensation: results from the Italian survey on acute heart failure. J Cardiovasc Med 11:234–243
Heywood JT, Fonarow GC, Costanzo MR, Mathur VS, Wigneswaran JR, Wynne J, ADHERE Scientific Advisory Committee and Investigators (2007) High prevalence of renal dysfunction and its impact on outcome in 118, 465 patients hospitalized with acute decompensated heart failure: a report from the ADHERE database. J Card Fail 13:422–430
Jie KE, Verhaar MC, Cramer MJ, van der Putten K, Gaillard CA, Doevendans PA et al (2006) Erythropoietin and the cardiorenal syndrome: cellular mechanisms on the cardiorenal connectors. Am J Physiol Renal Physiol 291:F932–F944
Kazory A, Ross EA (2009) Anemia: the point of convergence or divergence for kidney disease and heart failure? J Am Coll Cardiol 53:639–647
Ronco C, Haapio M, House AA, Anavekar N, Bellomo R (2008) Cardiorenal syndrome. J Am Coll Cardiol 52:1527–1539
Herzog CA, Muster HA, Li S, Collins AJ (2004) Impact of congestive heart failure, chronic kidney disease, and anemia on survival in the Medicare population. J Card Fail 10:467–472
Nash K, Hafeez A, Hou S (2002) Hospital-acquired renal insufficiency. Am J Kidney Dis 39:930–936
du Cheyron D, Parienti JJ, Fekih-Hassen M, Daubin C, Charbonneau P (2005) Impact of anemia on outcome in critically ill patients with severe acute renal failure. Intensive Care Med 31:1529–1536
Kovesdy CP, Trivedi BK, Kalantar-Zadeh K, Anderson JE (2006) Association of anemia with outcomes in men with moderate and severe chronic kidney disease. Kidney Int 69:560–564
Tehrani F, Dhesi P, Daneshvar D, Phan A, Rafique A, Siegel RJ et al (2009) Erythropoiesis stimulating agents in heart failure patients with anemia: a meta-analysis. Cardiovasc Drugs Ther 23:511–518
Anker SD, Comin Colet J, Filippatos G, Willenheimer R, Dickstein K, Drexler H et al, the FAIR-HF Trial Investigators (2009) Ferric carboxymaltose in patients with heart failure and iron deficiency. N Engl J Med 361:2436–2448
Acknowledgments
The study was partially supported by an unrestricted educational grant from Abbott Italy.
Conflict on interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
On behalf of Italian Survey on Acute Heart Failure Investigators.
The complete list of the Italian Survey on Acute Heart Failure Investigators has been already published as Appendix of ref 10.
Rights and permissions
About this article
Cite this article
Tarantini, L., Oliva, F., Cantoni, S. et al. Prevalence and prognostic role of anaemia in patients with acute heart failure and preserved or depressed ventricular function. Intern Emerg Med 8, 147–155 (2013). https://doi.org/10.1007/s11739-011-0601-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11739-011-0601-z