
Abstract
Association between fine particulate matter (PM2.5) and respiratory health has attracted great concern in China. Substantial epidemiological evidences confirm the correlational relationship between PM2.5 and respiratory disease in many Chinese cities. However, the causative impact of PM2.5 on respiratory disease remains uncertain and comparative analysis is limited. This study aims to explore and compare the correlational relationship as well as the causal connection between PM2.5 and upper respiratory tract infection (URTI) in two typical cities (Beijing, Shenzhen) with rather different ambient air environment conditions. The distributed lag nonlinear model (DLNM) was used to detect the correlational relationship between PM2.5 and URTI by revealing the lag effect pattern of PM2.5 on URTI. The convergent cross mapping (CCM) method was applied to explore the causal connection between PM2.5 and URTI. The results from DLNM indicate that an increase of 10 μg/m3 in PM2.5 concentration is associated with an increase of 1.86% (95% confidence interval: 0.74%-2.99%) in URTI at a lag of 13 days in Beijing, compared with 2.68% (95% confidence interval: 0.99–4.39%) at a lag of 1 day in Shenzhen. The causality detection with CCM quantitatively demonstrates the significant causative influence of PM2.5 on URTI in both two cities. Findings from the two methods consistently show that people living in low-concentration areas (Shenzhen) are less tolerant to PM2.5 exposure than those in high-concentration areas (Beijing). In general, our study highlights the adverse health effects of PM2.5 pollution on the general public in cities with various PM2.5 levels and emphasizes the needs for the government to provide appropriate solutions to control PM2.5 pollution, even in cities with low PM2.5 concentration.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The health effects associated with fine particulate matter (PM2.5) have attracted great public attention in recent decades. Substantial epidemiological evidences have confirmed the correlation between respiratory disease and a certain time exposure in contaminated air environment (especially PM2.5) for general population (Huang 2014; Cohen et al. 2017; Shaddick et al. 2018; Wang et al. 2018; Burnett et al. 2014). A variety of time series and case-crossover studies are carried out to investigate the short-term health effects of exposures to PM2.5 on the respiratory system by analyzing the variation trend of mortality or healthcare visits in a certain area. Significant associations between PM2.5 pollution episodes and the morbidity as well as the mortality of respiratory diseases are commonly found in cities around the world (Lin et al. 2016; Atkinson et al. 2015; Shang et al. 2013).
In recent decades, PM2.5 pollution has always been a challenging environmental concern in a great number of cities in China (Liu et al. 2016; Song et al. 2017), especially the first-tier cities. Acute upper respiratory disease is one of the most common health issues, whose infection rates could be exacerbated by air pollution (Cheng et al. 2021). The nose and upper respiratory tract act as sentinels in the respiratory system. Inhalation particles of different sizes tend to impact and interact with the upper airway mucosa, thereby resulting in viral infection. Many studies have investigated short-term effects of air pollution on the respiratory infections, and significant associations between PM2.5 levels and respiratory disease have been observed in heavily polluted regions, including Beijing (Li et al. 2018), Shanghai (Chen et al. 2008), Wuhan (Qian et al. 2007), and Lanzhou (Tao et al. 2013). However, evidences in other countries have shown that exposure to PM2.5, even at levels which are not much greater than normal background concentration (e.g., 3–5 μg/m3 in Western Europe), may lead to increased risk of mortality due to respiratory diseases (Kioumourtzoglou et al. 2016; WHO Regional Office for Europe 2013). A similar conclusion has been confirmed in China. Li et al. (2020) found out that short-term PM exposures were associated with increased respiratory diseases among children, even for PM2.5 levels below current Chinese National Ambient Air Quality Standards II in certain cities in China. Yu and Chien (2016) also pointed out that PM2.5 increase at relatively lower levels can increase the same-day respiratory health risks of children under 14 years old in China.
As the rising demands of harmless air environment from the Chinese public, a great number of researches concerning the relationship between air pollution and respiratory health have been conducted nationwide and demonstrated this correlation in cities with various levels of PM2.5 pollution. However, there are still some insufficiency in current researches. On one hand, the most of the researches are conducted in a single city and lack the comparative analysis on effect pattern of PM2.5 among cities with different pollution levels. On the other hand, time series analysis based on the regression model which mainly focuses on the correlational relationship is widely used in current researches; the causal connection between the two is still uncertain. In this research, we intended to investigate the health effect of PM2.5 on the upper respiratory tract in two typical cities with rather different ambient air environment conditions and compare the effect pattern of PM2.5 in distinct levels. Except for exploring the correlational relationship between PM2.5 concentration and upper respiratory diseases using a time series analysis based on the regression model, the causal connection between the two was also detected by applying a model-free method, which helps to distinguish causality from standard correlations.
Methods and materials
Study areas
This study aims to explore the relationship between PM2.5 pollution and acute upper respiratory disease in two typical cities with rather different ambient air environment conditions. For highly polluted city, Beijing where has suffered severe haze weather in recent years is chosen, while for a slightly polluted city, Shenzhen is picked since its air quality is always among the best in China.
Beijing, as the capital city, is the political and economic center of China. Located in the Jing-Jin-Ji metropolitan area which is dominated by heavy industry, Beijing has been deeply affected by the surrounding anthropogenic pollution emissions as a result of the rapid development in this area (Dominici and Mittleman 2012). In addition, the geographical location of Beijing generally tends to prevent the air pollutants from spreading out, which also aggravates the air pollution in Beijing. In view of this, Beijing urban area, including Dongcheng, Xicheng, Chaoyang, Haidian, Fengtai, and Shijingshan), is chosen as the typical area the suffered from heavy air pollution in this study.
Shenzhen, a young city in China, was once praised as an Environmental Protection Model City in 1997 for its favorable air environment. In recent years, as a member of the Pearl River Delta (PRD) region which is one of the most developed regions with the highest aggregation of industry in China, Shenzhen has experienced deterioration in its air environment quality. Influenced by local pollution as well as pollution from surrounding areas, air quality in Shenzhen has deteriorated gradually and affected the living quality of local people to some extent (Xia et al. 2017a, Xia and Yao 2019). However, the air environment condition in Shenzhen is still considered pleasant compared with Beijing (Xia et al. 2017b). In this study, Shenzhen city is chosen as the typical area with mild air pollution for comparison.
Data collection
Daily counts of respiratory illness cases from Jan 1 to Dec 31, 2013, were collected from ten comprehensive hospitals located in urban areas in Beijing (obtained from Xu et al. (2016) ) and 66 major hospitals in Shenzhen City. According to the International Classification of Diseases 10th Revision Code (ICD-10), cases of upper respiratory tract infection (URTI) (ICD-10: J00, J02-J06) were picked out from all the respiratory illness cases. In this study, we only focus on the association between short-term exposure to PM2.5 and URTI, since URTI is generally considered to be associated with the external environment.
Hourly concentrations of PM2.5 are released by the Ministry of Ecology and Environment of the People’s Republic of China (http://air.cnemc.cn:18007), following the Chinese National Ambient Air Quality Standards (GB3095-2012) (MEP 2012). Daily-averaged concentration PM2.5 (μg/m3) data during the study period were collected to represent the degree of the exposure to PM2.5, including data from 17 ambient air quality monitoring stations located in urban areas in Beijing city and 19 stations in Shenzhen City. The spatial distributions of the hospitals and monitoring sites are shown in Figure 1. The rate of the missing values from the 17 monitoring stations in Beijing is relatively high. To solve this problem, we use the linear interpolation method to fill the missing date range when it is less than or equal to 3 days. No missing date is observed in the time series of daily concentration of PM2.5 in Shenzhen during the study period.

Distributions of involved hospitals and monitoring sites in Beijing urban areas and Shenzhen City
Meanwhile, to control for the effects of weather conditions during the same period, daily meteorological data were collected from the official website of the Chinese Meteorological Bureau, including daily mean temperature (°C) and relative humidity daily (%).
Distributed lag nonlinear model
Distributed lag nonlinear model (DLNM) has been widely used to estimate the exposure-response relationship between environmental pollution and diseases in a lot of epidemiological studies (Lall et al. 2010; Shrestha 2007). The exposure-response relationship generally represents the correlational relationship between the level of exposure and the occurrence of certain diseases of the human body.
Based on the generalized additive model, DLNM is developed to evaluate the lag effect by involving a detailed time-course representation of the exposure-response relationship (Gasparrini et al. 2010). The main advantage of the DLNM is that it is able to provide an estimate of the cumulative lag effect as the sum of the single-day lag effect upon the whole period. Considering the confounding factors, penalized smoothing splines of calendar time and metrological conditions (temperature, relative humidity) were added to improve the performance of the model. Degrees of freedom (df) for the smoothers are determined using the generalized the cross validation until the sum of absolute difference reached the minimum. In this study, df for calendar time is set to 7, and df for temperature and relative humidity is set to 3 in both two study areas to account for the potential nonlinear effects. We also include two dummy variables for the day of the week and holiday, respectively. The model is of the form:
where t is the day of observation; Xt − L represents the concentration of PM2.5 on L days ahead day t; E(Yt) is the expected number of cases on day t; α is the intercept term; β represents the log-relative risk (RR) of cases associated with a unit increase of PM2.5.; S(time, df) and S(Zt, df) are the penalized smoothing splines of calendar time and metrological conditions (temperature, relative humidity); and DOW and Holiday stand for the day of week and holiday with βw and βh as the corresponding coefficients.
To perform the model, DLNM and Mixed GAM Computation Vehicle (MGCV) packages in R (Wood 2017) were used. All results are presented as relative risk (RR) or percent change in daily case amount and its 95% confidence interval (CI) in association with a 10-μg/m3 increase of PM2.5 concentration.
Convergent cross mapping method
The convergent cross mapping (CCM) method is the first proposed by Sugihara and May (1990) to deal with the illusory correlation in the complex system. It helps in distinguishing the causality from standard correlations between pairs of time series (at least 25 observations) (Maher and Hernandez 2015).
Based on Takens’ theorem, the CCM algorithm is model-free and robust to unmeasured confounding which may induce false associations (Deyle and Sugihara 2011). It allows reconstructing high dimensional system dynamics with a time series of a single variable under mild assumptions. In CCM, the complex and nonlinear systems are analyzed through state-space reconstruction, which has advantages in solving problems in various fields, e.g., wildlife management and cerebral autoregulation (Vanderweele and Arah 2011). Unlike the most frequently used Granger causality analysis (Granger 1980) which behaves poorly in a weak-to-moderate coupling, CCM is more suitable for detecting illusory correlation and revealing potential causality in complex ecosystems (Sugihara et al. 2012).
Giving two time series of variables X {x1,x2,…,xL} and Y{y1,y2,…yL} (L is the length of time period), dimension E in which the reconstructed attractor is embedded and time lag τ, CCM algorithm is implemented in the following steps:
-
Step 1.
Rebuild the shadow manifold Mx and My from the lagged-coordinate vectors X and Y, which is:
where t = 1+(E-1) τ to t = L. A small region around yt will map to a small region around xt to estimate xt since My is diffeomorphic to Mx. Note that at least E+1 points are needed to form a bounding simplex around yt (Sugihara and May 1990).
-
Step 2.
Create a cross mapped estimation of yt, denoted by \( {\hat{y}}_t\left|{M}_x\right. \). Firstly, find the simultaneous lagged-coordinate vector on Mx, x(t) and its E + 1 nearest neighbors. For each x(t), the nearest neighbor search gets a set of distances sorted from the closest to the outermost by an associated set of time {t1,t2,…,tE+1}. The distance d[x(t), x(s)] is measured by the Euclidean distance between the two vectors.
-
Step 3.
Calculate with a weighted mean the nearest neighbors in My. The weight wi is defined as:
where
-
Step 4.
Explore neighbors in y with {t1, t2, …, tE+1}. The estimate of yt is a locally weighted mean of the E+1, and \( {y}_{t_i} \) is calculated as:
-
Step 5.
. Calculate the CCM correlation. The Pearson correlation coefficient between original and estimated time series is expressed as:
Meanwhile, a t-statistic for correlation coefficient at a level of significance is calculated as:
where N is the length of the time series process. The Pearson correlation coefficient ρYX between the L true values from Y, and the L cross mapped estimates are an indicator of how much the dynamics of Y impacts the dynamics of X (Dan et al. 2017).
For CCM method, E and τ are two important parameters which need to be optimized. Based on previous findings, CCM is suggested to be insensitive to the manual setting of parameters and can extract reliable causality between diverse variables (Chen et al. 2017). Assuming that Emax is the optimal dimension, Whitney’s theorem indicates that the dimensionality is generically between (Emax −1)/2 and Emax (Deyle and Sugihara 2011). In this study, dimension (E) from the two times series equals 2 using the false nearest neighbor method, and the value of τ is set to 2 based on the average mutual information criterion for both study areas.
Results and discussion
Descriptive statistics
A total of 51134 and 18354 URTI cases were recorded, respectively, from the hospitals in Beijing and Shenzhen in 2013. Table 1 summarizes the statistical characteristics of URTI, PM2.5 concentration, and meteorological factors in Beijing and Shenzhen in 2013. The daily mean count of URTI was 140 in Beijing (ranged from 65 to 347) and 50 in Shenzhen (ranged from 1 to 87). The time series graph in Figure 2 shows the daily variations of URTIs and PM2.5 concentrations in 2013.

Time series graph of URTI (number of daily cases) and daily PM2.5 concentrations in (a) Beijing and (b) Shenzhen in 2013
During the study period, the overall daily mean PM2.5 concentration was 102 μg/m3 (ranged from 6.7 μg/m3 to 508.5 μg/m3) in Beijing and 37 μg/m3 (ranged from 7.9 μg/m3 to 129.8 μg/m3) in Shenzhen. Referring to the Chinese Ambient Air Quality Standards (Grade II, 75 μg/m3 for 24-hour average PM2.5 concentration), 45.7% (155 days) of the daily PM2.5 concentrations in Beijing and 88% (321 days) in Shenzhen were below the standard. While referring to the WHO Air Quality Standards (25 μg/m3 for 24-h average PM2.5 concentration), only 30 days in Beijing and 120 days in Shenzhen met the standard. Judging by the number of days which meet the two kinds of standard, PM2.5 pollution in Beijing was much more severe than that in Shenzhen in 2013. In addition, meteorological conditions in the two cities are also different. Located in relatively lower latitudes, Shenzhen has a warmer and wetter climate than Beijing.
The lag effect of PM2.5 on URTI
To explore the lagged health effect of PM2.5 on the upper respiratory tract of the human body, a time series analysis based on DLNM was carried out. We investigated the lag effect of PM2.5 up to a lag of 7 days in Shenzhen and 14 days in Beijing. There were clear exposure-response relationships between PM2.5 concentration and URTI cases. As shown in Figure 3, the exposure-response patterns for Beijing and Shenzhen are both approximately linear, with slight fluctuations when the PM2.5 concentrations are below a certain value (300 μg/m3 for Beijing and 70 μg/m3 for Shenzhen) and a sharper rise at higher PM2.5 concentrations. Different patterns of response at the same PM2.5 levels are observed in the two study areas, which implies that citizens in Shenzhen are more sensitive to PM2.5 exposure while citizens in Beijing are more tolerant to PM2.5 exposure.

Smoothed exposure-response graph of daily mean PM2.5 concentrations at a lag of 0–1 day against the risk of URTI. The X-axis shows the moving averages of PM2.5 concentrations. The Y-axis is the predicted relative risk (RR). The red line represents central estimates, and the grey-shaded area represents the 95% CI
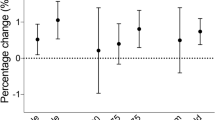
In this study, the DLNM was applied to evaluate the effects of PM2.5 on the upper respiratory track as a linear exposure-response relationship between them. The relative risk for URTI was denoted as a change in the number of daily URTI cases associated with a 10-μg/m3 increase of PM2.5 concentration. The resulting exposure-response patterns for both single-day lag effect and cumulative lag effect are shown in Figure 4, with black bars and gray areas representing the 95% CI. The cumulative lag effect was obtained by applying a polynomial curve fitting on single-day lag effect at a degree of 3.

Lag-response relationship between PM2.5 and relative risk (RR) of URTI for (a) single-day lag effect in Beijing, (b) cumulative lag effect in Beijing, (c) single-day lag effect in Shenzhen, and (d) cumulative lag effect in Shenzhen
Table 2 and Table 3 show the relative risk for URTI associated with a 10-μg/m3 increase in PM2.5, together with the 95% CI in Beijing urban area and Shenzhen City. For Beijing urban area, significant single-day lag effects were observed at a lag ranging from 6 days to 12 days, with the maximum appeared at a lag of 10 days; significant cumulative lag effects appeared at a lag of 6 days and remained significant until a lag of 14 days. For Shenzhen City, a significant single-day lag effect was only observed at a lag of 1 day, and significant cumulative lag effects were observed at a lag ranging from 1 day to 5 days. Considering the cumulative lag effect, each 10-μg/m3 increase in PM2.5 concentration was maximally associated with 1.86% (95%CI: 0.74–2.99%) and 2.68% (95%CI: 0.99–4.39%) increase in URITs in Beijing (at a lag of 13 days) and Shenzhen (at a lag of 1 day), respectively.
Although significant lag effects were detected in both two study areas, the lag patterns were quite different. The lag effect of PM2.5 on URTI in Beijing was more delayed and lasts longer than that in Shenzhen. Judging by the RR values, the same amounts of increases in PM2.5 concentration in Shenzhen had a greater effect on URTI than in Beijing.
This section focused on the comparison of the exposure-response relationship between PM2.5 and URTI in a highly polluted area and a slightly polluted area. It was found out that, after a short-term exposure in PM2.5, response on URTI in the slightly polluted area (Shenzhen) was more significant than in the highly polluted area (Beijing), in terms of response time and degree of effect.
The causative influence of PM2.5 on URTI
The lag effect analysis using DLNM in section 3.2 is a regression analysis which can only detect whether the two variables have a correlational relationship. However, correlation does not mean causality [33]. To explore the causative influence of PM2.5 on URTI, a time series analysis based on the CCM method was applied.
The convergent cross maps of Beijing urban area and Shenzhen City are shown in Figure 5, where the red lines represent the causative influence of the number of URTI cases on PM2.5 concentrations while the blue lines represent the opposite. The ρ value itself cannot indicate the positive or negative impact, and only the positive ρ value with a stable convergent trend implies the causative impact may exist between the two variables. Significant convergent patterns of blue lines are observed for two study areas, indicating that PM2.5 concentration causatively impacts the number of URTI in Beijing and Shenzhen. While regard to the red lines, no significant patterns were detected, which implies that the number of URTI has no impact on PM2.5 concentration. This logical result also verifies the feasibility and effectiveness of CCM method. Quantitative results (ρ value) in Table 4 represent the strength of the causative impact, and it shows that the strength of the impact in Shenzhen is larger than that in Beijing.

Convergent cross maps demonstrating the causality between PM2.5 concentration and URTI in (a) Beijing and (b) Shenzhen in 2013. PM2.5-URTI indicates the influence of PM2.5 on URTI, and URTI-PM2.5 is the opposite
Comparative discussions on the finding
Significant associations between PM2.5 concentration and URTI cases in terms of correlation relationship as well as causal connection were both observed in Beijing urban area and Shenzhen City. That is, short-term exposure to PM2.5 does have a significant adverse effect on the upper respiratory track of the general population regardless of the pollution level of PM2.5. However, when concerning the effect patterns, such as the lag period and strength of effect, it shows quite different outcomes. The results from DLNM and CCM both show that the strength of the impact of PM2.5 in Shenzhen City is larger than that in Beijing urban areas. This finding is consistent with other studies carried out in China and other countries. Table 5 summarizes the findings in relevant studies concerning the associations between PM2.5 and respiratory disease in recent years.
Table 5 contains the study area, PM2.5 level, increased percent of the respiratory disease (including the number of all diseases, number of upper respiratory infection, mortality of all disease) from the recent studies, and they are arranged in the order of PM2.5 level from low to high. We can see that increased risks in the study areas with lower PM2.5 levels are generally higher than those with higher PM2.5 levels. For mortality of all respiratory disease, for each 10-μg/m3 increase in PM2.5 concentration, it showed 2.0–4.01% (95% CI: 0.15–7.52%) increases in Tokyo, Shenzhen, and Zhuhai (mean PM2.5: 16.0–34.23 μg/m3), 0.90–0.97% (95% CI: 0.01–1.94%) increases in Hefei and Shenyang (mean PM2.5: 66.18–75 μg/m3), while only 0.63% (95% CI: 0.07–1.19%) increase in Shijiazhuang (mean PM2.5: 118.8 μg/m3). Besides, for numbers of all respiratory disease, each 10-μg/m3 increase in PM2.5 concentration showed 1.06–1.19% (95% CI: 0.20–2.19%) increases in Shenzhen and Guangzhou (mean PM2.5: 23.7–35.8 μg/m3), 0.53–0.73% (95% CI: 0.22–0.87%) increases in Shanghai and Lanzhou (mean PM2.5: 55.5–61.11 μg/m3), while only 0.23–0.57% (95% CI: 0.02–0.66%) increases in Chengdu and Jinan (mean PM2.5: 96.9–100 μg/m3). As for upper respiratory infection, for each 10-μg/m3 increase in PM2.5 concentration, it showed 4.8% (95% CI: 2.8–6.9%) in Korea (mean PM2.5: 21.1 μg/m3), 2.68% (95% CI: 0.99–4.39%) in Shenzhen (mean PM2.5: 50 μg/m3), while 1.86% (95% CI: 0.74–2.99%) in Beijing (mean PM2.5: 140 μg/m3). A systematic review study conducted by Sun et al. (2020) similarly found out that a low increased risk of respiratory disease (0.62%, 95% CI: 0.57–0.66%) was identified at a high level of annual mean PM2.5 concentrations (41.36–110.80 μg/m3 ) with 1.82% (95% CI: 1.72–1.92%) at a low level of annual mean PM2.5 concentrations (29.86–40.20 μg/m3 ), which can also support the finding in this study.
Conclusions
In this study, a comparative analysis on the health effect of PM2.5 is conducted in two typical cities with different pollution levels, by applying time series analysis based on the DLNM and CCM method. Both correlational relationship and causal connection between PM2.5 concentration and URTI cases are detected in two study areas. In addition, the results from DLNM and CCM method consistently show that the strength of the impact of PM2.5 in Shenzhen is larger than that in Beijing, which implies that people living in low-concentration areas (Shenzhen) are less tolerant to PM2.5 exposure than those in high-concentration areas (Beijing). In conclusion, our study highlights the adverse health effects of PM2.5 pollution on the general public in cities with various PM2.5 levels in China and emphasizes the need for the government to provide appropriate solutions to control PM2.5 pollution, even in cities with low PM2.5 levels.
Availability of data and materials
All data generated or analyzed during this study in this article are available from the corresponding author on reasonable request.
References
Atkinson RW, Mills IC, Walton HA, Anderson HR (2015) Fine particle components and health: a systematic review and meta-analysis of epidemiological time series studies of daily mortality and hospital admissions. J Expo Sci Environ Epidemiol 25:208–214
Burnett RT, Pope CR, Ezzati M, Olives C, Lim SS, Mehta S, Shin HH, Singh G, Hubbell B, Brauer M, Anderson HR, Smith KR, Balmes JR, Bruce NG, Kan H, Laden F, Prüss-Ustün A, Turner MC, Gapstur SM, Diver WR, Cohen A (2014) An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ Health Perspect 122:397–403
Cai J, Peng C, Yu S, Pei Y, Liu N, Wu Y, Fu Y, Cheng J (2019) Association between PM2.5 exposure and all-cause, non-accidental, accidental, different respiratory diseases, sex and age mortality in Shenzhen, China. Int J Environ Res Public Health 16(3):401
Chai G, He H, Sha Y, Zhai G, Zong S (2019) Effect of PM2.5 on daily outpatient visits for respiratory diseases in Lanzhou, China. Sci. Total Environ 649:1563–1572
Chen G, Song G, Jiang L, Zhang Y, Zhao N, Chen B, Kan H (2008) Short-term effects of ambient gaseous pollutants and particylate matter on daily mortality in Shanghai. China J Occup Health 50:41–47
Chen Z, Cai J, Gao B, Xu B, Dai S, He B, Xie X (2017) Detecting the causality influence of individual meteorological factors on local PM2.5 concentration in the Jing-Jin-Ji region. Sci Rep 7(1):40735
Cheng J, Su H, Xu Z (2021) Intraday effects of outdoor air pollution on acute upper and lower respiratory infections in Australian children. Environ Pollut 268:115698
Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, Balakrishnan K, Brunekreef B, Dandona L, Dandona R, Feigin V, Freedman G, Hubbell B, Jobling A, Kan H, Knibbs L, Liu Y, Martin R, Morawska L, Pope CA III, Shin H, Straif K, Shaddick G, Thomas M, van Dingenen R, van Donkelaar A, Vos T, Murray CJL, Forouzanfar MH (2017) Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study. Lancet 389(10082):1907–1918
Dan M, Fusaroli R, Tylén K, Roepstorff A, Sherson JF (2017) Causal inference from noisy time-series data — testing the convergent cross-mapping algorithm in the presence of noise and external influence. Futur Gener Comput Syst 73:52–62
Deyle ER, Sugihara G (2011) Generalized theorems for nonlinear state space reconstruction. PLoS One 6(3):e18295
Dominici F, Mittleman MA (2012) China’s air quality dilemma: reconciling economic growth with environmental protection. JAMA 307(19):2100–2102
Duan Z, Gao X, Du H, Qin F, Chen J, Ju Y (2015) Analysis on the relationship between PM2.5 concentration in ambient air and hospital outpatients with respiratory diseases in Chengdu. Mod. Prev. Med. 42(4):611–614
Feng J, Sun H, Du Y, Zhang X, Di H (2018) Analysis on the acute effects of PM2.5 pollutants concentration on mortality of residents in Shijiazhuang. Mod Prev Med 45(4):603–608
Gasparrini A, Armstrong B, Kenward MG (2010) Distributed lag non-linear models. Stat Med 29(21):2224–2234
Granger CWJ (1980) Testing for causality: a personal viewpoint. J Econom Dyn Contro 2:329–352
Huang YC (2014) Outdoor air pollution: a global perspective. J Occup Environ Med 56:S3–S7
Kim KN, Kim S, Lim YH, Song IG, Hong YC (2020) Effects of short-term fine particulate matter exposure on acute respiratory infection in children. Int J Hyg Environ Health 229:113571
Kioumourtzoglou MA, Schwartz J, James P, Dominici F, Zanobetti A (2016) PM2.5 and mortality in 207 US cities: Modification by temperature and city characteristics. Epidemiology 27:221–227
Lall R, Ito K, Thurston G (2010) Distributed lag analyses of daily hospital admissions and source-apportioned fine particle air pollution. Environ Health Perspect 119(4):455–460
Li Y, Ma Z, Zheng C, Shang Y (2015) Ambient temperature enhanced acute cardiovascular-respiratory mortality effects of PM2.5 in Beijing China. Int J Biometeorol 59(12):1761–1770
Li T, Yan M, Sun Q, Anderson GB (2018) Mortality risks from a spectrum of causes associated with wide-ranging exposure to fine particulate matter: a case-crossover study in Beijing, China. Environ Int 111:52–59
Li M, Tang J, Yang H, Zhao L, Liu Y, Xu H, Fan Y, Hong J, Long Z, Li X, Zhang J, Guo W, Liu M, Yang L, Lai X, Zhang X (2020) Short-term exposure to ambient particulate matter and outpatient visits for respiratory diseases among children: a time-series study in five Chinese cities. Chemosphere 263:128214
Lin H, Ma W, Qiu H, Vaughn MG, Nelson EJ, Qian Z, Tian L (2016) Is standard deviation of daily PM2.5 concentration associated with respiratory mortality? Environ Pollut 216:208–214
Lin H, Liu T, Xiao J, Zeng W, Li X, Guo L, Xu Y, Zhang Y, Vaughn MG, Nelson EJ, Qian Z, Ma W (2016b) Quantifying short-term and long-term health benefits of attaining ambient fine particulate pollution standards in Guangzhou. China Atmos Environ 137:38–44
Liu M, Huang Y, Ma Z, Jin Z, Liu X, Wang H, Liu Y, Wang J, Jantunen M, BiDr J, Kinney PL (2016) Spatial and temporal trends in the mortality burden of air pollution in China: 2004–2012. Environ Int 98:75–81
Liu J, Li Y, Li J, Liu Y, Tao N, Song W, Cui L, Li H (2019) Association between ambient PM2.5 and children’s hospital admissions for respiratory diseases in Jinan, China. Environ Sci Pollut Res 26:24112–24120
Lu F, Liu Y, Li X, Dong S (2017) A case-crossover study on air pollution and outpatient visits for respiratory diseases. J Environ Hyg 7(5):408–412
Ma Y, Chen R, Pan G, Xu X, Song W, Chen B, Kan H (2011) Fine particulate air pollution and daily mortality in Shenyang, China. Sci Total Environ 409(13):2473–2477
Maher MC, Hernandez RD (2015) CauseMap: fast inference of causality from complex time series. PeerJ 3:e824
Michikawa T, Yamazaki S, Ueda K, Yoshino A, Sugata S, Saito S, Hoshi J, Nitta H, Takami A (2020) Effects of exposure to chemical components of fine particulate matter on mortality in Tokyo: a case-crossover study. Sci Total Environ 755:142489
Ministry of Environmental Protection of the People’s Republic of China (MEP) (2012) Ambient Air quality standards (on trial). in national environmental protection standards of the People’s Republic of China, GB3095 edn. Ministry of Environmental Protection of the People’s Republic of China (MEP), Beijing
Qian Z, He Q, Lin HM, Kong L, Liao D, Yang N (2007) Short-term effects of gaseous pollutants on cause-specific mortality in Wuhan, China. J Air Waste Manage Assoc 57:785–793
Ren Z, Liu X, Liu T, Chen D, Jiao K, Wang X, Suo J, Yang H, Liao J, Ma, L. (2020) Effect of ambient fine particulate (PM2.5) on hospital admissions for respiratory and cardiovascular diseases in Wuhan, China. Res Square.
Shaddick G, Thomas ML, Amini H, Broday D, Cohen A, Frostad J, Green A, Gumy S, Liu Y, Martin RV, Pruss-Ustun A, Simpson D, van Donkelaar A, Brauer M (2018) Data integration for the assessment of population exposure to ambient air pollution for global burden of disease assessment. Environ Sci Technol 52(16):9069–9078
Shang Y, Sun Z, Cao J, Wang X, Zhong L, Bi X (2013) Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality. Environ Int 54:100–111
Shrestha SL (2007) Time series modelling of respiratory hospital admissions and geometrically weighted distributed lag effects from ambient particulate air pollution within Kathmandu Valley. Nepal Environ Model Assess 12(3):239–251
Song C, He J, Wu L, Jin T, Chen X, Li R, Ren P, Zhang L, Mao H (2017) Health burden attributable to ambient PM 2.5 in China. Environ Pollut. 223:575–586
Sugihara G, May RM (1990) Nonlinear forecasting as a way of distinguishing chaos from measurement error in time series. Nature 344(6268):734–741
Sugihara G, May R, Ye H, Hsieh C, Deyle E, Fogarty M, Munch S (2012) Detecting causality in complex ecosystems. Science 338:496–500
Sui X, Zhang J, Zhang Q, Sun S, Lei R, Zhang C, Cheng H, Ding L, Ding R, Xiao C, Li X, Cao J (2021) The short-term effect of PM 2.5/O 3 on daily mortality from 2013 to 2018 in Hefei, China. Environ Geochem Health 43(1):153–169
Sun J, Zhang N, Yan X, Wang M, Wang J (2020) The effect of ambient fine particulate matter (PM2.5) on respiratory diseases in China: a systematic review and meta-analysis. Stoch Env Res Risk A 34:593–610
Tao Y, Mi S, Zhou S, Wang S, Xie X (2013) Air pollution and hospital admissions for respiratory diseases in Lanzhou, China. Environ Pollut 185:196–201
Vanderweele TJ, Arah OA (2011) Bias formulas for sensitivity analysis of unmeasured confounding for general outcomes, treatments, and confounders. Epidemiology 22:42–52
Wang J, Chen S, Zhu M, Miao C, Song Y, He H (2018) Particulate matter and respiratory diseases: How Far have We gone? J Pulm Respir Med 8(4):465
WHO Regional Office for Europe (2013) Review of evidence on health aspects of air pollution—REVIHAAP Project. WHO Regional Office for Europe, Copenhagen, pp 38–41
Wood, S.N. Generalized additive models: an introduction with R, (2nd ed.). Chapman and Hall/CRC. 2017. https://doi.org/10.1201/9781315370279
Wu H, Tan A, Huang L, Xiao W, Liang X, Ning T (2017) Time-series analysis on association between atmospheric pollutants and daily mortality among residents in Zhuhai. J Environ Health 34(9):797–800
Xia X, Yao L (2019) Spatio-temporal differences in health effect of ambient PM2.5 pollution on acute respiratory infection between children and adults. IEEE Access 7:25718–25726
Xia X, Zhang A, Liang S, Qi Q, Jiang L, Ye Y (2017a) The association between air pollution and population health risk for respiratory infection: a case study of Shenzhen, China. Int J Environ Res Public Health 14(9):950
Xia X, Qi Q, Liang H, Zhang A, Jiang L, Ye Y, Liu C, Huang Y (2017b) Pattern of spatial distribution and temporal variation of atmospheric pollutants during 2013 in Shenzhen, China. ISPRS Int J Geo-Inf 6(1):2
Xu Q, Li X, Wang S, Wang C, Huang F, Gao Q, Wu L, Tao L, Guo J, Wang W, Guo X (2016) Fine particulate air pollution and hospital emergency room visits for respiratory disease in urban areas in Beijing, China, in 2013. PLoS One 11(4):e0153099
Yang C, Yang X, Shen X (2017) A time-series study on association between ambient air pollutants and hospital outpatients in a district of Shanghai. J Environ Occup Med 34(3):235–238
Yang H, Yan C, Li M, Zhao L, Long Z, Fan Y, Zhang Z, Chen R, Huang Y, Lu C, Zhang J, Tang J, Liu H, Liu M, Guo W, Yang L, Zhang X (2021) Short term effects of air pollutants on hospital admissions for respiratory diseases among children: a multi-city time-series study in China. Int J Hyg Environ Health 231:113638
Yu H, Chien L (2016) Short-term population-based non-linear concentration-response associations between fine particulate matter and respiratory diseases in Taipei (Taiwan): a spatiotemporal analysis. J Expo Sci Environ Epidemiol 26(2):197–206
Yu Y, Yao S, Dong H, Wang L, Wang C, Ji X, Ji M, Yao X, Zhang Z (2018) Association between short-term exposure to particulate matter air pollution and cause-specific mortality in Changzhou, China. Environ Res 170:7–15
Zhang Y, Ding Z, Xiang Q, Wang W, Huang L, Mao F (2019) Short-term effects of ambient PM1 and PM2.5 air pollution on hospital admission for respiratory diseases: case-crossover evidence from Shenzhen, China. Int J Hyg Environ Health 224:113418
Zhu F, Chen L, Qian Z, Liao Y, Zhang Z, McMillin SE, Wang X, Lin H (2021) Acute effects of particulate matter with different sizes on respiratory mortality in Shenzhen, China. Environ Sci Pollut Res Int 28:37195–37203
Funding
This work is jointly supported by grants from the National Natural Science Foundation of China (grant number 41771380), Key Special Project for Introduced Talents Team of Southern Marine Science and Engineering Guangdong Laboratory (grant number GML2019ZD0301), the GDAS’ Project of Science and Technology Development (grant numbers 2020GDASYL-20200103003, 2020GDASYL-20200103006), the China Postdoctoral Science Foundation (grant number 2020M682628), a grant from State Key Laboratory of Resources and Environmental Information System, the National Postdoctoral Program for Innovative Talents (grant number BX20200100), China, and the Open Research Fund of National Earth Observation Data Center (grant number NODAOP2020002).
Author information
Authors and Affiliations
Contributions
XX and LY developed the concept of research work. XX, LY, and JL conceived and designed the study, collected the data, and carried out research works. XX and JL analyzed the data. LY provided oversight for the research. XX prepared the initial draft of the manuscript. YXL, WJ, and YL revised the subsequent versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Xia, X., Yao, L., Lu, J. et al. Observed causative impact of fine particulate matter on acute upper respiratory disease: a comparative study in two typical cities in China. Environ Sci Pollut Res 29, 11185–11195 (2022). https://doi.org/10.1007/s11356-021-16450-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-021-16450-5