
Abstract
Background
Regularity and continuity of general practitioner (GP) contacts are associated with reduced hospitalisation. Opportunities for improved medication management are cited as a potential cause.
Objective
Determine associations between continuity and regularity of primary care and statin use amongst individuals at risk of cardiovascular disease (CVD) outcomes.
Design
Observational cohort study using self-report and administrative data from 267,153 participants of the Sax Institute’s 45 and Up Study conducted in New South Wales, Australia. from 2006 to 2009. Medicare Benefits Schedule (MBS) and Pharmaceutical Benefits Scheme (PBS) data, from Services Australia, were linked to survey, hospital and death data by the NSW Centre for Health Record Linkage.
Participants
The 45 and Up Study participants at risk of CVD outcomes based on self-report and administrative data, divided into existing users and potential users based on dispensing records through the exposure period.
Main Measures
The Continuity of Care index (COC), measuring whether patients see the same GP, and an index assessing whether GP visits are on a regular basis, measured from July 2011 to June 2012. Amongst potential users, statin initiation from July 2012 to June 2013 was assessed using logistic regression; amongst existing users, adherence was assessed from July 2012 to June 2015 using Cox regression (non-adherence being 30 days without statins).
Key Results
Amongst 29,420 potential users, the most regular quintile had 1.22 times the odds of initiating statin (95%CI 1.11–1.34), while the high continuity group had an odds ratio of 1.12 (95%CI 1.02–1.24). Amongst 30,408 existing users, the most regular quintile had 0.82 the hazard of non-adherence (95%CI 0.78–0.87); the high continuity group had a hazard ratio of 0.89 (95%CI 0.84–0.94).
Conclusions
Regularity and continuity of care impact on medication management. It is possible that this mediates impacts on hospitalisation. Where there is a risk of unobserved confounding, potential causal pathways should be investigated.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
Within primary care, continuity of care can be defined as a relationship between a practitioner and patient extending beyond specific episodes of illness or disease, implying a sense of affiliation.1 Definitions describe continuity as including multiple dimensions, for example the 1975 definition by Hennen2 which outlined chronological, geographical, interdisciplinary and interpersonal continuity. Continuity of care has been demonstrated to be associated with reduced hospitalisations,3,4,5,6,7,8 emergency department use,6, 7, 9 mortality3 and healthcare costs.3, 4, 6, 8 Although there are many indices for measuring continuity of care,10, 11 most measure whether a patient consistently visits the same general practitioner (GP) or switches between providers. In recognition of the broader definitions of the concept, our research group has assessed continuity by measuring the regularity of GP contact, as distinct from the frequency of contact. In this context, frequency refers simply to the number of GP contacts a patient may have through a measurement period, while regularity refers to the spread of these visits over time. Regular GP contact may reflect a planned and proactive approach to care, while irregular contact (a period without any GP contact followed by repeated visits in a short timeframe) may reflect more reactive care. Regular GP contact has been demonstrated to be associated with improved outcomes, including reduced hospital use in certain chronic conditions.12, 13
Researchers assessing these relationships generally describe potential causal mechanisms via which GP contact may affect hospitalisation. These include an improved knowledge of the patient’s health by the GP, an improved ability to detect and respond to problems and an improved patient-provider communication.3, 5, 7, 14 Many also suggest that where continuity of care exists, patient adherence with treatment may improve,3,4,5,6,7, 15,16,17,18,19,20,21 resulting from increased trust in the doctor.2, 5,6,7, 9, 22 In comparison to the volume of research assessing downstream outcomes of hospitalisation and mortality, there is little research assessing intermediate outcomes such as the medical management of conditions. Understanding the effects of GP contact on these outcomes is an important step to determining potential causal pathways, and hence suitability of these exposures as intervention targets.
In assessing medical management, statins present a suitable area of study, on account of their impact on hospitalisation,23,24,25,26 evidence that many people at high risk of cardiovascular events do not initiate statins through primary care,27, 28 and evidence indicating that adherence is often poor amongst those using statins.29,30,31 Improved statin use therefore presents a pathway via which regularity/continuity of GP contact may influence hospitalisation. One previous study has assessed associations between continuity of care32 (i.e. repeat visits to the same provider) and statin adherence amongst existing statin users, finding higher continuity to be associated with improved adherence. Gaps remain in the literature concerning the impact of continuity of care on the initiation of new statin therapy amongst those at risk. Additionally, the effect of regularity of GP contact on statin use has not been investigated; hence, there is potential for an improved understanding of the patterns of GP contact on statin outcomes.
The objective of this project was to determine associations between regularity/continuity of GP contact and statin initiation and adherence, amongst a cohort of patients at high risk of cardiovascular disease (CVD) or who had a prior history of CVD over a 3-year period of follow-up.
METHODS
Data
This study used the Sax Institute’s 45 and Up Study,33 based in the population of the state of New South Wales (NSW), Australia. Prospective participants were randomly sampled from the Services Australia (formerly the Australian Government Department of Human Services) enrolment database, which provides near-complete population coverage. People 80+ years of age and residents of rural and remote areas were oversampled. A total of 267,153 participants joined the study by completing a baseline questionnaire (between January 2006 and December 2009) and giving signed consent for follow-up and linkage of their information to routine health databases. About 18% of invitees participated and participants included about 11% of the NSW population aged 45 years and over.
This study used the Study baseline questionnaire (https://www.saxinstitute.org.au/our-work/45-up-study/) linked to (i) the NSW Admitted Patient Data Collection (APDC), covering all public and private hospital discharges (2005–2017); (ii) the Pharmaceutical Benefits Scheme (PBS) capturing dispensed subsidised prescription medicines (2005–2017); (iii) the Medicare Benefits Schedule (MBS) covering all claims for medical and diagnostic services through Medicare, Australia’s universal health insurance scheme (2005–2017); and (iv) the NSW Register of Births Deaths and Marriages (RBDM) (2006–2017). Linkage of APDC and RBDM to the survey data was conducted by the NSW Centre for Health Record Linkage (http://www.cherel.org.au). MBS and PBS data were supplied by Services Australia and linked by the Sax Institute using a unique identifier provided by Services Australia. Quality assurance of the data linkage method showed false-positive and false-negative rates of <0.5 and <0.1%, respectively.34 CHeReL performs linkage using probabilistic matching complemented by a clerical review of uncertain matches, with reviews of random samples for quality assurance.
Approvals were provided by the Curtin University Human Research Ethics Committee and the NSW Population and Health Services Research Ethics Committee. The 45 and Up Study was approved by the University of NSW Human Research Ethics Committee.
Cohort
Our study included individuals aged 55–75 at risk of CVD as of July 2011. It was selected following Liu et al.35 with modifications.
The cohort consisted of two groups: those at high risk of CVD (primary prevention group) and those with a history of CVD. Those at high risk of CVD were selected using self-reported age, sex, diabetes status, smoking status, hypertension and high cholesterol, based on a threshold equivalent to a risk of CVD over 5 years of >15% (details in Appendix 1). Those with a history of CVD were captured from (i) hospitalisation with a diagnosis of ischaemic heart disease (IHD), transient ischaemic attack (TIA), ischaemic stroke, atrial fibrillation or other CVD, or a procedure pathognomic of IHD; (ii) MBS items pathognomic of IHD or ischaemic stroke; (iii) PBS records for drugs pathognomic of IHD; or (iv) self-reported heart attack/angina/stroke or self-reported operation for heart disease or TIA (codes in Appendix 1).
The cohort was further divided into two sub-cohorts analysed separately: those taking statins during the exposure period, for whom adherence was assessed, and those who had no history of statin use, for whom the outcome was statin initiation. These are called ‘existing users’ and ‘potential users’, respectively.
Exclusions were as follows: apparent linkage errors, potential users who died during follow-up, anyone who died prior to the end of the exposure period, those with fewer than three GP contacts during the exposure period as regularity and continuity could not be calculated and those who received statin medication during the pre-exposure period but not the exposure period as categorisation of their usage is unclear. A flow chart is included in Appendix 2.
Design
Figure 1 presents information assessed in the pre-exposure (July 2006–June 2011), exposure (July 2011–June 2012) and follow-up (July 2012–June 2015) periods.

Study time period and main measurements. Measurement of exposure and outcome variables underlined.
Exposure Variables
Exposures were regularity and continuity of GP contact. GP contact was captured based on MBS claims for ‘attendances by General Practitioners.’36 Regularity refers to the distribution of GP contacts over time, as distinct from the frequency (number) of contacts, with regularly spaced visits assumed to indicate planned, proactive care. This was captured using our Modified Regularity Index37, based on the variation in the number of days between GP contacts. For each GP visit, the number of days since the prior visit is counted, and the coefficient of variation in this number of days calculated. An index (R) is calculated using the formula R=1/1+(coefficient of variation (days between visits)). This ranges from 0 to 1 (1 being most regular) and is grouped into quintiles based on the score’s distribution within each cohort.
Continuity measures assess whether a patient is consistently seeing the same GP, or switching between providers. Continuity was measured using the Continuity of Care (COC) index38 which assesses the dispersion of visits across providers:
where N is the total number of GP visits, nj the number of visits to GP j; j, a given GP; and M, the number of GPs. This formula results in a score ranging from 0 to 1. For analysis, patients are often categorised to aid interpretation though there are no universally accepted cut-offs for categorisation;3, 7 in this study, patients were allocated to four groups: low (index range 0–0.49), moderate (0.5–0.74), high (0.75–0.99) and perfect (1) continuity.
The frequency (count) of GP contacts within the exposure year was also calculated.
Outcomes
Two outcomes were defined. The first was statin initiation, i.e. any statin dispensed during the follow-up period, assessed amongst potential users.
The second was time to non-adherence amongst existing users, typically defined as occurring where patient records indicate a given number of days without statins in supply.39,40,41 Patients were non-adherent if they spent 30 consecutive days without statin supply during follow-up, which in Australia reflects one dispensing being missed. The ‘failure’ date was the first day of this 30-day period. Days in hospital were removed, as the hospital pharmacy would supply patients at these times. Where a packet was dispensed, early overlapping days were carried forward.42 Other common measures of adherence, for example the Medication Possession Ratio, do not support the use of time-to-event analyses which was the preferred method for the current study.
Study Period
As displayed in Figure 1, exposures were measured through the 2011/2012 financial year. The statin initiation outcome was measured through the 2012/2013 financial year, i.e. for the 12 months to 30 June 2013. Time to non-adherence was measured from the start of the 2012/2013 financial year through to the end of the 2014/2015 financial year, i.e. for 36 months, and censored by death or study end.
The administrative data covered 5 years prior to the exposure period to measure comorbidity indicators and capture statin dispensing prior to exposure, ensuring potential users were correctly identified.
Covariates
The 45 and Up Study data includes self-report information on a range of factors including socio-demographics, health conditions and family history, limitations, self-rated health and quality of life and behaviours such as smoking and exercise.33 Comorbidity was assessed based on PBS data using the RxRisk indicator43 and additionally assessed via inpatient diagnoses using the Multipurpose Australian Comorbidity Scoring System (MACSS),44 through the pre-exposure period. For existing users, information on the first statin dispensed during the exposure period was derived including the dose (low, medium or high45) and prescriber (GP or other). A variable stating whether an individual belonged to the group at high risk or the group with a history of CVD was used as a covariate. Socioeconomic status and service accessibility were based on postcode using the Socioeconomic Index for Areas (SEIFA) Index of Relative Socio-economic Disadvantage46 and the Accessibility/Remoteness Index of Australia (ARIA),47 respectively. Missing data on categorical variables were given values to prevent data loss.
Analysis
Multivariable logistic regression assessed statin initiation amongst potential users. Multivariable Cox regression assessed time to non-adherence amongst existing users.
In each case, outcomes were regressed on regularity, continuity, frequency and covariates selected via forward stepwise selection. Covariates were selected based on their impact on associations between GP contact and statin outcomes. Models were run in which outcomes were regressed on regularity, continuity and frequency and then compared to models where each individual candidate covariate was included. Covariates were ranked based on how they affected coefficients for the regularity variable, from the largest to smallest change. Covariates were then added iteratively and kept if they improved model fit according to Bayes Information Criterion (BIC) and discarded; otherwise, the model was final when no further additions improved BIC.
Proportionality of hazards was tested using a Cox model including interactions between all independent variables and time; significant interactions indicated non-proportionality.48 As large sample sizes can make inconsequential violations significant, proportionality was also assessed by examining graphs of the scaled Schoenfeld residuals, with a zero slope indicating proportionality.48 Where proportionality was violated, problematic variables were included as stratifying variables rather than covariates.48 Model fit was assessed by examining the Cox-Snell residuals.
Two sensitivity analyses were performed. Firstly, the model assessing statin initiation was repeated with a 2-year follow-up, rather than 1 year. Secondly, adherence was assessed with ‘failure’ defined by 60 rather than 30 days without statin supply.
Stata version 15 was used49 with a significance level of α=0.05 for all analyses.
RESULTS
Cohort Description
The cohort of potential users (without statin dispensed during or prior to the exposure period) included 29,420 individuals and there were 30,408 existing users (with medication dispensed during the exposure period).
Cohort characteristics are described in Table 1. In line with the higher risk of CVD in males, the cohort had a majority of men: potential users 73.4% and existing users 63.4%. Existing users were slightly older, with the largest group being those aged 65–70 (30.2%) compared to 60–65 (27.6%) for potential users. Amongst existing users, 40.1% described their health as ‘good,’ while amongst potential users there was an even split between those reporting good (36.4%) and very good (36.3%) health. The majority were ex-smokers (56.3% of potential users and 51.0% of existing users). Amongst potential users, 70.1% were at high risk of CVD (i.e. where statins, if used, would represent primary prevention) while the cohort of existing users was equally split between those at high risk (49.9%) and those with a history of previous CVD (50.1%). In terms of outcomes, 25.7% of potential users initiated statins during follow-up, while 53.8% of existing users recorded a failure during follow-up, with the remainder censored by death (3.0%) or study end (43.2%).
Table 2 compares cohort members to those excluded due to either <3 GP contacts (n=8325) or other reasons (mainly lower CVD risk, n=198,094). Those with <3 contacts were more often male, had better self-rated health and lived in areas of lower disadvantage. In this group, potential statin users were less likely to initiate than cohort members (9.0% vs 25.7%) and existing users were more often non-adherent (58.5% vs 41.1%). Those excluded for other reasons, compared to cohort members, were more likely female, younger, self-reported better health and smoked less.
Initiation amongst Potential Statin Users
Amongst statin potential users, higher continuity and regularity were associated with increased odds of statin dispensing during follow-up (Table 3). After adjustment, the most regular quintile had 1.22 times the odds of commencing on a statin medication compared with least regular (95% CI 1.11–1.34). High provider continuity was associated with 1.12 times the odds of statin initiation compared to low continuity (95% CI 1.02–1.24), though the perfect continuity group reported a non-significant odds ratio of 1.07 (95% CI 0.99–1.15). Several influential covariates were included resulting from the stepwise selection. These included the RxRisk index, the presence of several specific comorbidities and one demographic (language spoken at home).
Adherence amongst Existing Statin Users
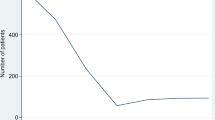
Figure 2 displays the cumulative hazard of non-adherence. A brief increase in hazard appears after 460 days, coinciding with a documentary critical of statins airing on television in Australia, and known to have influenced usage.50

Line chart representing the cumulative proportion of cohort members failing to adhere to statin therapy according to dispensing records, over time. Day 0 indicates the first day of follow-up, the vertical line indicates the date of a documentary critical of statins airing in Australia.
Violations of proportionality were observed for one level of regularity, age, prescriber, language spoken at home and one level of socio-economic status (results not shown). Therefore, in the final model, these covariates were included as stratifying variables rather than predictors. Regularity was retained as a predictor as coefficients were required for exposure variables. The plot of scaled Schoenfeld residuals displayed zero slopes for each level of regularity (see Appendix 3), suggesting that violations of proportionality were not practically meaningful. Cox-Snell residuals indicated that the model fit was good (Appendix 3).
Higher regularity/continuity was associated with a reduced hazard of non-adherence amongst existing users as displayed in Table 4. The most regular quintile had a hazard ratio of 0.82 (95% CI 0.78–0.87) compared to the least regular (i.e. a 16% reduction in likelihood of non-adherence). The perfect continuity group had a hazard ratio of 0.90 (95% CI 0.86–0.94) compared to the low continuity group. As with the model of statin initiation, the RxRisk index was included as a covariate along with certain comorbidities and demographics, though the specific conditions and demographics differed between models.
Sensitivity analyses suggested that findings were robust. When a 60-day period without supply was used to define non-adherence (rather than 30 days), a slight increase in the hazard rates for regularity and continuity was observed (Appendix 3). When statin initiation was assessed with a 2-year rather than 1-year follow-up, coefficients on the regularity variable decreased by about 20–30%, while coefficients on the continuity variable changed by 20–50% (Appendix 3).
DISCUSSION
Higher continuity and regularity of GP contact were associated with a higher likelihood of statin initiation amongst people at risk of CVD outcomes, and with improved adherence after initiation. This highlights the importance of ongoing relationships between GPs and at-risk patients. Policies which interfere with such relationships therefore have implications for the quality of preventive care received. In recent years, policies such as compulsory patient co-payments for GP visits have been proposed in Australia with discussion on the potential impact of such policies on preventive care.51 Meanwhile, a trend towards larger practice sizes52 and the impacts of this for provider continuity53 has implications for the patient-provider relationship.
Much work assesses relationships between GP contact and hospitalisation outcomes, and researchers have hypothesised that associations observed between these results from improved medical management. While the current observational work cannot establish causation, it does suggest that medication management is a plausible mechanism by which continuity/regularity may influence hospitalisation. As previous studies involve health service use as both exposure (continuity) and outcome (hospitalisation) variables, the risk of confounding by unobserved patient factors is high and work to better understand the plausibility of causation is worthwhile. While an association between statin adherence and continuity has previously been reported,32 this study additionally demonstrates an association with the initiation of statins amongst those at high risk of cardiovascular disease. Given that previous primary care studies have reported that only a minority of patients at high risk of cardiovascular disease are initiated on statins,27, 28 evidence to improve the understanding of factors contributing to initiation, in addition to understanding adherence amongst existing users, is valuable. This work also provides evidence regarding the impact of patterns of GP contact beyond the commonly used provider continuity measures, by additionally assessing the regularity of contacts. This provides a more comprehensive understanding of patterns of GP contact on statin use and potential downstream outcomes.
To some extent, a relationship between GP contact and statin adherence is self-evident, as a GP visit must occur to receive a prescription. However, statin prescriptions are generally provided with five monthly ‘repeats’ in Australia. A single prescription therefore can provide for a 6-month supply, meaning that adherence can be achieved with only two GP visits per year. As this analysis is restricted to people with ≥3 GP contacts, all cohort members have the potential to remain compliant; furthermore, analyses are adjusted for the number of GP contacts.
In Australia, GPs perform most prescribing, in particular for common medications such as statins, though in some cases, specialists may have a larger role in prescribing and condition management. Australia’s universal public insurance system, Medicare, reimburses GPs on a fee-for-service basis (though GPs may charge additional out-of-pocket fees)54 and medications are subsidised via the PBS,55 with small co-payments required. Patients in Australia are free to choose their GP and may switch at any time. In countries with different registration systems, different prescribing practices or where different financial barriers exist, the associations reported here may differ.
Strengths
A strength of this study is the comprehensiveness of the data available. The combination of self-reported and administrative collections provides information on a range of patient demographics, behaviours, health status and use of health services, reducing the likelihood of omitted variable bias.
Limitations
We did not have access to a practice identifier. It is unclear if patients with low continuity visited different GPs at the same practice (i.e. where patient records would still be available), or visited different practices, and how continuity of practice may differ from the continuity of GP. Unobserved patient characteristics are also a potential issue. Although the survey captured information on a range of characteristics, there are likely factors which are difficult for a survey to fully capture such as participants’ personal characteristics, family dynamics which may influence the use of services, and so on.
Reasons for statin cessation were unknown. Statin therapy may be stopped for clinical reasons such as adverse events, in which case people may have been incorrectly categorised as non-adherent. Symptoms of intolerance may occur in approximately 20% of statin users, but may usually be resolved with dose reduction or switching.56 Where these approaches are used, patients would remain adherent in these analyses, so this is unlikely to impact findings.
The participation rate of the 45 and Up Study was approximately 18%.33 As a result, the study population may not be representative of the broader community. However, a previous validation study has suggested that even with this low response rate, exposure-outcome estimates derived in this cohort may remain generalizable, based on comparisons to relationships derived from a comparable cohort with a higher response rate.57
This study ended in 2015, and it is possible that the relationships observed have changed since. However, analysing a later period would increase the risk of misclassification bias due to participants’ status on baseline survey variables changing; hence, the time period used was considered suitable to balance currency of findings against the risk of bias.
Finally, this analysis is restricted to those with at least 3 visits per year. The analysis suggested that those with fewer than 3 visits per year differed from the study cohort both on baseline characteristics and on statin use outcomes; findings here are not meaningful in relation to this excluded group.
Conclusion
Regularity and continuity of care are associated with improved medication management, which offers a plausible pathway for continuity/regularity of care to influence hospitalisation. Future research could explore mechanisms of action by investigating other measures of patient health, such as biomedical markers captured in pathology tests. Future research could also assess the impact of comorbid conditions on relationships observed.
References
Haggerty JL, Reid RJ, Freeman GK, Starfield BH, Adair CE, McKendry R. Continuity of care: a multidisciplinary review. BMJ. 2003;327(7425):1219-21.
Hennen BK. Continuity of Care in Family Practice, Part 1: Dimensions of Continuity. Journal of Family Practice. 1975;2(5):371-2.
Hong JS, Kang HC. Continuity of ambulatory care and health outcomes in adult patients with type 2 diabetes in Korea. Health Policy. 2013;109(2):158-65.
Romaire MA, Haber SG, Wensky SG, McCall N. Primary care and specialty providers: an assessment of continuity of care, utilization, and expenditures. Medical Care. 2014;52(12):1042-9.
Barker I, Steventon A, Deeny SR. Association between continuity of care in general practice and hospital admissions for ambulatory care sensitive conditions: cross sectional study of routinely collected, person level data. BMJ. 2017;356(j84).
Chen CC, Chen SH. Better continuity of care reduces costs for diabetic patients. American Journal of Managed Care. 2011;17(6):420-7.
Katz DA, McCoy KD, Vaughan-Sarrazin V. Does Greater Continuity of Veterans Administration Primary Care Reduce Emergency Department Visits and Hospitalization in Older Veterans? Journal of the American Geriatrics Society. 2015;63(12):2510-8.
Bazemore A, Petterson S, Peterson LE, Bruno R, Chung Y, Phillips RLJ. Higher Primary Care Physician Continuity is Associated With Lower Costs and Hospitalizations. Annals of Family Medicine. 2018;16(6):492-7.
Gill GM, Mainous AG R, Nsereko M. The effect of continuity of care on emergency department use. Archives of Family Medicine. 2000;7(4):333-8.
Jee SH, Cabana MD. Indices for continuity of care: a systematic review of the literature. Medical Care Research and Review. 2006;63(2):158-88.
Saultz JW. Defining and Measuring Interpersonal Continuity of Care. Annals of Family Medicine. 2003;1(3):134-43.
Einarsdottir K, Preen DB, Emery JD, Kelman C, Holman CDJ. Regular Primary Care Lowers Hospitalisation Risk and Mortality in Seniors with Chronic Respiratory Diseases. Journal of General Internal Medicine. 2010;25(8):766-73.
Moorin RE, Youens D, Preen DB, Harris M, Wright CM. Association between continuity of provider-adjusted regularity of general practitioner contact and unplanned diabetes-related hospitalisation: a data linkage study in New South Wales, Australia, using the 45 and Up Study cohort. BMJ Open. 2019;9(6):e027158.
Hansen MF. Continuity of Care in Family Practice. Part 3: Measurement and Evaluation of Continuity of Care. The Journal of Family Practice. 1975;2(6):439-44.
Burge F, Lawson B, Johnston G. Family Physician Continuity of Care and Emergency Department Use in End-of-Life Cancer Care. Medical care. 2003;41(8):992-1001.
Christakis DA, Wright JA, Koepsell TD, Emerson S, Connell FA. Is Greater Continuity of Care Associated With Less Emergency Department Utilization? Pediatrics. 1999;103(4):738-42.
Chu HY, Chen CC, Cheng SH. Continuity of Care, Potentially Inappropriate Medication, and Health Care Outcomes Among the Elderly: Evidence From a Longitudinal Analysis in Taiwan. Medical Care. 2012;50(11):1002-9.
Franklin B. The Impact of Continuity of Care on A1c Levels in Adult Type 2 Diabetic Patients: A Review of the Literature. The Journal for Nurse Practitioners. 2014;10(7):486-92.
Menec VH, Sirski M, Attawar D, Katz A. Does continuity of care with a family physician reduce hospitalizations among older adults? Journal of Health Services Research and Policy. 2006;11(4):196-201.
Steinwachs DM. Measuring Provider Continuity in Ambulatory Care: An Assessment of Alternative Approaches. Medical Care. 1979;17(6):551-65.
van Walraven C, Oake N, Jennings A, Forster AJ. The association between continuity of care and outcomes: a systematic and critical review. Journal of Evaluation in Clinical Practice. 2010;16(5):947-56.
Gill GM, Mainous AG R. The Role of Provider Continuity in Preventing Hospitalizations. Archives of Family Medicine. 1998;7(4):352-7.
Aubert RE, Yao J, Xia F, Garavaglia SB. Is There a Relationship Between Early Statin Compliance and a Reduction in Healthcare Utilization? The American Journal of Managed Care. 2010;16(6):459-66.
Degli Esposti L, Saragoni S, Batacchi P, Benemei S, Geppetti P, Sturani A, et al. Adherence to Statin Treatment and Health Outcomes in an Italian Cohort of Newly Treated Patients: Results From an Administrative Database Analysis. Clinical Therapeutics. 2012;34(1):190-9.
Scirica BM, Morrow DA, Cannon CP, Ray KK, Sabatine MS, Jarolim P, et al. Intensive Statin Therapy and the Risk of Hospitalization for Heart Failure After an Acute Coronary Syndrome in the PROVE IT-TIMI 22 Study. Journal of the American College of Cardiology. 2006;47(11):2326-31.
Eilat-Tsanani S, Mor E, Schonmann Y. Statin Use Over 65 Years of Age and All-Cause Mortality: A 10-Year Follow-Up of 19 518 People. Journal of the American Geriatrics Society. 2019;67(10):2038-44.
Robinson T, Jackson, R., Wells, S., Kerr, A., Marshall, R. An observational study of how clinicians use cardiovascular risk assessment to inform statin prescribing decisions. The New Zealand Medical Journal. 2017;130(1463):28-38.
Finnikin S, Ryan, R., Marshall, T. Statin initiations and QRISK2 scoring in UK general practice: a THIN database study. British Journal of General Practice. 2017;67(665):e881-e7.
Romanelli RJ, Segal JB. Predictors of Statin Compliance after Switching from Branded to Generic Agents among Managed-Care Beneficiaries. Journal of General Internal Medicine. 2014;29(10):1372-8.
Wawruch M, Wimmer G, Murin J, Paduchova M, Tesar T, Hlinkova L, et al. Patient-Associated Characteristics Influencing the Risk for Non-Persistence with Statins in Older Patients with Peripheral Arterial Disease. Drugs & Aging. 2019;36(9):863-73.
Phan DQ, Duan L, Lam B, Hekiman A, Wee Z, Zadegan R, et al. Statin Adherence and Mortality in Patients Aged 80 Years and Older After Acute Myocardial Infarction. Journal of the American Geriatrics Society. 2019;67(10):2045-9.
Warren R, Falster, M.O., Tran, B., Jorm, L. Association of Continuity of Primary Care and Statin Adherence. PLOS ONE. 2015;10(10):e0140008.
45 and Up Study Collaborators. Cohort profile: the 45 and up study. International Journal of Epidemiology. 2008.
Lawrence G, Dinh I, Taylor L. The Centre for Health Record Linkage: a new resource for health services research and evaluation. Health Information Management Journal. 2008;37(2):60-2.
Liu Z, Moorin R, Worthington J, Tofler G, Bartlett M, Khan R, et al. Using Large-Scale Linkage Data to Evaluate the Effectiveness of a National Educational Program on Antithrombotic Prescribing and Associated Stroke Prevention in Primary Care. Journal of the American Heart Association. 2016;5(10).
Australian Government Department of Health. Medicare Benefits Schedule Book. Canberra: Department of Health; 2020.
Youens D, Harris M, Robinson S, Preen DB, Moorin RE. Regularity of contact with GPs: Measurement approaches to improve valid associations with hospitalization. Family Practice. 2019;Online ahead of publication (cmz002).
Bice T, Boxerman S. A Quantitative Measure of Continuity of Care. Medical Care. 1977;15(4):347-9.
Wallach-Kildemoes H, Andersen M, Diderichsen F, Lange T. Adherence to preventive statin therapy according to socioeconomic position. European Journal of Clinical Pharmacology. 2013;69(8):1553-63.
Jackevius C, Mamdani M, Tu J. Adherence With Statin Therapy in Elderly Patients With and Without Acute Coronary Syndromes. JAMA. 2002;288(4):462-7.
Yu A, Yu Y, Nichol M, Gwardry-Sridhar F. Delay in Filling the Initial Prescription for a Statin: A Potential Early Indicator of Medication Nonpersistence. Clinical Therapeutics. 2008;30(4):761-74.
Lavikainen P, Helin-Salmivaara A, Eerola M, Fang G, Hartikainen J, Huupponen R, et al. Statin adherence and risk of acute cardiovascular events among women: a cohort study accounting for time-dependent confounding affected by previous adherence. BMJ Open. 2016;6(e011306).
Pratt N, Kerr M, Barratt J, Kemp-Casey A, Kalisch Ellett L, Ramsay E, et al. The validity of the Rx-Risk Comorbidity Index using medicines mapped to the Anatomical Therapeutic Chemical (ATC) Classification System. BMJ Open. 2018;8(e021122).
Holman C, Preen D, Baynham N, Finn J, Semmens J. A multipurpose comorbidity scoring system performed better than the Charlson index. Journal of Clinical Epidemiology. 2005;58(10):1006-14.
Chou R, Dana T, Blazina I. Statin Use for the Prevention of Cardiovascular Disease in Adults: A Systematic Review for the U.S. Preventive Services Task Force Rockville (MD): National Centre for Biotechnology Information; 2016 [Available from: https://www.ncbi.nlm.nih.gov/books/NBK396417/table/ch1.t1/.
Australian Bureau of Statistics. Socio-Economic Indexes for Areas Canberra2018 [Available from: https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa.
Housing HCfPa. Accessibility/Remoteness Index of Australia (ARIA) Adelaide: The University of Adelaide; 2020 [Available from: https://www.adelaide.edu.au/hugo-centre/services/aria.
Bellera C, MacGrogan G, Debled M, Tunon de Lara C, Brouste V, Mathoulin-Pelissier S. Variables with time-varying effects and the Cox model: Some statistical concepts illustrated with a prognostic factor study in breast cancer. BMC Medical Research Methodology. 2010;10(20).
StataCorp. Stata. 16.0 ed. College Station, Texas: StataCorp; 2019.
Schaffer A, Buckley N, Dobbins T, Banks E, Pearson S. The crux of the matter: Did the ABC's Catalyst program change statin use in Australia? MJA. 2015;202(11):591-4.
Del Mar C. Copayments for general practice visits. MJA. 2014;200(7):367.
Scott A. Health Sector Report: General Practice Trends. Melbourne: The University of Melbourne; 2017.
Guthrie B, Wyke S. Does continuity in general practice really matter? BMJ. 2000;321:734-6.
Duckett S, Wilcox, S. The Australian Health Care System. 4th edition ed. Melbourne: Oxford University Press; 2011.
Willis E, Reynolds, L., Keleher, H. Understanding the Australian Health Care System. 3rd edition ed. NSW: Elsevier; 2016.
Toth P, Patti A, Giglio R, Nikolic D, Castellino G, Rizzo M, et al. Management of Statin Intolerance in 2018: Still More Questions Than Answers. American Journal of Cardiovascular Drugs. 2018;18(3):157-76.
Mealing N, Banks E, Jorm L, Steel D, Clements M, Rogers K. Investigation of relative risk estimates from studies of the same population with contrasting response rates and designs. BMC Medical Research Methodology. 2010;10(26).
Acknowledgements
The 45 and Up Study is managed by the Sax Institute in collaboration with major partner Cancer Council NSW; and partners: the National Heart Foundation of Australia (NSW Division); NSW Ministry of Health; NSW Government Family & Community Services – Ageing, Carers and the Disability Council NSW; and the Australian Red Cross Blood Service. We thank the many thousands of 45 and Up Study participants.
Funding
This work was funded by the National Health and Medical Research Council, project grant APP1078345, and completed using data collected through the 45 and Up Study (www.saxinstitute.org.au).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 738 kb)
Rights and permissions
About this article

Cite this article
Youens, D., Doust, J., Robinson, S. et al. Regularity and Continuity of GP Contacts and Use of Statins Amongst People at Risk of Cardiovascular Events. J GEN INTERN MED 36, 1656–1665 (2021). https://doi.org/10.1007/s11606-021-06638-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-021-06638-3