
Abstract
Summary
This study from southern India showed that yearly administration of zoledronic acid demonstrated significant improvement in BMD at lumbar spine following two doses and no decline in BMD at femoral neck or hip and trabecular bone score (TBS) in postmenopausal women.
Purpose
There is limited information available with regard to the impact of zoledronic acid treatment on bone mineral density (BMD) and trabecular bone score (TBS) in Indian postmenopausal women with osteoporosis. We studied the changes in BMD at femoral neck (FN), hip and lumbar spine (LS), and in TBS following yearly administration of zoledronic acid (ZA) in subjects with postmenopausal osteoporosis.
Material and methods
This was a prospective-retrospective study which included subjects on follow-up after administration of yearly zoledronic acid, over the past 6 years. Postmenopausal women with a T score of ≤ − 2.5 at any site, assessed by dual energy X-ray absorptiometry (DXA), were included.
Results
A total of 620 subjects had received ZA during the study period, 197 postmenopausal women were eligible, and follow-up data were available in 164 and 103 at 1st and 2nd follow-up yearly visits respectively. The mean (SD) age and BMI of the women were 63.2 (8.5) years and 25.6 (4.5) kg/m2 respectively. There was significant increment in LS BMD from baseline to the 1st and 2nd follow-up visits, respectively (mean (SD), 0.718 (0.116), 0.734 (0.104), 0.762 (0.127) g/cm2, p = 0.024). No decline in the BMD at FN and hip at first and second follow visit was found. The TBS scores (n = 90) on baseline and follow-up visits were 1.260 (±0.11), 1.256 (± 0.15), and 1.242 (± 0.17) (p value = 0.71).
Conclusion
Lumbar spine BMD showed significant improvement with zoledronic acid treatment. No decline was noted in femoral neck BMD and TBS with treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteoporosis is often a forerunner of fragility fractures, which are associated with a high morbidity and mortality [1].These fractures could largely be prevented by early recognition and appropriate management of osteoporosis. Although several therapeutic options for the treatment of osteoporosis are available today, parenteral bisphosphonates are a commonly used, relatively inexpensive, and a well-tolerated preferred option. Several clinical trials have proven the efficacy of yearly intravenous zoledronic acid, the most potent third-generation bisphosphonate, in patients with osteoporosis [2, 3]. However, these trials had limited representation of Asian ethnicities and the effectiveness of zoledronic acid is sparsely known in Indian postmenopausal women [4].
Moreover, individuals from countries like India are known to have a lower peak bone mass, higher prevalence of nutritional calcium and vitamin D deficiency, and more severe osteoporosis, which initiates at an earlier age, as compared with their western counterparts [5, 6]. This is further exemplified by the influence ethnicity specific databases can have on the interpretation of bone mineral density in different Asian ethnicities [7, 8]. Therefore, it is important to study the impact of bisphosphonates on bone health, specifically in this population, as it may not be similar to that in other women [9].
Furthermore, there is paucity of literature on the impact of zoledronate on trabecular bone score (TBS), a novel gray-scale texture measurement predicting the trabecular bone microarchitecture, based on the assessment of 2-D DXA images. A low TBS has shown to be an independent predictor of fractures, irrespective of BMD [10]. A study by Shin et al. showed a significant increase in TBS following zoledronate administration, during a 3-year follow-up study [11].
In this study, we explored the longitudinal changes on the BMD at different sites (femoral neck (FN), hip and lumbar spine (LS)) following yearly administration of zoledronic acid in Indian postmenopausal women. We also studied the serial changes in trabecular bone score following intravenous zoledronate. This study will provide regional data to suggest the expected impact of this widely used drug in the Indian population.
Material and methods
This single-center retrospective-prospective study was conducted in a 2858 bedded multi-specialty tertiary care center of southern India. Postmenopausal women were eligible for inclusion if they had a BMD T score of − 2.5 or less at the spine (L1–L4) or total hip or femoral neck with or without evidence of fragility fracture. We included those who were treated with yearly parenteral zoledronic acid for management of osteoporosis, between 1 January 2013 and 31 October 2018. Women with active cancer, other metabolic bone diseases, secondary causes of osteoporosis, deranged renal function tests, and hypercalcemia and those with history of prior therapy with either bisphosphonates, hormone replacement therapy, or teriparatide were excluded.
Medical records of eligible subjects were retrieved from computerized hospital information processing system (CHIPS) department. Data from baseline visit and subsequent follow-up visits were noted and subjected to analysis. Baseline data was collected for age, height, weight, body mass index (BMI), and menopausal age. Weight was recorded in kilogram using an electronic scale, and standing height was measured to the nearest centimeter with a stadiometer, with subjects wearing light indoor clothing without shoes.
Fasting (overnight for 8 h) venous blood samples were collected for the measurement of serum calcium (N 8.3–10.4 mg/dL), phosphorus (N 2.5–4.5 mg/dL), alkaline phosphatase (N 40–125 U/L), albumin (N 3.5–5.0 g/dL), creatinine (N 0.6–1.4 mg/dL), and 25-hydroxy vitamin D (N 30–75 ng/mL). Blood calcium, phosphate, albumin, creatinine, and alkaline phosphatase were measured using colorimetric method with Beckman Coulter (Beckman Coulter AU 5800). BMD was assessed with a Hologic DXA QDR 4500 Discovery A scanner at lumbar spine, total hip, and femoral neck. Daily quality control was performed with a phantom provided by the manufacturer, and machine was calibrated using a standard protocol.
TBS (L1–L4) measurements were performed using TBS iNsight Software version 3 (Med-Imaps, Bordeaux, France). It was retrospectively calculated as the mean of the individual measurements for vertebrae L1–L4 from the original DXA images that corresponded to the region in which the BMD was evaluated [12, 13]. The standard quality control procedures of these devices were followed.
As per our department protocol, subjects with vitamin D deficiency were optimally treated with oral cholecalciferol therapy prior to initiation of bisphosphonate. This was followed by replacement doses of cholecalciferol (1000–2000 IU/day) and supplemented with oral elemental calcium 500–1000 mg/day along with yearly zoledronic acid. Baseline data on prevalent fractures were noted from the patient records. Subjects who had two follow-up DXA scans were contacted telephonically, and information regarding incident fragility fractures was collected prospectively.
Statistical analyses were performed using SPSS v 16 software for Windows. Continuous variables were expressed as mean (SD). Paired Student t test and ANOVA were used to estimate the longitudinal changes in BMD. A p value of less than 0.05 was considered significant.
Results
A total of 620 patients had received zoledronic acid in the Department of Endocrinology during the study period. One hundred ninety-seven of them had received zoledronic acid as management of postmenopausal osteoporosis (31.7%). The mean age of the women was 63.2 (8.5) years. The mean BMI was 25.6 (4.5) kg/m2. The mean (SD) menopausal age of the women 46.8 (5.7) years. At baseline, 64 subjects had documented fractures. This included 43 subjects with documented vertebral fractures and 20 peripheral fragility fractures (including 6 subjects with hip fractures). The baseline serum calcium, phosphorus, albumin, corrected calcium, and creatinine were within the normal limits. The mean 25-hydroxyvitamin D levels were 31.7 (14.6) ng/mL; 19.5% of them had vitamin D deficiency (< 20 ng/mL) and 29.8% of them having levels between 20 and 30 ng/mL. The baseline clinical and biochemical characteristics of the study population are summarized in Table 1.
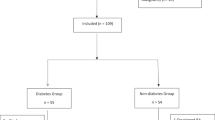
Among 197 subjects who received zoledronic acid, first follow-up BMD was available in 164 subjects. Although 132 had completed the second follow-up visit, second follow-up DXA scans could be retrieved for only 103 subjects (Fig. 1). The mean (SD) BMD (in g/cm2) in 103 subjects at lumbar spine was 0.718 (0.116), 0.734 (0.104), 0.762 (0.127) at baseline, first, and second follow-up DXA scans respectively. The increment was statistically significant between all measurement (p = 0.024). Similarly, the mean (SD) BMD (in g/cm2) in them at femoral neck and hip was 0.572 (0.087), 0.581 (0.081), 0.589 (0.077), and 0.642 (0.068), 0.648 (0.061), 0.655 (0.067) at baseline, first, and second follow-up, respectively. Although the change in BMD was not statistically significant, there was no further age-related decline in the BMD. On telephonic follow-up of 103 subjects, 84 were contactable and 8 subjects reported new onset peripheral fractures (one humerus fracture, two hip fractures, and five distal forearm fractures).

Diagram representing follow-up of study subjects
The TBS score was compared among those who had two follow-up scans available (n = 103), of which only 90 scans were evaluable. The mean (SD) TBS at baseline, first, and second follow-up was (n = 90) 1.260 (0.11), 1.256 (0.15), 1.242 (0.17) (p value = 0.71). The sequential TBS scores for other sites are summarized in Table 2. The mean (SD) serum total alkaline phosphatase (U/L) level was 87.7 (31.7), 80.1 (31.1), 72.4 (30.5) at baseline, first follow-up, second follow-up yearly visit. The decline observed in these visits was statistically significant (p = 0.008).
Discussion
This is the first data from southern India to study the longitudinal change in bone mineral density and trabecular bone score following yearly zoledronic acid infusion in postmenopausal osteoporosis. We found that there was a significant improvement in BMD at lumbar spine following two doses of zoledronic acid and no further decline in BMD at the femoral neck and hip. In addition, the expected age-related decline in TBS was not seen in subjects receiving zoledronic acid.
The ultimate goal in the treatment of osteoporosis is prevention of fragility fractures, and periodic BMD measurement by DXA scan is used in clinical practice to predict therapeutic response. Previous studies have confirmed the benefit of once-yearly zoledronic acid infusions in this setting. It has been demonstrated that zoledronic acid significantly reduces the risk of morphometric and clinical vertebral fracture, and increases total hip, femoral neck, and trochanter BMD [14, 15]. Our results showed a statistically significant improvement in BMD at lumbar spine between baseline, first, and second follow-up visits. At 2 years, there was a net increase in the BMD from baseline by 6.1% at and was comparable with a previous study by Huang et al. showing increments of up to 5.7% [16].
The BMD increase at total hip and femoral neck during follow-up, though not statistically significant, remained stable, and no age-related decline was seen. Unlike our study, Huang et al. reported a net increase in BMD at femoral neck by 3.36% over a follow-up period of 2 years.
In the current study, about only one-fifth of study subjects had vitamin D deficiency (< 20 ng/mL) and these individuals were adequately treated with vitamin D and calcium, prior to the initiation of bisphosphonate therapy. Vitamin D deficiency can lead to bone loss by inciting secondary hyperparathyroidism [17]. It is imperative to adequately replace calcium along with vitamin D, in deficient patients who are planned to receive bisphosphonates therapy for more than one reason. This may prevent severe symptomatic hypocalcemia in severe vitamin D–deficient patients and may also enhance the BMD accrual rate in these subjects [18]. In a study by Adami et al. [19], it was found that the odds of incident fracture in subjects with vitamin D deficiency was 1.7 times higher as compared with those who are vitamin D replete, thus emphasizing the importance of its correction prior to initiation of bisphosphonate therapy.
In our study there was no significant decline in the TBS on follow-up after administration of zoledronic acid. This is the first Indian study to demonstrate the effect of bisphosphonates on TBS in the Indian population, and limited literature is available on this subject in other ethnicities. In a study from south Korea, there was a marginal increase in TBS of postmenopausal women; however, several different types of oral and intravenous bisphosphonates were used in this study [11]. At present, there is no consensus on how to predict response to therapy based on TBS in postmenopausal women and further follow-up to determine its utility in predicting fragility fractures would throw more light on its use. There was also significant decline in the levels of serum total alkaline phosphatase, as expected due to the action of zoledronic acid on reducing the net bone resorption [20].
This is the first study assessing the real-time effectiveness of zoledronic acid in clinical practice from the Indian subcontinent; however, there were several limitations in this study. Being a retrospective study, it comes with the disadvantage of selection bias. Incidence of new onset fragility fracture especially vertebral fracture and the bone turnover markers which gauge the antiresorptive effectiveness of zoledronic acid were not available. In addition, serum parathormone levels were not available in the study subjects.
In conclusion, yearly zoledronic acid infusion for postmenopausal osteoporosis causes a significant increase in the BMD at the lumbar spine and stable BMD at total hip or femoral neck in Indian women. It also prevents the expected age-related decline in TBS. However, long-term efficacy and safety data in the Indian population need to be assessed with prospective trials in future.
References
Dhanwal DK, Siwach R, Dixit V, Mithal A, Jameson K, Cooper C (2013) Incidence of hip fracture in Rohtak district, North India. Arch Osteoporos 8:135
Black DM, Delmas PD, Eastell R, Reid IR, Boonen S, Cauley JA, Cosman F, Lakatos P, Leung PC, Man Z, Mautalen C, Mesenbrink P, Hu H, Caminis J, Tong K, Rosario-Jansen T, Krasnow J, Hue TF, Sellmeyer D, Eriksen EF, Cummings SR, HORIZON Pivotal Fracture Trial (2007) Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med 356(18):1809–1822
Higgs R (2010) Osteoporosis: zoledronic acid for osteoporosis treatment--a matter of time. Nat Rev Rheumatol 6(7):382
Khosla S, Bilezikian JP, Dempster DW, Lewiecki EM, Miller PD, Neer RM, Recker RR, Shane E, Shoback D, Potts JT (2012) Benefits and risks of bisphosphonate therapy for osteoporosis. J Clin Endocrinol Metab 97(7):2272–2282
Handa R (2004) Management of osteoporosis: the Indian perspective. Clin Calcium 14(9):100–105
Mithal A, Kaur P (2012) Osteoporosis in Asia: a call to action. Curr Osteoporos Rep 10(4):245–247
Shetty S, Kapoor N, Naik D, Asha HS, Thomas N, Paul TV (2014) The impact of the Hologic vs the ICMR database in diagnosis of osteoporosis among south Indian subjects. Clin Endocrinol 81(4):519–522
Cherian KE, Kapoor N, Asha HS, Thomas N, Paul TV (2018) Influence of different reference databases on categorization of bone mineral density: a study on rural postmenopausal women from southern India. Indian J Endocrinol Metab 22(5):579–583
Mithal A, Bansal B, Kyer CS, Ebeling P (2014) The Asia-Pacific regional audit-epidemiology, costs, and burden of osteoporosis in India 2013: a report of International Osteoporosis Foundation. Indian J Endocrinol Metab 18(4):449–454
Hans D, Barthe N, Boutroy S, Pothuaud L, Winzenrieth R, Krieg M-A (2011) Correlations between trabecular bone score, measured using anteroposterior dual-energy X-ray absorptiometry acquisition, and 3-dimensional parameters of bone microarchitecture: an experimental study on human cadaver vertebrae. J Clin Densitom Off J Int Soc Clin Densitom 14(3):302–312
Shin M-S, Cho E-H, Kim HY (2017) Longitudinal change in trabecular bone score during and after treatment of osteoporosis in postmenopausal Korean women. J Bone Metab 24(2):117–124
Dufour R, Winzenrieth R, Heraud A, Hans D, Mehsen N (2013) Generation and validation of a normative, age-specific reference curve for lumbar spine trabecular bone score (TBS) in French women. Osteoporos Int J Establ Result Coop Eur Found Osteoporos Natl Osteoporos Found USA 24(11):2837–2846
Silva BC, Leslie WD, Resch H, Lamy O, Lesnyak O, Binkley N, McCloskey EV, Kanis JA, Bilezikian JP (2014) Trabecular bone score: a noninvasive analytical method based upon the DXA image. J Bone Miner Res Off J Am Soc Bone Miner Res 29(3):518–530
Black DM, Reid IR, Boonen S, Bucci-Rechtweg C, Cauley JA, Cosman F, Cummings SR, Hue TF, Lippuner K, Lakatos P, Leung PC, Man Z, Martinez RLM, Tan M, Ruzycky ME, Su G, Eastell R (2012) The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: a randomized extension to the HORIZON-Pivotal Fracture Trial (PFT). J Bone Miner Res Off J Am Soc Bone Miner Res 27(2):243–254
Black DM, Reid IR, Cauley JA, Cosman F, Leung PC, Lakatos P, Lippuner K, Cummings SR, Hue TF, Mukhopadhyay A, Tan M, Aftring RP, Eastell R (2015) The effect of 6 versus 9 years of zoledronic acid treatment in osteoporosis: a randomized second extension to the HORIZON-Pivotal Fracture Trial (PFT). J Bone Miner Res Off J Am Soc Bone Miner Res 30(5):934–944
Huang S, Lin H, Zhu X, Chen X, Fan L, Liu C (2014) Zoledronic acid increases bone mineral density and improves health-related quality of life over two years of treatment in Chinese women with postmenopausal osteoporosis. Endokrynol Pol 65(2):96–104
Lips P, van Schoor NM (2011) The effect of vitamin D on bone and osteoporosis. Best Pract Res Clin Endocrinol Metab 25(4):585–591
Ishijima M, Sakamoto Y, Yamanaka M, Tokita A, Kitahara K, Kaneko H, Kurosawa H (2009) Minimum required vitamin D level for optimal increase in bone mineral density with alendronate treatment in osteoporotic women. Calcif Tissue Int 85(5):398–404
Adami S, Giannini S, Bianchi G, Sinigaglia L, Di Munno O, Fiore CE et al (2009) Vitamin D status and response to treatment in post-menopausal osteoporosis. Osteoporos Int J Establ Result Coop Eur Found Osteoporos Natl Osteoporos Found USA. 20(2):239–244
Mukaiyama K, Kamimura M, Uchiyama S, Ikegami S, Nakamura Y, Kato H (2015) Elevation of serum alkaline phosphatase (ALP) level in postmenopausal women is caused by high bone turnover. Aging Clin Exp Res 27(4):413–418
Acknowledgments
We would like to acknowledge Mr. Kali Periyasamy for his contribution in DXA report archival.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sooragonda, B., Cherian, K.E., Jebasingh, F.K. et al. Longitudinal changes in bone mineral density and trabecular bone score following yearly zoledronic acid infusion in postmenopausal osteoporosis—a retrospective-prospective study from southern India. Arch Osteoporos 14, 79 (2019). https://doi.org/10.1007/s11657-019-0630-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-019-0630-1