
Abstract
Recent efforts to explain the stark social and racial disparities in adverse birth outcomes that have persisted for decades in the U.S. have looked beyond prenatal factors, to explore preconception social conditions that may influence perinatal health via dysregulation of physiologic processes. The extant evidence supporting this link however remains limited, both due to a lack of data and theory. To address the latter, this manuscript generates a structured set of theoretical insights that further develop the link between two preconception social conditions—place and social relationships—and perinatal health. The insights propose the following. Place: necessarily encompasses all social contexts to which females are exposed from infancy through young adulthood; encompasses a variety of related exposures that, when possible, should be jointly considered; and may compound the effect of poverty—in childhood, adolescence, or young adulthood—on perinatal health. Social relationships: span relationships from early life through adulthood, and extend to intergenerational associations; often involve (or induce) major changes in the lives of individuals and should be examined with an emphasis on the developmental stage in which the change occurred; and can reflect a lack of social integration, or, social isolation. We also identify potential biological and social-structural mechanisms linking these preconception social conditions to perinatal health, and conclude by identifying promising directions for future research.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Adverse birth outcomes including preterm birth (PTB; delivery at less than 37 weeks) and low birth weight (LBW; <2500 g) represent the leading cause of neonatal and infant mortality, are associated with increased risk of health problems both in infancy as well as later in life, and are estimated to cost over $25 billion annually in the U.S. alone (Behrman and Butler 2005; Pallotto and Kilbride 2006; Blencowe et al. 2013). Moreover, these outcomes exhibit substantial racial, socioeconomic, and geographic disparities such that the most disadvantaged groups—i.e., non-Hispanic Black women, women with less than a high school education, women living in poor neighborhoods—exhibit the highest risk of adverse outcomes (Blumenshine et al. 2010; Schaaf et al. 2013; Hamilton et al. 2015). Of particular concern is that these disparities have persisted for decades and are not fully explained by the individual-level medical, behavioral, and social risk factors typically assessed during pregnancy (Culhane and Goldenberg 2011; Lhila and Long 2012; Braveman et al. 2015).
Scholars are increasingly shifting their focus to the preconception period (Atrash et al. 2006), given that prenatal care is increasingly considered “too little, too late” in terms of an opportunity to effectively intervene on factors that could prevent an adverse birth outcome (Lu et al. 2003). Much of this burgeoning literature examines women’s exposure to risk factors that are embedded within preconception social conditions (e.g., chronic stressors such as childhood poverty, abuse, and neglect; stressful life events); it is thought that such exposures can diminish perinatal health via behavioral or biological mechanisms [some key examples are: (Collins et al. 2009; Harville et al. 2010; Strutz et al. 2014; Witt et al. 2014a, b)].
However, the current state of evidence linking preconception social conditions to perinatal health outcomes is limited, largely due to two major barriers: the dearth of prospective, population-level data (preferably on a socioeconomically and racially diverse cohort of women) that are needed to test such pathways, and a lack of theoretical clarity about which—and through what pathways—social conditions may influence perinatal health. Thus, the extant body of literature has emerged more as a collection of risk factors identified based on data availability, rather than a systematic, deductive investigation of preconception social conditions most likely to influence perinatal health and pregnancy outcomes. The first barrier—a lack of data—is being addressed in exciting ways via new data collection efforts [see for example (Harris et al. 2013; Moss and Harris 2015)]. Addressing the second barrier—a lack of theoretical clarity—is the topic of the current paper.
The goal of this paper is to provide a structured set of theoretical insights into the preconception social conditions that likely influence perinatal health, and to identify plausible pathways of risk linking these social conditions to perinatal health. As we argue below, this is necessarily an interdisciplinary endeavor. On that basis, we define social conditions as “factors that involve a person’s relationships to other people,” in line with Link and Phelan's (1995) landmark study on social conditions as fundamental causes of disease (p. 81). Social conditions can thus include factors ranging from interpersonal relationships to positions occupied within social and economic structures in society and may include race, socioeconomic status, gender, stressful life events, or social support (p. 81). This definition is particularly well-suited for achieving the stated goal of this paper, because it encompasses a more traditional definition of social conditions—e.g., poverty, residential environment, factors that reflect the position one occupies within the social and economic structures of society—as well as a more nuanced definition that embeds individuals within social context, by including factors such as social support, stressful life events of a social nature, and relationships with intimates.
To accomplish this goal, we draw upon a wide body of theory and empirical evidence from sociology, epidemiology, psychology, and economics describing, in general terms, how social conditions influence health. When available, we incorporate theory and empirical evidence specifically related to the effect of social conditions on perinatal health. On this basis, we identify three preconception social conditions that plausibly have a demonstrable impact on perinatal health: childhood poverty, place, and social relationships. We focus our attention on place and social relationships because these have received relatively less attention in the literature. [See, for example, these studies examining childhood poverty/parental SES on perinatal health risk: (Harville et al. 2010, 2012; Gavin et al. 2011; Kane 2015; Margerison-Zilko et al. 2016)]. In doing so, this paper contributes a stronger theoretical foundation to this literature that can reinvigorate research on the preconception predictors of adverse birth outcomes; it also contributes greater cohesion to the extant research on preconception social conditions.
Conceptual Framework Guiding This Work
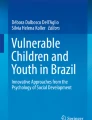
The figure (below) summarizes the theoretical insights proposed in this paper, and also visually situates these insights within the broader conceptual framework guiding this manuscript. Two key preconception social conditions—place and social relationships—are embedded within a broader social, structural, economic, and historical landscape. These two key social conditions are likely not independent, but rather intricately connected, often sharing a common context or cause. We propose that place and social relationships are linked with perinatal health, at least partially, through the set of mechanisms shown in the middle box, including access to resources, discrimination, dysregulation of the HPA axis, dampened or heightened immune response, changes in vasculature, neurocognitive changes, and health behaviors. These represent a rich, though not exhaustive, set of pathways linking place and social relationships to perinatal health. These mechanisms are assumed to operate primarily through a stress process model (Pearlin et al. 1981; Pearlin 1989, 1999). [We use the term “stress” loosely here; stress is a notably ambiguous term that is defined and interpreted in various ways throughout the literature (McEwen 2008). A useful working definition is provided by Gunnar and Quevedo (2007) who describe stress as, “a psychological condition in which the individual perceives or experiences challenges to physical or emotional well-being as overwhelming their ability and resources for coping.” Debate exists over whether the body’s developmental response to stress—particularly early life stress—is primarily pathological (i.e., the accumulation of stress damages health and development), or primarily adaptive (i.e., stress directs individuals to develop in ways that are adaptive to the perceived conditions, although development may appear pathological). Both perspectives, however, support the idea that early life stressors shape organisms’ development and health throughout life (Hostinar and Gunnar 2013)]. Undergirding these associations are a set of core theoretical perspectives guiding the theoretical insights proposed herein. The pathways depicted here may operate non-linearly and may not reflect direct causation; this is reflected in the figure by the inclusion of curved arrows linking each box to another.
Theory Describing How Social Conditions Impact Health
Scholars across multiple disciplines have developed numerous, overlapping theoretical frameworks to more fully describe how social conditions may impact health in general, and, perinatal health in particular (Syme and Berkman 1986; Hogue et al. 2001; Kramer et al. 2001; Ben-Shlomo and Kuh 2002; Misra et al. 2003; Culhane and Elo 2005; Rich-Edwards and Grizzard 2005; Glass and McAtee 2006; Warnecke et al. 2008; Kramer and Hogue 2009a, b; Center on the Developing Child at Harvard University 2010; Russ et al. 2014; Ramey et al. 2015a, b). To a large extent, these frameworks reflect the principles of four core theoretical perspectives: life course theory, life course epidemiology, biological embedding, and embodiment. Also relevant here is life course health development—a perspective developed specifically within the maternal and child health arena (Halfon and Hochstein 2002).
In the sections that follow, we first broadly argue why place and social relationships are plausibly linked with perinatal health through a stress process model, and describe a specific set of distal and proximal mechanisms proposed in the literature. We then introduce a set of six theoretical insights generated by studying the previously noted theoretical perspectives in depth, and outline the current state of evidence in each area. We conclude with an extensive discussion of promising directions for future research. [Hereafter, note that our use of the term “perinatal health” encompasses the clinical and sub-clinical health and well-being of both the mother and developing infant, and includes pregnancy complications, and outcomes such as LBW, PTB, and neonatal mortality].
Plausible Mechanisms Linking Two Key Preconception Social Conditions, Place and Social Relationships, to Perinatal Health
A stress process model connects three conceptually distinct but related areas: the sources of stress (circumstances such as life events, life strains, or self-concepts), mediating resources (such as coping or social supports), and manifestations of stress (the outcome, whether physiological, socioemotional, or otherwise) (Pearlin et al. 1981). In his influential early work on the sociology of stress, Pearlin (1989) emphasized the role of social conditions in this process: “Many stressful experiences, it should be recognized, don’t spring out of a vacuum but typically can be traced back to surrounding social structures and people’s locations within them” (p. 242). One example of social structures are social systems of stratification (e.g., social class, race/ethnicity, gender, age); when resources and opportunities are unequally distributed across society as a result of stratification, then low status within these social systems is a source of adversity and a drain on individuals’ capacity to cope (Pearlin 1989, 1999).
Next, we describe a set of distal (social) and proximate (biological, behavioral) mechanisms that are commonly referenced in the literature linking social conditions to health.
Distal (Social) Mechanisms
Understanding how place and social relationships influence an individual’s health and well-being is central to the field of sociology; therefore, we look to sociological theory and research to further understand potential mechanisms through which these social conditions influence perinatal health.
One fundamental sociological concept dates back to social theorist Max Weber, who argued that resources within the social environment are a key element linking the structure and process of place to individual well-being. Contemporary scholars expanded this notion, asserting that social conditions are a fundamental cause of disease, on the basis that social conditions constrain or promote access to key resources—such as knowledge, money, power, prestige, and interpersonal social networks and support—that can be used to prevent or treat disease (Link and Phelan 1995). The importance of resources and resource acquisition for one’s health has been similarly emphasized by public health scholars (Diez Roux and Mair 2010); indeed, Marmot (2005) argues that unequal access to resources and material deprivation are two key determinants of health disparities.
Consistent with a fundamental causes approach, place and social relationships are social conditions that can regulate access to the types of resources women can use to either prevent poor perinatal health or treat key risk factors of poor perinatal health. For example, place may condition access to knowledge about the importance of healthy eating and physical activity or the risks of smoking before or during pregnancy, which often circulates through local social networks. Social relationships may regulate access to financial resources: for example, married, and to a certain extent cohabiting, women often benefit from economies of scale that are associated with higher purchasing power to prevent or treat key risk factors of poor perinatal health.
Social environments also influence health by shaping social norms that govern individual behaviors, attitudes, and practices, facilitating high (or low) levels of social control that can limit (or foster) opportunities for individuals to engage in illegal or harmful behavior, and functioning as a source of social support and cohesion (Sampson et al. 2002; Kawachi and Berkman 2003; Sampson 2003; Braveman and Gottlieb 2014). Discrimination and institutional racism likely further condition women’s access to resources in ways that systematically diminish the perinatal health of Black (versus White) women (Feagin and Bennefield 2014; Phelan and Link 2015).
Another theoretical perspective on this topic emphasizes the role of risk regulators, which are characteristics of the social or built environments that promote (or constrain) individual-level health behaviors linked with the onset or progression of disease (Glass and McAtee 2006). Several categories of risk regulators are proposed; we propose suppositions regarding preconception risk regulators within most of original set of categories that may be particularly central in linking place to perinatal health. In the category of material conditions, sufficient availability of nutritious foods throughout early life is a plausible risk regulator in that it is structured by place, and has important consequences for the development of healthy eating habits that can carry over into pregnancy, thereby influencing perinatal health. Similarly, residential segregation (falling in the category of discriminatory practices) and fear of crime (falling in the category of neighborhood/community conditions) are plausible risk regulators in that each is structured by place and has important implications for the adoption of protective or detrimental health behaviors throughout the preconception period. A lower-than-average cigarette tax (in the category of laws, policies, and regulations) in addition to social norms that convey a widespread tolerance of smoking (in the category of behavioral norms) may promote adolescent initiation of smoking, which is linked with long-term smoking behavior and higher levels of addiction, both of which increase women’s risk of continued smoking throughout pregnancy—a clear risk factor for poor perinatal health.
This discussion of risk regulators brings to mind the notion that women arrive at pregnancy in very different states (physical, mental, emotional, and otherwise), and these states likely influence perinatal health. An embodiment perspective takes this notion one step further, proposing that current health is a function of past experiences; therefore, it is necessary to consider the life course exposure history of a person up until the point she is exposed to a certain social condition. This is important because not all bodies are similarly equipped to resist physiological dysregulation (for example) resulting from social stress (Del Giudice et al. 2011). More broadly, this perspective emphasizes the dual importance of understanding the health effects of place and social relationships as well as the biological process through which social conditions manifest in the body. The next logical step is to further understand proximate (biological and behavioral) mechanisms linking preconception social conditions to perinatal health.
Proximate (Biological and Behavioral) Mechanisms
Culhane and Elo (2005) proposed a novel framework whereby neighborhood context (indicated by the social environment, service environment, and physical characteristics) and individual-level factors (psychosocial well-being, social support, health behaviors) impact birth outcomes directly and indirectly via maternal stress physiology. Their framework broadly reflects the concepts of biological embedding and embodiment given that social conditions directly or indirectly influence biological and physiological pathways that in turn influence health. On this basis, we now speculate on a likely set of potential biological and behavioral mechanisms linking place and social relationships, as two key preconception social conditions, to perinatal health.
Biological embedding highlights several specific candidate mechanisms by which social conditions gets under the skin. These include the hypothalamic–pituitary–adrenal (HPA) axis, autonomic nervous system (epinephrine and norepinephrine), development of the prefrontal cortex (memory, attention, and executive function), and systems of social affiliation (neural basis) (Hertzman and Boyce 2010).
The HPA axis is one of two primary systems, along with the sympathetic-adrenomedullary system, by which stress responses are affected in humans (Gunnar and Quevedo 2007). Hormones related to the HPA axis have received substantial attention as a possible mechanism transmitting social stress to perinatal outcomes. In particular, corticotropin-releasing hormone (CRH) is associated with the cascade of events that includes cervical softening, weakening of fetal membranes, uterine contractions, and birth (Challis et al. 2000) and is elevated in women who go on to deliver preterm (Hobel et al. 1999). However, a causal relationship linking CRH to PTB has not been confirmed. Glucocorticoids (GCs) are also thought to play a critical role in fetal development and long-term outcomes (Seckl and Meaney 2004).
Immune or inflammatory mechanisms have also been proposed as mechanisms connecting social stress and perinatal health. Evidence suggests that, whereas acute stress upregulates immune responses, chronic stress downregulates—i.e., suppresses—immune activity, potentially leaving the immune system weakened and more susceptible to infection. Indeed, infections such as bacterial vaginosis (BV)—a risk factor for PTB that is more prevalent in Black compared to White women—have been proposed as one pathway linking social stress to perinatal outcomes. Evidence of this pathway is mixed however (Kramer and Hogue 2009a, b).
Vascular function, particularly as it relates to the development of and blood flow to the placenta, is another proposed mechanism by which social stress may impact perinatal health. Cardiovascular disease research suggests that social stress may be related to vascular function, but little empirical work has examined this hypothesis during pregnancy. Increasingly, pregnancy studies are collecting placentas [see for example (Kelly et al. 2009)], providing an opportunity to examine the placenta for pathological indicators of vascular damage.
Emerging evidence suggests other biological mechanisms that could also play a role in the biological embedding of social conditions with respect to perinatal health. For example, stress may have effects on neurocognitive or neurobehavioral pathways (Hertzman and Boyce 2010); indeed animal studies have demonstrated effects of stress on neural structure and functioning (Christoffel et al. 2011). Epigenetic pathways whereby stress may impact gene expression without altering the DNA structure have also been proposed (Thayer and Kuzawa 2011; Russ et al. 2014). Researchers have also recently begun to investigate the role of the vaginal and even placental microbiome in perinatal health; the role of social factors and stress in this relationship remains unknown.
Much work has identified associations between self-reported measures of social stress—such as life events, daily hassles, and pregnancy anxiety—and increased risk of PTB and LBW (Kramer and Hogue 2009a, b; Dunkel Schetter 2011). Yet, despite the identification of these associations and the biological plausibility of mechanisms by which social stress may influence perinatal health, empirical work has largely failed to find connections between proposed biomarkers of stress (e.g., plasma CRH, maternal hair cortisol, or placental histological features consistent with inflammation/infection or vascular damage) and self-reported measures of stress, distress, or anxiety in pregnant women (Kramer et al. 2009, 2013). Thus, the link between social stress, biological mechanisms, and birth outcomes remains largely hypothetical.
Much of the aforementioned empirical research has, however, focused on examining measures of both social and biological stress during pregnancy. The perspective termed accelerated or reproductive aging suggests that exposure to cumulative social disadvantage and inequality across the life course—as well as across generations—results in biological wear and tear on women’s bodies that become manifest in perinatal health outcomes. Geronimus (1992) proposed that the health of Black women may begin deteriorating earlier in life compared to the health of White women due to years of “weathering” associated with accumulated exposure to systematic inequality. Indeed, Geronimus found that the black–white disparity in LBW increases with age and that this increase is most extreme for poor Black mothers (even relative to non-poor Black mothers). A related concept termed “allostatic load” describes the cumulative biological wear and tear on bodies resulting from chronic stress; measures of allostatic load utilize multiple biomarkers to measure functioning across organ systems including cardiovascular, immune, and the HPA axis (Seeman et al. 2010; Ramey et al. 2015a, b). Relatedly, telomere length has been proposed as a possible mechanism linking stress experienced in a parental generation to offspring health (Haussmann and Heidinger 2015). New advances in measuring telomere length may provide a measure of biological aging that could be used in future research on this topic.
Place as a Key Preconception Social Condition Influencing Perinatal Health
As we have argued, place is an important preconception social condition with critical consequences for perinatal health. On that basis, we propose three theoretical insights that further develop this notion. [Note that place is often associated with childhood poverty—another preconception social condition we identify. Here we attempt to identify some of the unique contributions of place to perinatal health by drawing upon specific assertions of the five core theoretical perspectives we consider that are squarely focused on place].
Theoretical Insight 1: Place, as a Key Preconception Social Condition, Necessarily Encompasses all Social Contexts to Which Females are Exposed from Infancy through Young Adulthood
Life course theory, which emerged from sociology and human development, proposes that the trajectories individuals follow—health-related or otherwise—are enveloped within a lifetime of experiences spanning both time (at a unique point in history) and place (within a specific geographical context). These trajectories are influenced by (and simultaneously influence) the people with whom individuals engage, and the social institutions individuals encounter, on a daily basis. The interplay of these macro and micro-level factors shapes the exposures, constraints, and opportunities that individuals encounter as they move through the life course (Elder 1977, 1998; Elder and Giele 2009). Furthermore, as a developmental theory, life course theory proposes that individuals will be differentially influenced by varying social contexts through the life course (Elder and Rockwell 1979). [Note that these are also key notions of ecological systems theory; see (Bronfenbrenner 1979, 1994). More is said on this theory in Kramer et al.’s contribution to this volume]. For example, the home is particularly important for infants and children; schools are especially the key during adolescence; neighborhoods and workplaces are influential in young adulthood as individuals strike out on their own and enter the labor market.
Along these same lines, life course health development (LCHD), proposed by Halfon and Hochstein (2002), posits that accumulations of health deficits across the life course are likely to be more important indicators of perinatal health risk than simply poor health or low SES during pregnancy. Health assets (the converse of health deficits) are fundamentally shaped not only by a woman’s biology, but also by health-promoting and risk-reducing strategies present in the social conditions she encounters throughout the life course.
A similar principle is foundational to life course epidemiology—a theoretical perspective that builds on life course theory but explicitly integrates evidence of the social and biological origins of disease from across the life course (Ben-Shlomo and Kuh 2002; Kuh et al. 2003). This perspective emerged in part as an attempt to explain the socioeconomic gradient observed in many health outcomes, which often cannot be fully explained by examining risk factors contemporaneous with the health outcome—a notion that implies the necessity of looking further back in the early life course, to identify stressful or toxic exposures that are ultimately linked with the development of adult morbidity. Place represents a key source of such exposures that may impact development of health either during discrete periods or in a cumulative manner.
Thus, by examining multiple theoretical perspectives, it becomes clear that it is not only necessary to locate women within a given social and historical place, but it is also necessary to factor in the lifetime of previous experiences and exposures women encounter, Indeed, scholars have argued for the importance of examining the effects of lifetime neighborhood environments on perinatal health risk [see for example, (Love et al. 2010)]. On the basis of the theory described here, we propose the need to expand this view even further, to also include the home, school, and workplace environments from infancy through young adulthood. Therefore, we derive the insight that place, as a key preconception social condition, should be (a) characterized by females’ neighborhood, school, home, work, and social environments, (b) considered in a historical context, and (c) examined from infancy to adulthood.
As a concrete example, consider that girls growing up in resource-poor neighborhoods are likely to be regularly exposed to other place-based stressors, including resource-poor school districts, high rates of neighborhood crime, and stressful home environments. Thus, in the language of life course epidemiology, such a constellation of place-based stressors likely accumulate across the life course, ultimately overwhelming the body’s capacity to function in a normal, healthy state. Living in a disadvantaged neighborhood or home may also increase a young girl’s risk of experiencing events labeled by life course epidemiology as “trigger events,” meaning events that set off a chain of risk factors leading to an adverse health outcome later on. Trigger events such as physical or sexual abuse or witnessing violence in the neighborhood for example may lead to more risky health behaviors and eventually impact women’s health during pregnancy.
Health-promoting factors—e.g., adequate nutrition, healthy diet, opportunities for physical activity, and appropriate health and sex education—during critical or sensitive periods (Ben-Shlomo and Kuh 2002; Kuh et al. 2003; Kuh and Shlomo 2004) are more likely to be absent in socially disadvantaged homes, schools, and neighborhoods. This buttresses our theoretical insight in that we would expect life course risk to be greater among those who are situated in these disadvantaged “places,” and particularly among those that have experienced this disadvantage for some length of time and/or during early life.
Such an examination would substantially extend past research, which has nearly exclusively examined mother’s neighborhood environment at the time of birth, instead of her neighborhood (or home, or school) environment at the time of preconception, adolescence, or childhood. One important exception is Love et al. (2010) who found that Black women who are born in poor neighborhoods and are still poor as mothers (indicating cumulative exposure to disadvantage) exhibit significant weathering (indicated by increasing risk with increasing maternal age) with respect to LBW and small for gestational age (although not for PTB). On the other hand, Black women who lived in upper-income areas both at birth and at the time of their own pregnancy demonstrated little evidence of weathering, similar to White women.
Beyond these studies, however, we know very little about the longer term pathways that may trace perinatal health risk back to (1) exposure to deleterious neighborhood environments during critical or sensitive periods, and/or (2) cumulative exposure to deleterious neighborhood environments across the life span. Consistent with ecological systems theory, it is possible that the effects of neighborhoods in childhood have less of a direct impact in comparison with the effects of the home environment; still, analyses exploring both types of exposure are necessary, and theoretically sound. Furthermore, no work we know of has examined the role of the school environment on perinatal health, which may be particularly important during the developmental stage of adolescence; nor has any work examined how females’ neighborhood, home, school, and work environments independently (or jointly) contribute to perinatal health risk.
Indirect support of the life course place-based approach we identify stems from studies documenting that risk factors for adverse perinatal outcomes measured during pregnancy often do not fully explain socioeconomic or racial/ethnic disparities in those outcomes (Culhane and Goldenberg 2011; Lhila and Long 2012; Braveman et al. 2015); we interpret this as evidence pointing to the need to examine life course influences (and not as evidence suggesting these disparities are biologically predetermined). Indirect evidence also stems from other literatures: a recent study examined neighborhood exposures over the life course and found that omitting earlier life course neighborhood environments overestimated the effect of current neighborhood environment on personal income and underestimated the total effect of neighborhoods (Miltenburg and van der Meer 2016). Other research finds that long-term measures of neighborhood, e.g., duration of exposure to neighborhood disadvantage, are more strongly associated with self-rated health compared to measures of neighborhood at a single point in time (Do 2009). This logic plausibly extends to the case of perinatal outcomes.
Theoretical Insight 2: Place, as a Key Preconception Social Condition, Encompasses a Variety of Related Exposures That, When Possible, Should be Jointly Considered
The concept of embodiment, put forth by Krieger (2005a, b) is grounded in social epidemiology and is poised to understand health at the population-level. This perspective suggests that bodies tell stories about the “dynamic social, material, and ecological contexts into which we are born, develop, interact, and endeavor to live meaningful lives” [p. 350, (Krieger 2005a, b)], thereby illuminating an array of interrelated place-based stressors. This focus on a multiplicity of interrelated stressors is also central to one of the core contributions of embodiment—that is, a shift away from a more classic “disembodied” epidemiologic approach that focuses on isolated risk factors measured at a single point in a person’s life course, and towards a perspective that examines whether health disparities are biological manifestations of many social factors, such as racism, discrimination, or inequality. A key emphasis here is on the process through which an individuals’ exposure to social conditions is internalized, thereby altering physiological function; this process is necessarily multilevel, integrating factors across the micro, meso, and macro levels.
Based on this perspective, it is clear that exposure to unhealthy social conditions—such as low quality housing, toxicants in the environment, or unsafe neighborhoods throughout a woman’s life—may, to some extent, be manifestations of the same macro-level process signaling institutionalized discrimination towards racial minorities or the unjust structuring of society relative to income and socioeconomic position. Although these notions are generally contextualized within urban environments, exposure to the same unhealthy social conditions in rural areas can also signal an unjust structuring of society along the lines of social class, as studies from Appalachia and other rural areas have shown (Hartley 2004). Overall, these unhealthy social conditions can therefore signal place-based processes through which racial or social inequality can be embodied among mothers, ultimately shaping population-level patterns of inequalities in perinatal health. Thus, we propose that exposure to multiple place-based social conditions should be considered jointly, whenever possible. Such an endeavor would likely be advantageous, both empirically—in terms of avoiding omitted variable bias—and conceptually—in terms of illuminating the same macro-level process underlying several place-based social conditions.
In the extant literature, evidence has amassed linking LBW and PTB to socially patterned neighborhood exposures, resources, and stressors, including neighborhood deprivation (Pickett et al. 2002; Buka et al. 2003; Messer et al. 2006), neighborhood poverty histories (Margerison-Zilko et al. 2015), neighborhood affluence (Kane et al. 2016), residential segregation (Bell et al. 2006; Grady 2006; Walton 2009), local crime rates (Morenoff 2003; Messer et al. 2006; Schempf et al. 2009), environmental toxicants (Morello-Frosch and Shenassa 2006), and mother’s negative perception of her neighborhood environment (as it relates to police presence, social services, cleanliness, level of noise, and quality of schools) (Collins et al. 1998; Wallace et al. 2015). However, very few studies, examine more than one type of exposure within the same study. More work is needed that jointly examines exposures to multiple place-based social conditions, and how they contribute to perinatal health. Advanced statistical models allowing for the joint estimation of neighborhood-effects and school-effects, via cross-classified multiple membership models for example [see Teitler and Weiss (2000) for a substantive application of this method], could be useful in testing this theoretical insight in the case of perinatal health.
Theoretical Insight 3: Place, as a Key Preconception Social Condition, May Compound the Effect of Poverty—in Childhood, Adolescence, or Young Adulthood—on Perinatal Health
Similar to life course epidemiology, biological embedding emerged as a way of understanding and explaining the socioeconomic gradient in health. Diverging from the classic medical and epidemiological thinking regarding disease causation, however, Hertzman and Boyce (2010) argued that exposure to social conditions can impact developmental outcomes in a way that is non-linear and sometimes unpredictable, unlike the specific relationship between, for example, infection and disease.
More specifically, this perspective posits that adverse experiences in early life, such as persistent childhood poverty, are biologically embedded in individuals via physiological processes involving neural development, gene regulation of brain and body development, and adaptation of the stress response system (Hertzman 2006; Center on the Developing Child at Harvard University 2010; Hertzman and Boyce 2010). Furthermore, exposure to a harsh environment in childhood and adolescence—or, one that involves multiple and cumulative stressors over time—can hinder the body’s ability to deal with stressors or insults stemming from other risk factors such as socioeconomic disadvantage, effectively amplifying the deleterious effects of childhood poverty on health (Flier et al. 1998; Hertzman and Power 2006; Center on the Developing Child at Harvard University 2010). Thus, the influence of childhood poverty on health may be conditioned by place-based social conditions within the family, neighborhood, or school. This also illustrates the broader principle that social exposures are nested within complex, dynamic systems that involve interaction between aspects of the system over time. Therefore, we propose that the link between early life poverty and perinatal health may be compounded by place, with the poorest outcomes observed among women exposed to both early life poverty and multiple, severe negative place-based social conditions (in the neighborhood, home, school, or social environment).
No studies have yet examined this proposition in relation to perinatal health. However, considerable evidence supporting this type of moderating effect has emerged in studies examining early life adversity and pro-inflammatory responses (Miller and Chen 2010; Saxton et al. 2011; McDade 2012), childhood poverty and social subordination in classrooms (Boyce et al. 2012), low maternal education and maternal negativity (Browne and Jenkins 2012), and parental death and familial susceptibility to suicide (Hollingshaus et al. 2016).
Social Relationships as a Key Preconception Social Condition Influencing Perinatal Health
Children’s social relationships in early life with both adults (vertical attachments) and peers (horizontal attachments) (Hartup 1989) are key sources of support and socialization—provided these relationships are generally positive and not extremely stressful (McLeod and Almazan 2003)—that also have important implications for health (Repetti et al. 2002; Shonkoff et al. 2012). Recall that Link and Phelan’s definition of social conditions encompasses relationships to intimates. Therefore, we propose that social relationships are a key preconception social condition with important consequences for perinatal health. Note that, although social relationships are related, to some extent, to experiences of early life adversity such as childhood poverty, abuse, neglect, and/or a harsh family environment, in this paper we focus on the nuances that distinguish it as its own construct, and the unique way in which preconception social relationships matter for perinatal health.
Theoretical Insight 4: Social Relationships, as a Key Preconception Social Condition, Span Relationships from Early Life through Adulthood, and Extend to Intergenerational Associations
The principles of lifespan development and linked lives suggested by life course theory and life course epidemiology propose that individual well-being is shaped by one’s experiences and exposures encountered throughout the lifespan, and is also critically affected by the experiences of previous generations. Indeed, scholars have proposed that perinatal health has roots in the mother’s physiological health, behaviors, and exposures not only during pregnancy, but also during the mother’s early life (e.g., in childhood, adolescence) and dating back to previous generations (Richardson et al. 2012). LCHD expands upon this notion in that health potential, or more specifically “reproductive potential,” is conceptualized as a combination of multiple factors: intergenerational effects (a woman’s “starting” value), acceleration or deceleration in women’s developmental trajectory during sensitive periods, and the number of risk factors (dampening health potential) and protective factors (boosting health potential) across the life course (Halfon and Hochstein 2002; Lu and Halfon 2003).
Biological embedding adds an important nuance. Whereas life course epidemiology—which stems from the epidemiology of chronic disease literature—focuses more on specific, discrete, and non-quotidian exposures, biological embedding—which stems more from the human development literature—focuses more on mundane exposures (e.g., daily hassles, chronic strain). Therefore, a biological embedding perspective would add the important qualification that poor perinatal health risk can be traced back to social relationships in early life and to intergenerational exposures, and, these need not be exceptional, but may be unremarkable in nature. Therefore, we suggest that social relationships as a key preconception social condition span relationships, both ordinary and exceptional, from early life through adulthood and date back to intergenerational associations.
Past empirical studies have assessed the role of mother–father relationships during pregnancy in contributing to perinatal health (Padilla and Reichman 2001; Kimbro 2008); others have focused on prenatal social support from a number of different social ties [see for example, Feldman et al. (2000)]. Additionally, considerable attention has been placed on intergenerational associations and birth weight. One set of studies examine similarities between mothers’ and daughters’ birth weight outcomes, and the social processes—such as maternal income—mediating this association (Conley and Bennett 2000, 2001; Currie and Moretti 2003, 2007). Other studies identify risk factors and pathways of risk contributing to poor perinatal health that date back multiple generations, such as intergenerational transmissions of low maternal education (Kane 2015; McFarland et al. 2016).
In contrast, only a handful of studies have examined the effect of social relationships in early life on perinatal health. Physical violence in (pre-pregnancy) dating relationships has been linked with lower birth weight among Black teen mothers (Madkour et al. 2014). Early life sexual and physical abuse also has clear implications for birth outcomes (Noll et al. 2007; Nerum et al. 2013; Schei et al. 2014; Margerison-Zilko et al. 2016). Richer insights however would likely emerge through an assessment of a broader set of social relationships across the early life course.
We also know little about potential risk factors that are on the pathway between early life social relationships and perinatal health. Compelling indirect evidence stems from a study by Harville et al. (2010) that found a consistent, graded association between exposure to hardships (e.g., low levels of parent–child warmth, material deprivation) in childhood and adolescence, with a higher risk of maternal smoking during pregnancy and adverse birth outcomes. Other work indicates that exposure to abuse and economic problems in both childhood and adulthood are associated with increased depressive symptomology during pregnancy (Holzman et al. 2006). Future work should build on this foundation, more explicitly tracking the effects of a variety of key social relationships in early life on perinatal health, with an eye towards understanding longer term intergenerational processes that may contribute to poor perinatal health.
Theoretical Insight 5: Social Relationships, as a Key Preconception Social Condition, Often Involve (or Induce) Major Changes in the Lives of Individuals and Should be Examined with an Emphasis on the Developmental Stage in Which the Change Occurred
The principle of linked lives proposes that the lives of children are inextricably linked to that of their parents, particularly early on (Elder 1996). Thus, challenges facing parents are necessarily shared by children insofar as they induce change in a realm that is shared by all family members. For example, a parental job loss that causes a family to move from one city to another in search of new employment necessarily affects all members of the family. Residential mobility often requires children to change schools and form new friendships—both of which can be stressful experiences, particularly during key stages of development, such as adolescence. Multiple spells of parental unemployment (Christoffersen 1994) and residential mobility among children in fragile or unsupportive families (Hagan et al. 1996) have been shown to be problematic for children.
Cleavages of key family relationships, such as parental divorce or death, are another major change that can be particularly stressful for children, especially if the event occurs within a sensitive or critical period of child or adolescent development. If the event is combined with other interpersonal stressors (such as a move, or starting a new school), a life course epidemiology approach would propose that an accumulation of risks model may apply—whereby the accumulated risks overwhelm the body’s capacity to function in a normal, healthy state. A chains of risk model may also be theoretically supported wherein one exposure leads to another, which in turn leads to another exposure or health outcome. Chains of risk may include trigger events (e.g., divorce, loss of a family member, a move, a health event, experiencing abuse or trauma) that may help identify key points in the life course where chains of risk can be broken for vulnerable individuals. Life course epidemiology also tells us that (a) these models likely operate simultaneously within individuals, (b) risk factors and environments contemporaneous with the outcome also matter, and (c) life course models must be specific to the exposures and outcomes of interest.
To the extent that major changes in social relationships early on in life involve a change in social conditions (e.g., a move to a poorer neighborhood), these experiences may also leave indelible physiological marks on women’s bodies through biological embedding or embodiment. According to embodiment for example, food insecurity or exposure to toxicants—both of which may result from a sudden reduction in family income (in the case of parental job loss) or a move to a poorer neighborhood (in the case of parental death, divorce, or job loss)—are concrete experiences through which social disadvantages experienced in early life may potentially be embodied within individuals in the form of worse perinatal health. Overall, these suppositions suggest a potential linkage between major changes in key social relationships in early life—particularly if these occur during a sensitive period in the life course—and higher risk for poor perinatal health.
Specifically related to timing, life course theory emphasizes that the timing of events and life transitions is key. Life course epidemiology proposes a number of pathways through which early life exposures, such as childhood poverty or cumulative adversity, influence adult health outcomes. For example, the actions of certain exposures may act only during critical periods, resulting in irreversible, lifelong effects on the structure or function of the body (e.g., lack of folate around the time of conception is linked to neural tube defects), or during sensitive periods (e.g., childhood nutrition is important for growth but nutrition can affect growth at other times as well) (Flinn and England 1997; Ben-Shlomo and Kuh 2002; Kuh et al. 2003; Evans and Kim 2007). [Attention to developmental stage is likely to be important for the entire set of theoretical insights proposed herein, although, for the sake of space, we selected only this insight to more fully develop this notion. Note that developmental stage is implicitly addressed in Theoretical Insights 1, 3, and 4].
One potentially relevant sensitive period may be early childhood—a period in which socialization is paramount, and the precursors of adulthood human and financial capital begin to take shape. Another may be adolescence when a young woman enters puberty and her reproductive life span begins. However, as an important caveat, the biological embedding perspective cautions against drawing artificially clear-cut and unidirectional links between these potentially sensitive periods and health, because social causation is iterative, and recursive, and leads to cumulative wear and tear.
To date, scholars have formed insightful scales representing an array of preconception stressful life events—some of which involve major changes in social relationships, such as death of a loved one or parental divorce—and demonstrate implications for perinatal health (Khashan et al. 2009; Witt et al. 2014a, b; Cheng et al. 2015). Less attention has been devoted however to contextualizing these events within a given developmental stage. Another study found that, when combined into a scale, chronic stressors experienced in childhood and adolescence (e.g., low parental education or income, parent receiving public assistance, not having health insurance, living without either biological parent, living in a high-poverty or high-unemployment neighborhood), but not acute stressors (e.g., death of a family member or friend; respondent attempted suicide; respondent reported being threatened with or injured by a knife or gun, was shot or stabbed), were associated with lower birth weight (Strutz et al. 2014). Growing up in a single-parent or stepparent family (versus two biological parent family) may influence the birth weight of a woman’s infant later in life (Kane 2016). More research is needed to clarify the association between major changes in preconception social relationships and perinatal health, with an emphasis on developmental stage in which the change occurred.
Furthermore, many of the major changes we discuss reflect parent–child processes. However, no study has yet explored the theoretical underpinnings of these processes the way we do here. Doing so illuminates the multi-generational process that reflects the principle of linked lives, and underlies many of the major changes in social relationships discussed herein. This is a subtle, but theoretically important point that has not yet been a focus in this literature.
Our proposed conceptualization also brings into focus the cumulative nature of some of the major changes in social relationships we discuss (e.g., when a parental divorce induces a residential move, a change in schools, and the formation of new friendship groups) that can leave indelible physiological marks on individuals and ultimately impact perinatal health. This type of approach would benefit from the application of different statistical methods than have been used in the past—e.g., a principal components analysis to identify a set of major changes in social relationships that tend to cluster together, and then assessing the effect of this cluster on perinatal health.
In addition, it would be illuminating to evaluate these multi-generational processes as well as the cumulative nature of major changes in social relationships with a focus on the developmental stage in which the events occurred. Two studies have paved the way for such a venture. Harville et al. (2010) examined multiple hardships in both childhood and adolescence and found that exposure to violence and dealing with mental health problems during early adolescence (ages 12–16) had a stronger impact on LBW than did exposure to the same stressors before age 11, lending evidence that adolescence may be a sensitive period for such exposures. Additionally, Margerison-Zilko et al. (2016) examined stressors related to economic issues, loss of a loved one, abuse, and substance use in someone close, comparing exposures in childhood, adulthood, and just prior to pregnancy. Abuse, particularly sexual abuse, in both childhood and adulthood emerged as an independent risk factor for PTB, suggesting that—at least with regards to abuse—chronic exposure, rather than exposure only during a sensitive period, might be most risky. Future work should build on these studies by assessing the multi-generational processes underlying such hardships and stressors, and exploring alternative ways to model the accumulation of stressors and its impact on perinatal health.
Theoretical Insight 6: Social Relationships, as a Key Preconception Social Condition, Can Reflect a Lack of Social Integration, or, Social Isolation
Social isolation, or a lack of social interaction, is a well-known and powerful predictor of poor health (Berkman and Glass 2000; Berkman et al. 2000). In population-based, prospective studies, social isolation in childhood has been linked with elevated levels of C-reactive protein (Lacey et al. 2014) and increased cardiovascular risk (Caspi et al. 2006) in adulthood. Here, we consider theory that links social isolation to perinatal health.
The principle of linked lives underscores the importance of social integration and social ties (Elder 1995); both of these factors critically shape behaviors, beliefs, and attitudes via processes such as socialization and social control (Erikson 1950). This socialization is the key to understanding social inequalities in health (Singh-Manoux and Marmot 2005). Women without strong ties to parents or peers in childhood and adolescence may experience undue levels of stress, and therefore may be at particularly high risk of poor perinatal health. As previously argued, when parental job loss necessitates a family move, this places a strain on children’s (or adolescent’s) peer relationships given that moves are commonly associated with temporary spells of social isolation for youth. Re-integration with peers in the new location is essential for children in terms of limiting the health effects of the social isolation spell. If a move occurs within a sensitive period, the effect of social isolation may be more deleterious to the child’s health than if the move occurred at another point in the life course. In addition, social isolation is associated with poorer psychological health and depressive symptomology (Thoits 1983), which may lead to uptake of, or increase in, unhealthy behaviors such as smoking. Depression may influence perinatal health via increased smoking behavior (Zuckerman et al. 1989; Orr et al. 2002).
According to biological embedding, a positive family environment demonstrated by high levels of parent–child warmth, communication, and caring can likely mitigate the deleterious effects of early life adversity on health (Connor and Brink 1999; Shonkoff and Phillips 2000; Kristenson et al. 2004; Hertzman and Power 2006; Evans and Kim 2007; Center on the Developing Child at Harvard University 2010; Hertzman and Boyce 2010); this likely holds for perinatal health as well. Conversely, it is plausible that social isolation reflects a negative social environment that modulates the stress response system, neural development, and systems of social affiliation in such a way that increases the risk of poor perinatal health.
No studies we are aware of have directly examined the effects of social isolation on perinatal health. However, we can draw on the adult health literature to formulate hypotheses about what we would expect to find. A large body of work shows a clear association between social isolation and mortality risk (Holt-Lunstad et al. 2010). Furthermore, a recent study produced causal evidence for a mechanism linking social integration/social isolation to health (measured with both biomarkers and self-reports) via physiological regulation across the life course (Yang et al. 2016). An innovative and complex conceptual model proposes a link from social networks to health via a variety of psychosocial mechanisms (e.g., social support, social influence, social engagement, person-to-person contact, and access to resources and material goods) and pathways (health, psychological, and physiologic) (Berkman et al. 2000). Together, this body of research buttress the plausibility of an effect of social isolation on perinatal health; potential mechanisms may be physiologic, health, and/or psychological dysregulation. Future studies should test these suppositions.
Promising Directions for Future Research
Demographic Approaches Could be Employed to Test Some of the Proposed Theoretical Insights
Demographers regularly examine changes in a phenomenon across historical time by distinguishing between age, period, and cohort effects; another common approach is to parse out the timing, duration, spacing, and order of events across the life course (McLeod and Almazan 2003). Both approaches could be useful in further understanding the role of preconception place and social relationships in contributing to perinatal health. There is a lack of demographic analyses such as these in the perinatal health literature, although one recent study examined age, period, and cohort effects in relation to perinatal health and identified a strong relationship between maternal birth cohort (i.e., when the mother was born) and risk of having a small for gestational age baby later in life (Margerison-Zilko 2014). In particular, among Black women only, mothers born in the 50s and 60s exhibited declining risks of having a small for gestational age infant, whereas mothers born in the 70s or 80s exhibited increasing risks of small for gestational age (regardless of when the mother actually gave birth), illustrating the importance of accounting for the social context experienced by a woman from birth through pregnancy. Potential explanations for these findings include that improving social conditions for Black people during the 50s and especially during the Civil Rights Movement of the 1960s may have become embodied in Black women in such a way as to improve their perinatal health later in life. Moreover, social and economic changes that especially burdened the Black community in the 1970s and 1980s—including declining manufacturing jobs, growing inner city poverty, and increasing proportions of single-parent families—may have also become embodied in ways that led to greater perinatal risk later in life.
Multi-Generational Processes Should be Further Explored
A common theme throughout many of the theoretical insights proposed herein is that potentially rich insights may be gleaned by conceptualizing and modeling preconception social conditions through an intergenerational lens. Indeed, understanding not only the mother’s early life course experiences through a more comprehensive lens of place and social relationships, but also understanding the experiences of her parents, which may have critically shaped her early life experiences, could lend a more comprehensive understanding of the set of risk factors leading to poor perinatal health. As previously noted, prior studies have laid the groundwork for exploring these associations (Conley and Bennett 2000, 2001; Currie and Moretti 2003, 2007; Kane 2015; McFarland et al. 2016), but much more work is needed to parse out these socially and biologically complex pathways. Furthermore, such explorations could expand our understanding of infant health as a mechanism transmitting social, health, and economic, disadvantage from one generation to the next (Case et al. 2002; Case and Paxson 2006; Kane 2015, 2016). This topic holds particular significance in the field of population health, given that the very nature of this intergenerational transmission implies that improving infant health for all and reducing racial and social class disparities in infant health could have dramatic implications not only for the health and well-being of future generations but also for population-level patterns of racial and social inequality.
A Need to Examine Racial Stratification of these Pathways in Relation to Perinatal Health
Although our paper focuses primarily on conceptualizing pathways through which place and social relationships, as preconception social conditions, influence perinatal health, future work should explore stratification of these pathways by race/ethnicity. Substantial and persistent racial disparities are evident in perinatal health, particularly in the U.S. For example, Black U.S. women have almost twice the risk of delivering a baby preterm or low birth weight compared to White women. Because Black women are more likely to live in disadvantaged neighborhoods throughout their lifetime, to grow up and live in poverty, and to experience more family instability and family related stressors than White women in the U.S. (Bumpass and McLanahan 1989; Geronimus 1996; Collins et al. 2009), it is plausible that detrimental exposures within these preconception social conditions place a unique burden on Black women, children, and families. Furthermore, racism—at the institutional-level and the individual-level—is a fundamental cause of health inequalities (Phelan and Link 2015) that affects Black women and women of other marginalized or non-majority groups (Feagin and Bennefield 2014). The effects of racism are particularly pernicious given that racism conditions access to resources in such a way that systematically advantage the majority group. These resources can span from an individual’s social psychological beliefs in the superiority of one group over another, to the dense concentration of Whites in positions of power and authority in both the public and private sectors. Therefore, future research should pay considerable attention to the way that these processes act to structure and/or interact with place and social relationships.
A Focus on Resilience, Not Just Risk
An important area of focus for future work lies in identifying, examining, and potentially developing interventions around sources of resiliency at the individual, family, and community levels (Ramey et al. 2015a, b). For example, evidence suggests that the detrimental effects of stress on health may be mitigated by high levels of mastery, self-esteem, and/or social support (Thoits 2010); such factors may be important moderators of the association between preconception social conditions and adverse birth outcomes.
Sources of resiliency at the family-level are under-researched in this area; the role of the father in perinatal health has been particularly under-explored [see Landale and Oropesa (2001) and Kimbro (2008) for two key exceptions]. Evidence suggests that the mere absence of a father’s name on the birth certificate (an omission that likely proxies for low levels of paternal involvement) is correlated with infant mortality and that paternal absence increases the Black–White gap in infant mortality by approximately fourfold (Alio et al. 2011). At the same time, researchers should not underestimate the power of alternative or non-traditional relationships in developing resiliency. Mothers may rely not only on the father, but also on family members, friends, or community sources of social support (Collins 2005; Hrdy 2009). In fact, recent work in the field of communications identified online social support groups, particularly those on Facebook, as key sources of information and support for new mothers (Holtz et al. 2015).
Improvements in Measuring Preconception Social Conditions
The difficulty of gathering valid and reliable indicators of social conditions is well-documented in the perinatal health literature and beyond (Thoits 1982; Collins et al. 1993). Objective measures of place such as the Euclidean distance from a women’s home to the nearest OB/GYN facility or healthy food market oversimplifies the role of place in a woman’s life. For example, if two women live equidistant from an OB/GYN facility, one may have more trouble accessing the resource due to a lack of transportation, lack of child care, or lack of social support. Moreover, other aspects of place (e.g., perceived safety, social cohesion) are difficult to measure objectively.
Considerable difficulty emerges from measuring social relationships as well. Families are becoming increasingly complex and diverse as divorce, cohabitation, and non-marital childbearing are becoming more commonplace in the U.S. (Bumpass et al. 1995). With respect to romantic relationships, cohabitation is particularly difficult to measure (Knab and McLanahan 2006) for two reasons: dates of union entry or exit are difficult to pinpoint (Manning and Smock 2005), and cohabitation includes a diverse array of residential arrangements (Sassler 2004). Furthermore, changes in relationship status between the time when couples learn of a pregnancy and the time of birth (e.g., unmarried to married, or non-residential to cohabiting) are not uncommon (Bachu 1999; Rackin and Gibson-Davis 2012); importantly, the influence of marriage on birth outcomes differs based on the timing of marriage (whether it was formalized before or during the pregnancy) (Kane 2016). Yet nearly all studies examining the influence of marriage on birth outcomes measure marital status at the time of birth, and not the time of conception.
The theoretical insights expressed here suggest the need to measure several, multilevel exposures at multiple time points—as well as biological indicators of proximal processes and perinatal health—among girls and women. This need to measure a “totality of exposure” [related to the epidemiologic concept of the “exposome” (DeBord et al. 2016)], suggests the need for compiling measurements from diverse methods such as biomarker collection, sensors, geographic, or spatial systems, as well as from traditional surveys, data linkage, and vital statistics.
A particular problem in perinatal health research is that, to maximize resources, women are typically enrolled in studies once pregnant, instead of being enrolled before conception. Thus, assessment of any preconception risk factors relies on either retrospective self-report or record linkage (which is notoriously difficult and limited, especially in the U.S.). However, longitudinal, population-based studies such as the National Longitudinal Study of Adolescent to Adult Health offer promising new opportunities to test the influence of preconception risk factors and pathways of risk on perinatal health. Add Health has prospectively tracked men and women from ages 12–19 (Wave I, 1994–5) to ages 24–32 (Wave IV, 2008–9), with current efforts underway to collect a new wave of data (Wave V, 2016–18). Many of these respondents have had children; those who have transitioned to parenthood provide reports of the infant’s birth weight, gestational age, etc. These data can be further mined to more fully explore and test some of the preconception pathways proposed in this paper.
Using Quasi-Experimental and Other Complex Modeling Strategies
Whereas traditional statistical methods have focused on modeling associations between one exposure and an outcome, the ideas and relationships expressed in this paper will require statistical methods designed to incorporate multilevel, complex, dynamic, life course, and/or intergenerational exposures. Such methods may include structural equation or complex systems models. Quasi-experimental study designs including instrumental variables, difference-in-difference models, and regression discontinuity should also be considered. Future work should also more explicitly test the robustness of these associations by employing multiple methods in a single study, or by performing cross-national tests of documented pathways.
Specific challenges to statistical modeling include the difficulty of explicitly linking preconception social conditions to measures of proximal mechanisms (e.g., physiological dysregulation), and then to perinatal health. This limitation stems from two factors: a lack of data needed to test such hypotheses, and the complexity of statistical models required to test such hypotheses.
Another remaining challenge is how to explicitly test multiple life course epidemiology models—i.e., cumulative exposure, sensitive/critical periods, chains of risk—with the goal of identifying whether and how timing of exposure matters for perinatal health. As described above, the small but growing empirical literature has identified that being born in a disadvantaged neighborhood, experiencing hardships in childhood, experiencing abuse, and loss/death of loved ones in the years just prior to pregnancy are all related to adverse birth outcomes. On the other hand, upward social mobility appears protective against adverse birth outcomes. Taken together, the existing literature suggests that exposure to social stress or disadvantage at all of these time points can be detrimental to perinatal health. Yet few studies have tested multiple time periods or different life course models against each other. Moreover, the possibility remains that current research indicating risk based on exposure in all time periods reflects only publication bias against studies not identifying associations between early life disadvantage and perinatal outcomes.
More Attention to Selection Processes Confounding the Effect of Preconception Social Conditions on Perinatal Health
Rooted in our efforts to advocate for the identification of theoretically relevant pathways that should be tested in future research is the notion that future researchers should be expressly mindful of the underlying selection mechanisms that may confound the association between preconception social conditions and perinatal health. Such mechanisms could reflect health selection—wherein poor health either structures women’s social relationships or limits women’s earnings thereby impacting where she lives [see (Halfon and Hochstein 2002; Russ et al. 2014)]—or social selection (pathways leading poor women into low status jobs, low wage jobs, or unsafe neighborhoods).
It is also true that not all factors that precede preconception social conditions (e.g., the social, structural, economic, and historical landscape referenced in Fig. 1) and also affect perinatal health are observable, no matter how rich the data. Therefore, the effect of preconception social conditions on perinatal health remains confounded unless we explicitly account for this in some way. This point reiterates the necessity of using quasi-experimental methods to achieve unbiased estimates of the effect of preconception social conditions on perinatal health. The evidence stemming from studies employing econometric methods (such as instrumental variables modeling) that shore up evidence of a causal effect of prenatal smoking on poor perinatal health (Rosenzweig and Schultz 1983; Lien and Evans 2005; Reichman and Teitler 2005; Wehby et al. 2011) is one concrete example of the type of work that could be undertaken in the future to tease out the effects of preconception social conditions.

Conceptual framework describing how two key preconception social conditions that are embedded within a broader social, structural, economic, and historical landscape may influence perinatal health
Another key example is a set of studies arguing that our understanding of the (potentially) causal role of place on perinatal health is still quite limited (Oakes 2004; Roux 2004; Subramanian 2004). Of particular difficulty, here is the inability (thus far) to adequately model processes that select individuals into the neighborhoods in which they reside—an issue that creates problems related to confounding and omitted variable bias. A related limitation that has, to the best of our knowledge, not yet been addressed is that scholars in this field have not yet attempted to estimate the causal effects of neighborhoods on perinatal health apart from the causal effects of families on perinatal health. This is an area of strong interest in economics [see for example Plotnick and Hoffman (1999)]. Future work testing the theoretical insights developed in this paper should, whenever possible, use quasi-experimental methods that take into account some of these issues related to these selection processes.
Conclusion
LCHD scholars have laid the groundwork for considering preconception risk and protective factors for perinatal health (Halfon and Hochstein 2002; Russ et al. 2014), yet a lack of theoretical work has limited researchers from forming well-grounded hypotheses about which factors to examine. The goal of this paper was to provide a structured set of theoretical insights for understanding the preconception social conditions that likely influence perinatal health. To that end, this paper introduced two key preconception social conditions—place and social relationships—that have received relatively less attention in the literature than the other social condition we identify (childhood poverty). This paper also generated a set of new, integrative theoretical insights by drawing upon life course theory, life course epidemiology, life course health development, biological embedding, and embodiment. We put forth hypotheses as to a set of (distal) social-structural and (proximate) biological and behavioral mechanisms linking these preconception social conditions to perinatal health outcomes. Lastly, we identified several promising areas for future research in this area. Taken together, these insights contribute more solid theoretical grounding for future research to test specific hypotheses related to the role of preconception social conditions in perinatal health than has been offered in the past. Along with new data collection efforts that seek to gather the population-level data (on socioeconomically and racially/ethnically diverse sets of individuals) needed to test such claims, future research can and should begin testing the theoretical insights and mechanisms identified in this paper.
References
Alio, A. P., Mbah, A. K., Kornosky, J. L., Wathington, D., Marty, P. J., & Salihu, H. M. (2011). Assessing the impact of paternal involvement on racial/ethnic disparities in infant mortality rates. Journal of Community Health, 36(1), 63–68.
Atrash, H. K., Johnson, K., Adams, M., Cordero, J. F., & Howse, J. (2006). Preconception care for improving perinatal outcomes: The time to act. Maternal and Child Health Journal, 10(1), 3–11.
Bachu, A. (1999). Trends in premarital childbearing: 1930 to 1994. US Department of Commerce, Economics and Statistics Administration, US Census Bureau.
Behrman, R., & Butler, A. (Eds.). (2005). Preterm birth: Causes, consequences, and prevention. National Academies Press: Washington, DC.
Bell, J. F., Zimmerman, F. J., Almgren, G. R., Mayer, J. D., & Huebner, C. E. (2006). Birth outcomes among urban African-American women: a multilevel analysis of the role of racial residential segregation. Social Science & Medicine, 63, 3030–3045.
Ben-Shlomo, Y., & Kuh, D. (2002). A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. International Journal of Epidemiology, 31(2), 285–293.
Berkman, L. F., & Glass, T. (2000). Social integration, social networks, social support, and health. Social Epidemiology, 1, 137–173.
Berkman, L. F., Glass, T., Brissette, I., & Seeman, T. E. (2000). From social integration to health: Durkheim in the new millennium. Social Science and Medicine, 51(6), 843–857.
Blencowe, H., Cousens, S., Chou, D., Oestergaard, M., Say, L., Moller, A. B., et al. (2013). Born too soon: The global epidemiology of 15 million preterm births. Reprod Health, 10(Suppl 1), S2.
Blumenshine, P., Egerter, S., Barclay, C. J., Cubbin, C., & Braveman, P. A. (2010). Socioeconomic disparities in adverse birth outcomes: A systematic review. American Journal of Preventive Medicine, 39(3), 263–272.
Boyce, W. T., Obradović, J., Bush, N. R., Stamperdahl, J., Kim, Y. S., & Adler, N. (2012). Social stratification, classroom climate, and the behavioral adaptation of kindergarten children. Proceedings of the National Academy of Sciences, 109(Supplement 2), 17168–17173.
Braveman, P., & Gottlieb, L. (2014). The social determinants of health: It’s time to consider the causes of the causes. Public health Reports, 129, 19–31.
Braveman, P. A., Heck, K., Egerter, S., Marchi, K. S., Dominguez, T. P., Cubbin, C., et al. (2015). The role of socioeconomic factors in black–white disparities in preterm birth. American Journal of Public Health, 105(4), 694–702.
Bronfenbrenner, U. (1979). Contexts of child rearing: Problems and prospects. American Psychologist, 34(10), 844.
Bronfenbrenner, U. (1994). Ecological models of human development. Readings on the Development of Children, 2, 37–43.
Browne, D. T., & Jenkins, J. M. (2012). Health across early childhood and socioeconomic status: Examining the moderating effects of differential parenting. Social Science and Medicine, 74(10), 1622–1629.
Buka, S. L., Brennan, R. T., Rich-Edwards, J. W., Raudenbush, S. W., & Earls, F. (2003). Neighborhood support and the birth weight of urban infants. American Journal of Epidemiology, 157(1), 1.
Bumpass, L., & McLanahan, S. (1989). Unmarried motherhood: Recent trends, composition, and black-white differences. Demography, 26(2), 279–286.
Bumpass, L. L., Raley, R. K., & Sweet, J. A. (1995). The changing character of stepfamilies: Implications of cohabitation and nonmarital childbearing. Demography, 32(3), 425–436.
Case, A., Lubotsky, D., & Paxson, C. (2002). Economic status and health in childhood: The origins of the gradient. American Economic Review, 92, 1308–1334.
Case, A., & Paxson, C. H. (2006). Children’s health and social mobility. The Future of Children, 16(2), 151–173.
Caspi, A., Harrington, H., Moffitt, T. E., Milne, B. J., & Poulton, R. (2006). Socially isolated children 20 years later: Risk of cardiovascular disease. Archives of Pediatrics and Adolescent Medicine, 160(8), 805–811.
Center on the Developing Child at Harvard University. (2010). The foundations of lifelong health are built in early childhood. Retrieved from http://developingchild.harvard.edu/.
Challis, J. R., Matthews, S. G., Gibb, W., & Lye, S. J. (2000). Endocrine and paracrine regulation of birth at term and preterm 1. Endocrine Reviews, 21(5), 514–550.
Cheng, E. R., Park, H., Wisk, L. E., Mandell, K. C., Wakeel, F., Litzelman, K., Chatterjee, D., & Witt, W. P. (2015). Examining the link between women’s exposure to stressful life events prior to conception and infant and toddler health: the role of birth weight. Journal of Epidemiology and Community Health: jech-2015-205848.
Christoffel, D. J., Golden, S. A., & Russo, S. J. (2011). Structural and synaptic plasticity in stress-related disorders. Reviews in the Neurosciences, 22(5), 535–549.
Christoffersen, M. N. (1994). A follow-up study of longterm effects of unemployment on children: loss of self-esteem and self-destructive behavior among adolescents. Childhood, 2(4), 212–220.
Collins, P. H. (2005). The meaning of motherhood in black culture and black mother–daughter relationships. In M. B. Zinn, P. Hondagneu-Sotelo, M. A. Messner, & A. M. Denissen (Eds.), Gender through the prism of difference (pp. 285–295). New York: Oxford University Press.
Collins, J. W., David, R. J., Symons, R., Handler, A., Wall, S., & Andes, S. (1998). African-American mothers’ perception of their residential environment, stressful life events, and very low birthweight. Epidemiology, 9(3), 286–289.
Collins, N. L., Dunkel-Schetter, C., Lobel, M., & Scrimshaw, S. C. (1993). Social support in pregnancy: psychosocial correlates of birth outcomes and postpartum depression. Journal of Personality and Social Psychology, 65(6), 1243.
Collins, J. W., Jr., Wambach, J., David, R. J., & Rankin, K. M. (2009). Women’s lifelong exposure to neighborhood poverty and low birth weight: a population-based study. Maternal and Child Health Journal, 13(3), 326–333.
Conley, D., & Bennett, N. G. (2000). Is biology destiny? Birth weight and life chances. American Sociological Review, 458–467.
Conley, D., & Bennett, N. G. (2001). Birth weight and income: interactions across generations. Journal of Health and Social Behavior, 450–465.
Connor, S., & Brink, S. (1999). Understanding the early years: Community impacts on child development. Working Paper No. W-099-6E. Ottawa: Human Resources Development Canada, Applied Research Branch.
Culhane, J. F., & Elo, I. T. (2005). Neighborhood context and reproductive health. American Journal of Obstetrics and Gynecology, 192(5), S22–S29.
Culhane, J. F., & Goldenberg, R. L. (2011). Racial disparities in preterm birth. Seminars in perinatology. St Louis: Elsevier.
Currie, J., & Moretti, E. (2003). Mother’s education and the intergenerational transmission of human capital: Evidence from college openings. The Quarterly Journal of Economics, 118(4), 1495–1532.
Currie, J., & Moretti, E. (2007). Biology as Destiny? Short-and long-run determinants of intergenerational transmission of birth weight. Journal of Labor Economics, 25(2), 231–264.
DeBord, D. G., Carreón, T., Lentz, T. J., Middendorf, P. J., Hoover, M. D., & Schulte, P. A. (2016). Use of the “exposome” in the practice of epidemiology: A primer on-omic technologies. American Journal of Epidemiology, kwv325.
Del Giudice, M., Ellis, B. J., & Shirtcliff, E. A. (2011). The adaptive calibration model of stress responsivity. Neuroscience and Biobehavioral Reviews, 35(7), 1562–1592.
Diez Roux, A. V., & Mair, C. (2010). Neighborhoods and health. Annals of the New York Academy of Sciences, 1186(1), 125–145.
Do, D. P. (2009). The dynamics of income and neighborhood context for population health: Do long-term measures of socioeconomic status explain more of the black/white health disparity than single-point-in-time measures? Social Science and Medicine, 68(8), 1368–1375.
Dunkel Schetter, C. (2011). Psychological science on pregnancy: stress processes, biopsychosocial models, and emerging research issues. Annual Review of Psychology, 62, 531–558.
Elder, G. H. (1977). Family history and the life course. Journal of Family History, 2(4), 279.
Elder, G. H., Jr. (1998). The life course as developmental theory. Child Development, 69(1), 1–12.
Elder, G. H., Jr., & Giele, J. Z. (2009). Life course studies: An evolving field. In G. H. Elder Jr. & J. Z. Giele (Eds.), The Craft of life course research (pp. 1–24). New York: The Guilford Press.
Elder Jr, G. H. (1995). The life course paradigm: Social change and individual development. In Moen, P., Elder Jr, G. H. & K. Lüscher (Eds.), Examining lives in context: Perspectives on the ecology of human development (pp. 101–139). Washington, DC, US: American Psychological Association. doi:10.1037/10176-003.
Elder Jr, G. H. (1996). Human lives in changing societies: Life course and developmental insights. Developmental Science, 31–62.
Elder, G. H., & Rockwell, R. C. (1979). The life-course and human development: An ecological perspective. International Journal of Behavioral Development, 2(1), 1–21.
Erikson, E. H. (1950). Childhood and society. New York: WW Norton & Company.
Evans, G. W., & Kim, P. (2007). Childhood poverty and health cumulative risk exposure and stress dysregulation. Psychological Science, 18(11), 953–957.
Feagin, J., & Bennefield, Z. (2014). Systemic racism and US health care. Social Science and Medicine, 103, 7–14.
Feldman, P. J., Dunkel-Schetter, C., Sandman, C. A., & Wadhwa, P. D. (2000). Maternal social support predicts birth weight and fetal growth in human pregnancy. Psychosomatic Medicine, 62(5), 715–725.
Flier, J. S., Underhill, L. H., & McEwen, B. S. (1998). Protective and damaging effects of stress mediators. New England Journal of Medicine, 338(3), 171–179.
Flinn, M. V., & England, B. G. (1997). Social economics of childhood glucocorticoid stress response and health. American Journal of Physical Anthropology, 102(1), 33–53.
Gavin, A. R., Hill, K. G., Hawkins, J. D., & Maas, C. (2011). The role of maternal early-life and later-life risk factors on offspring low birth weight: Findings from a three-generational study. Journal of Adolescent Health, 49(2), 166–171.
Geronimus, A. (1992). The weathering hypothesis and the health of African-American women and infants: evidence and speculations. Ethnicity and Disease, 2(3), 207.
Geronimus, A. T. (1996). Black/white differences in the relationship of maternal age to birthweight: A population-based test of the weathering hypothesis. Social Science and Medicine, 42(4), 589–597.
Glass, T. A., & McAtee, M. J. (2006). Behavioral science at the crossroads in public health: extending horizons, envisioning the future. Social Science and Medicine, 62(7), 1650–1671.
Grady, S. C. (2006). Racial disparities in low birthweight and the contribution of residential segregation: A multilevel analysis. Social Science and Medicine, 63(12), 3013–3029.
Gunnar, M., & Quevedo, K. (2007). The neurobiology of stress and development. Annual Review of Psychology, 58, 145–173.
Hagan, J., MacMillan, R., & Wheaton, B. (1996). New kid in town: Social capital and the life course effects of family migration on children. American Sociological Review, 368–385.
Halfon, N., & Hochstein, M. (2002). Life course health development: an integrated framework for developing health, policy, and research. Milbank Quarterly, 80(3), 433–479.
Hamilton, B. E., Martin, J. A., Osterman, M., Curtin, S., & Matthews, T. (2015). Births: Final data for 2014. National Vital Statistics Reports, 64(12), 1–64.
Harris, K. M., Halpern, C. T., Hussey, J., Whitsel, E. A., Killeya-Jones, L., Tabor, J., et al. (2013). Social, behavioral, and genetic linkages from adolescence into adulthood. American Journal of Public Health, 103(Suppl 1), S25–S32.
Hartley, D. (2004). Rural health disparities, population health, and rural culture. American Journal of Public Health, 94(10), 1675–1678.
Hartup, W. W. (1989). Social relationships and their developmental significance. American Psychologist, 44(2), 120.
Harville, E. W., Boynton-Jarrett, R., Power, C., & Hypponen, E. (2010). Childhood hardship, maternal smoking, and birth outcomes: A prospective cohort study. Archives of Pediatrics and Adolescent Medicine, 164(6), 533.
Harville, E. W., Madkour, A. S., & Xie, Y. (2012). Predictors of birth weight and gestational age among adolescents. American Journal of Epidemiology, 176(suppl 7), S150–S163.
Haussmann, M. F., & Heidinger, B. J. (2015). Telomere dynamics may link stress exposure and ageing across generations. Biology Letters, 11(11), 20150396.
Hertzman, C. (2006). The biological embedding of early experience and its effects on health in adulthood. Annals of the New York Academy of Sciences, 896(1), 85–95.
Hertzman, C., & Boyce, T. (2010). How experience gets under the skin to create gradients in developmental health. Annual Review of Public Health, 31, 329–347.
Hertzman, C., & Power, C. (2006). A life course approach to health and human development. In J. Heymann, C. Hertzman, M. L. Barer, & R. G. Evans (Eds.), Healthier societies: From analysis to action (pp. 83–106). New York: Oxford University Press.
Hobel, C. J., Dunkel-Schetter, C., Roesch, S. C., Castro, L. C., & Arora, C. P. (1999). Maternal plasma corticotropin-releasing hormone associated with stress at 20 weeks’ gestation in pregnancies ending in preterm delivery. American Journal of Obstetrics and Gynecology, 180(1), S257–S263.
Hogue, C. J., Hoffman, S., & Hatch, M. C. (2001). Stress and preterm delivery: A conceptual framework. Paediatric and Perinatal Epidemiology, 15(s2), 30–40.
Hollingshaus, M. S., Coon, H., Crowell, S. E., Gray, D. D., Hanson, H. A., Pimentel, R., et al. (2016). Differential vulnerability to early-life parental death: The moderating effects of family suicide history on risks for major depression and substance abuse in later life. Biodemography and Social Biology, 62(1), 105–125.
Holt-Lunstad, J., Smith, T. B., & Layton, J. B. (2010). Social relationships and mortality risk: A meta-analytic review. PLoS Medicine, 7(7), e1000316.
Holtz, B., Smock, A., & Reyes-Gastelum, D. (2015). Connected motherhood: Social support for moms and moms-to-be on Facebook. Telemedicine and e-Health, 21(5), 415–421.
Holzman, C., Eyster, J., Tiedje, L. B., Roman, L. A., Seagull, E., & Rahbar, M. H. (2006). A life course perspective on depressive symptoms in mid-pregnancy. Maternal and Child Health Journal, 10(2), 127–138.
Hostinar, C. E., & Gunnar, M. R. (2013). The developmental effects of early life stress an overview of current theoretical frameworks. Current Directions in Psychological Science, 22(5), 400–406.
Hrdy, S. B. (2009). Allomothers across species, across cultures, and through time. Substitute Parents, 3.
Kane, J. B. (2015). An integrative model of inter- and intragenerational preconception processes influencing birthweight in the United States. Journal of Health and Social Behavior, 56(2), 246–261.
Kane, J. B. (2016). Marriage advantages in perinatal health: Evidence of marriage selection or marriage protection? Journal of Marriage and Family, 78(1), 212–229.
Kane, J. B., Miles, G., Yourkavitch, J., & King, K. (2016). The role of neighborhoods in perinatal health outcomes and maternal health behaviors: Going beyond disadvantage, Incorporating Affluence. Miami, FL: Society for Paediatric and Perinatal Epidemiology.
Kawachi, I., & Berkman, L. F. (2003). Neighborhoods and health. New York: Oxford University Press.
Kelly, R., Holzman, C., Senagore, P., Wang, J., Tian, Y., Rahbar, M., et al. (2009). Placental vascular pathology findings and pathways to preterm delivery. American Journal of Epidemiology, 170(2), 148–158.
Khashan, A., McNamee, R., Abel, K., Mortensen, P. B., Kenny, L., Pedersen, M. G., et al. (2009). Rates of preterm birth following antenatal maternal exposure to severe life events: A population-based cohort study. Human Reproduction, 24(2), 429–437.
Kimbro, R. T. (2008). Together forever? Romantic relationship characteristics and prenatal health behaviors. Journal of Marriage and Family, 70(3), 745–757.
Knab, J. T., & McLanahan, S. (2006). Measuring cohabitation: Does how, when, and who you ask matter. In S. L. Hofferth & L. M. Casper (Eds.), Handbook of measurement issues in family research (pp. 19–33). Mahwah, New Jersey: Lawrence Erlbaum Associates Inc.
Kramer, M. S., Goulet, L., Lydon, J., Séguin, L., McNamara, H., Dassa, C., et al. (2001). Socio-economic disparities in preterm birth: causal pathways and mechanisms. Paediatric and Perinatal Epidemiology, 15(s2), 104–123.
Kramer, M. R., & Hogue, C. R. (2009a). What causes racial disparities in very preterm birth? A biosocial perspective. Epidemiologic Reviews, 31(1), 84–98.
Kramer, M. R., & Hogue, C. R. (2009b). What causes racial disparities in very preterm birth? A biosocial perspective. Epidemiologic Reviews, 31, 84–98.
Kramer, M. S., Lydon, J., Goulet, L., Kahn, S., Dahhou, M., Platt, R. W., et al. (2013). Maternal stress/distress, hormonal pathways and spontaneous preterm birth. Paediatric and Perinatal Epidemiology, 27(3), 237–246.
Kramer, M. S., Lydon, J., Séguin, L., Goulet, L., Kahn, S. R., McNamara, H., et al. (2009). Stress pathways to spontaneous preterm birth: the role of stressors, psychological distress, and stress hormones. American Journal of Epidemiology, 169(11), 1319–1326.
Krieger, N. (2005a). Embodiment: A conceptual glossary for epidemiology. Journal of Epidemiology and Community Health, 59(5), 350–355.
Krieger, N. (2005b). Embodying inequality: Epidemiologic perspectives. Amityville, NY: Baywood Publishing Company Inc.
Kristenson, M., Eriksen, H. R., Sluiter, J. K., Starke, D., & Ursin, H. (2004). Psychobiological mechanisms of socioeconomic differences in health. Social Science and Medicine, 58(8), 1511–1522.
Kuh, D., Ben-Shlomo, Y., Lynch, J., Hallqvist, J., & Power, C. (2003). Life course epidemiology. Journal of Epidemiology and Community Health, 57(10), 778.
Kuh, D., & Shlomo, Y. B. (2004). A life course approach to chronic diseases epidemiology. USA: Oxford University Press.
Lacey, R. E., Kumari, M., & Bartley, M. (2014). Social isolation in childhood and adult inflammation: Evidence from the National Child Development Study. Psychoneuroendocrinology, 50, 85–94.
Landale, N. S., & Oropesa, R. (2001). Father involvement in the lives of mainland Puerto Rican children: Contributions of nonresident, cohabiting and married fathers. Social Forces, 79(3), 945–968.
Lhila, A., & Long, S. (2012). What is driving the black–white difference in low birthweight in the US? Health Economics, 21(3), 301–315.
Lien, D. S., & Evans, W. N. (2005). Estimating the impact of large cigarette tax hikes. Journal of Human Resources, 40(2), 373–392.
Link, B. G., & Phelan, J. (1995). Social conditions as fundamental causes of disease. Journal of Health and Social Behavior, 80–94.
Love, C., David, R. J., Rankin, K. M., & Collins, J. W., Jr. (2010). Exploring weathering: effects of lifelong economic environment and maternal age on low birth weight, small for gestational age, and preterm birth in African-American and white women. American Journal of Epidemiology, 172(2), 127–134.
Lu, M. C., & Halfon, N. (2003). Racial and ethnic disparities in birth outcomes: A life-course perspective. Maternal and Child Health Journal, 7(1), 13–30.
Lu, M. C., Tache, V., Alexander, G. R., Kotelchuck, M., & Halfon, N. (2003). Preventing low birth weight: Is prenatal care the answer? Journal of Maternal-Fetal and Neonatal Medicine, 13(6), 362–380.
Madkour, A. S., Xie, Y., & Harville, E. W. (2014). Pre-pregnancy dating violence and birth outcomes among adolescent mothers in a national sample. Journal of Interpersonal Violence, 29(10), 1894–1913.
Manning, W. D., & Smock, P. J. (2005). Measuring and modeling cohabitation: New perspectives from qualitative data. Journal of Marriage and Family, 67(4), 989–1002.
Margerison-Zilko, C. (2014). The contribution of maternal birth cohort to term small for gestational age in the united states 1989–2010: An age, period, and cohort analysis. Paediatric and Perinatal Epidemiology, 28(4), 312–321.
Margerison-Zilko, C., Cubbin, C., Jun, J., Marchi, K., Fingar, K., & Braveman, P. (2015). Beyond the cross-sectional: Neighborhood poverty histories and preterm birth. American Journal of Public Health, 105(6), 1174–1180.
Margerison-Zilko, C., Strutz, K. L., Li, Y., & Holzman, C. (2016). Stressors across the life-course and preterm delivery: Evidence from a pregnancy cohort. Maternal and Child Health Journal, 1–11.
Marmot, M. (2005). Social determinants of health inequalities. The Lancet, 365(9464), 1099–1104.
McDade, T. W. (2012). Early environments and the ecology of inflammation. Proceedings of the National Academy of Sciences, 109(Supplement 2), 17281–17288.
McEwen, B. S. (2008). Central effects of stress hormones in health and disease: Understanding the protective and damaging effects of stress and stress mediators. European Journal of Pharmacology, 583(2), 174–185.
McFarland, M. J., McLanahan, S. S., Goosby, B. J., & Reichman, N. E. (2016). Grandparents’ education and infant health: Pathways across generations. Journal of Marriage and Family. doi:10.1111/jomf.12383.
McLeod, J. D., & Almazan, E. P. (2003). Connections between childhood and adulthood. In J. T. Mortimer & M. J. Shanahan (Eds.), Handbook of the life course (pp. 391–411). New York: Springer.
Messer, L. C., Kaufman, J. S., Dole, N., Savitz, D. A., & Laraia, B. A. (2006a). Neighborhood crime, deprivation, and preterm birth. Annals of Epidemiology, 16(6), 455–462.
Messer, L. C., Laraia, B. A., Kaufman, J. S., Eyster, J., Holzman, C., Culhane, J., et al. (2006b). The development of a standardized neighborhood deprivation index. Journal of Urban Health, 83(6), 1041–1062.
Miller, G. E., & Chen, E. (2010). Harsh family climate in early life presages the emergence of a proinflammatory phenotype in adolescence. Psychological Science, 21(6), 848–856.
Miltenburg, E. M., & van der Meer, T. W. (2016). Lingering neighbourhood effects: A framework to account for residential histories and temporal dynamics. Urban Studies, 0042098016639012.
Misra, D. P., Guyer, B., & Allston, A. (2003). Integrated perinatal health framework: A multiple determinants model with a life span approach. American Journal of Preventive Medicine, 25(1), 65–75.
Morello-Frosch, R., & Shenassa, E. D. (2006). The environmental” riskscape” and social inequality: Implications for explaining maternal and child health disparities. Environmental Health Perspectives, 1150–1153.
Morenoff, J. D. (2003). Neighborhood mechanisms and the spatial dynamics of birth weight. American Journal of Sociology, 108(5), 976–1017.
Moss, J. L., & Harris, K. M. (2015). Impact of maternal and paternal preconception health on birth outcomes using prospective couples’ data in add health. Archives of Gynecology and Obstetrics, 291(2), 287–298.
Nerum, H., Halvorsen, L., Straume, B., Sørlie, T., & Øian, P. (2013). Different labour outcomes in primiparous women that have been subjected to childhood sexual abuse or rape in adulthood: A case–control study in a clinical cohort. BJOG, 120(4), 487–495.
Noll, J. G., Schulkin, J., Trickett, P. K., Susman, E. J., Breech, L., & Putnam, F. W. (2007). Differential pathways to preterm delivery for sexually abused and comparison women. Journal of Pediatric Psychology, 32(10), 1238–1248.
Oakes, J. M. (2004). The (mis) estimation of neighborhood effects: Causal inference for a practicable social epidemiology. Social Science and Medicine, 58(10), 1929–1952.
Orr, S. T., James, S. A., & Prince, C. B. (2002). Maternal prenatal depressive symptoms and spontaneous preterm births among African-American women in Baltimore, Maryland. American Journal of Epidemiology, 156(9), 797–802.
Padilla, Y. C., & Reichman, N. E. (2001). Low birthweight: Do unwed fathers help? Children and Youth Services Review, 23(4), 427–452.
Pallotto, E. K., & Kilbride, H. W. (2006). Perinatal outcome and later implications of intrauterine growth restriction. Clinical Obstetrics and Gynecology, 49(2), 257–269.
Pearlin, L. I. (1989). The sociological study of stress. Journal of Health and Social Behavior, 241–256.
Pearlin, L. I. (1999). The stress process revisited. Handbook of the sociology of mental health (pp. 395–415). New York: Springer.
Pearlin, L. I., Menaghan, E. G., Lieberman, M. A., & Mullan, J. T. (1981). The stress process. Journal of Health and Social Behavior, 337–356.
Phelan, J. C., & Link, B. G. (2015). Is racism a fundamental cause of inequalities in health? Annual Review of Sociology, 41, 311–330.
Pickett, K. E., Ahern, J. E., Selvin, S., & Abrams, B. (2002). Neighborhood socioeconomic status, maternal race and preterm delivery: A case-control study. Annals of Epidemiology, 12(6), 410–418.
Plotnick, R. D., & Hoffman, S. D. (1999). The effect of neighborhood characteristics on young adult outcomes: Alternative estimates. Social Science Quarterly, 1–18.
Rackin, H., & Gibson-Davis, C. M. (2012). The role of pre-and postconception relationships for first-time parents. Journal of Marriage and Family, 74(3), 526–539.
Ramey, S. L., Schafer, P., DeClerque, J. L., Lanzi, R. G., Hobel, C., Shalowitz, M., et al. (2015). The preconception stress and resiliency pathways model: A multi-level framework on maternal, paternal, and child health disparities derived by community-based participatory research. Maternal and Child Health Journal, 19(4), 707–719.
Reichman, N. E., & Teitler, J. O. (2005). Timing of enhanced prenatal care and birth outcomes in New Jersey’s HealthStart program. Maternal and Child Health Journal, 9(2), 151–158.
Repetti, R. L., Taylor, S. E., & Seeman, T. E. (2002). Risky families: Family social environments and the mental and physical health of offspring. Psychological Bulletin, 128(2), 330.
Richardson, L. J., Hussey, J. M., & Strutz, K. L. (2012). A life course perspective in maternal and child health. In J. B. Kotch (Ed.), Maternal and child health: Programs, problems, and policy (pp. 65–85). Gaithersburg, MD: Aspen Publishers Inc.
Rich-Edwards, J. W., & Grizzard, T. A. (2005). Psychosocial stress and neuroendocrine mechanisms in preterm delivery. American Journal of Obstetrics and Gynecology, 192(5), S30–S35.
Rosenzweig, M. R., & Schultz, T. P. (1983). Estimating a household production function: Heterogeneity, the demand for health inputs, and their effects on birth weight. The Journal of Political Economy, 91, 723–746.
Roux, A. V. D. (2004). Estimating neighborhood health effects: The challenges of causal inference in a complex world. Social Science and Medicine, 58(10), 1953–1960.
Russ, S. A., Larson, K., Tullis, E., & Halfon, N. (2014). A lifecourse approach to health development: Implications for the maternal and child health research agenda. Maternal and Child Health Journal, 18(2), 497–510.
Sampson, R. J. (2003). Neighborhood-level context and health: Lessons from sociology. In I. Kawachi & L. F. Berkman (Eds.), Neighborhoods and health (pp. 132–146). New York: Oxford University Press.
Sampson, R. J., Morenoff, J. D., & Gannon-Rowley, T. (2002). Assessing” neighborhood effects”: Social processes and new directions in research. Annual Review of Sociology, 28, 443–478.
Sassler, S. (2004). The process of entering into cohabiting unions. Journal of Marriage and Family, 66(2), 491–505.
Saxton, K. B., John-Henderson, N., Reid, M. W., & Francis, D. D. (2011). The social environment and IL-6 in rats and humans. Brain, Behavior, and Immunity, 25(8), 1617–1625.
Schaaf, J. M., Liem, S. M., Mol, B. W. J., Abu-Hanna, A., & Ravelli, A. C. (2013). Ethnic and racial disparities in the risk of preterm birth: a systematic review and meta-analysis. American Journal of Perinatology, 30(06), 433–450.
Schei, B., Lukasse, M., Ryding, E. L., Campbell, J., Karro, H., Kristjansdottir, H., et al. (2014). A history of abuse and operative delivery–results from a European multi-country cohort study. PLoS ONE, 9(1), e87579.
Schempf, A., Strobino, D., & O’Campo, P. (2009). Neighborhood effects on birthweight: an exploration of psychosocial and behavioral pathways in Baltimore, 1995–1996. Social Science and Medicine, 68(1), 100–110.
Seckl, J. R., & Meaney, M. J. (2004). Glucocorticoid programming. Annals of the New York Academy of Sciences, 1032(1), 63–84.
Seeman, T., Epel, E., Gruenewald, T., Karlamangla, A., & McEwen, B. S. (2010). Socio-economic differentials in peripheral biology: Cumulative allostatic load. Annals of the New York Academy of Sciences, 1186(1), 223–239.
Shonkoff, J. P., Garner, A. S., Siegel, B. S., Dobbins, M. I., Earls, M. F., McGuinn, L., et al. (2012). The lifelong effects of early childhood adversity and toxic stress. Pediatrics, 129(1), e232–e246.
Shonkoff, J. P., & Phillips, D. (2000). From neurons to neighborhoods: The science of early childhood development. Washington (DC): National Academies Press.
Singh-Manoux, A., & Marmot, M. (2005). Role of socialization in explaining social inequalities in health. Social Science and Medicine, 60(9), 2129–2133.
Strutz, K. L., Hogan, V. K., Siega-Riz, A. M., Suchindran, C. M., Halpern, C. T., & Hussey, J. M. (2014). Preconception stress, birth weight, and birth weight disparities among US women. American Journal of Public Health, 104(8), e125–e132.
Subramanian, S. (2004). The relevance of multilevel statistical methods for identifying causal neighborhood effects. Social Science and Medicine, 58(10), 1961–1967.
Syme, S. L., & Berkman, L. F. (1986). Social class, susceptibility, and sickness. In P. Conrad (Ed.), The sociology of health and illness: Critical perspectives (pp. 24–29). New York, NY: Worth Publishers.
Teitler, J. O., & Weiss, C. C. (2000). Effects of neighborhood and school environments on transitions to first sexual intercourse. Sociology of Education, 112–132.
Thayer, Z. M., & Kuzawa, C. W. (2011). Biological memories of past environments: Epigenetic pathways to health disparities. Epigenetics, 6(7), 798–803.
Thoits, P. A. (1982). Conceptual, methodological, and theoretical problems in studying social support as a buffer against life stress. Journal of Health and Social Behavior, 145–159.
Thoits, P. A. (1983). Multiple identities and psychological well-being: A reformulation and test of the social isolation hypothesis. American Sociological Review, 174–187.
Thoits, P. A. (2010). Stress and health major findings and policy implications. Journal of Health and Social Behavior, 51(1 suppl), S41–S53.
Wallace, M. E., Mendola, P., Liu, D., & Grantz, K. L. (2015). Joint effects of structural racism and income inequality on small-for-gestational-age birth. American Journal of Public Health, 105(8), 1681–1688.
Walton, E. (2009). Residential segregation and birth weight among racial and ethnic minorities in the United States. Journal of Health and Social Behavior, 50(4), 427–442.
Warnecke, R. B., Oh, A., Breen, N., Gehlert, S., Paskett, E., Tucker, K. L., et al. (2008). Approaching health disparities from a population perspective: The National Institutes of Health Centers for Population Health and Health Disparities. American Journal of Public Health, 98(9), 1608–1615.
Wehby, G. L., Fletcher, J. M., Lehrer, S. F., Moreno, L. M., Murray, J. C., Wilcox, A., et al. (2011). A genetic instrumental variables analysis of the effects of prenatal smoking on birth weight: Evidence from two samples. Biodemography and Social Biology, 57(1), 3–32.
Witt, W. P., Cheng, E. R., Wisk, L. E., Litzelman, K., Chatterjee, D., Mandell, K., et al. (2014a). Maternal stressful life events prior to conception and the impact on infant birth weight in the United States. American Journal of Public Health, 104(S1), S81–S89.
Witt, W. P., Cheng, E. R., Wisk, L. E., Litzelman, K., Chatterjee, D., Mandell, K., et al. (2014b). Preterm birth in the United States: The impact of stressful life events prior to conception and maternal age. American Journal of Public Health, 104(S1), S73–S80.
Yang, Y. C., Boen, C., Gerken, K., Li, T., Schorpp, K., & Harris, K. M. (2016). Social relationships and physiological determinants of longevity across the human life span. Proceedings of the National Academy of Sciences, 113(3), 578–583.
Zuckerman, B., Amaro, H., Bauchner, H., & Cabral, H. (1989). Depressive symptoms during pregnancy: Relationship to poor health behaviors. American Journal of Obstetrics and Gynecology, 160(5), 1107–1111.
Acknowledgements
The Funding was provided by Eunice Kennedy Shriver National Institute of Child Health and Human Development (Grant Nos. HD075860, HL128843).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Kane, J.B., Margerison-Zilko, C. Theoretical Insights into Preconception Social Conditions and Perinatal Health: The Role of Place and Social Relationships. Popul Res Policy Rev 36, 639–669 (2017). https://doi.org/10.1007/s11113-017-9430-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11113-017-9430-8