
Abstract
In Lebanon, approximately one in four adolescents suffers from a psychiatric disorder. Alarmingly, 94% of adolescents with a mental disorder have not sought any treatment. This study assessed the effectiveness of an evidence-based school-based universal mental health intervention (the FRIENDS program) in reducing depression and anxiety symptoms in middle school students in Lebanon. A total of 280 6th graders aged 11–13 years were recruited from 10 schools in Beirut. Schools were matched on size and tuition and randomly assigned to intervention or control groups. The FRIENDS program was translated into Arabic, adapted, and then implemented by trained mental health professionals during 10 classroom sessions over 3 months. We assessed sociodemographic and relevant psychological symptoms by self-report, using the Scale for Childhood Anxiety and Related Disorders (SCARED), Mood and Feelings Questionnaire (MFQ), and Strengths and Difficulties Questionnaire (SDQ), at baseline. We re-administered these scales at 3 months post-intervention. There was a significant time × group interaction for the SDQ emotional score (p = 0.011) and total MFQ score (p = 0.039) indicating significant improvement in depressive and emotional symptoms in the intervention group. Subgroup analysis by gender showed a significant time × group interaction for the total SCARED score (p = 0.025) in females but not in males (p = 0.137), consistent with a reduction of anxiety symptoms in this stratum of the intervention group as compared with the control group. The FRIENDS program was effective in reducing general emotional and depressive symptoms among middle school students in this Lebanese study population. This intervention provides an opportunity for promoting mental health in Lebanese schools and reducing the treatment gap in mental health care.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Mental disorders are the leading contributor to years lived with disability in children and youth (Erskine et al. 2015) and are among the most prevalent disorders in childhood, affecting up to 14% of children and adolescents globally (Polanczyk et al. 2015). In the Eastern Mediterranean region, mental disorders are the greatest source of non-fatal disease burden, with the burden of depressive and anxiety disorders peaking in early adolescence (Charara et al. 2017). Despite their prevalence and burden in this age group, mental disorders remain underrecognized and undertreated, especially in Low- and Middle-Income Countries (LMICs) (Kieling et al. 2011). In Lebanon, for example, approximately 25% of adolescents are living with at least one mental disorder, with only 6% of those affected having ever sought professional mental health help (Maalouf et al. 2016).
Given this large treatment gap and the fact that more than 70% of mental disorders start before the age of 25 (Kieling et al. 2011), prevention and early intervention efforts are crucial (Kieling et al. 2011; Rahman et al. 2019). Recent evidence shows that interventions that target building resilience in school-aged children may be effective in reducing mental health problems (Davydov et al. 2010; Dray et al. 2017; Luthar et al. 2000). Resilience is the ability to maintain positive mental health and well-being despite emergent adversities (Herrman et al. 2011). The literature suggests that indicators of resilience include, but are not limited, to lower levels of anxiety and depressive symptoms, and higher scholastic performance and social skills (Herrman et al. 2011).
Multiple studies have shown promising effects for school-based interventions aimed at building resilience in children and adolescents (Dray et al. 2017; Murphy et al. 2017). One such intervention is the FRIENDS program, a universal preventive cognitive behavioral school-based intervention. The program was initially developed to treat childhood anxiety and depression in group settings, and since its initial trials in the 1990s, the program has accrued evidence not only of its effectiveness for the treatment of childhood anxiety in a group setting (Dadds et al. 1997; Shortt et al. 2001) but also of its benefits when delivered as a universal preventive intervention in the school environment (Barrett et al. 2006; Rose et al. 2009). The program has evolved from aiming to treat and prevent mental health difficulties to promote positive emotional well-being by focusing more on development of strengths. It is grounded in the principles of cognitive behavior therapy (CBT) aiming at building adaptive ways of thinking, behaving, and feeling (Beck 2011), and aligns with the core tenets of Positive Psychology focusing on skills/strengths building (Suldo 2016).
The FRIENDS program has been shown to be effective in reducing anxiety symptoms in youth (Barrett and Turner 2001; Lowry-Webster et al. 2012) with some existing evidence of greater reduction of these symptoms in girls as compared with boys (Lock and Barrett 2003; Pahl and Barrett 2010). Reductions in anxiety and depressive symptoms at 1-year follow-up were also observed (Lock and Barrett 2003). A subsequent follow-up study showed that the reductions in depression and anxiety symptoms were maintained for up to 3 years for grade six students whereas they were lost after 1 year for grade 9 students. This finding suggests that interventions targeting the reduction of anxiety and depression may have longer term benefits for younger students and that early preventive intervention may therefore be more advantageous than intervention at a later age (Barrett et al. 2006).
This is particularly relevant to disadvantaged communities, in which children are at higher risk of developing mental health difficulties (Kataoka et al. 2002). Lendrum et al. (2013) point out the urgent need for interventions to be translated and culturally adapted to specific communities at risk (e.g., from ethnic minority backgrounds in LMICs). For example, Barrett et al. (2000) adapted the FRIENDS program to a migrant refugee population in Australia and showed that it significantly reduced internalizing symptoms. In addition, Iizuka et al. (2014) adapted the intervention by replacing activities requiring reading and writing with creative tasks, music and art and conducted a study targeting ethnic minority groups in Australia. Results showed that the intervention benefited participants who were at risk for mental health problems at baseline.
The FRIENDS program was selected for implementation in this study given its strong evidence-base and endorsement by the World Health Organization as an effective intervention for the treatment and prevention of childhood anxiety and depression (World Health Organization (WHO) 2004). A meta-analysis related to the prevention of childhood and adolescent anxiety has shown that the FRIENDS program was more effective than other preventive interventions (Fisak et al. 2011). The My FRIENDS Youth program used in the current study is part of the FRIENDS’ intervention suite (Fun FRIENDS, FRIENDS for Life, My FRIENDS Youth, and Adult Resilience – Strong Not Tough). All of these versions share a similar theoretical background and framework, but each has different activities that are geared toward participants at specific stages of human development.
Although originally developed in English, the FRIENDS program has been translated into several other languages and has been successfully implemented in high-income countries (HICs) such as Sweden and Japan (Ahlen et al. 2012; Matsumoto and Shimizu 2016) as well as in LMICs such as Brazil and Mexico (Gallegos et al. 2012; World Health Organization (WHO) 2004).
Lebanon, a LMIC, has a history of war and civil strife that spanned decades (BBC 2018). Despite this context of conflict, trauma, and displacement, few school-based mental health interventions have been implemented locally, and these have been limited to post-war trauma group interventions (Karam et al. 2008). This study, therefore, aimed to (1) translate and adapt the FRIENDS program to the context of Lebanon, and (2) implement and evaluate the adapted Arabic version of the program in a sample of middle-school students in Lebanon. This paper focuses on the latter aim and examines the effectiveness of the adapted Arabic version of the program in reducing anxiety and depressive symptoms in a sample of 6th graders using a randomized controlled trial (RCT) design. Accordingly, we hypothesized that participants in the intervention group would show a reduction in emotional difficulties, depressive symptoms, and anxiety symptoms as compared with the control group.
Method
Intervention Adaptation and Implementation
My FRIENDS Youth, the version of the FRIENDS program targeting adolescents, was translated into the Arabic language by the research team. The lesson plans were translated to Arabic by three bilingual mental health professionals from the research team (translation) and then compared with the original English version by four members of the team who were not involved in the prior stage of the translation process (i.e., no back translation was conducted). Adjustments to the Arabic version were then made accordingly. All team members involved in the translation process were native Arabic speakers who were fluent in both written and oral English and Arabic.
The adaptation to the Arabic culture included substitution of examples given in the original curriculum to more locally salient ones (e.g., surfing changed to playing basketball). Likewise, content adjustment encompassed the replacement of English names and role models in the workbook with more culturally relevant and familiar Arabic names (e.g., replacing foreign entertainers with Arab ones). The adapted FRIENDS intervention delivery followed the original program’s protocol recommendations and comprised 10 weekly sessions lasting 45–50 min each. The sessions covered a variety of concepts related to resilience and mental health including understanding feelings, practicing empathy, learning to relax, challenging one’s thoughts, problem solving, and making and keeping friends.
The intervention was delivered in participating schools by facilitators and co-facilitators who were members of the research team; these facilitators and co-facilitators were all native Arabic speakers and were mental health professionals or trainees (i.e., master’s students in psychology, clinical psychologists, psychiatry residents, and post-doctoral research fellows). Six (86%) of the team members were female, and three (38%) were above the age of 30. Facilitators were responsible for the administration of the intervention and were assisted by co-facilitators who helped in managing the classroom and administering certain activities. All facilitators and co-facilitators underwent similar training on the FRIENDS program by trainers who had attended a 20-h certified “training-the-trainers” course. The course was also attended by other senior research team members. Weekly meetings were held with the facilitators and co-facilitators assigned to different schools to prepare for each week’s session and discuss challenges. After the delivery of each session, team members provided feedback on the process of implementation of that session.
School and Study Participant Selection
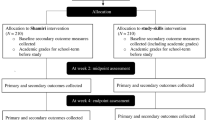
Schools in the greater Beirut area, where Lebanon’s capital is located, were identified from a list of schools posted on the website of the Ministry of Education. Inclusion criteria for schools were as follows: being private (independent schools), mixed-gender, tuition fees in the middle range, and having both grades six and seven (with two or more sections in grade six). Each school site was also required to have at least 15 consenting students in order to be included as a participating school (Fig. 1). Private schools were chosen given that most students in Lebanon attend private schools (Central Administration of Statistics, April 2012). Administrators of the schools that met inclusion criteria were contacted directly by telephone and were invited to participate in the study. Face-to-face meetings were then held with the school principals to go over the study protocol.

CONSORT flow diagram of participant recruitment, enrollment and progression through the study enrollment
Study Procedure
After a school agreed to participate, parents of students in grade six were invited to an in-school session held outside school hours to learn about the study. Subsequently, consent forms were sent out to parents along with the parental data collection forms (see “Assessments and Outcome Measures” section). After the baseline data collection was completed by consenting parents, children of consenting parents were approached in a classroom-based session during which the study was explained to them by the research team. Children of consenting parents who wished to participate in the study were assented by a research team member. Schools with a sufficient number of consenting parents and assenting participants were then randomized to either receive the intervention immediately (n = 5) or to the control group (n = 5). Schools that were in the control group were all waitlisted to receive the intervention the following academic year should it prove effective (Fig. 1). This process of recruitment resulted in the enrollment of 280 students in 10 schools.
Assessments and Outcome Measures
Participating students and their parents were asked to complete the self-report questionnaires listed below at baseline and immediately after the intervention (at 3 months). At baseline, parents were asked to provide sociodemographic information, including parental marital status, education, and employment, in addition to relevant clinical history (i.e., child history of seeking mental health care and family history of psychiatric illness) and academic information (parent’s perception of child’s school performance) concerning their child.
Strengths and Difficulties Questionnaire
The Strengths and Difficulties Questionnaire (SDQ) (Goodman 1997) is a 25-item, Likert-type rating scale used as general measure of emotional and behavioral difficulties of the child. It yields five subscores (emotional, conduct, hyperactivity, peer problems, and prosocial) and a total difficulties score (Goodman et al. 2018). The SDQ has presented satisfactory internal reliability (Cronbach’s α = 0.82) for the total scale (Warnick et al. 2008). The Arabic version of the SDQ that had been previously validated was used (Almaqrami and Shuwail 2004). We used the emotional subscale score as our main outcome measure since it is a proxy measure for emotional difficulties, and we used the total difficulties score as our secondary outcome measure. In our sample, the total SDQ score showed an acceptable internal reliability (Cronbach’s α = 0.71) with the SDQ emotional subscale showing a borderline acceptable reliability (Cronbach’s α = 0.68).
Mood and Feelings Questionnaire
The Mood and Feelings Questionnaire (MFQ) (Costello and Angold 1988) is a self-report measure of depressive symptoms for children and adolescents aged eight to eighteen. Both child and parent forms encompass items rated on a 3-point Likert type scale. An Arabic version was validated in a sample of Lebanese children and adolescents (Tavitian et al. 2014). It showed good internal reliability with a Cronbach’s α = 0.904 for the adolescent’s self-report. In our sample, the scale showed good reliability (Cronbach’s α = 0.92).
The Screen for Child Anxiety Related Emotional Disorders
The Scale for Childhood Anxiety and Related Disorders (SCARED) (Birmaher et al. 1997) is a self-report scale for children aged eight and above and their parents consisting of 41 Likert-like items. It screens for anxiety disorders in children and adolescents. We used the Arabic version that was validated in a sample of Lebanese children and adolescents and demonstrated good internal consistency (Cronbach’s α = 0.91) (Hariz et al. 2013). In our sample, the scale showed good reliability (Cronbach’s α = 0.92).
Data Analysis and Missing Data
We assessed the difference in sociodemographic characteristics and baseline scores of the above scales between the intervention and control groups. A chi-squared test was used to examine the association between two categorical variables and Student’s t test was used to compare mean values of variables across binary categories. Outcome variables were checked for normality and missing data using Little’s MCAR method (Lipsitz et al. 2000). Missing data were found to be missing at random.
For the SDQ subscales, missing data was replaced using the guidelines set by the SDQ developers. Participants with more than three items missing on a subscale were considered to have the entire subscale missing and had the score on that subscale replaced by the average score of that subscale of their assigned group (intervention or control) and gender that the participant with missing data values belonged to. Participants who had fewer than 25% of the items missing on the SCARED or MFQ subscales/scale had the missing items replaced by the participant’s average score of items on that subscale/scale. Participants who had 25% or more of items of the SCARED or MFQ subscales/scale missing were considered to have the entire scale missing and had the score on that scale replaced by the average score of that scale of the assigned group (intervention or control) and gender to which the participant belonged (Supplementary Table 1). Participants who did not fill out the questionnaires, at least partially, at baseline (n = 3) were excluded from the analysis, although they still took part in the program.
To address the issue of missing post-intervention data, a multiple imputation was used where 20 different imputations were run using a model that incorporated group status, baseline scores of the primary outcome variables, gender, and school ID. Generalized estimating equation (GEE) models were created to test the effect of the My FRIENDS Youth program on the primary outcome measures (SDQ emotional score, total SCARED score, and total MFQ score) and secondary outcome measures (SCARED subscale scores, SDQ subscale scores, and total SDQ score) as reported by the adolescents. GEE is a semiparametric statistical technique that is less sensitive to the misspecification of the covariance structure, or when the correlation between outcomes is unknown. GEE allows for analysis of repeated measurements and assumes that data within clusters are, to a certain degree, dependent (Hanley et al. 2003; Zeger et al. 1988). To decide what sociodemographic and clinical variables to include in the final model, variables were tested in a model that predicted the outcome variable score based on the variable of interest, time effect, and variable × time interaction. Final models included variables that were associated with the outcome measure (at a significance level < 0.05 for variable of interest effect or time × variable of interest effect), baseline scores of each of the outcome variables, and history of receiving psychiatric treatment (given its clear predictive association with the outcomes). To test the effect of the intervention on the outcome variables, a time × group interaction term was used with alpha set at 0.05.
The possible moderating effect of gender was tested by creating a three-way interaction term (gender × time × group). A similar three-way interaction was created to test the moderating effect of baseline risk status. The Statistical Package for the Social Sciences (SPSS) version 25 and STATA (version 13) were used to conduct the analysis.
Ethical Considerations
The study was approved by the Institutional Review Boards of the American University of Beirut and Harvard Medical School. Students who participated in the study signed an assent form and their parents/legal guardians provided written consent. In addition, after students completed assessments, team members screened the questionnaires to identify any student who answered in the affirmative to two questions concerning self-harm on the MFQ: “I thought about death or dying” and/or “I thought about killing myself.” These students were then assessed privately and face-to-face by a clinical psychologist or a psychiatrist/psychiatry resident who also contacted a parent/legal guardian by phone when indicated for follow-up care. Out of the 53 (19%) students who screened positively on the suicidality questions, none was deemed to be in immediate need of emergency services. Parents of all study participants were also provided with a list of mental health clinics. Schools that were waitlisted to receive the intervention were offered the intervention the following year.
Results
FRIENDS Implementation
Out of the 280 students enrolled in the 6th grade, 277 provided baseline data and were included in the analysis: 144 in the intervention group and 133 in the control group. In the intervention group, 11.8% of the participants (n = 17) attended one to three of the 10 sessions, 13.9% (n = 20) attended four to six sessions, and 74.3% (n = 107) attended seven or more sessions. Approximately 19% (n = 52) of the 277 students who were included in the analysis did not have post-intervention data. Out of the 52 participants with missing post-intervention data, more were from the intervention group than the control group (83% vs 17%; p < 0.001). There were no statistically significant differences between participants with missing post-intervention data and those with no missing post-intervention data with regard to MFQ, SCARED, and SDQ emotional and all sociodemographic variables (p > 0.05). Data was collected on several implementation measures including participant satisfaction and implementation delivery by facilitators and observers pertaining to dose received and dose delivered. We report in detail on those measures in an upcoming manuscript. With regard to fidelity, all facilitators delivering the sessions answered questions regarding intervention delivery. In total, 78 out of the total 107 sessions had forms filled by facilitators. When facilitators were asked to report on whether they were able to deliver the objectives of the sessions as outlined in the intervention manual (Extent of delivery, 0–25%, 26–50%, 51–75%, or 76–100%). Facilitators reported that in 78% of the sessions, 76 to 100% of the objectives were met.
Sociodemographic Characteristics of the Baseline Sample
The mean age of the participants was 12 years (+ − 0.50 years). Approximately half (53%) of the participants were girls; there were no between group differences in gender composition (p = 0.279). Participants in the intervention group had a significantly higher frequency of unmarried biological/adoptive parents compared with the control group (15% vs 5%; p = 0.011). At baseline, participants in the intervention group had higher scores on SDQ emotional (p = 0.002), SCARED (p = 0.002), and MFQ (p = 0.001) than those in the control group (Table 1).
Effect of FRIENDS Intervention on Primary and Secondary Outcomes
In the overall sample, there was a significant effect of time for the SDQ emotional subscale, the total SCARED score, and the total MFQ score (p < 0.001 for each) (Table 2). The impact of the intervention was observed via a significant time × group effect for the SDQ emotional symptoms (p = 0.011) and MFQ for depressive symptoms (p = 0.039) scores indicating that being in the intervention group was associated with a significant decrease in emotional and depressive symptoms compared with the control group over time (Table 2). No significant time × group effect was found for the total SCARED score nor any of the secondary outcomes (Total SDQ, SDQ conduct, SDQ hyperactivity, SDQ prosocial, SDQ peer problems, and SCARED subscale scores (p > 0.05 for all) (Table 2).
Additional Analyses
Moderating Effect of Gender on Anxiety Symptoms
The moderating effect of gender was observed via a statistically significant time × group × gender effect for the total SCARED score (p < 0.001). In post hoc analyses, the intervention was associated with a significant decrease in anxiety symptoms in girls (as measured by total SCARED scores) in the intervention group as compared with the control group as manifested by a significant time × group interaction (p = 0.025) which was not observed in boys (p > 0.05).
Sensitivity Analysis
Similar results to the general model were obtained for the main outcome variables when repeating the analysis without multiple imputation and when analyzing the data after excluding participants who attended fewer than seven sessions. In addition, when the analysis was repeated after excluding participants who did not have post-intervention data (N = 52), similar results regarding the SDQ emotional symptoms subscale and the total scores on the SCARED for anxiety symptoms to those presented above were obtained. In this model, however, the group × time effect on the total MFQ scores (depressive symptoms) approached statistical significance (p = 0.065).
Discussion
This study describes the first school-based preventive intervention that we know of which used the My FRIENDS Youth adapted program targeting emotional resilience in youth in Lebanon and neighboring Arab countries. Our results showed that the My FRIENDS Youth program was effective in reducing general emotional and depressive symptoms in 6th graders—and in reducing anxiety symptoms in 6th grade girls—who received the intervention as compared with a control group. This finding is consistent with previous studies that have shown the effectiveness of this intervention in reducing internalizing symptoms in other settings (Barrett et al. 2006; Lowry-Webster et al. 2012; Maggin and Johnson 2014).
Whereas the overall sample in the intervention group showed greater improvement in general emotional and depressive symptoms as compared with controls, only girls showed significant improvement in specific anxiety symptoms. This gender disparity in the anxiety outcome in this study sample was not surprising since previous research elsewhere has shown that girls responded better to the intervention (Barrett et al. 2006). One explanation may be that most of the facilitators and co-facilitators were females (Chan et al. 2006). Another explanation may be that boys were not as engaged as girls with the intervention. Our findings suggest that future implementation should consider possible adjustments in the intervention that respond to gender-specific differences and needs (for example, the inclusion of activities that enhance the engagement of male participants).
In addition, the fact that there was a significant improvement in emotional symptoms as measured by the SDQ emotional subscale in the overall intervention group as compared with controls but not in anxiety symptoms as measured by the SCARED may suggest that the SDQ emotional subscale—a measure of combined depression, anxiety, and somatic symptoms—is more sensitive to universal interventions than a specific anxiety scale such as the SCARED (Goodman et al. 2018). Our findings on depressive symptoms only approached statistical significance when the analysis was repeated after excluding participants who did not have post-intervention data. Although this difference in findings is most likely because the analytic sample for the sensitivity analysis was underpowered, the findings on depressive symptoms (as measured by MFQ) appear to be less robust than those on general emotional symptoms (as measured by SDQ).
An important study limitation relates to the poor parental response to parent-versions of the psychological assessments (only 40%). As a result, our analyses were based solely on adolescents’ self-reported measures which are limited by the fact that comprehension of the items may be affected by emotional and cognitive maturity of the adolescent (Grills and Ollendick 2003). Low parental response may stem from lack of interest, stigma toward mental health research and lack of psychological literacy (Maalouf et al. 2019). Future studies should aim at engaging multiple informants, including fathers, mothers, and teachers. Combining information from all these sources would provide a more accurate measure of the adolescent’s symptomatology (Jansen et al. 2017).
Future studies should also consider the inclusion of positive aspects of functioning in the assessment package, which would arguably provide a more robust assessment of resilience. However, the incorporation of additional assessments should be done with care, as our experience shows that lengthy assessments can increase the rates of missing data or decrease the number of participants who are willing to complete the assessment package.
In addition, participants in the intervention group had more severe symptoms of anxiety and depression at baseline than those in the control group. The choice of GEE in our analysis addresses the issue of baseline differences between the two groups since this statistical approach allows the groups to have different slopes and intercepts (Wang 2014). Baseline scores were also included in the analytic models in order to account for these differences.
Another study limitation was the sizeable attrition rate at post-intervention (almost 20%). However, compared with the percentage found in the literature, a retention rate of 80% is highly acceptable and similar to previous studies that have implemented this intervention (Lock and Barrett 2003). Although the major findings did not differ when using the imputed vs. the original datasets, it remains unclear how the attrition rate may have impacted our findings. In addition, we did not correct for family-wise when we ran each outcome as a separate model.
Classroom-specific factors such as class size, time allotted for the intervention, class dynamics, and facilitator characteristics may have also influenced the participants’ response to the intervention. These factors may have resulted in suboptimal implementation, although we provided quality control through ongoing monitoring in order to make sure that the objectives of each session were met in addition to weekly team meetings to discuss difficulties and possible solutions.
Conclusion
Our study is the first to show the effectiveness of a school-based intervention in reducing emotional symptoms—and thereby potentially building emotional resilience—in adolescents in Lebanon and the Arab world. In this regard, the My FRIENDS Youth program shows promise as an approach that can augment a response to the mental health needs of this population. This school-based approach has the potential to reduce the burden associated with mental illness and is aligned with the global mental health agenda of scaling up preventive interventions and interventions that improve access to care in low-resource settings such as Lebanon (Patel et al. 2013).
Targeting preventive interventions for adolescents is especially relevant, since developmentally, they are more likely to engage in health-risk behaviors, such as smoking, drinking, drug use, violence, and risky sexual behaviors (Jackson et al. 2012). Preventing the development of emotional difficulties and promoting positive social and emotional development in this age-group can have benefits throughout the life course and thus can support the improvement of general mental health and well-being of the general population (Jamal et al. 2013).
Future research should aim at testing the replicability of the intervention in a larger sample of students in both public and private schools while addressing the limitations faced in this early study. In addition, investigating the effectiveness of this intervention when implemented by teachers and when administered to special populations, such as refugees, would potentially inform an expanded scope of its practical relevance. The FRIENDS program has also shown promising results with former Yugoslavian refugees (Barrett et al. 2000). With Lebanon housing more than a million Syrian refugees (UNHCR 2018) and thousands of Palestinian refugees, extending the FRIENDS program to refugee children in Lebanon and the Middle East is highly relevant and could potentially mitigate the major public health burden of mental illness among a particularly vulnerable subpopulation.
References
Ahlen, J., Breitholtz, E., Barrett, P. M., & Gallegos, J. (2012). School-based prevention of anxiety and depression: A pilot study in Sweden. Advances in School Mental Health Promotion, 5, 246–257. https://doi.org/10.1080/1754730X.2012.730352.
Almaqrami, M. H., & Shuwail, A. Y. (2004). Validity of the self-report version of the strengths and difficulties questionnaire in Yemen. Saudi Medical Journal, 25, 592–601.
Barrett, P., & Turner, C. (2001). Prevention of anxiety symptoms in primary school children: Preliminary results from a universal school-based trial. The British Journal of Clinical Psychology, 40, 399–410. https://doi.org/10.1348/014466501163887.
Barrett, P. M., Moore, A. F., & Sonderegger, R. (2000). The FRIENDS program for young former-Yugoslavian refugees in Australia: A pilot study. Behaviour Change, 17, 124–133. https://doi.org/10.1375/bech.17.3.124.
Barrett, P. M., Farrell, L. J., Ollendick, T. H., & Dadds, M. (2006). Long-term outcomes of an Australian universal prevention trial of anxiety and depression symptoms in children and youth: An evaluation of the friends program. Journal of Clinical Child and Adolescent Psychology, 35, 403–411. https://doi.org/10.1207/s15374424jccp3503_5.
BBC (2018 ). Lebanon profile - Timeline. Retrieved from https://www.bbc.com/news/world-middle-east-14649284
Beck, J. S. (2011). Cognitive therapy for challenging problems: What to do when the basics don’t work. New York: Guilford Press.
Birmaher, B., Khetarpal, S., Brent, D., Cully, M., Balach, L., Kaufman, J., & Neer, S. M. (1997). The screen for child anxiety related emotional disorders (SCARED): Scale construction and psychometric characteristics. Journal of the American Academy of Child & Adolescent Psychiatry, 36, 545–553. https://doi.org/10.1097/00004583-199704000-00018.
Central Administration of Statistics, L. (2012). Education in Lebanon. Retrieved from http://www.cas.gov.lb/images/PDFs/SIF/CAS_Education_In_Lebanon_SIF3.pdf.
Chan, K. S., Bird, C. E., Weiss, R., Duan, N., Meredith, L. S., & Sherbourne, C. D. (2006). Does patient–provider gender concordance affect mental health care received by primary care patients with major depression? Women's Health Issues, 16, 122–132. https://doi.org/10.1016/j.whi.2006.03.003.
Charara, R., Forouzanfar, M., Naghavi, M., Moradi-Lakeh, M., Afshin, A., Vos, T., . . . Mokdad, A. H. (2017). The burden of mental disorders in the eastern Mediterranean region, 1990-2013. PLoS One, 12, e0169575. https://doi.org/10.1371/journal.pone.0169575.
Costello, E. J., & Angold, A. (1988). Scales to assess child and adolescent depression: Checklists, screens, and nets. Journal of the American Academy of Child & Adolescent Psychiatry, 27, 726–737. https://doi.org/10.1097/00004583-198811000-00011.
Dadds, M. R., Spence, S. H., Holland, D. E., Barrett, P. M., & Laurens, K. R. (1997). Prevention and early intervention for anxiety disorders: A controlled trial. Journal of Consulting and Clinical Psychology, 65, 627. https://doi.org/10.1037//0022-006x.65.4.627.
Davydov, D. M., Stewart, R., Ritchie, K., & Chaudieu, I. (2010). Resilience and mental health. Clinical Psychology Review, 30, 479–495. https://doi.org/10.1016/j.cpr.2010.03.003.
Dray, J., Bowman, J., Campbell, E., Freund, M., Wolfenden, L., Hodder, R. K., . . . Wiggers, J. (2017). Systematic review of universal resilience-focused interventions targeting child and adolescent mental health in the school setting. Journal of the American Academy of Child & Adolescent Psychiatry, 56, 813–824. https://doi.org/10.1016/j.jaac.2017.07.780.
Erskine, H. E., Moffitt, T. E., Copeland, W. E., Costello, E. J., Ferrari, A. J., Patton, G., . . . Scott, J. G. (2015). A heavy burden on young minds: The global burden of mental and substance use disorders in children and youth. Psychological Medicine, 45, 1551–1563. https://doi.org/10.1017/S0033291714002888.
Fisak, B. J., Richard, D., & Mann, A. (2011). The prevention of child and adolescent anxiety: A meta-analytic review. Prevention Science, 12, 255–268. https://doi.org/10.1007/s11121-011-0210-0.
Gallegos, J., Rodríguez, A., Gómez, G., Rabelo, M., & Gutiérrez, M. F. (2012). The FRIENDS for life program for Mexican girls living in an orphanage: A pilot study. Behaviour Change, 29, 1–14. https://doi.org/10.1017/bec.2012.8.
Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38, 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x.
Goodman, R., Ford, T., Simmons, H., Gatward, R., & Meltzer, H. (2018). Using the Strengths and Difficulties Questionnaire (SDQ) to screen for child psychiatric disorders in a community sample. British Journal of Psychiatry, 177, 534–539. https://doi.org/10.1192/bjp.177.6.534.
Grills, A. E., & Ollendick, T. H. (2003). Multiple informant agreement and the anxiety disorders interview schedule for parents and children. Journal of the American Academy of Child and Adolescent Psychiatry, 42, 30–40. https://doi.org/10.1097/00004583-200301000-00008.
Hanley, J. A., Negassa, A., Edwardes, M. D. D., & Forrester, J. E. (2003). Statistical analysis of correlated data using generalized estimating equations: An orientation. American Journal of Epidemiology, 157, 364–375. https://doi.org/10.1093/aje/kwf215.
Hariz, N., Bawab, S., Atwi, M., Tavitian, L., Zeinoun, P., Khani, M., ... & Maalouf, F. T. (2013). Reliability and validity of the Arabic Screen for Child Anxiety Related Emotional Disorders (SCARED) in a clinical sample. Psychiatry Research, 209, 222–228. https://doi.org/10.1016/j.psychres.2012.12.002.
Herrman, H., Stewart, D. E., Diaz-Granados, N., Berger, E. L., Jackson, B., & Yuen, T. (2011). What is resilience? The Canadian Journal of Psychiatry, 56, 258–265. https://doi.org/10.1177/070674371105600504.
Iizuka, C. A., Barrett, P. M., Gillies, R., Cook, C. R., & Miller, D. (2014). The FRIENDS emotional health program for minority groups at risk. The Journal of School Health, 84, 124–132. https://doi.org/10.1111/josh.12127.
Jackson, C., Geddes, R., Haw, S., & Frank, J. (2012). Interventions to prevent substance use and risky sexual behaviour in young people: A systematic review. Addiction, 107, 733–747.
Jamal, F., Fletcher, A., Harden, A., Wells, H., Thomas, J., & Bonell, C. (2013). The school environment and student health: A systematic review and meta-ethnography of qualitative research. BMC Public Health, 13, 798.
Jansen, M., Bodden, D. H. M., Muris, P., van Doorn, M., & Granic, I. (2017). Measuring anxiety in children: The importance of separate mother and father reports. Child & Youth Care Forum, 46, 643–659. https://doi.org/10.1007/s10566-017-9402-5.
Karam, E. G., Fayyad, J., Nasser Karam, A., Cordahi Tabet, C., Melhem, N., Mneimneh, Z., & Dimassi, H. (2008). Effectiveness and specificity of a classroom-based group intervention in children and adolescents exposed to war in Lebanon. World psychiatry : official journal of the World Psychiatric Association (WPA), 7, 103–109. https://doi.org/10.1002/j.2051-5545.2008.tb00170.x.
Kataoka, S. H., Zhang, L., & Wells, K. B. (2002). Unmet need for mental health care among US children: Variation by ethnicity and insurance status. American Journal of Psychiatry, 159, 1548–1555. https://doi.org/10.1176/appi.ajp.159.9.1548.
Kieling, C., Baker-Henningham, H., Belfer, M., Conti, G., Ertem, I., Omigbodun, O., . . . Rahman, A. (2011). Child and adolescent mental health worldwide: Evidence for action. Lancet, 378(9801), 1515–1525. https://doi.org/10.1016/s0140-6736(11)60827-1.
Lendrum, A., Humphrey, N., & Wigelsworth, M. (2013). Social and emotional aspects of learning (SEAL) for secondary schools: Implementation difficulties and their implications for school-based mental health promotion. Child and Adolescent Mental Health, 18(3), 158–164. https://doi.org/10.1111/camh.12006.
Lipsitz, S. R., Molenberghs, G., Fitzmaurice, G. M., & Ibrahim, J. (2000). GEE with Gaussian estimation of the correlations when data are incomplete. Biometrics, 56, 528–536. https://doi.org/10.1111/j.0006-341X.2000.00528.x.
Lock, S., & Barrett, P. M. (2003). A longitudinal study of developmental differences in universal preventive intervention for child anxiety. Behaviour Change, 20, 183–199. https://doi.org/10.1375/bech.20.4.183.29383.
Lowry-Webster, H. M., Barrett, P. M., & Lock, S. (2012). A universal prevention trial of anxiety symptomology during childhood: Results at 1-year follow-up. Behaviour Change, 20, 25–43. https://doi.org/10.1375/bech.20.1.25.24843.
Luthar, S. S., Cicchetti, D., & Becker, B. (2000). The construct of resilience: A critical evaluation and guidelines for future work. Child Development, 71, 543–562. https://doi.org/10.1111/1467-8624.00164.
Maalouf, F. T., Ghandour, L. A., Halabi, F., Zeinoun, P., Shehab, A. A., & Tavitian, L. (2016). Psychiatric disorders among adolescents from Lebanon: Prevalence, correlates, and treatment gap. Social Psychiatry and Psychiatric Epidemiology, 51, 1105–1116. https://doi.org/10.1007/s00127-016-1241-4.
Maalouf, F. T., Alamiri, B., Atweh, S., Becker, A. E., Cheour, M., Darwish, H., Ghandour, L. A., Ghuloum, S., Hamze, M., Karam, E., Khoury, B., Khoury, S. J., Mokdad, A., Meho, L. I., Okasha, T., Reed, G. M., Sbaity, E., Zeinoun, P., & Akl, E. A. (2019). Mental health research in the Arab region: Challenges and call for action. Lancet Psychiatry. https://doi.org/10.1016/S2215-0366(19)30124-5.
Maggin, D. M., & Johnson, A. H. (2014). A meta-analytic evaluation of the FRIENDS program for preventing anxiety in student populations. Education and Treatment of Children, 37, 277–306. https://doi.org/10.1353/etc.2014.0018.
Matsumoto, Y., & Shimizu, E. (2016). The FRIENDS cognitive behavioral program in Japanese schools: An examination of the treatment effects. School Psychology International, 37, 397–409. https://doi.org/10.1177/0143034316649639.
Murphy, J. M., Abel, M. R., Hoover, S., Jellinek, M., & Fazel, M. (2017). Scope, scale, and dose of the world’s largest school-based mental health programs. Harv Rev Psychiatry, 25, 218–228. https://doi.org/10.1097/hrp.0000000000000149.
Pahl, K. M., & Barrett, P. M. (2010). Preventing anxiety and promoting social and emotional strength in preschool children: A universal evaluation of the Fun FRIENDS program. Advances in School Mental Health Promotion, 3, 14–25. https://doi.org/10.1080/1754730X.2010.9715683.
Patel, V., Kieling, C., Maulik, P. K., & Divan, G. (2013). Improving access to care for children with mental disorders: A global perspective. Archives of Disease in Childhood, 98, 323–327.
Polanczyk, G. V., Salum, G. A., Sugaya, L. S., Caye, A., & Rohde, L. A. (2015). Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry, 56, 345–365. https://doi.org/10.1111/jcpp.12381.
Rahman, A., Hamoda, H. M., Rahimi-Movaghar, A., Khan, M., & Saeed, K. (2019). Mental health services for youth in the eastern Mediterranean region: Challenges and opportunities (editorial). Eastern Mediterranean Health Journal, 25, 80–81. https://doi.org/10.26719/2019.25.2.80.
Rose, H., Miller, L., & Martinez, Y. (2009). “Friends for life”: The results of a resilience-building, anxiety-prevention program in a Canadian elementary school. Professional School Counseling, 12, 400–407. https://doi.org/10.1177/2156759X0901200612.
Shortt, A. L., Barrett, P. M., & Fox, T. L. (2001). Evaluating the FRIENDS program: A cognitive-behavioral group treatment for anxious children and their parents. Journal of Clinical Child Psychology, 30, 525–535. https://doi.org/10.1207/S15374424JCCP3004_09.
Suldo, S. M. (2016). Promoting student happiness: Positive psychology interventions in schools. New York: Guilford Publications.
Tavitian, L., Atwi, M., Bawab, S., Hariz, N., Zeinoun, P., Khani, M., & Maalouf, F. T. (2014). The Arabic Mood and Feelings Questionnaire: psychometrics and validity in a clinical sample. Child Psychiatry and Human Development, 45, 361–368. https://doi.org/10.1007/s10578-013-0406-6.
UNHCR. (2018). Situation Syria regional refugee response. Retrieved from: https://data2.unhcr.org/en/situations/syria/location/71
Wang, M. (2014). Generalized estimating equations in longitudinal data analysis: A review and recent developments (Vol. 2014).
Warnick, E. M., Bracken, M. B., & Kasl, S. (2008). Screening efficiency of the Child Behavior Checklist and Strengths and Difficulties Questionnaire: A systematic review. Child and Adolescent Mental Health, 13, 140–147. https://doi.org/10.1111/j.1475-3588.2007.00461.x.
World Health Organization (WHO). (2004). Prevention of mental disorders: Effective interventions and policy options. Geneva: Author.
Zeger, S. L., Liang, K.-Y., & Albert, P. S. (1988). Models for longitudinal data: A generalized estimating equation approach. Biometrics, 44, 1049–1060. https://doi.org/10.2307/2531734.
Funding
This study was funded by the Harvard Medical School Center for Global Health Delivery–Dubai.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of Interest
Dr. Anne Becker reports the following: “Routledge/Taylor & Francis; anticipated royalties for edited book on global mental health training under contract.” Dr. Paula Barrett is the Director of Friends Resilience Pty Ltd. and Author of Friends Programs. She reports the following: “The research is Not for Profit based so no conflict of interest exists.” All other authors declare no conflict of interest.
Ethical Approval
The study was approved by the Institutional Review Boards of the American University of Beirut (AUB) and the Harvard Medical School (HMS). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (AUB IRB Protocol ID: PSY.FM.11 and HMS IRB Protocol ID: IRB17-0374) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Participants’ parents signed written informed consent and participants signed written assent.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
ESM 1
(DOCX 26 kb)
Rights and permissions
About this article

Cite this article
Maalouf, F.T., Alrojolah, L., Ghandour, L. et al. Building Emotional Resilience in Youth in Lebanon: a School-Based Randomized Controlled Trial of the FRIENDS Intervention. Prev Sci 21, 650–660 (2020). https://doi.org/10.1007/s11121-020-01123-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11121-020-01123-5