
Abstract
Purpose
The JSMP01 dosimetry protocol had adopted the provisional 60Co calibration coefficient \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\), namely, the product of exposure calibration coefficient N C and conversion coefficient k D,X. After that, the absorbed dose to water D w standard was established, and the JSMP12 protocol adopted the \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\) calibration. In this study, the influence of the calibration shift on the measurement of D w among users was analyzed.
Materials and methods
The intercomparison of the D w using an ionization chamber was annually performed by visiting related hospitals. Intercomparison results before and after the calibration shift were analyzed, the deviation of D w among users was re-evaluated, and the cause of deviation was estimated.
Results
As a result, the stability of LINAC, calibration of the thermometer and barometer, and collection method of ion recombination were confirmed. The statistical significance of standard deviation of D w was not observed, but that of difference of D w among users was observed between N C and \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\) calibration.
Conclusion
Uncertainty due to chamber-to-chamber variation was reduced by the calibration shift, consequently reducing the uncertainty among users regarding D w. The result also pointed out uncertainty might be reduced by accurate and detailed instructions on the setup of an ionization chamber.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Because of the steep dose–response curves, tumor control and normal tissue complications are affected by the dose delivered to the patient in radiation therapy. Overall uncertainty is estimated to be 5% (with coverage factor k = 1) at present [1, 2], and 3% should be the goal of the delivered dose in the near future [1]. If 3% were required as the overall uncertainty [1], 1% should be the goal of the absorbed dose to water (D w) at the calibration point.
To reduce the uncertainty of D w at the calibration point, the 60Co calibration coefficient \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\), in terms of the absorbed dose to water, has been introduced in the global standard dosimetry protocols [2, 3]. In the protocols, D w,Q for therapy-level megavoltage photons at beam quality Q is given by.
where M Q is the corrected charge reading, and \(k_{{{\text{Q,Q}}_{ 0} }}^{{}}\) is the beam quality conversion factor to correct for the response of the ionization chamber between the reference beam quality 60Co γ-rays and the user beam quality Q. In 2002, the Japan Society of Medical Physics (JSMP) adopted \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\) formalism in the dosimetry protocol (JSMP01) [4]. However, the D w standard had not been established at that time. For that reason, provisional \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\) was given by
where N C is the exposure calibration coefficient for 60Co γ-rays and k D,X is the exposure to the absorbed dose conversion coefficient for 60Co γ-rays. Table 1 shows the uncertainty budget of the comparison between dosimetry protocols. Despite the relative standard uncertainty of the N C being 0.74% [4], the relative standard uncertainty of the N C k D,X (provisional \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\)) was estimated to be 1.5% [4] because the k D,X was calculated using nominal dimensions and the material of the ionization chamber rather than individual ones. As a result, the original purpose of JSMP01—namely reduction of D w uncertainty by adopting the D w standard, was not achieved until 2012.
The D w standard in 60Co γ-rays was established at the National Metrology Institute of Japan (NMIJ) in 2011 [5] and the \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\) calibration service has been provided by the Association for Nuclear Technology in Medicine (ANTM) as an Secondary Standards Dosimetry Laboratories (SSDL) since 2012. The relative standard uncertainty of \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\) was estimated as 0.52% by direct \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\) calibration. A new standard dosimetry protocol (JSMP12) was issued in 2012 [6]. The combined relative standard uncertainty of D w was estimated at 1.5%, which was reduced from 2.0% in the case of the JSMP01, and the deviation of D w among users was expected to become smaller.
The ANTM investigated the deviation of D w among users by a mailed dose audit with a radiophotoluminescent glass dosimeter (RGD) [7]. Despite a sufficient number of samples, there was no significant difference in the standard deviation of D w between these two protocols.
The intercomparison of the D w using an ionization chamber was annually performed by visiting related hospitals. In this study, intercomparison results before and after the calibration shift were analyzed, the deviation of D w among users was re-evaluated, and the cause of deviation was estimated.
Materials and methods
Intercomparison by visiting related hospitals
The intercomparison of D w was annually performed for quality assurance of related hospitals (RH) that belong to the Tokyo metropolitan government from 2007 to 2014, except 2012 due to a transition period of the standard dosimetry protocol. The number of hospitals and photon beams in each fiscal year are shown in Table 2. A total of 157 photon beams, including 4 MV (0.615 ≤ TPR 20,10 ≤ 0.640), 6 MV (0.663 ≤ TPR 20,10 ≤ 0.684), and 10 MV (0.735 ≤ TPR 20,10 ≤ 0.748), were investigated.
The combination of LINAC, ionization chamber, and electrometer in the RH is shown in Table 3. The table also shows nominal energy and the beam quality index TPR 20,10 of each LINAC. The 30013 ionization chamber (PTW, Freiburg) was used at most hospitals in this investigation. Since it occupies about a 78% share of the market in Japan [8], the result in this report represents the current situation. The measurement equipment of our institute (OI), the Tokyo metropolitan university, is shown in Table 4. Other than the ionization chamber and electrometer, a water tank, calibrated barometer and thermometer were also used in the RH. The measurement equipment of RH and OI was completely separated and the setting of equipment was performed by own staff. Besides the D w at calibration depth, TPR 20,10, \(k_{{{\text{Q,Q}}_{ 0} }}^{{}}\), the ion recombination correction factor k s, and the temperature and pressure correction factor k TP were determined individually. The D w and factors for D w determination were recorded, and results were compared using the recording form shown in Fig. 1.

Recording form for intercomparison
Deviation of the D w and factors for D w determination
After sufficient pre-irradiation, each measurement was performed on at least five exposures under the same monitor unit and reference conditions: a calibration depth of 10 cm for a 10-cm × 10-cm field and a source-to-chamber distance of 100 cm. D w had been evaluated by Eq. (1) and provisional \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\) by Eq. (2) according to JSMP01 until 2011, or by only Eq. (1) according to JSMP12 since 2013. However, the results in fiscal year 2007 and 2008 are not included in this report because an uncalibrated barometer was used in some hospitals.
When D w determined by OI (D w)OI was assumed to be standard, the relative difference δ (D w) between (D w)RH and (D w)OI was given by:
Analogous to Eq. (3), the relative difference δ of k TP, k s, TPR 20,10 and \(k_{{{\text{Q,Q}}_{ 0} }}^{{}}\) between RH and OI was analyzed. However, the δ of those factors was derived from whole samples since 2009, because those factors have no relation to calibration shift.
Results
Deviation of the D w
A histogram for δ (D w) from 2010 to 2014 is shown in Fig. 2; that for 2009 is not shown because it is almost identical to that for 2010 and 2011. The standard deviations σ of δ (D w) in 2010, 2011, 2013, and 2014 were 0.57, 0.69, 0.43, and 0.56, respectively. The results of F tests for σ are shown in Table 5. No statistical significance (P < 0.05) was observed, except between 2011 and 2013. The cause of the statistical significance may be that the number of hospitals in 2013 was less than that in other fiscal years, because the protocol shift to JSMP12 was not completed in 2013 in some small-scale hospitals.

Temporal change of relative difference of D w, δ (D w) from fiscal year 2010 to 2014
The means of δ (D w) in 2010, 2011, 2013, and 2014 were −0.49, −0.67, −0.11, and −0.15, respectively. The results of Student’s or Welch’s t test are shown in Table 5. Statistical significance (P < 0.05) was observed between before and after calibration shift, although the change was within the range of the σ.
Deviation of factors for D w determination
The relative difference in factors for D w determination [δ (k TP), δ (k s), δ (TPR20,10) and δ (\(k_{{{\text{Q,Q}}_{ 0} }}^{{}}\))] is shown in Fig. 3; δ was derived from whole samples of the intercomparison, because no difference was observed between fiscal years. The σ of δ (k TP), δ (k s), and δ (\(k_{{{\text{Q,Q}}_{ 0} }}^{{}}\)) was 0.11, 0.08, and 0.14%, respectively. On the other hand, σ of the δ (TPR 20,10) was 0.42%.

Relative difference of k TP, k s, TPR 20,10, and \(k_{{{\text{Q,Q}}_{ 0} }}^{{}}\) between related hospitals (RH) and our institution (OI)
Discussion
According to JSMP01, the ratio between D w estimated by RH and OI in Eq. (3) is expanded as follows:
In a similar fashion, the ratio of D w according to JSMP12 is expanded as follows:
These quantities have items of uncertainty, as shown in Table 6, and can be separated into two categories: dependent or independent between the numerator and denominator. When items are dependent, they have the same quantity and direction of uncertainty, so that they could cancel each other out and do not contribute to the uncertainty of δ (D w). N C and \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\), except the item “measurement by the user electrometer and ionization chamber” at the calibration, are dependent because the entire ionization chamber was calibrated by the ANTM. The k D,X and \(k_{{{\text{Q,Q}}_{ 0} }}^{{}}\), except the item chamber-to-chamber variation of perturbation correction, are also dependent, because they are calculated using nominal dimensions and material for each model.
On the other hand, M in the numerator and denominator are independent, because the measurement by RH and OI was completely separated. The variation of δ (D w) was caused mainly by the variation of M. Therefore, items of uncertainty of M were analyzed. The coefficient of variation of electrometer readings M raw, δ (k TP), and δ (k s) were within 0.1%, so that the stability of LINAC, calibration of the thermometer and barometer, and collection method of ion recombination were confirmed.
The variation of TPR 20,10 is insensitive to \(k_{{{\text{Q,Q}}_{ 0} }}^{{}}\) [2]. However, it represents variation of ionization chamber positioning so that it might involve the variation of D w. The σ of (TPR 20,10) was larger than other factors: 0.42% is equivalent to ± 1.6 mm of water depth displacement for 10 MV X-rays and corresponds to 0.4% of dose difference. Figure 4 shows the relative difference distribution between TPR 20,10 in the fiscal year concerned (TPR 20,10)con and that in the preceding fiscal year (TPR 20,10)pre by (a) RH and (b) OI. The σ of the relative difference by RH and OI was 0.31% and 0.22%, respectively. The σ is smaller than the estimated uncertainty of the “Reference condition” (0.4%) by IAEA and JSMP as shown in Table 1. However, by the F tests of σ, statistical significance (P < 0.05) was observed between RH and OI. This may be because the OI owns a measurement procedure manual with step-by-step description and a specified person managed the measurement. Therefore, uncertainty could be reduced by detailed documentation on how to set up an ionization chamber with reference conditions accurately for every measurement. As an example, the instruction of checking if the cylinder chamber and its reflection in water image form a perfect circle with the eye at the same level as the water level needs to be added to a condition of setting the center of the chamber at the water surface [9].

Relative difference between TPR 20,10 of the current and preceding fiscal year
The uncertainty of M between JSMP01 and JSMP12 was identical, and chamber-to-chamber variation of \(k_{{{\text{Q,Q}}_{ 0} }}^{{}}\) was within 0.1% [10]. Consequently, the difference of the δ (D w) in the two protocols might be mainly caused by reduced chamber-to-chamber variation of k D,X. Analogous to Eq. (3), frequency distribution of the relative difference between N C k D,X and \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\), δ (k D,X) for 14 Farmer-type chambers (30013) is shown in Fig. 5. Mean and σ were −0.77% and 0.32%, respectively. Sakata et al. [8] reported the mean was −0.64% and the σ was 0.41% with 30013 ionization chambers (n = 866). δ (k D,X) in this study shows good agreement with findings of the previous study. Although N D,w was determined 1 year later than N C calibration, change of response between calibration years could be ignored, because the δ (k D,X) of OI’s chamber (−0.37%) was comparable to the δ (k D,X) (−0.43%) determined by the pilot study of N D,w calibration performed 1 year prior by the ANTM and OI [11].

Relative difference between N C, k D,X, and \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\) δ (k D,X) for 30013 Farmer-type chamber
No statistical significance of σ of δ(D w) between JSMP01 and JSMP12 was observed by intercomparison. In contrast, statistical significance of the mean of the δ (D w) between JSMP01 and JSMP12 was observed. Mean of δ (D w) −0.67% in 2011 decreased to −0.15% in 2014. This 0.42% decrease coincides with the difference between mean of δ (k D,X) of RH −0.77% and δ (k D,X) of OI −0.37%, as shown in Fig. 5. Therefore, uncertainty due to chamber-to-chamber variation was reduced by the calibration shift from N C to \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\), and uncertainty of D w in users was consequently reduced.
Conclusion
To evaluate influence of the calibration shift from N C to \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\), the results of a intercomparison before and after the calibration shift were analyzed. The deviation of D w among users was re-evaluated, and the cause of deviation was estimated.
As a result, we confirmed the stability of LINAC, calibration of the thermometer and barometer, and collection method of ion recombination in user hospitals. The statistical significance of D w was not observed, but that of difference of D w among users was observed between N C and \(N_{{{\text{D,w,Q}}_{ 0} }}^{{}}\) calibration. Therefore, uncertainty due to chamber-to-chamber variation was reduced by the calibration shift and the uncertainty of D w among users was consequently reduced. The result also pointed out the uncertainty among users regarding D w might be reduced by accurate and detailed instructions on the setup of an ionization chamber for reference condition.
References
Papanikolaou N, Battista JJ, Boyer AL, Kappas C, Klein E, Mackie TR, et al. American association of physicists in medicine (AAPM) Radiation Therapy Committee Task Group 65: Tissue inhomogeneity corrections for megavoltage photon beams: AAPM report No. 85. Madison: Medical Physics Publishing; 2004.
Andreo P, Burns DT, Hohlfeld K, Huq, Knai T, Laitano F, et al. Absorbed dose determination in external beam radiotherapy: An International Code of Practice for Dosimetry based on Standards of Absorbed Dose to Water: TRS-398 V.12. Vienna: International Atomic Energy Agency; 2006.
Almond PR, Biggs PJ, Coursey BM, Hanson WF, Huq MS, Nath R, et al. AAPM’s TG-51 protocol for clinical reference dosimetry of high-energy photon and electron beams. Med Phys. 1999;26(9):1847–70.
Nishidai T, editor. Standard dosimetry of absorbed dose in external beam radiotherapy. Tsusho Sangyo Kenkyu Sha: Tokyo; 2002.
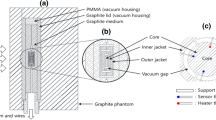
Morishita Y, Kato M, Takata N, Kurosawa T, Tanaka T, Saito N. A standard for absorbed dose rate to water in a 60Co field using a graphite calorimeter at the National Metrology Institute of Japan. Radiat Prot Dosim. 2013;154(3):331–9.
Saitoh H, editor. Standard dosimetry of absorbed dose to water in external beam radiotherapy. Tsusho Sangyo Kenkyu Sha: Tokyo; 2012.
Okuyama H, Sakata S, Fukumura A, Mizuno H. The results of external dose audits for therapeutic high-energy X-rays by ANTM. Jpn J Med Phys. 2015;35(3):88.
Sakata S, Chiryoyou senryokei kousei no jisseki. In: Association for Nuclear Technology in Medicine (ed). Therapy-Level Dosimetry Calibration 4. Tokyo: Association for Nuclear Technology in Medicine; 2014. p. 16–23.
Das IJ, Cheng CW, Watts RJ, Ahnesjö A, Gibbons J, Li XA, et al. Accelerator beam data commissioning equipment and procedures: report of the TG-106 of the Therapy Physics Committee of the AAPM. Med Phys. 2008;35(9):4186–215.
Muir BR, Rogers DWO. Monte Carlo calculations of k Q, the beam quality conversion factor. Med Phys. 2010;37(11):5939–50.
Yajima K, Suoh S, Katayose T, Yamashita W, Takase N, Fukumura A, et al. Comparison of absorbed dose to water calibration factors obtained from in air and in water calibration method. Jpn J Med Phys. 2013;33(3):117.
Acknowledgements
We would like to thank our colleagues and staff of the Radiation Therapy Department of Tokyo Metropolitan Hospitals for their cooperation. This work was partially supported by a JSPS Grant-in-Aid for Scientific Research (c) (Multi-year Fund) Number JP26460729.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest associated with this manuscript.
About this article

Cite this article
Katayose, T., Saitoh, H., Igari, M. et al. Changes in deviation of absorbed dose to water among users by chamber calibration shift. Jpn J Radiol 35, 389–397 (2017). https://doi.org/10.1007/s11604-017-0644-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11604-017-0644-9