
Abstract
Background
Morbidity after gastrectomy remains high. The potentially modifiable risk factors have not been well described. This study considers a series of potentially modifiable patient-specific and perioperative characteristics that could be considered to reduce morbidity and mortality after gastrectomy.
Methods
This retrospective cohort study includes adults in the ACS NSQIP PUF dataset who underwent gastrectomy between 2011 and 2013. Sequential multivariable models were used to estimate effects of clinical covariates on study outcomes including morbidity, mortality, readmission, and reoperation.
Results
Three thousand six hundred and seventy-eight patients underwent gastrectomy. A majority of patients had distal gastrectomy (N = 2,799, 76.1 %) and had resection for malignancy (N = 2,316, 63.0 %). Seven hundred and ninety-eight patients (21.7 %) experienced a major complication. Reoperation was required in 290 patients (7.9 %). Thirty-day mortality was 5.2 %. Age (OR = 1.01, 95 % CI = 1.01–1.02, p = 0.001), preoperative malnutrition (OR = 1.65, 95 % CI = 1.35–2.02, p < 0.001), total gastrectomy (OR = 1.63, 95 % CI = 1.31–2.03, p < 0.001), benign indication for resection (OR = 1.60, 95 % CI = 1.29–1.97, p < 0.001), blood transfusion (OR = 2.57, 95 % CI = 2.10–3.13, p < 0.001), and intraoperative placement of a feeding tubes (OR = 1.28, 95 % CI = 1.00–1.62, p = 0.047) were independently associated with increased risk of morbidity. Association between tobacco use and morbidity was statistically marginal (OR = 1.23, 95 % CI = 0.99–1.53, p = 0.064). All-cause postoperative morbidity had significant associations with reoperation, readmission, and mortality (all p < 0.001).
Conclusions
Mitigation of perioperative risk factors including smoking and malnutrition as well as identified operative considerations may improve outcomes after gastrectomy. Postoperative morbidity has the strongest association with other measures of poor outcome: reoperation, readmission, and mortality.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Surgical quality improvement is at the forefront of outcome initiatives at both institutional and national levels.1–3 Advances in data collection and process management driven within the surgical community by the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) have led to increased awareness of perioperative morbidity and development of programs to improve patient-specific outcomes. Recent improvements in NSQIP include the addition of targeted modules for certain disease groups, including hepatobiliary, vascular, and colorectal among others, as well as more granular data abstraction to better highlight procedure-specific complications and risk factors.4, 5 Despite data suggesting considerable morbidity, gastrointestinal operations have not been the focus of recent targeted NSQIP improvement.6
Medical treatments of peptic ulcer disease and endoscopic advances have changed the landscape of upper gastrointestinal surgery. At present, gastric operations are largely resections for cancer or a part of high-volume bariatric subspecialty. Despite this perception, gastrectomy remains an important and morbid general surgery operation.7–11 A recent NSQIP study evaluating morbidity associated with gastrectomy for gastric cancer identified 5 % post-operative mortality after total gastrectomy—higher than current mortality after major hepatectomy or pancreaticoduodenectomy.8, 12, 13
From a perioperative perspective, the risks after gastrectomy have not been adequately explored. Institutional and registry data suggest an overall morbidity of approximately 20 % and increased risk of readmissions among patients who developed complications.7, 10, 14, 15 The individual effects associated with specific and potentially modifiable risk factors remain poorly defined. This study considers a series of patient-specific and perioperative characteristics, including diagnosis, extent of resection, intra- and post-operative blood transfusion, and use of surgically placed feeding tubes, on post-operative morbidity and mortality after gastrectomy. We hypothesized significant effects of these important clinical covariates on post-operative outcomes and aimed to identify potentially modifiable risk factors.
Materials and Methods
Patient Selection, Characteristics, and Outcome Definitions
The current study used patient records obtained from the ACS NSQIP public use file (PUF). NSQIP is a nationally maintained database that contains aggregated, patient-level, Health Insurance Portability and Accountability Act (HIPAA) compliant data provided by participating hospitals. The University of Virginia Institutional Review Board (UVA IRB) for Health Sciences Research (HSR) has designated the NSQIP PUF as a public data set; however, since a partial merger between NSQIP PUF data and institutional data was planned to evaluate associations between gastrectomy and readmission, this study was reviewed and approved by the UVA HSR IRB (IRB-HSR no. 18610).
All adult patients (≥18 years of age) who underwent gastrectomy for benign and malignant pathology between 2011 and 2013 were included in this retrospective cohort study. Readmission data collection was started in 2011; as such, that year was selected as the beginning of the cohort. All UVA patients who had gastrectomy and required readmission were re-reviewed and merged with institutional data to facilitate data interpretation. Gastrectomy was defined according to the index operation using current procedural terminology (CPT) codes: total gastrectomy (43620, 43621, 43622) and distal gastrectomy (43631, 43632, 43633, 43634). Patients who had partial or wedge non-anatomic gastric resection and did not require gastrointestinal reconstruction were not included in this study. Indication for resection, defined by final post-operative diagnosis including pathologic confirmation, was stratified into malignant and benign diagnoses using the International Classification of Diseases, 9th revision (ICD-9) codes (Appendix).
The primary outcome was occurrence of 30-day morbidity. Composite all-cause 30-day morbidity was defined as the occurrence of one or more of the following NSQIP-defined variables: pneumonia, reintubation, failure to wean off the ventilator, renal insufficiency, renal failure, cardiac arrest, myocardial infarction, coma, stroke, sepsis, septic shock, fascial dehiscence, organ space infection, or venous thromboembolism (deep vein thrombosis and/or pulmonary embolism). Secondary outcome measures included mortality, readmission, and reoperation. Standard NSQIP definitions of 30-day readmission and mortality were used. Reoperation was defined as any return to the operating room related to the index procedure or to a complication related to the index procedure. Preoperative malnutrition was defined as a preoperative albumin of less than 3 g/dL and/or preoperative weight loss of greater than 10 % of body weight. Patients receiving intraoperative placement of feeding tubes concomitant with the index gastrectomy procedure were identified using CPT codes for gastrostomy (43830) and jejunostomy (44015). Perioperative blood transfusion was defined as any transfusion of one or more units of packed red blood cells given from the start time of the index procedure through 72 h postoperatively.
Data analysis
Summary data for the patient cohort were aggregated to describe the demographic and clinical factors including, age, sex, body mass index, race, ethnicity, diabetes, tobacco use, serum albumin, indication for resection (benign or malignant), American Society of Anesthesiologists (ASA) class, operative duration, blood transfusion, surgical feeding tube placement, post-operative morbidity, readmission, reoperation, and mortality. Univariable and multivariable logistic regression analyses were used to test the effect of clinical covariates on study outcomes: morbidity, reoperation, readmission, and mortality. For each multivariable model, variables from univariate analyses that were defined a priori to reach the <0.05 significance threshold were included in multivariable analysis. Multivariable models testing the associations between covariates and mortality were performed with and without the readmission variable. For the purposes of the logistic regression analysis, operative time was categorized at the median (median operative time = 194 min). STATA version 14.1 (StataCorp LP, College Station, TX, USA) software was used for data management and statistical analysis.
Results
Patient Characteristics and Preoperative Risk Factors
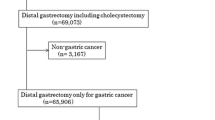
A total of 3,678 patients underwent distal or total anatomic gastrectomy during the study period. A majority of patients had distal gastrectomy (N = 2,799, 76.1 %), and the remaining 879 patients (23.9 %) underwent total gastrectomy. A majority of patients (N = 2,316, 63.0 %) underwent resection for malignancy. Patient demographics and perioperative factors are summarized in Table 1. Intra- and post-operative blood transfusions were required in 22.7 % of the cohort. Surgically placed feeding tubes (including gastrostomy and jejunostomy) were used in 14.4 % of the patients. Seven hundred and ninety-eight patients (21.7 %) had one or more instances of major morbidity. Frequencies of post-operative NSQIP morbidities are summarized in Table 2. The two most common complications were organ space surgical site infection (7.1 %) and sepsis (6.8 %). Reoperation was required in 290 patients (7.9 %), and 447 patients (12.2 %) were readmitted within 30 days of discharge.
Estimates of Covariate Associations with Morbidity, Reoperation, and Readmission
Univariable and multivariable models were tested to estimate associations between demographic and clinical factors and post-operative morbidity (Table 3). Univariable analysis identified age, race, preoperative malnutrition, tobacco use, ASA class 4 and 5, total gastrectomy, benign indication for operation, perioperative blood transfusion, operative duration ≥ median, and placement of surgical feeding tube as associated with postoperative morbidity (all p ≤ 0.036). After adjusting for significant demographic and clinical covariates, age (OR = 1.01, 95 % CI = 1.01–1.02, p = 0.001), preoperative malnutrition (OR = 1.65, 95 % CI = 1.35–2.02, p < 0.001), total gastrectomy (OR = 1.63, 95 % CI = 1.31–2.03, p < 0.001), benign indication for resection (OR = 1.60, 95 % CI = 1.29–1.97, p < 0.001), blood transfusion (OR = 2.57, 95 % CI = 2.10–3.13, p < 0.001), operative time ≥ median (OR = 1.43, 95 % CI = 1.18–1.73, p < 0.001), and intraoperative placement of a feeding tube (OR = 1.28, 95 % CI = 1.00–1.62, p = 0.047) were independently associated with postoperative morbidity. Associations between tobacco use and greater morbidity were marginal (OR = 1.23, 95%CI = 0.99–1.53, p = 0.064).
There was no difference in age (p = 0.60) or ASA class (p = 0.070) between patient cohorts who had surgically inserted feeding tubes and patients who had gastrectomy without placement of an intraoperative feeding tube. Patients who had intraoperative feeding tubes were more likely to have preoperative malnutrition (28.9 vs. 24.1 %, p = 0.019), total gastrectomy (50.6 vs. 19.4 %, p < 0.001), malignant diagnoses (71.7 vs. 61.5 %, p < 0.001), and perioperative blood transfusion (26.0 vs. 22.1 %, p = 0.046). Significantly greater proportion of patients with benign (non-malignant) indication for resection had higher preoperative ASA class 4/5 compared to patients with malignant diagnosis (17.6 vs. 7.7 %, respectively, p < 0.001).
Univariable and multivariable models testing the associations between clinical covariates and reoperation and readmission are summarized in Tables 4 and 5, respectively. After adjustment for covariates, tobacco use was the only preoperative risk factor associated with increased risk of reoperation (OR = 1.51, 95 % CI = 1.12–2.05, p = 0.008). Postoperative morbidity was strongly associated with reoperation (OR = 10.7, 95 % CI = 7.94–14.4, p < 0.001). The association between perioperative blood transfusion and risk of reoperation approached significance (OR = 1.30, 95 % CI = 0.96–1.76, p = 0.088). Age, reoperation, and all-cause morbidity (all p ≤ 0.003) were independently associated with readmission after gastrectomy (Table 5).
Postoperative Mortality After Gastrectomy
Thirty-day mortality in the study population was 5.2 %. There was no difference in mortality after distal and total gastrectomy (5.0 vs. 5.7 %, respectively, p = 0.45). Univariable and multivariable analyses demonstrating associations between study covariates and mortality are summarized in Table 6. Univariable comparisons identified age, Hispanic ethnicity, preoperative malnutrition, ASA class 4 and 5, non-malignant indication for resection, blood transfusion, operative time less than the median, all-cause morbidity, and reoperation as significantly associated with mortality (all p ≤ 0.043). After adjustment for covariates, age (OR = 1.04, 95 % CI = 1.03–1.06, p < 0.001), preoperative malnutrition (OR = 1.86, 95 % CI = 1.31–2.65, p = 0.001), blood transfusion (OR = 2.00, 95 % CI = 1.40–2.87, p < 0.001), all-cause morbidity (OR = 6.78, 95 % CI = 4.62–9.95, p < 0.001), and reoperation (OR 1.74, 95 % CI = 1.15–2.65, p = 0.010) were independently associated with mortality (Table 6).
The reported multivariable mortality model does not include the readmission variable. When included in the model, readmission is associated with decreased NSQIP-reported mortality (OR = 0.37, 95 % CI = 0.20–0.69, p = 0.002). Using the current NSQIP variable definition, the patient who is readmitted and dies within a 30-day period would not be reported as dead within the NSQIP PUF. To further explore association between readmission and mortality, all patients who had gastrectomy at our institution were examined. Of 42 institutional patients who had gastrectomy during the study period, none died within 30 days of operation; two (4.8 %) died within 90 days of operation. Further statistical analysis is not feasible.
Discussion
Gastrectomy remains the preferred surgical treatment option for many benign and malignant diseases affecting the upper gastrointestinal tract. Common indications for gastrectomy include malignancy (i.e., adenocarcinoma, gastrointestinal stromal tumors, selected neuroendocrine neoplasms, etc.) and recalcitrant peptic ulcer disease or one of its long-term sequelae such as bleeding, perforation, or stricture. Outcomes after gastrectomy in non-bariatric patients have arguably received less scrutiny than outcomes after hepatobiliary, pancreatic, or colorectal resections. At present, gastrectomy is not one of the NSQIP targeted modules, which has direct implications for limited data collection and less targeted areas for performance improvement.
Indeed, for targeted surgical procedure modules, operation-specific complications, such as anastomotic leaks, fistula, or postoperative ileus are identified using extended data collection. Without focused data collection, gastrectomy cases are not well represented among the larger population of complex abdominal cases and lack granular targeted-module data. Not surprisingly, and consistent with published data, surgical site infection and sepsis are the two most common metrics of NSQIP measured morbidity in this study.16 The organ space SSI of 7.05 % is consistent with published rates of anastomotic leaks in recent literature ranging from 5 to 7 %; however, without targeted NSQIP data collection, the exact proportion of anastomotic leaks rather than other surgically-related causes of intra-abdominal infection cannot be defined precisely.17–20
NSQIP-reported mortality after gastrectomy is higher than mortality after major hepatectomy, pancreaticoduodenectomy, and esophagectomy.12, 13, 21 Indeed, our study identified a 30-day mortality rate of 5.2 %. While some institutional studies have described 0 % mortality, database and multi-center collaborative studies consistently report significantly higher patient mortality.9, 11, 22–28 A recent multi-center study from the US Gastric Cancer Collaborative of 447 sub-total resections for gastric cancer between 2000 and 2012 reported a similar 4.9 % mortality rate for all patients.29 Mortality rates following total gastrectomy have also varied from as low as zero in single-center studies to >6 % in multi-center analyses.24, 30, 31 To address potentially modifiable risk factors in patients undergoing gastrectomy, we explored a series of clinical perioperative covariates using sequential multivariable models.
Not surprisingly, age and emergent operation (ASA class 4 and 5 patients) were associated with increased morbidity. After multivariable adjustments: tobacco use, preoperative malnutrition, total gastrectomy, benign (non-malignant) indication for resection, feeding tube insertion, and blood transfusion are all associated with an increase in postoperative morbidity. Tobacco use is a potentially modifiable risk factor and preoperative smoking cessation has been reported to improve outcomes after gastrectomy for malignancy.32 Malnutrition, extent of resection, and blood transfusion have been recognized as important contributors to morbidity. Blood transfusions in gastric cancer patients have also been associated with decreased recurrence-free and overall survival.33 While indication for resection is not a modifiable risk factor, it is important to recognize that even after adjustment for significant factors including emergency operation, non-malignant diagnoses were associated with increased morbidity. Sequelae of gastric ulcer disease remain an important contributor to patient morbidity, highlighted in this patient cohort where over 35 % of gastric resections were performed for a non-malignant diagnosis. Greater than 80 % of patients with benign diagnoses had operation for peptic ulcer disease or one of its sequelae including perforation, bleeding, or stricture/obstruction. Significantly more patients with benign diagnosis had ASA class 4/5 and required an emergent operation which likely contributed to increased morbidity and mortality in this group.
Similarly, feeding tube insertion was associated with higher morbidity. Patients who had feeding tubes were more likely to have malignancy, preoperative malnutrition, require total gastrectomy, and receive perioperative blood transfusion. While intraoperative insertion of feeding tubes was associated with greater morbidity, causation is likely multifactorial. Comparisons of surgical risk based on age and ASA class did not reveal significant differences between those patients who had feeding tubes and those who did not. However, patients who had feeding tubes were more likely to have preoperative malnutrition, total gastrectomy, as well as malignant diagnosis. While malnutrition, extent of resection, and diagnosis are included in the multivariable morbidity model, more granular data including complications specific to feeding tubes, such as re-operation for complication of feeding tubes, tube dislodgment, tube feed intolerance, are not available. We do not believe that our study contains sufficient data to recommend either placement or avoidance of feeding tubes in this patient population.
Review of reoperation, readmission, and mortality models is important. All cause morbidity is the most significant variable associated with all three of these specific complications. Smoking is independently associated with reoperation; the association between blood transfusion and reoperation nearly reached significance (p = 0.088). Age, malnutrition, blood transfusion, reoperation, and all-cause morbidity are all independently associated with mortality; however, the association between NSQIP defined readmission and mortality is difficult to define.
In this study, 12.2 % of patients required readmission, which is comparable to published data.7, 10, 14, 15 If included in the model for mortality, NSQIP defined readmission is associated with lower risk of mortality. This is likely due to two different and opposite circumstances1: inadequate data capture—NSQIP data collection only includes mortality for 30 days post-procedure or to the time of first discharge exclusive of discharge after readmission, or2 hospital readmission resulted in patient care that avoided death. In an attempt to better understand this relationship, we examined institutional data for patients who had gastrectomy at our institution. Unfortunately, given relatively few cases and only two readmissions, the relationship between readmission and mortality could not be further defined. Ongoing improvements in NSQIP data collection, including further incorporation and improvement of readmission variable and further development of targeted modules, might help explain associations between readmission and mortality.
Recent expansion of minimally invasive techniques has altered approaches to surgical gastric disease at selected institutions. While choice of techniques and expertise differs, in general minimally invasive approaches are as safe or perhaps safer in selected patients.23, 34, 35 Without a targeted NSQIP module, inclusion of minimally invasive techniques is not possible and represents a limitation of the current study. Introduction of specific minimally invasive gastric resection CPT codes or development of a targeted gastric or gastrointestinal module with improved capture of minimally invasive approach (in the absence of new CPT codes) would improve data collection and use in this patient population with higher overall mortality compared to many other major abdominal operations.
Our study demonstrates significant associations between smoking, preoperative malnutrition, blood transfusions, extent of resection, benign diagnosis, and post-gastrectomy morbidity. Post-gastrectomy morbidity is the most significant variable affecting reoperation, readmission, and mortality. Limitations in data collection, including lack of a NSQIP targeted module, restrict available analyses and interpretation of data. While institutional studies include more granular data, patient selection bias limits generalizability to broad patient population. However, certain study variables, such as readmission, are difficult to interpret given current NSQIP data collection and can be better examined using multi-institutional collaboratives. To date, recent collaboratives have focused on patients with malignancy, excluding nearly 40 % of patients requiring gastrectomy for non-malignant diagnosis. Consideration of significant postoperative morbidity and mortality in this patient population should improve process of care and patient outcomes.
Conclusions
Based on the current study, at least four potentially modifiable patient factors can be considered in limiting morbidity and mortality after gastrectomy1: smoking cessation and2 preoperative nutritional optimization should be pursued3, meticulous operative technique should limit use of perioperative blood transfusions, and4 patients with non-malignant indications for resection and/or total gastrectomy should be considered higher risk patients with appropriately designated postoperative care pathways.
References
Lucas DJ, Pawlik TM. Quality improvement in gastrointestinal surgical oncology with American College of Surgeons National Surgical Quality Improvement Program. Surgery. 2014;155(4):593–601.
Day RW, Badgwell BD, Fournier KF, Mansfield PF, Aloia TA. Defining the Impact of Surgical Approach on Perioperative Outcomes for Patients with Gastric Cardia Malignancy. J Gastrointest Surg. 2016;20(1):146–53.
Cloyd JM, Ma Y, Morton JM, Kurella Tamura M, Poultsides GA, Visser BC. Does chronic kidney disease affect outcomes after major abdominal surgery? Results from the National Surgical Quality Improvement Program. J Gastrointest Surg. 2014;18(3):605–12.
Kohut AY, Liu JJ, Stein DE, Sensenig R, Poggio JL. Patient-specific risk factors are predictive for postoperative adverse events in colorectal surgery: an American College of Surgeons National Surgical Quality Improvement Program-based analysis. Am J Surg. 2015;209(2):219–29.
Epelboym I, Gawlas I, Lee JA, Schrope B, Chabot JA, Allendorf JD. Limitations of ACS-NSQIP in reporting complications for patients undergoing pancreatectomy: underscoring the need for a pancreas-specific module. World J Surg. 2014;38(6):1461–7.
Turrentine FE, Denlinger CE, Simpson VB, Garwood RA, Guerlain S, Agrawal A, et al. Morbidity, mortality, cost, and survival estimates of gastrointestinal anastomotic leaks. J Am Coll Surg. 2015;220(2):195–206.
Merchant SJ, Ituarte PH, Choi A, Sun V, Chao J, Lee B, et al. Hospital Readmission Following Surgery for Gastric Cancer: Frequency, Timing, Etiologies, and Survival. J Gastrointest Surg. 2015;19(10):1769–81.
Papenfuss WA, Kukar M, Oxenberg J, Attwood K, Nurkin S, Malhotra U, et al. Morbidity and mortality associated with gastrectomy for gastric cancer. Ann Surg Oncol. 2014;21(9):3008–14.
Selby LV, Vertosick EA, Sjoberg DD, Schattner MA, Janjigian YY, Brennan MF, et al. Morbidity after Total Gastrectomy: Analysis of 238 Patients. J Am Coll Surg. 2015;220(5):863–71 e2.
Ahmad R, Schmidt BH, Rattner DW, Mullen JT. Factors influencing readmission after curative gastrectomy for gastric cancer. J Am Coll Surg. 2014;218(6):1215–22.
Jeong O, Ryu SY, Choi WY, Piao Z, Park YK. Risk factors and learning curve associated with postoperative morbidity of laparoscopic total gastrectomy for gastric carcinoma. Ann Surg Oncol. 2014;21(9):2994–3001.
Newhook TE, LaPar DJ, Lindberg JM, Bauer TW, Adams RB, Zaydfudim VM. Morbidity and mortality of pancreaticoduodenectomy for benign and premalignant pancreatic neoplasms. J Gastrointest Surg. 2015;19(6):1072–7.
Newhook TE, LaPar DJ, Lindberg JM, Bauer TW, Adams RB, Zaydfudim VM. Morbidity and mortality of hepatectomy for benign liver tumors. Am J Surg. 2016;211(1):102–8.
Kim MC, Kim KH, Jung GJ. A 5 year analysis of readmissions after radical subtotal gastrectomy for early gastric cancer. Ann Surg Oncol. 2012;19(8):2459–64.
Zhuang CL, Wang SL, Huang DD, Pang WY, Lou N, Chen BC, et al. Risk factors for hospital readmission after radical gastrectomy for gastric cancer: a prospective study. PLoS One. 2015;10(4):e0125572.
Migita K, Takayama T, Matsumoto S, Wakatsuki K, Enomoto K, Tanaka T, et al. Risk factors for surgical site infections after elective gastrectomy. J Gastrointest Surg. 2012;16(6):1107–15.
Andreou A, Biebl M, Dadras M, Struecker B, Sauer IM, Thuss-Patience PC, et al. Anastomotic leak predicts diminished long-term survival after resection for gastric and esophageal cancer. Surgery. 2016.
Sierzega M, Kolodziejczyk P, Kulig J, Polish Gastric Cancer Study G. Impact of anastomotic leakage on long-term survival after total gastrectomy for carcinoma of the stomach. Br J Surg. 2010;97(7):1035–42.
Samples JE, Snavely AC, Meyers MO. Postoperative Morbidity in Curative Resection of Gastroesophageal Carcinoma Does Not Impact Long-term Survival. Am Surg. 2015;81(12):1228–31.
Doglietto GB, Papa V, Tortorelli AP, Bossola M, Covino M, Pacelli F, et al. Nasojejunal tube placement after total gastrectomy: a multicenter prospective randomized trial. Arch Surg. 2004;139(12):1309–13; discussion 13.
Dhungel B, Diggs BS, Hunter JG, Sheppard BC, Vetto JT, Dolan JP. Patient and peri-operative predictors of morbidity and mortality after esophagectomy: American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP), 2005–2008. J Gastrointest Surg. 2010;14(10):1492–501.
Jeong O, Park YK, Ryu SY. Early experience of duet laparoscopic distal gastrectomy (duet-LDG) using three abdominal ports for gastric carcinoma: surgical technique and comparison with conventional laparoscopic distal gastrectomy. Surg Endosc. 2015. doi:10.1007/s00464-015-4653-4.
Lee JH, Nam BH, Ryu KW, Ryu SY, Kim YW, Park YK, et al. Comparison of the long-term results of patients who underwent laparoscopy versus open distal gastrectomy. Surg Endosc. 2015. doi:10.1007/s00464-015-4215-9.
Bo T, Peiwu Y, Feng Q, Yongliang Z, Yan S, Yingxue H, et al. Laparoscopy-assisted vs. open total gastrectomy for advanced gastric cancer: long-term outcomes and technical aspects of a case–control study. J Gastrointest Surg. 2013;17(7):1202–8.
Kurita N, Miyata H, Gotoh M, Shimada M, Imura S, Kimura W, et al. Risk Model for Distal Gastrectomy When Treating Gastric Cancer on the Basis of Data From 33,917 Japanese Patients Collected Using a Nationwide Web-based Data Entry System. Ann Surg. 2015;262(2):295–303.
Yoshikawa T, Cho H, Rino Y, Yamamoto Y, Kimura M, Fukunaga T, et al. A prospective feasibility and safety study of laparoscopy-assisted distal gastrectomy for clinical stage I gastric cancer initiated by surgeons with much experience of open gastrectomy and laparoscopic surgery. Gastric Cancer. 2013;16(2):126–32.
Hu Y, Huang C, Sun Y, Su X, Cao H, Hu J, et al. Morbidity and Mortality of Laparoscopic Versus Open D2 Distal Gastrectomy for Advanced Gastric Cancer: A Randomized Controlled Trial. J Clin Oncol. 2016;34(12):1350–7.
Imamura H, Takiguchi S, Yamamoto K, Hirao M, Fujita J, Miyashiro I, et al. Morbidity and mortality results from a prospective randomized controlled trial comparing Billroth I and Roux-en-Y reconstructive procedures after distal gastrectomy for gastric cancer. World J Surg. 2012;36(3):632–7.
Tran TB, Worhunsky DJ, Squires MH, Jin LX, Spolverato G, Votanopoulos KI, et al. To Roux or not to Roux: a comparison between Roux-en-Y and Billroth II reconstruction following partial gastrectomy for gastric cancer. Gastric Cancer. 2016;19(3):994–1001.
Cuschieri A, Fayers P, Fielding J, Craven J, Bancewicz J, Joypaul V, et al. Postoperative morbidity and mortality after D1 and D2 resections for gastric cancer: preliminary results of the MRC randomised controlled surgical trial. The Surgical Cooperative Group. Lancet. 1996;347(9007):995–9.
Higgins RM, Kubasiak JC, Jacobson RA, Janssen I, Myers JA, Millikan KW, et al. Outcomes and Use of Laparoscopic Versus Open Gastric Resection. JSLS. 2015;19(4):e2015.00095.
Jung KH, Kim SM, Choi MG, Lee JH, Noh JH, Sohn TS, et al. Preoperative smoking cessation can reduce postoperative complications in gastric cancer surgery. Gastric Cancer. 2015;18(4):683–90.
Squires MH, 3rd, Kooby DA, Poultsides GA, Weber SM, Bloomston M, Fields RC, et al. Effect of Perioperative Transfusion on Recurrence and Survival after Gastric Cancer Resection: A 7-Institution Analysis of 765 Patients from the US Gastric Cancer Collaborative. J Am Coll Surg. 2015;221(3):767–77.
Kim W, Kim HH, Han SU, Kim MC, Hyung WJ, Ryu SW, et al. Decreased Morbidity of Laparoscopic Distal Gastrectomy Compared With Open Distal Gastrectomy for Stage I Gastric Cancer: Short-term Outcomes From a Multicenter Randomized Controlled Trial (KLASS-01). Ann Surg. 2016;263(1):28–35.
Vinuela EF, Gonen M, Brennan MF, Coit DG, Strong VE. Laparoscopic versus open distal gastrectomy for gastric cancer: a meta-analysis of randomized controlled trials and high-quality nonrandomized studies. Ann Surg. 2012;255(3):446–56.
Acknowledgments
American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of a portion of data used herein; they have not verified and are not responsible for the statistical validity of the data analyses or the conclusions derived by the authors. This study was supported in part by funding support provided by the Institutional National Research Service Award T32 CA 163177 from the National Cancer Institute to A.N.M.
Author information
Authors and Affiliations
Corresponding author
Appendix
Appendix
Malignant ICD-9 Diagnoses for Gastrectomy
145.9, 150.2, 150.5, 150.8, 150.9, 151, 151.1, 151.2, 151.3, 151.4, 151.5, 151.6, 151.8, 151.9, 152, 152.1, 152.8, 152.9, 153, 153.1, 153.2, 153.9, 154, 154.3, 155.1, 157, 157.8, 157.9, 158, 158.8, 159.1, 159.9, 162.9, 171.5, 174.8, 174.9, 183, 185, 189, 191.9, 194, 195.2, 196.2, 197.4, 197.5, 197.6, 197.7, 197.8, 198.89, 199.1, 200.2, 200.3, 200.33, 200.63, 202.8, 202.83, 209, 209.01, 209.23, 209.25, 209.29, 209.3, 209.72, 209.79, 230.2, 230.9, 235.2, 235.3, 235.5, 238, 238.1, 239, 239.2, 239.89, V10.04, V66.7
Benign ICD-9 Diagnoses for Gastrectomy
38.41, 38.9, 200.52, 209.4, 209.41, 209.6, 209.63, 209.65, 209.69, 211, 211.1, 211.2, 211.3, 211.8, 211.9, 214.3, 215.5, 228.04, 237.71, 250.6, 250.61, 250.63, 255.41, 258.01, 259.2, 263.9, 277.03, 280.9, 285.1, 285.22, 441.4, 442.83, 453, 482.82, 507, 530, 530.1, 530.11, 530.3, 530.4, 530.5, 530.81, 530.85, 530.87, 531, 531.01, 531.1, 531.11, 531.2, 531.3, 531.31, 531.4, 531.41, 531.5, 531.51, 531.6, 531.61, 531.7, 531.71, 531.9, 531.91, 532, 532.01, 532.1, 532.11, 532.2, 532.31, 532.4, 532.41, 532.5, 532.51, 532.6, 532.7, 532.71, 532.9, 532.91, 533, 533.1, 533.4, 533.41, 533.5, 533.51, 533.6, 533.7, 533.71, 533.9, 533.91, 534, 534.01, 534.2, 534.3, 534.4, 534.41, 534.5, 534.6, 534.7, 534.71, 534.9, 534.91, 535, 535.01, 535.1, 535.11, 535.2, 535.4, 535.41, 535.5, 535.61, 536.1, 536.3, 536.41, 536.8, 536.9, 537, 537.1, 537.3, 537.4, 537.6, 537.8, 537.82, 537.83, 537.84, 537.89, 537.9, 551.3, 552.2, 552.3, 552.8, 553.21, 553.3, 553.9, 555, 557, 557.1, 557.9, 560.2, 560.31, 560.8, 560.81, 560.89, 560.9, 562, 562.02, 562.1, 564.2, 564.3, 564.89, 567.21, 567.22, 567.29, 567.38, 567.89, 567.9, 568, 568.81, 568.89, 569.69, 569.81, 569.83, 569.89, 572.3, 574.1, 575, 575.12, 576.2, 576.8, 577.1, 577.2, 577.8, 577.9, 578, 578.9, 584.9, 648.93, 682.2, 717.83, 750.7, 751.5, 751.7, 758.9, 786.09, 787, 787.02, 787.2, 789, 789.07, 789.3, 793.89, 799.89, 879.2, 935.2, 936, 995.92, 996.59, 996.69, 997.4, 997.49, 998.09, 998.11, 998.2, 998.3, 998.59, 998.6, 998.89, E878.2, V12.71, V16.0, V50.49, V83.89
Rights and permissions
About this article

Cite this article
Martin, A.N., Das, D., Turrentine, F.E. et al. Morbidity and Mortality After Gastrectomy: Identification of Modifiable Risk Factors. J Gastrointest Surg 20, 1554–1564 (2016). https://doi.org/10.1007/s11605-016-3195-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-016-3195-y