
Abstract
Recent epidemiological studies pointed out that air pollution has a significant impact on pediatric asthma. Shanghai is one of the biggest cities in China, and the short-term effect of atmospheric particulate matter on the incidence of pediatric asthma has become a hot topic. From January 1, 2009, to December 31, 2010, we used daily measurements of pollutant concentrations, daily weather data, and daily records of pediatric asthma hospital visits from local authorities to evaluate the short-term effect of air pollution on pediatric asthma incidence in Shanghai, China. We used a generalized additive model (GAM) in the analysis, and the controlled confounding factors include long-term trends, day-of-the-week effects, and weather elements. We divided the entire study group into different age-subgroups. In addition, we took a variety of lag models into consideration. The results showed a strong connection between concentrations of fine particulate matter (PM2.5) and pediatric asthma hospital visits from 2009 to 2010 in Shanghai, China. For the entire study group, the greatest relative risk (RR) of PM2.5 on pediatric asthma hospital visits was 1.060 on a lag of 4 days. As for the three different age-subgroups, the greatest RR of PM2.5 on pediatric asthma hospital visits was 1.061 (at a lag of 5 days), 1.071 (at a lag of 4 days), and 1.052 (at a lag of 2 days), for the under-2-year-olds, 3-to-5-year-olds, and the 6-to-18-year-olds, respectively. The overall short-term effect of PM2.5 on pediatric asthma hospital visits was relatively stronger in younger children. Within the year, we detected the strongest seasonal effect of PM2.5 on pediatric asthma hospital visits in Summer. When adding other air pollutants in the analysis model, RR of PM2.5 on pediatric asthma hospital visits would be increased.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In recent years, due to the fast development of urbanization in China, PM2.5 has rapidly become a serious problem (Wang et al. 2017). Previous epidemiological studies have pointed out that PM2.5 has a great impact on human health (Kioumourtzoglou et al. 2016; Bell et al. 2007 and Schlesinger 2007; Shi et al. 2016). Especially, PM2.5 has a strong impact on the incidence of respiratory diseases (Polezer et al. 2018; Liu et al. 2016; Hakantecer et al. 2008). From 1996 to 2016, the prevalence and severity of asthma have significantly increased around the world (Maio et al. 2016), and the affected population was up to 300 million (Torgerson et al. 2011). Generally, children are more susceptible to asthma than adults (Guyatt et al. 1997). In the USA, the under-4-year-olds account for 71.8% of the total patients with persistent asthma (Zahran et al. 2014). Asthma has been found to be associated with several environmental factors such as air temperature and vapor pressure (Ito et al. 1992), as well as fine particulate matter (Peng et al. 2008).
Worldwide, many studies have been conducted to explore the correlations between fine particulate matter and asthma incidence (Yun et al. 2002; An 2013; Han et al. 2014). As compared with coarse PM, fine PM are more closely related to the increase of asthma prevalence and morbidity (Keet et al. 2018). Several researches found that PM1.0 were closely associated with climate, air quality, and human health (Zang et al. 2018; Zang et al. 2019; Zou et al. 2017). Although people began to pay attention to and monitor PM1.0, studies on the relationship between PM1.0 and health are still rare. For example, in Canada, the relative risk of asthma incidence increased by 2.24% (95% confidence interval (95% CI) 0.93–5.38) for per 10 μg/m3 increase in concentrations of PM2.5 every 2 years from 2007 to 2014 in 117 populated areas (Requia et al. 2017). In the USA, pediatric asthma incidence would increase by 0.9% with each interquartile range (IQR) (6.7 μg/m3) of PM2.5 of the previous day in an agricultural community in Washington State; meanwhile, the forced expiratory volume during the first second of the forced breath (FEV1) for these affected children would drop by 0.9% (Loftus et al. 2015). The lag effect of PM2.5 on asthma incidence for the entire population in the USA occurred at lag 1 day, however, the lag was at 1 to 3 days for the African American population (Glad et al. 2012). The effect of (outdoor) atmospheric particulate matter (5.0 ppb per 10 μg/m3 increase in PM2.5) on asthma incidence is usually stronger than that of indoor particulate matter (3.3 ppb per 10 μg/m3 increase in PM2.5) (Koenig et al. 2005). In particular, traffic-related PM2.5 emission is a major concern, which was found to be positively correlated with asthma exacerbation for children in the USA (Spira-Cohen et al. 2009). When children are exposed to PM2.5 that is direct emission from traffic, the cases of asthma symptoms would keep increasing until reaching a peak at lag 3 days (Gent et al. 2009). For every 5 μg/m3 increase in the concentrations of PM2.5, the odds ratio (OR) of wheezing and shortness of breath would increase by 1.16 (95% CI 1.11–1.21) and 1.61 (95% CI 1.45–1.78), respectively (Dany et al. 2017).
In China, the impact of PM2.5 on asthma incidence has become a hot topic in recent years. From 1997 to 2002, PM2.5 was closely related to pediatric asthma admission rates for the under-18-year-olds in Hong Kong; when the concentrations of PM2.5 increased by 20.6 μg/m3, asthma-related admission rate for the under-18-year-olds would increase by 3.24% (95% CI 0.93–5.60) (Lee et al. 2006). In Shanghai, childhood asthma prevalence has significantly increased (Shanghai Medical Association Pediatric Professional Committee Respiratory Group 2014), which is closely related to PM2.5 (Pan and Kuai 2017). From 2007 to 2010, childhood asthma prevalence for the 6–14-year-olds increased from 5.92 to 10% in Shanghai (Yuan et al. 2007). For every 10 μg/m3 increase in PM2.5, the number of pediatric asthma patients for the 3-to-14-year-olds would increase by 0.78% (95% CI 0.16–1.4) in Shanghai (Mo et al. 2014). However, a comprehensive study on the effect of PM2.5 on childhood asthma prevalence for different age groups on different timescales in Shanghai has not yet been reported.
In this study, we assumed that PM2.5 has a hysteresis effect on childhood asthma prevalence in Shanghai, China. Based on the daily data (including hospital visit records, weather data, and the air quality data) from January 1, 2009, to December 31, 2010, we analyzed the short-term effect of PM2.5 on pediatric asthma hospital visits in Shanghai, China. We divided the entire study group into different age-subgroups and ran the analysis for a total of five timescales, including annual, Spring (from March to May), Summer (from June to August), Autumn (from September to November), and Winter (from December to the next February). As for the hysteresis effect, we used both single- and multi-pollutant models to estimate the relative risk of PM2.5 on pediatric asthma hospital visits at lag of 0–6 days (i.e., from the current day to the previous 6 days). By providing a comprehensive report on the short-term effect of PM2.5 on childhood asthma prevalence in Shanghai, China, our goal is to assist local health and human service authorities to reduce asthma prevalence in children.
Data and methods
Study area and data
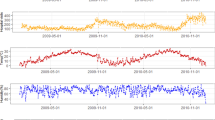
Shanghai (121° 48′ E, 31° 22′ N) is located in eastern China, and the total resident population was about 24.2 million in 2017. Shanghai has a subtropical humid maritime monsoon climate, with an annual average air temperature of 17.7 °C and humidity of 69.4%. Based on the data availability, our study focuses on the period of January 1, 2009, to December 31, 2010. We obtained the daily average concentrations of air pollutants (i.e., PM2.5, PM10, SO2, and NO2) from the Shanghai Environmental Protection Bureau. We collected the daily weather data from the Shanghai Meteorological Bureau, including average air temperature (°C), wind speed (m/s), air pressure (hPa), and relative humidity (%). We acquired daily records of asthma-related hospital visits from the Shanghai Medical Insurance Affairs Management Center, including date of visit, age, sex, and diagnosis code. These daily medical records cover all the patients that have social medical insurance. It is required by the law for every resident to have social medical insurance, whether as a primary or secondary health insurance. Therefore, the acquired daily hospital visit records represent the entire resident population in Shanghai, China. In this study, we divided the entire study group into three age-subgroups, including the under-2-year-olds, the 3-to-5-year-olds, and the 6-to-18-year-olds.
Methods
We used a generalized additive model (GAM, Eq. (1)) (Samet et al. 2000) in the time series analysis to evaluate the short-term effect of PM2.5 on pediatric asthma hospital visits in Shanghai, China. We chose the relative risk (RR) as the index, which is the ratio of morbidity or mortality in the exposed and non-exposed groups. RR is an indicator of the extent to which the exposed research object is susceptible to a certain disease (asthma in this study). We presented the RR values as well as the 95% CI for per IQR increase in PM2.5 (Ma et al. 2018; Wang et al. 2012; Kan et al. 2008).
where Yi is the number of respiratory disease emergency department visits on day i, E(Yi) is the expected emergency department visits on day i; α is the intercept; β is the coefficient of exposure response; Xi is the explanatory variable that produces a linear effect; DOW is day of the week; holiday includes all statutory holidays; s is a nonparametric smoothing function; df is degree of freedom; PM10 indicates the average concentrations of PM10 at a df of 4; time is the calendar date variable, ranging from 1 to 730, with a df of 3; N is the child population from 2009 to 2010 in the study area, with a df of 3; T is daily average air temperature, with a df of 4; P is daily average air pressure, with a df of 3; H is daily relative humidity, with a df of 4; and W is daily average wind speed, with a df of 5.
In order to achieve an optimal fitting in the model, we used the Akaike information criterion (AIC) (Akaike 1975) to detect and adjust the df of variable smoothing terms (Guo et al. 2011). The smaller the AIC value is, the better fitting of the model is. In order to acquire the smallest AIC value in the model, we adjusted and screened the df of each variable in Eq. (1) to select the optimal combinations. Then we derived the exposure response coefficient in the optimal model to compute RR values (as well as the 95% CI) for per IQR increase in PM2.5 (35.63 μg/m3) using Eqs. (2) and (3).
RR indicates the effect of the per unit change in the concentrations of air pollutants (per IQR) on the number of respiratory disease emergency department visits. If RR is greater than 1, it indicates a positive effect; if RR is smaller than 1, it indicates a negative effect. In addition, we analyzed the lag effects of air pollutants on the number of respiratory disease emergency department visits on the current day (lag 0) and the previous 1–6 days (lag 1–6 days). We selected the lag days that show the highest RR in the core model for further analysis. We used both single- and multi-pollutant models in the analysis. Single-pollutant model (Eq. (1)) has PM2.5 as the only air pollutant, and multi-pollutant model (Eq. (4)) also has SO2, and NO2 as the other air pollutants. In the multi-pollutant model, we added the other air pollutants one at a time to run the analysis.
where Zi is the concentrations of the added air pollutants, and other parameters are the same as in Eq. (1).
We used the MGCV package in R3.5.0 to adjust the single- and multi-pollutant models. The statistical significance level of RR is at p < 0.05.
Results
From 2009 to 2010, daily average concentrations of PM2.5, PM10, and SO2 were 44.04 μg/m3, 76.68 μg/m3, and 31.20 μg/m3, respectively, in Shanghai, China. Daily average pediatric asthma hospital visits were 169, including 79 for the under-2-year-olds, 61 for the 3-to-5-year-olds, and 29 for the 6-to-18-year-olds (Table 1). For the entire study group, the number of pediatric asthma hospital visits was positively correlated with the concentrations of air pollutants at a statistically significant level of p < 0.01. Among the three types of air pollutants, the highest correlation coefficient was between PM10 and the number of pediatric asthma hospital visits for the entire study group. In particular, the under-2-year-olds subgroup showed a relatively high positive correlation coefficient (p < 0.01) between the concentrations of PM2.5 and the number of pediatric asthma hospital visits. For the entire study group, the correlation coefficients between the number of pediatric asthma hospital visits and the four weather elements were all statistically significant at p < 0.01. For the four weather elements, the number of pediatric asthma hospital visits for the entire study group was negatively correlated with wind speed, relative humidity, and average air temperature, but positively correlated with air pressure. Among the three age-subgroups, the number of pediatric asthma hospital visits was most closely related to air pressure and average air temperature for the under-2-year-olds, to relative humidity for the 3-to-5-year-olds, and to wind speed for the 6-to-18-year-olds (Table 2).
From 2009 to 2010 in Shanghai, China, at lag 4 days, annual pediatric asthma hospital visits for the entire study group would rapidly increase as the concentrations of PM2.5 were increasing. When the concentrations of PM2.5 were increased to 120 μg/m3, annual pediatric asthma hospital visits for the entire study group would reach a peak, then began to fall (Fig. 1). From lag 0 to lag 6 days (current day to the previous 6 days), the highest RR (1.060) of PM2.5 on annual pediatric asthma hospital visits occurred at lag 4 days for the entire study group. Among the three age-subgroups, the highest RR of PM2.5 on annual pediatric asthma hospital visits occurred at lag 5 days for the under-2-year-olds (with a RR of 1.061), at lag 4 days for the 3-to-5-year-olds (with a RR of 1.071), and at lag 2 days for the 6-to-18-year-olds (with a RR of 1.052). Overall, PM2.5 showed a relatively stronger short-term effect on annual pediatric asthma hospital visits for the 3-to-5-year-olds as compared with the other two age-subgroups (Fig. 2).

Exposure-response curve for concentrations of PM2.5 and logarithm of RR in annual pediatric asthma hospital visits for the entire study group at lag 4 days from 2009 to 2010 in Shanghai, China

RRs of PM2.5 on annual pediatric asthma hospital visits for the entire study group as well as the three age-subgroups (under-2-year-olds, 3-to-5-year-olds, and 6-to-18-year-olds) at lag 0 (current day) and lag 1–6 days (previous 1–6 days) from 2009 to 2010 in Shanghai, China. RR values are statistically significant at p < 0.05 with the exceptions of that for the entire study group at lag 1 day and that for the 6-to-18-year-olds at lag 0. The “central dot” represents the mean of RR, and the vertical line extending from the central dot indicates the 95% CI of RR. The same definitions apply in Fig. 3
In Spring, the highest RR (1.041) of PM2.5 on seasonal pediatric asthma hospital visits occurred at lag 0 for the entire study group. As for the three age-subgroups, the highest RR (1.045, 1.039, and 1.025 for the under-2-year-olds, 3-to-5-year-olds, and 6-to-18-year-olds, respectively) of PM2.5 on seasonal pediatric asthma hospital visits all occurred at lag 0 (Fig. 3(a)). In Summer, the highest RR of PM2.5 on seasonal pediatric asthma hospital visits occurred at lag 0 for the entire study group (with a RR of 1.192) as well as the three age-subgroups (with a RR of 1.216, 1.267, and 1.054 for the under-2-year-olds, 3-to-5-year-olds, and 6-to-18-year-olds, respectively) (Fig. 3(b)). In Autumn, the highest RR of PM2.5 on seasonal pediatric asthma hospital visits occurred at lag 3 days for the entire study group (1.073) and the under-2-year-olds (1.112). Meanwhile, the highest RR of PM2.5 on seasonal pediatric asthma hospital visits occurred at lag 0 for the 3-to-5-year-olds (1.064) and the 6-to-18-year-olds (1.081) (Fig. 3(c)). In Winter, the highest RR of PM2.5 on seasonal pediatric asthma hospital visits occurred at lag 4 days for the entire study group (1.087) and the 6-to-18-year-olds (1.089). Meanwhile, the highest RR of PM2.5 on seasonal pediatric asthma hospital visits occurred at lag 0 for the under-2-year-olds (1.089) and at lag 5 days for the 3-to-5-year-olds (1.132) (Fig. 3(d)). In general, RR of PM2.5 on seasonal pediatric asthma hospital visits was relatively high in Summer for the entire study group as well as the under-2-year-olds and 3-to-5-year-olds. As for the 6-to-18-year-olds, RR of PM2.5 on seasonal pediatric asthma hospital visits was relatively high in Winter. In Spring and Autumn, the under-2-year-olds subgroup was more susceptible to asthma caused by PM2.5 than the other two subgroups. By contrast, in Summer and Winter, the 3-to-5-year-olds subgroup was more susceptible to asthma caused by PM2.5 than the other two subgroups.

RR of PM2.5 on seasonal (Spring, Summer, Autumn, and Winter) pediatric asthma hospital visits for the entire study group as well as the three age-subgroups (under-2-year-olds, 3-to-5-year-olds, and 6-to-18-year-olds) at lag 0 (current day) and lag 1–6 days (previous 1–6 days) from 2009 to 2010 in Shanghai, China. “a” on the error bar means that RR values are statistically significant at p < 0.05
When adding SO2 or NO2 or both SO2 and NO2 in the analysis model, RR of PM2.5 on annual pediatric asthma hospital visits showed little change for the entire study group, the under-2-year-olds, and the 3-to-5-year-olds but a gradual increase for the 6-to-18-year-olds. For the entire study group and the under-2-year-olds, RR of PM2.5 on seasonal pediatric asthma hospital visits in Spring barely changed when adding SO2 in the GAM but decreased when adding NO2 or both SO2 and NO2. For the 3-to-5-year-olds, RR of PM2.5 on seasonal pediatric asthma hospital visits in Spring showed similar changes as the annual metric when adding SO2 or NO2 or both SO2 and NO2 in the GAM. As for the 6-to-18-year-olds, RR of PM2.5 on seasonal pediatric asthma hospital visits in Spring was not statistically significant (p < 0.05) when adding SO2 or NO2 or both SO2 and NO2 in the GAM. In Summer, RR of PM2.5 on seasonal pediatric asthma hospital visits generally increased when adding NO2 in the GAM but decreased when adding SO2 or both SO2 and NO2, with the exception of the 6-to-18-year-olds. In Autumn and Winter, for the entire study group and the under-2-year-olds, RR of PM2.5 on seasonal pediatric asthma hospital visits decreased when adding SO2 or NO2 or both SO2 and NO2 in the GAM. For the 3-to-5-year-olds, RR of PM2.5 on seasonal pediatric asthma hospital visits increased in Autumn but decreased in Winter when adding SO2 or NO2 or both SO2 and NO2 in the GAM. As for the 6-to-18-year-olds, RR of PM2.5 on seasonal pediatric asthma hospital visits only decreased when adding SO2 in Autumn or when adding NO2 in Winter (Table 3).
Discussion
In this study, we found that the number of pediatric asthma hospital visits was positively correlated with average air pressure but negatively correlated with average wind speed, relative humidity, and air temperature. These results are consistent with that from Chan et al. (2018), Hu et al. (2015), and Jun et al. (2009). From 2009 to 2010 in Shanghai, China, the daily number of pediatric asthma hospital visits would increase with the increase in daily concentrations of PM2.5. From 2006 to 2007 in Australia, asthma-related emergency department visits would increase by 1.96% (95% CI 0.02–3.94%) for per IQR increase in area PM2.5 (8.6 μg/m3) (Haikerwal et al. 2016). From 2010 to 2014 in the state of Florida, USA, for per 10 μg/m3 increase in PM2.5, asthma-related emergency department visits would go up by 2% for the 5-to-12-year-olds and 0.6% for the 13-to-18-year-olds; when the concentrations of PM2.5 reached 64.66 μg/m3, RR of PM2.5 on childhood asthma incidence was up to 1.08 (95% CI 1.05–1.11) (Mehra 2017).
We observed some lag effects of PM2.5 on the number of pediatric asthma hospital visits from 2009 to 2010 in Shanghai, China. Annually, PM2.5 showed the strongest effect on the number of pediatric asthma hospital visits at a lag of 4 days for the under-2-year-olds, a lag of 5 days for the 3-to-5-year-olds, and a lag of 2 days for the 6-to-18-year-olds. In Spring and Summer, the highest RR of PM2.5 on the number of pediatric asthma hospital visits occurred unanimously at a lag of 0 days. In Autumn, the highest RR of PM2.5 on the number of pediatric asthma hospital visits occurred at a lag of 3 days for the under-2-year-olds, but a lag of 0 day for both 3-to-5-year-olds and 6-to-18-year-olds. In Winter, the highest RR of PM2.5 on the number of pediatric asthma hospital visits occurred at a lag of 0 day for the under-2-year-olds, a lag of 5 days for the 3-to-5-year-olds, and a lag of 4 days for the 6-to-18-year-olds. The lag effects of PM2.5 on pediatric asthma hospital visits could be related to seasonal allergens such as pollen. Similar lag effects were also reported in other locations. For example, in Changhua (central county) and Yunlin (western county) in Taiwan, RR of PM2.5 on the number of pediatric asthma hospital visits for the under-15-year-olds was higher on lag 2 days than on the current day (the concentrations of PM2.5 increased from 36.17 to 81.26 μg/m3) (Chien et al. 2018). In the state of Massachusetts, USA, a case-crossover study on the effect of early life exposure to PM2.5 on risk of acute asthma clinical encounters among children showed that the OR value of PM2.5 exposure on children asthma clinical encounters was close to 1.0 at lags of 0, 1, and 2 days (Khalili et al. 2018). In particular, for per IQR (5.9 μg/m3) increase in PM2.5, the clinical risk of asthma for children with low birth weight (LBW < 2500 g) would increase at a lag of 1 day, with an OR value of 1.08 (95% CI 1.01–1.15) (Khalili et al. 2018). In Tacoma, WA, USA, RR of PM2.5 on asthma-related emergency department visits was 1.04 (95% CI 1.01–1.07) at lag 2 days and 1.03 (95% CI 1.0–1.06) at lag 3 days (Mar et al. 2010).
We ran seasonal analysis for the three different age-subgroups and found that RR of PM2.5 on pediatric asthma hospital visits was relatively high in Spring and Autumn for the under-2-year-olds, in Summer and Winter for the 3-to-5-year-olds, and in Winter for the 6-to-18-year-olds. A previous study reported that with per 10 μg/m3 increase in PM2.5, the number of asthma emergency visits would increase by more in warm season (with a rate of 3.7%, 95% CI 0.5–6.9%) than in cold season (with a rate of 2.6%, 95% CI 0.7–4.6%) (Fan et al. 2016). Nevertheless, another study pointed out that the effect of PM2.5 on asthma was stronger in cold season than in warm season (Jung et al. 2017), mostly due to the fact children were exposed to higher concentrations of PM2.5 in Winter than in Summer (Zhang et al. 2015). In the Northern New Jersey-New York City metro area of the USA, asthma incidence was closely correlated with air pollution in relatively warm months based on a 15-year summary of airborne allergens (Port et al. 2006). During the warm season, the amount of pollen (e.g., trees, grass, weeds, and ragweed) reaches the peak, which is positively correlated to the incidence of respiratory diseases (CarracedoMartinez et al. 2010). Therefore, some studies only focus on the effects of atmospheric particulate matter on asthma during warm season (Gleason et al. 2014). However, in some regions of the world, the concentrations of PM2.5 reach the peak in Winter mostly due to direct emissions produced by burning fuel (especially coal) for heat (Song et al. 2015).
In different seasons, the maximum RR value appears in different lag days. According to the research in New York State from 2000 to 2005, PM2.5 has the greatest impact on respiratory hospitalizations at lag 4, 1, 4, 0, and 0 days around the year, Spring, Summer, Fall, and Winter, respectively. And RR values in Summer are much higher than other seasons, which is consistent with the results of this study (Jones et al. 2015). In Taipei and Kaohsiung, the maximum OR values of PM2.5 on childhood asthma hospitalization are found at lag 2, 3, 1, and 3 days for Spring, Summer, Autumn, and Winter, respectively, with the RR values of 0.998 (95% CI 0.823–1.210), 1.085 (95% CI 0.739–1.593), 0.966 (95% CI 0.787–1.186), and 1.109 (95% CI 0.885–1.388) (Kuo et al. 2018).
In the multi-pollutant models, RR of PM2.5 on pediatric asthma hospital visits was generally higher than that in the single-pollutant model from 2009 to 2010 in Shanghai, China. However, the amplitude of the increase in RR varied to different extents for the three age-subgroups during the four seasons. In Beijing, China, both the single- and multi-pollutant models showed the highest increase percentage (IP) of RR for the under-15-year-olds (Ma et al. 2018). In Atlanta, GA, USA, the multi-pollutant model usually showed smaller estimates on the number of pediatric asthma emergency department visits than the single-pollutant model (Winquist et al. 2014). In addition, the warm-season joint impact of models without nonlinear effects is usually stronger than that for the cold season (Winquist et al. 2014). O3 is a pollutant of primary concern in Hong Kong, China; the multi-pollutant model showed stronger effects of O3 on asthma-related hospitalization rate than that of NO2 and SO2 (Ko et al. 2010). In St. John’s, Canada, the multi-pollutant model showed that respiratory disease–related emergency department visits were caused more by O3 (with a rate of 3.9%, 95% CI 0.8–7.2%) than by SO2 (with a rate of 3.7%, 95% CI 1.5–6.0%) (David et al. 2000).
Inevitably, there are some limitations of the results in this study. First, we used the average daily concentrations of air pollutant that are derived from a variety of monitoring stations without eliminating the inherent measurement bias (Chen et al. 2012). Second, we assumed that all individuals in the study group were equally exposed to the same air pollutants at all times, which might not be consistent with reality. Third, due to the nature of the analysis model, multicollinearity between air pollutants and weather elements might cause some bias in the results. Therefore, we suggest that future studies should (a) homogenize air quality data from multiple monitoring stations; (b) acquire detailed information about the actual exposure in air pollutants for the study group; and (c) minimize the bias caused by multicollinearity in the analysis model.
Conclusions
Our study showed that PM2.5 has a significant short-term effect on the number of pediatric asthma hospital visits in Shanghai, China, from 2009 to 2010. We detected different seasonal lag effects for the entire study group as well as the three age-subgroups. For the entire study group, the highest RR value occurred at a lag of 4 days. Within the study group, the highest RR value occurred at a lag of 5 days for the under-2-year-olds, a lag of 4 days for the 3-to-5-year-olds, and a lag of 2 days for the 6–18-year-olds. Overall, the under-2-year-olds subgroup was the most affected by PM2.5 in pediatric asthma hospital visits, especially in Summer. When introducing other air pollutants (including SO2 and NO2) in the analysis model, the short-term effect of PM2.5 on pediatric asthma hospital visits is unchanging. The results in this study could be used by the local health and human services authority to help lowering childhood asthma prevalence in Shanghai.
References
Akaike H (1975) A new look at the statistical model identification. IEEE Trans Autom Control 19(6):716–723
An MY (2013) The association of PM2.5 and surface ozone with asthma prevalence among school children in Japan: 2006-2009. Health 5(10B):1–7
Bell ML, Dominici F, Ebisu K, Zeger SL, Samet JM (2007) Spatial and temporal variation in PM2.5 chemical composition in the United States for health effects studies. Environ Health Perspect 115(7):989–995
CarracedoMartinez E, Sanchez C, Taracido M, Saez M, Jato V, Figueiras A (2010) Effect of short-term exposure to air pollution and pollen on medical emergency calls: a case-crossover study in Spain. Allergy 63(3):347–353
Chan CL, Phan DV, Yang NP, Pan RH, Wu CY, Chen CL, Kuo CY (2018) A survey of ambulatory treated asthma and correlation with weather and air pollution conditions within Taiwan during 2001–2010. Journal of asthma, 1-22
Chen RJ, Somli E, Wong QM et al (2012) Associations between short-term exposure to nitrogen dioxide and mortality in 17 Chinese cities: the China air pollution and health effects study (CAPES). Environ Int 45:32–38
Chien LC, Chen YA, Yu HL (2018) Lagged influence of fine particulate matter and geographic disparities on clinic visits for children’s asthma in Taiwan. Int J Environ Res Public Health 15(4):829
Dany D, Kees DH, Nicole PH et al (2017) Residential air pollution and associations with wheeze and shortness of breath in adults: a combined analysis of cross-sectional data from two large European cohorts. Environ Health Perspect 125(9):097025
David MS, Robert CB, Jeffery RB et al (2000) Air pollution, aeroallergens and cardiorespiratory emergency department visits in Saint John, Canada. J Expo Anal Environ Epidemiol 10(5):461–477
Fan J, Li S, Fan C, Bai Z, Yang K (2016) The impact of PM2.5 on asthma emergency department visits: a systematic review and meta-analysis. Environ Sci Pollut Res 23(1):843–850
Gent JF, Koutrakis P, Belanger K et al (2009) Symptoms and medication use in children with asthma and traffic-related sources of fine particle pollution. Environ Health Perspect 117(7):1168–1174
Glad JA, Brink LL, Talbott EO, Lee PC, Xu X, Saul M et al (2012) The relationship of ambient ozone and PM2.5 levels and asthma emergency department visits: possible influence of gender and ethnicity. Arch Environ Occup Health 67(2):103–108
Gleason JA, Bielory L, Fagliano JA (2014) Associations between ozone, PM2.5, and four pollen types on emergency department pediatric asthma events during the warm season in New Jersey: a case-crossover study. Environ Res 132(132C):421–429
Guo YM, Barnett AG, Yu WW et al (2011) A large change in temperature between neighbouring days increases the risk of mortality. PLoS One 6(2):e16511
Guyatt GH, Juniper EF, Griffith LE, Feeny DH, Ferrie PJ (1997) Children and adult perceptions of childhood asthma. Pediatrics 99(2):165–168
Haikerwal A, Akram M, Sim MR, Meyer M, Abramson MJ, Dennekamp M (2016) Fine particulate matter (PM2.5) exposure during a prolonged wildfire period and emergency department visits for asthma. Respirology 21(1):88–94
HakanTecer L, OmarAlagha, FerhatKaraca, GürdalTuncel, NiluferEldes (2008) Particulate matter (PM2.5, PM10–2.5, and PM10) and children’s hospital admissions for asthma and respiratory diseases: a bidirectional case-crossover study. J Toxicol Environ Health, 71(8), 512–520
Han JB, Zhang ZH, Tong GQ, Jian-Jun XU, Qiu Y, Liu HF et al (2014) Effects of PM2.5 on inflammatory factors of patients with asthma in Taiyuan. J Environ Health 31(3):229–231
Hu XG, Jin Y, Jin JB, Lin L, Zhang HL, Li CC (2015) Relationship between air pollutants and respiratory diseases in children. J Bio-Educ 1:26–30
Ito S, Kawaoi T, Kondo Y, Hiruma F, Togo T, Takashima H et al (1992) Outbreaks of asthma attack and meteorological parameters—comparison between two areas. Arerugī = [Allergy] 41(4):475–484
Jones RR, Hogrefe C, Fitzgerald EF et al (2015) Respiratory hospitalizations in association with fine PM and its components in New York state. J Air Waste Manage Assoc 65(5):559–569
Jun LI, Sun CB, Liu XD, Dong SP, Guo J, Wang Y et al (2009) Non-parameter statistical analysis of impacts of meteorological conditions on PM concentration in Beijing. Res Environ Sci 22(06):663–669
Jung CR, Young LH, Hsu HT, Lin MY, Chen YC, Hwang BF et al (2017) PM2.5 components and outpatient visits for asthma: a time-stratified case-crossover study in a suburban area. Environ Pollut 231(Pt 1):1085–1092
Kan H, London SJ, Chen G et al (2008) Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: the public health and air pollution in Asia (PAPA) study. Environ Health Perspect 116(9):1183–1188
Keet CA, Keller JP, Peng RD (2018) Long-term Coarse PM Exposure is Associated with Asthma Among Children in Medicaid. Am J Respir Crit Care Med 197(6), 737–746
Khalili R, Bartell SM, Hu X, Liu Y, Chang HH, Belanoff C et al (2018) Early-life exposure to PM2.5 and risk of acute asthma clinical encounters among children in Massachusetts: a case-crossover analysis. Environ Health 17(1):25
Kioumourtzoglou MA, Schwartz J, James P et al (2016) PM2.5 and mortality in 207 US cities: modification by temperature and city characteristics. Epidemiology (Cambridge, Mass.) 27(2):221
Ko FWS, Tam W, Wong TW, Lai CKW, Wong GWK, Leung TF et al (2010) Effects of air pollution on asthma hospitalization rates in different age groups in Hong Kong. Clin Exp Allergy 37(9):1312–1319
Koenig JQ, Mar TF, Allen RW, Jansen K, Lumley T, Sullivan JH et al (2005) Pulmonary effects of indoor- and outdoor-generated particles in children with asthma. Environ Health Perspect 113(4):499–503
Kuo CY, Pan RH, Chan CK et al (2018) Application of a time-stratified case-crossover design to explore the effects of air pollution and season on childhood asthma hospitalization in cities of differing urban patterns: big data analytics of government open data. Int J Environ Res Public Health 15(4):647
Lee SL, Wong WHS, Lau YL (2006) Association between air pollution and asthma admission among children in Hong Kong. Clin Exp Allergy J Br Soc Allergy Clin Immunol 36(9):1138–1146
Liu CJ, Liu CY, Mong N, Chou C (2016) Spatial correlation of satellite-derived PM2.5 with hospital admissions for respiratory diseases. Remote Sens 8(11)
Loftus C, Yost M, Sampson P, Arias G, Torres E, Vasquez VB et al (2015) Regional PM2.5 and asthma morbidity in an agricultural community: a panel study. Environ Res 136:505–512
Ma YX, Yang SX, Zhou JD, Yu ZA, Zhou J (2018) Effect of ambient air pollution on emergency room admissions for respiratory diseases in Beijing, China. Atmos Environ 191:320–327
Maio S, Baldacci S, Carrozzi L (2016) Respiratory symptoms/diseases prevalence is still increasing a 25-yr population study. Respir Med 110:58–65
Mar TF, Koenig JQ, Primomo J (2010) Associations between asthma emergency visits and particulate matter sources, including diesel emissions from stationary generators in Tacoma, Washington. Inhal Toxicol 22(6):445
Mehra S (2017) Estimating the impact of a select criteria pollutant (PM2.5) on childhood asthma in Florida. Scholarcommons.usf.edu
Mo Z, Peng L, Yang DD et al (2014) Impact of weather and pollution on the number of children with asthma in Shanghai. Chinese Health Stat 31(5):827–829
Pan CL, Kuai WX (2017) The correlation study of atmospheric fine particles concentration and children with cough variant asthma. Anhui Med J 38(7):848–851
Peng G, Yokoyama K, Suenaga M, Kida H (2008) Mortality and life expectancy of Yokkaichi asthma patients, Japan: late effects of air pollution in 1960–70s. Environ Health,7,1(2008-02-26) 7(1):8
Polezer G, Tadano YS, Siqueira HV, Godoi A, Yamamoto CI, De PA et al (2018) Assessing the impact of PM2.5 on respiratory disease using artificial neural networks. Environ Pollut 235:394–403
Port AM, Hein JM, Wolff AM, Bielory LM (2006) Aeroallergen prevalence in the northern New Jersey-New York city metropolitan area: a 15-year summary. Ann Allergy Asthma Immunol 96(5):687–691
Requia WJ, Adams MD, Koutrakis P (2017) Association of PM2.5 with diabetes, asthma, and high blood pressure incidence in Canada: a spatiotemporal analysis of the impacts of the energy generation and fuel sales. Sci Total Environ 98(2):1077
Samet JM, Dominici F, Zeger SL (2000) The national morbidity, mortality, and air pollution study. Part I: methods and methodologic issues. Res Rep Health Eff Inst 94(2):5–14
Schlesinger RB (2007) The health impact of common inorganic components of fine particulate matter (PM2.5) in ambient air: a critical review. Inhal Toxicol 19(10):811
Shanghai Medical Association Pediatric Professional Committee Respiratory Group (2014) Epidemiological survey of asthma in children aged 0–14 years in seven districts of Shanghai. Chin J Pediatr 52(1):17–22
Shi L, Zanobetti A, Kloog I, Coull BA, Koutrakis P, Melly SJ et al (2016) Low-concentration PM2.5 and mortality: estimating acute and chronic effects in a population-based study. Environ Health Perspect 124(1):46–52
Song C, Pei T, Yao L (2015) Analysis of the characteristics and evolution modes of PM2.5 pollution episodes in Beijing, China during 2013. Int J Environ Res Public Health 12(2):1099
Spira-Cohen A, Chen LC, Kendall M et al (2009) Personal exposures to traffic-related particle pollution among children with asthma in the south Bronx, NY. J Expo Sci Environ Epidemiol 20(5):446–456
Torgerson DG, Ampleford EJ, Chiu GY, Gauderman WJ, Gignoux CR, Graves PE et al (2011) Meta-analysis of genome-wide association studies of asthma in ethnically diverse north American populations. Nat Genet 43(9):887–892
Wang M, Zheng S, Wang S et al (2012) A time-series study on the relationship between gaseous air pollutants and daily hospitalization of respiratory disease in Lanzhou City. J Hyg Res 41(5):771–775
Wang W, Mao FY, Du L et al (2017) Deriving hourly PM2.5 concentrations from Himawari-8 AODs over Beijing–Tianjin–Hebei in China. Remote Sens 9(8):858
Winquist A, Kirrane E, Klein M, Strickland M, Darrow LA, Sarnat SE et al (2014) Joint effects of ambient air pollutants on pediatric asthma emergency department visits in Atlanta, 1998-2004. Epidemiology 25(5):666–673
Yuan D, Shen CL, Jiang ZH, Huang HT, Gao HM, Liu HY, Li HL, Zhang SN (2007) An investigation on the prevalence of asthma and its influence factors among school age children in Shanghai. Environ Occup Med 24(6):573–576
Yun RS, Jin SU, Hong LY, Wei GZ (2002) Effects of environmental PM2.5 pollution on the morbidity of asthma and lung cancer. J Lab Med 23(4):367–378
Zahran HS, Bailey CM, Qin X, Moorman JE (2014) Assessing asthma severity among children and adults with current asthma. J Asthma 51(6):610–617
Zang L, Mao FY, Guo JP et al (2018) Estimating hourly PM1 concentrations from Himawari-8 aerosol optical depth in China. Environ Pollut 241(2018):654–663
Zang L, Mao FY, Guo JP et al (2019) Estimation of spatiotemporal PM1.0 distributions in China by combining PM2.5 observations with satellite aerosol optical depth. Sci Total Environ 658(2019):1256–1264
Zhang N, Han B, He F, Xu J, Niu C, Zhou J et al (2015) Characterization, health risk of heavy metals, and source apportionment of atmospheric PM2.5, to children in summer and winter: an exposure panel study in Tianjin, China. Air Qual Atmos Health 8(4):1–11
Zou Y, Wu Y, Wang Y et al (2017) Physicochemical properties, in vitro cytotoxic and genotoxic effects of PM1.0 and PM2.5 from Shanghai, China. Environ Sci Pollut Res 24:19508–19516
Acknowledgments
The authors would like to thank the Professional Services for Meteorology, Environment and Public Health of the National Scientific Data Sharing Platform for Population and Health for providing data for this study.
Funding
This research is financially supported by the National Natural Science Foundation of China (Grant nos. 91744311 and 41561037) and Environmental Protection Agency foundation (Grant no. 2018-007). Part of this study is funded by a China Scholarship Council (CSC) scholarship that was awarded to Yuxia Ma (file no. 201308625022).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Responsible editor: Philippe Garrigues
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 17 kb)
Rights and permissions
About this article

Cite this article
Ma, Y., Yu, Z., Jiao, H. et al. Short-term effect of PM2.5 on pediatric asthma incidence in Shanghai, China. Environ Sci Pollut Res 26, 27832–27841 (2019). https://doi.org/10.1007/s11356-019-05971-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-019-05971-9