
Abstract
Background
Chronic kidney disease (CKD) is very common now and is associated with high overall and cardiovascular mortality. Numerous studies have reported that elevated heart rate (HR) is a risk factor for cardiovascular mortality. We investigated the link between serum endocan and circadian heart rate variability in non-dialysis stage 5 CKD patients.
Methods
In a cross-sectional study, we enrolled 54 prevalent n non-dialysis stage 5 CKD patients (32 males, aged 48.2 ± 14.92 years). HR was measured with an automatic system. Serum endocan level was analyzed by ELISA.
Results
Night/day HR ratio was independently predicted by serum endocan level (P < 0.01) and hypertension history (P < 0.05). Adjusted R2 of the model was 0.222.
Conclusion
Increased serum endocan is significantly associated with circadian heart rate variability in non-dialysis stage 5 CKD patients. Further investigation is needed to explore the potential benefits of serum endocan lowering therapy in this patient group.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic kidney disease (CKD) has been a major problem in the world. A national epidemiological survey found that CKD affects 10.8% of the Chinese general population and imposes substantial morbidity and cost [1]. CKD associated with high overall and cardiovascular (CV) mortality [2, 3]. It is reported that up to 45% of pre-dialysis CKD patients may die before reaching end-stage renal disease (ESRD), which makes cardiovascular disease (CVD) the leading cause of death in CKD [4]. The reasons for this high cardiovascular mortality are not fully understood, but increased heart rate (HR) might be an important risk factor based on the association of elevated HR with increased CV morbidity and mortality in the general [5], in patients with ischemic heart disease [6], and CKD [7] populations.
HR is one of the simplest measures of hemodynamics in humans, and could be a marker of general health [8], but it is affected by a variety of conditions such as anemia or physical activity. Higher resting HR might reflect increased sympathetic and/or reduced parasympathetic activity. Early study also suggests that high resting HR, even within the normal range (< 100 beats/min), is a predictor of mortality in the general population [8]. Woodward et al., who analyzed a pooling data of 112,680 subjects in 12 cohort studies with 7.4-year follow-up, also showed that resting HR has positive associations with total mortality and a range of major cardiovascular events [9]. It is also found that HR non-dipping status, resting HR does not exhibit the typical nocturnal decline, was significantly associated with increased risk of CVD [10]. And it is also found that a greater increase in night/day HR ratio, i.e., a lesser decrease in nocturnal HR, was associated to increased arterial stiffness [11].
Endocan, previously called endothelial cell-specific molecule-1 (ESM-1), is a soluble proteoglycan (50 kDa), secreted by human vascular endothelial cells, which can be detected in the circulation and is an indicator of angiogenesis and endothelial cell activation [12]. Endocan increases in the presence of decreasing eGFR and influences all-cause mortality and CV events in patients with CKD independent of traditional and non-traditional risk factors [13].
In the present study, we aimed to investigate the link between circadian heart rate variability and endocan in non-dialysis stage 5 CKD patients.
Methods
Study population and biochemical measurements
All prevalent non-dialysis stage 5 CKD patients at the Division of Nephrology of the First Affiliated Hospital of Kunming Medical University were enrolled in a cross-sectional study. The exclusion criteria were (1) clinical or laboratory evidence of heart failure, coronary artery disease, and/or cerebrovascular disease; (2) less than 18 years old; (3) unwillingness to participate in the study. The ethics committee of Kunming Medical University approved this study protocol. Patients’ smoking status was recorded as non-smoking or smoking. Patients’ use of beta-blocker was recorded as using or non-using.
Glomerular filtration rate estimation
Glomerular filtration rate (GFR) was estimated according to the simplified version of the Modification of Diet in Renal Disease formula [14]:
\(\text{GFR} \left(\text{ml}/{\text{min}}/1.73\, {\text{m}}^2\right) = 186 \times {\text{Pcr}}^{-1.154}\times {\text{age}}^{-0.203} \times 0.742 \left(\text{if female}\right).\)
Pcr stands for plasma creatinine (mg/dL).
The ambulatory heart rate
Non-invasive HR was performed on a weekday with an automatic system (CB-2302-A, Bio Instrument, China), which recorded HR every 30 min from 8 am to 10 pm; and 60 min from 10 pm to 8 am next day. Resting and day time were defined on the basis of patients’ diaries recorded during ambulatory blood pressure monitoring (ABPM), and night/day HR ratio was calculated accordingly.
Serum endocan measurements
All blood samples were obtained from patients in the morning after 12 h of fasting. Blood samples were collected in plain tubes to measure serum endocan levels. Serum was separated from the blood after centrifugation for 10 min. The serum samples were stored at − 80 °C until analysis. The concentration of human endothelial cell-specific molecule-1 was analyzed by ELISA using commercial kits (Abnova Bioscience, Taoyuan, TWN), in accordance with the manufacturers’ instructions. Measurements were carried out using enzyme-linked immunosorbent assay plate reader Multiskan Go 1510-02669C spectrometer (Thermo Fisher Scientific Oy, Ratastie 2. FI-01620 Vantaa, Finland). Patients were divided into high serum endocan level (this cut-off value was set according to the mean of serum endocan value of the study population) and low serum endocan level groups according to serum endocan values.
Statistical analysis
Continuous variables were expressed as mean ± SD (normal distribution). Differences between groups were tested using independent-sample t test for normally distributed variables. Pearson’s correlation was performed when the relationship between parameters was explored. Multiple regression analysis was performed to identify the relative dependence of observed correlations of night/day HR ratio (stepwise method). All tests were two-sided. A value of P < 0.05 was considered statistically significant.
Results
Baseline characteristics
Baseline data were given in Table 1. Briefly, there were 54 non-dialysis stage 5 CKD patients (32 M/22 F) included in the present study. Patients’ age was 48.2 ± 14.92 years with GFR 8.0 ± 3.50 ml/min/1.732. No patient was on maintenance dialysis or had been transplanted.
Different clinical variables of serum endocan groups
Clinical parameters of 54 non-dialysis stage 5 CKD patients based on serum endocan level were listed in Table 2. Patients’ resting HR in low endocan group was significantly lower than that of high endocan group (P < 0.05). Night/day HR ratio in high endocan group was significantly higher than that of low group (P < 0.05). Patients in low endocan group had lower serum endocan value than that of high endocan group (P < 0.01). There were no significant difference between the two groups in patients’ age, gender, smoking status, hypertension history, diabetic history, use of beta-blocker, height, weight, BMI, hemoglobin, and awake HR.
Univariate correlations
Univariate correlations between night/day HR ratio with selected clinical and biochemical markers in non-dialysis stage 5 CKD patients were given in Table 3. Briefly, night/day HR ratio was positively correlated with age, serum endocan level, and resting HR. The relationship of night/day HR ratio and serum endocan level is shown in Fig. 1.

Correlation between serum endocan level and night/day HR ratio in the 54 non-dialysis stage 5 CKD patients
Regression models
The output from multivariate regression analysis of predictors for night/day HR ratio is shown in Table 4. Briefly, night/day HR ratio was independently predicted by serum endocan level (P < 0.01) and hypertension history (P < 0.05). Adjusted R2 of the model was 0.222.
Predictive performance of serum endocan for low and high night/day HR ratio
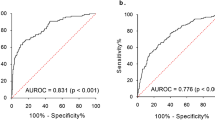
The ROC curve of serum endocan for the prediction of the low and high HR ratio is shown in Fig. 2. The area under the ROC curve of serum endocan for the prediction of the low and high night/day HR ratio was 0.702 (95% CI, 0.562–0.841) and the cut-off value was 495.0 pg/ml, with sensitivity of 66.7%, specificity of 70.4%.

ROC curve of serum endocan’s discriminatory ability regarding night/day HR ratio (low vs. high)
Discussion
In the present study, we found a significant association between elevated night/day HR ratio and increased serum endocan value in non-dialysis stage 5 CKD patients. This association was still present even after adjustment for confounders, such as gender, smoking, use of beta-blocker, renal function, and diabetic history. Thus, despite the high prevalence of anemia in the present study, serum endocan still appeared to be an important predictor of high night/day HR ratio, a lesser decrease in nocturnal heart rate (circadian heart rate variability), in non-dialysis stage 5 CKD patients.
It is well known that patients with CKD have approximately 20 times the mortality risk of the general population, and they mainly die from CV-related deaths [15]. Endothelial dysfunction plays a central role in the atherosclerotic process [16] and is considered of central importance in cardiovascular disease in CKD patients [17]. Comorbidities including obesity [18], inflammation [19], metabolic syndrome [20], and other environmental risk factors trigger a complex events engendering arterial stiffness. HR is in fact determined by a complex interplay of sympathetic and parasympathetic components of the autonomic nervous system (ANS) on the cardiac electrical system, baroreceptors, vascular tone, endothelial function, and cardiac contractility in response to different stimuli in physiological and pathological conditions. The night/day HR ratio expresses a lesser decrease in nocturnal HR, and has been found to have a direct relationship with all the parameters evaluating arterial stiffness, including PWV [11]. Our previous study also shows that increased sleep heart rate is significantly associated with elevated arterial stiffness in CKD patients [21]. HR reduction by ivabradine can improve endothelial function in patients with coronary artery disease [22].
Endocan is a soluble proteoglycan expressed by the vascular endothelium. It has reported that endocan is over-expressed in cancer [23] and is related to patients’ outcome [24]. Endocan also plays roles in the vascular contribution to organ-specific inflammation and in endothelium-dependent pathological disorders which may represent a novel endothelial cell dysfunction marker [25,26,27]. Endocan has been proved to correlate with cardiovascular risk and/or activity of disease in psoriasis vulgaris [28], Behçet disease [29], and Obstructive Sleep Apnea [30]. Our study found that an elevated night/day HR ratio, which represents lesser decrease in nocturnal HR, significantly associated with increased serum endocan value in non-dialysis stage 5 CKD patients. Our finding shows that serum endocan may take part into the endothelial damage caused by circadian HR variability, and further studies are needed to prove that.
De Souza et al. found a positive correlation between the serum endocan concentration and systolic blood pressure in renal transplant patients [31]. As endothelial dysfunction is associated with the development of hypertension and other cardiovascular diseases in CKD patients, it is possible that the presence of this condition could, at least in part, reflect the processes that were involved in increasing the endocan levels in our study population.
The potential effect of control of hyperlipidemia and pleiotropic effects of statin use on endocan levels were not discussed. Because we routinely stopped statin use when our CKD patients reach stage 5, for the lack of clear clinical benefits in this group of patients [32].
The main limitation of our study is its cross-sectional design, and our study group is too small by which a cause-and-effect relationship cannot be discerned. Future prospectively designed studies are needed to determine whether the serum endocan would predict night/day HR ratio in non-dialysis stage 5 CKD patients. Second, although a number of potential confounding factors have been evaluated, the existence of other unrecognized confounding variables should be considered.
In conclusion, increased serum endocan is significantly associated with elevated night/day HR ratio in non-dialysis stage 5 CKD patients. This suggests that serum endocan level maybe useful for predicting circadian heart rate variability in non-dialysis stage 5 CKD patients, and further investigation is needed to explore the potential benefits of serum endocan lowering therapy in this patient group.
References
Zhang L et al (2012) Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet 379(9818):815–822
Foley RN (2010) Clinical epidemiology of cardiovascular disease in chronic kidney disease. J Ren Care 36(Suppl 1):4–8
Go AS et al (2004) Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351(13):1296–1305
Keith DS et al (2004) Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med 164(6):659–663
Aune D et al (2017) Resting heart rate and the risk of cardiovascular disease, total cancer, and all-cause mortality: a systematic review and dose-response meta-analysis of prospective studies. Nutr Metab Cardiovasc Dis 27(6):504–517
Palatini P (2005) Heart rate: a strong predictor of mortality in subjects with coronary artery disease. Eur Heart J 26(10):943–945
Beddhu S et al (2009) Associations of resting heart rate with insulin resistance, cardiovascular events and mortality in chronic kidney disease. Nephrol Dial Transplant 24(8):2482–2488
Benetos A et al (1999) Influence of heart rate on mortality in a French population: role of age, gender, and blood pressure. Hypertension 33(1):44–52
Woodward M et al (2014) The association between resting heart rate, cardiovascular disease and mortality: evidence from 112,680 men and women in 12 cohorts. Eur J Prev Cardiol 21(6):719–726
Eguchi K et al (2009) Nocturnal nondipping of heart rate predicts cardiovascular events in hypertensive patients. J Hypertens 27(11):2265–2270
Garcia-Ortiz L et al (2011) Relationships of night/day heart rate ratio with carotid intima media thickness and markers of arterial stiffness. Atherosclerosis 217(2):420–426
Sarrazin S et al (2006) Endocan or endothelial cell specific molecule-1 (ESM-1): a potential novel endothelial cell marker and a new target for cancer therapy. Biochim Biophys Acta 1765(1):25–37
Yilmaz MI et al (2014) Plasma endocan levels associate with inflammation, vascular abnormalities, cardiovascular events, and survival in chronic kidney disease. Kidney Int 86(6):1213–1220
Levey AS et al (1999) A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med 130(6):461–470
Foley RN, Parfrey PS, Sarnak MJ (1998) Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis 32(5 Suppl 3):S112–S119
Tousoulis D, Charakida M, Stefanadis C (2006) Endothelial function and inflammation in coronary artery disease. Heart 92(4):441–444
Zoccali C (2006) Endothelial dysfunction and the kidney: emerging risk factors for renal insufficiency and cardiovascular outcomes in essential hypertension. J Am Soc Nephrol 17(4 Suppl 2):S61–S63
Zhe X et al (2012) Hypertriglyceridemic waist is associated with increased carotid atherosclerosis in chronic kidney disease patients. Nephron Clin Pract 122(3–4):146–152
Kaysen GA, Eiserich JP (2004) The role of oxidative stress-altered lipoprotein structure and function and microinflammation on cardiovascular risk in patients with minor renal dysfunction. J Am Soc Nephrol 15(3):538–548
Zhe XW et al (2008) Pulse wave velocity is associated with metabolic syndrome components in CAPD patients. Am J Nephrol 28(4):641–646
Bai Y et al (2013) Increased night heart rate is associated with worse large artery elasticity in chronic kidney disease patients. Int Urol Nephrol 45(6):1621–1627
Mangiacapra F et al (2017) Heart rate reduction by IVabradine for improvement of ENDothELial function in patients with coronary artery disease: the RIVENDEL study. Clin Res Cardiol 106(1):69–75
Delehedde M et al (2013) Endocan in cancers: a lesson from a circulating dermatan sulfate proteoglycan. Int J Cell Biol 2013:705027
Kim JH et al (2012) Expression of endothelial cell-specific molecule-1 regulated by hypoxia inducible factor-1alpha in human colon carcinoma: impact of ESM-1 on prognosis and its correlation with clinicopathological features. Oncol Rep 28(5):1701–1708
Scherpereel A et al (2006) Endocan, a new endothelial marker in human sepsis. Crit Care Med 34(2):532–537
Zhang SM et al (2012) Expression and distribution of endocan in human tissues. Biotech Histochem 87(3):172–178
Balta S et al (2015) Endocan: a novel inflammatory indicator in cardiovascular disease? Atherosclerosis 243(1):339–343
Balta I et al (2013) Elevated serum levels of endocan in patients with psoriasis vulgaris: correlations with cardiovascular risk and activity of disease. Br J Dermatol 169(5):1066–1070
Balta I et al (2014) Serum endocan levels as a marker of disease activity in patients with Behcet disease. J Am Acad Dermatol 70(2):291–296
Balta S, Ozturk C (2016) Endocan, obstructive sleep apnea, and vascular risk. Angiology 67(4):305–306
de Souza LC et al (2016) Serum endocan levels associated with hypertension and loss of renal function in pediatric patients after two years from renal transplant. Int J Nephrol 2016:2180765
Rysz J et al (2015) Should we use statins in all patients with chronic kidney disease without dialysis therapy? The current state of knowledge. Int Urol Nephrol 47(5):805–813
Acknowledgements
The authors thank all the patients and staff of the Division of Nephrology.
Funding
This work was funded by grant from Chinese Society of Blood Purification Administration (CHABP2016-07), supported by Chinese Society of Nephrology Grant (13030310416), and funded by Special Supporting Program for Young Teachers in Kunming Medical University. BY was supported by a grant from Graduate Innovation Fund in Kunming Medical University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None of the authors declare any conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments of comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Bao, Y., Wang, YA., Xiao, H. et al. Serum endocan and circadian heart rate variability in non-dialysis stage 5 chronic kidney disease patients. Int Urol Nephrol 50, 2061–2066 (2018). https://doi.org/10.1007/s11255-018-1993-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-018-1993-8