
Abstract
Objective To assess the impact of medication reconciliation interventions on medication error rates when elderly patients are discharged from hospital to community care or nursing homes.Setting Elderly patients (>65 years) living in nursing homes or in their own homes with care provided by the community nursing system. Method All medical records containing information on drug treatment were collected from hospital departments, the community care service and GPs. We then identified if there were any changes in the transfer of information i.e. if the drugs were not the same as before the transfer. Two different persons independently evaluated all information about the patients’ drugs to identify medication errors for three different time periods. During all three periods structured discharge information was used. In period 2, electronic medication lists were introduced and in period 3 we introduced specific routines and support by a clinical pharmacist to ensure prescription in the specific medication dispensing system (ApoDos). Asymptotic Linear by–Linear Association Test was used to compare number of medication errors in period 1, 2 and 3 respectively. Main outcome measure Number of medication errors per patient. Results A total of 123 patients were evaluated at discharge. For the 109 patients using the ApoDos system, there were significant differences in the number of medication errors between period 1 and 3 (P = 0.048), period 2 and 3 (P = 0.037 but not between period 1 and 2 (P = 0.41). The mean numbers of errors were 1.5, 1.1 and 0.5 for period 1, 2 and 3 respectively. The 14 patients not using the ApoDos system had on average 0.4 errors per patient. Among the 58 patients with medication errors, 34 were evaluated as having low clinical risk, 22 moderate, and 2 high clinical risk. Conclusion Medication errors are still common when elderly patients are transferred from hospital to community/primary care. The main risk factor seems to be the specific medication dispensing system (ApoDos) or rather the process on how to use it. When this system was supported by clinical pharmacists, the error rate dropped to the same level as for patients without ApoDos.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Impact of findings on practice
-
Medication reconciliation interventions with clinical pharmacists can reduce the number of medication errors when elderly patients are discharged from hospital.
-
Use of medication dispensing system (ApoDos) may increase the risk of medication errors when elderly patients are discharged from hospital, if the system is not accompanied by support from clinical pharmacists.
Introduction
Medication errors are common and may cause drug-related problems [1, 2]. Elderly patients are more susceptible to drug-related problems. A drug-related problem (DRP) is defined as “an event or circumstance that actually or potentially interferes with desired health outcomes” [3]. DRPs may lead to hospitalisation [4, 5] and increase the length of stay at the hospital [6–8]. Many of these drug-related problems are preventable [9, 10].
Medication errors can be of various types [11, 12] and when medication errors are reduced this may lead to reduction in drug-related problems and health care consumption [13].
There are experiences from hundreds of organisations showing that bad communication in medical care interfaces causes up to 50% of all medication errors in hospitals and up to 20% of adverse drug events [14]. Problems also arise outside of hospital as a result of poor communication within medical care interfaces; we have shown that mistakes in the medication reconciliation process at discharge from hospital can cause errors, risk of negative clinical consequences and also actual health care contacts due to the errors [13, 15]. Several national and international organisations state that errors in the medication reconciliation process is one of the major problems relating to patient safety and have suggestions for improvement [16]. In 2000–2001 we performed a study at the Department of Internal Medicine at Landskrona Hospital, to investigate errors in the medication lists when a patient is transferred between community care and hospital care [17]. We found several problems and have during the last couple of years used this setting, as well as departments at Lund University Hospital, to identify more problems. We have also developed tools to resolve problems such as medication errors and drug-related problems [13, 15, 18–21]. Since the previous study, a clinical pharmacy service including medication reconciliation and medication review in the Landskrona Integrated Medicines Management (LIMM) programme has been running [19, 20]. In this programme, started in 2005, the pharmacists assist the responsible physicians in preparing a correct medication list upon admission. This approach is based on evidence and recommendations indicating that the pharmacist is the most suitable professional to produce a correct medication list [16]. In our setting, the pharmacist normally performs the reconciliation within 24 h of a patient being admitted to hospital on normal office days.
We have shown that our developed medication report reduces not only error rate and the risk of negative clinical consequences, but also health care contacts due to medication errors when a patient is discharged from hospital [13, 15]. We have further developed the concept into a structured written summary of important aspects and changes in the patients’ drug therapy. The document, named “discharge information”, is written for the patient and contains:
-
General information (responsible physician, reason for admission to hospital, planned follow-up)
-
Medication report (a section with information on medication changes that were made and the reasons for these changes)
-
Medication list (a list of current medications, dosage and indication for each medication)
At discharge, the document should be discussed with and given to the patient and, if applicable, sent to the community health care service and the patient’s general practitioner (GP) within the same day.
We have previously shown that use of a specific medication dispensing system (ApoDos) increased the risk of medication errors in the transition of information [15, 17]. At discharge changes in the patients’ medication must be communicated to the regional ApoDos dispensing unit. The awareness and priority of this is low among many hospital physicians; we therefore focused on this issue.
Aim of the study
The aim was to study medication errors, in the patient medication lists upon discharge from hospital care after introduction of medication reconciliation interventions, and to evaluate the clinical risks of these errors.
Methods
In this study we were mainly interested in identifying and comparing errors in the discharge Medication Reconciliation process (identifying the most accurate list of a patient’s current medicines) after interventions during hospital care, as well as comparing the results with our previous study [17]. These interventions are described in Table 1. Since the paper-based medication lists in the hospital medical records were changed to electronic lists during the study period we decided to describe these periods separately, as this change could have major effects on the results of the study. Thus, we had three separate study periods.
Subjects, settings, data assessment, and definitions
Subjects, settings, and definitions
Elderly patients (>65 years) living in nursing homes or in their own homes with care provided by the community nursing system in the town of Landskrona were invited to participate if they had also been treated at one of the three departments of internal medicine at Landskrona hospital during the study periods. The patients were discharged to either community care or nursing homes.
The clinical pharmacists identified the patients. One of the authors (LB) gave patients or their relatives written and verbal information. Written consent was collected from all participants.
Study periods and interventions
The three study periods were August 18–October 29, 2008 (period 1), October 30, 2008–March 31, 2009 (period 2, medication list in the electronic patient medical records and quality control of discharge information), and April 1–June 30, 2009 (period 3 + focus on the Specific medication dispensing, ApoDos). The interventions are described in detail in Table 1. The interventions are mainly based on the LIMM-model, which is a systematic approach to individualise and optimise the drug treatment in elderly in-patients. Clinical pharmacists conduct the medication reconciliation upon admission of the patient to the ward and review and monitor medication during hospital stay according to the LIMM-model [21].
Specific medication dispensing system (ApoDos)
This is a complete list of all medications used by the patient. It is not a compulsory system. This system is however very common in Sweden and is used outside hospitals and particularly for elderly patients, with many medications, living in nursing homes or in their own homes. One reason for the use of this medication dispensing system is a supposed reduction in the risk of mistakes in medication handling. In brief, the medication dispensing system is a multi-dose system and, if possible, all medications that the patient should take at one time are machine-packed together in small, fully labelled plastic bags at a regional pharmacy-dispensing centre. For our setting, this means that the pharmacy instead of the nurse prepares the dosages. For ApoDos patients to receive correct medication (after discharge), changes must be made in a national electronic ApoDos database by the physicians using their individual access code. The ApoDos system and the electronic medical records are two different systems. Data cannot be transferred between the electronic ApoDos system and the medication list in the electronic patient medical records; the responsible physician must document changes in both systems. There is thus a risk of transcribing errors. Sometimes hospital physicians do not prescribe medications within the Medication Dispensing System, in that case, the prescriptions are not transferred.
Assessment of errors and risk
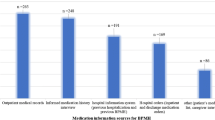
The pharmacists worked at the hospital and collected all medical records containing information on drug treatment from hospital departments and the general practitioners (GPs). Data from nursing homes and community nursing system were asked for and sent to the research group. We collected lists prior to and during hospital stay, as well as after discharge from hospital. All medication notes used for the transfer of information were collected.
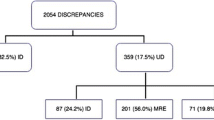
We then identified if there were any discrepancies between medication lists i.e. if the drugs were not the same as before the transfer [17]. If there was any indication that change of medication was intentional, it was not regarded as an error. Comments or notes in any record or written documentation, e.g., indicated an intentional change. Incorrect dosage interval was not an error if the total dose/24 h had not been changed. Change of generic medications or withdrawal of drugs with long dosage intervals, e.g., once monthly, was not regarded as an error. If drugs were added, withdrawn, or the dosage had changed without any documentation in medical records or medication lists, it was considered an error. At discharge, the in-hospital medication lists on the day of discharge were considered correct if no other information was documented as described in Fig. 1. This list was compared to the community care dispensing list when the first dose had been given. For ApoDos-patients, the ApoDos-list when first packages were delivered after 2–14 days was checked. The hospital should provide medications for the time until the first ApoDos packages are delivered.

Medication lists used to study the discharge process from hospital to community care. The lists used for assessment of errors are marked in grey. The local dispensing list should normally be the medication list in the Discharge Information. The new ApoDos medication list and multi dose medications are delivered between days 2–14
Any unintentional errors in the transfer of information were identified and the clinical risks, as a theoretical consequence of the errors, were evaluated for each patient and classified into one of three groups, (1) without clinical risk, (2) with moderate clinical risk (3) and with high clinical risk, using the same process as previously described [15]. All evaluations of errors and risks were performed by two persons (LB and MS) independently, after briefing concerning the method and discussions based on cases and instructions. Their evaluations were compared and agreed on. In case of disagreement, a third person (PM) was consulted. For each patient with an error, the evaluation was double-checked following the completion of the study.
Prior to the evaluation of risks, instructions to be used in the study were agreed upon by the entire research group. Errors were classified into three categories; 1 high clinical risk, 2 moderate clinical risk and 3 no clinical risk. The research group had a list of examples and agreed on the categories. Examples were; the erroneous addition of warfarin which was evaluated as a high clinical risk; the erroneous addition of enalapril after discharge from hospital which was evaluated as a moderate clinical risk; the prescription of zopiclone 5 mg instead of zopiclone 7.5 mg which was evaluated, and found to pose no clinical risk.
Statistics and data analysis
Computer software R version 2.5.1 was used for all statistical analyses (R Foundation for Statistical Computing, Vienna, Austria). The R COIN procedure (Asymptotic Linear by-Linear Association Test) was used to compare the number of medication errors between period 1, 2 and 3 respectively, for patients using ApoDos.
Ethics
The ethical committee at Lund University approved the study no. 282/2008.
Results
Evaluation of errors
The two persons evaluating errors and risks agreed in all but seven cases. For these seven cases a third person (PM), was consulted and disagreements were solved through discussions.
At admission
Patients had 12 drugs on average. The rate of medication errors at admission to hospital was similar in the three periods, with the mean number of errors per patient being 0.92, 1.0 and 0.95 in period 1, 2 and 3 respectively. These errors occur prior to any intervention. The most common medication error at admission to hospital care was that medications were erroneously omitted.
At discharge
Characteristics of included patients at discharge from hospital are described in Table 2.
Errors at discharge
In period 3, no patients with the specific medication dispensing system had more than two medication errors whereas in period 1, three out of 16 patients and in period 2, six out of 27 patients had three or more medication errors (Table 3). There were significant differences between period 1 and 3 (P = 0.048), period 2 and 3 (P = 0.037) but not between period 1 and 2 (P = 0.41).
The mean number of medication errors was lower in period 3 for ApoDos-patients (Table 4). There were few patients in all periods not using ApoDos, and therefore there are no comparisons between the periods regarding these patients, hence data for patients not using ApoDos is not presented in Table 4. In total there were 14 patients not using the ApoDos system and for these patients, the total number of errors was six, with a mean of 0.4 errors per patient.
The most common medication error in period 1, 2 and 3 was that medications were erroneously added.
All documents regarding medications at discharge were found by the pharmacists to contain errors, i.e. the medication report, the discharge medication list, and the ApoDos medication list. In period 3, the pharmacist identified discrepancies and suggested changes in 26 cases; the physicians accepted and corrected 14 of these discrepancies.
Clinical risks
A total of 58 patients had medication errors and for these, the clinical risks were evaluated.
Most errors were evaluated as having low clinical risk (34 out of 58 patients with medication errors), and only for two patients the errors were evaluated as having high clinical risk (Table 5).
Discussion
The elderly patients in this study used on average 12 drugs per patient. Even after our medication reconciliation interventions, medication errors were quite common when elderly patients were discharged from hospital care. The main risk factor seems to be the specific medication dispensing system (ApoDos). With this system there is slightly more than one error per patient. This is a small improvement compared to our previous study in the same setting [17]. In that study we also showed that patients without ApoDos had lower medication error rate than patients with ApoDos, thus there was a need for interventions to reduce the risks for patients with ApoDos.
When this system and the transfer process were supported by clinical pharmacists, the medication error rate dropped to the same level as for patients without the medication dispensing system. The error rate dropped to 0.46 medication errors per patient, which is at the same level as for patients without ApoDos, 0.43 medication errors per patient. One reason for the increased risk of error might be that ApoDos means an additional step in the prescribing process and all additional steps may increase the risk of errors.
The pharmacists presented the identified errors to the physicians orally. The reasons for not correcting these medication errors are not known.
There are different explanations to the medication errors. Errors at discharge can be due to errors at admission not being corrected properly, but also because of therapy changes not being documented and communicated correctly to involved units. In southern Sweden there is not a common electronic patient medical record and all medication lists must be sent between different levels of care and manually entered into different electronic medical records, hence errors in transcription can occur in all steps. In our setting clinical pharmacists’ perform medication reconciliation at admission. In this study, this activity is not included in the presentation of errors at admission. The reason for this is that, not only did we not focus on admission, but also, the clinical pharmacist activity occurs after the initial evaluation of medication errors.
Other studies have also shown that clinical pharmacy services may reduce the number of medication errors. In one such study, medication errors were reduced by 51% when a pharmacist participated in daily medical rounds [22]. In another study the authors showed that medicine reconciliation by a pharmacist within an emergency department reduced the medication error rate [23].
Our study has some limitations. We have only included elderly patients living in nursing homes or in their own homes with care provided by the community nursing system. We do not know if our results are generalizable to all elderly patients. There are two reasons for our choice of patients. First, these patients are frailer and thus susceptible to adverse drug events. Second, all patients received their medications from staff at nursing homes, in their own home or at hospital, i.e. we knew exactly what medicines they used before, during and after hospital care. We have evaluated errors and also clinical risks, as a theoretical consequence of the errors, but we have not evaluated any actual clinical outcomes due to medication errors.
Conclusion
Medication errors are still common when elderly patients are transferred from hospital to community/primary care. The main risk factor seems to be the specific medication dispensing system (ApoDos) or rather the process on how to use it. When this system and the transfer process were supported by clinical pharmacists, the medication error rate dropped to the same level as for patients without this system. There is need for more research with comparisons between different types of interventions, as well as the evaluation of the effects of interventions on clinical outcomes for these patients.
References
Lisby M, Nielsen LP, Mainz J. Errors in the medication process: frequency, type, and potential clinical consequences. Int J Qual Health Care. 2005;17(1):15–22.
Tam VC, Knowles SR, Cornish PL, Fine N, Marchesano R, Etchells EE. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. CMAJ. 2005;173(5):510–5.
Strand LM, Morley PC, Cipolle RJ, Ramsey R, Lamsam GD. Drug-related problems: their structure and function. Dicp. 1990;24(11):1093–7.
Beijer HJ, de Blaey CJ. Hospitalisations caused by adverse drug reactions (ADR): a meta-analysis of observational studies. Pharm World Sci. 2002;24(2):46–54.
Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998;279(15):1200–5.
Azaz-Livshits T, Levy M, Sadan B, Shalit M, Geisslinger G, Brune K. Computerized survelliance of adverse drug reactions in hospital: pilot study. Br J Clin Pharmacol. 1998;45(3):309–14.
Bates DW, Spell N, Cullen DJ, Burdick E, Laird N, Petersen LA, et al. The costs of adverse drug events in hospitalized patients. Adverse drug events prevention study group. JAMA. 1997;277(4):307–11.
Classen DC, Pestotnik SL, Evans RS, Lloyd JF, Burke JP. Adverse drug events in hospitalized patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1997;277(4):301–6.
Winterstein AG, Sauer BC, Hepler CD, Poole C. Preventable drug-related hospital admissions. Ann Pharmacother. 2002;36(7–8):1238–48.
Mjörndal T, Boman MD, Hägg S, Bäckström M, Wiholm BE, Wahlin A, et al. Adverse drug reactions as a cause for admissions to a department of internal medicine. Pharmacoepidemiol Drug Saf. 2002;11(1):65–72.
Dean B, Schachter M, Vincent C, Barber N. Prescribing errors in hospital inpatients: their incidence and clinical significance. Qual Saf Health Care. 2002;11(4):340–4.
Runciman WB, Roughead EE, Semple SJ, Adams RJ. Adverse drug events and medication errors in Australia. Int J Qual Health Care. 2003;15(1):i49–59.
Midlöv P, Deierborg E, Holmdahl L, Höglund P, Eriksson T. Clinical outcomes from the use of medication report when elderly patients are discharged from hospital. Pharm World Sci. 2008;30(6):840–5.
IHI MedReconcilliation. Prevent adverse drug events. Cited 16 Dec 2011. Available from: http://www.ihi.org/IHI/Programs/Campaign/ADEsMedReconciliation.htm.
Midlöv P, Holmdahl L, Eriksson T, Bergkvist A, Ljungberg B, Widner H, et al. Medication report reduces number of medication errors when elderly patients are discharged from hospital. Pharm World Sci. 2008;30(1):92–8.
National Institute for Health and Clinical Excellence. Technical patient safety solutions for medicines reconciliation on admission of adults to hospital. 2007 Cited 16 Dec 2011; Available from: http://www.nice.org.uk/guidance/index.jsp?action=byID&o=11897.
Midlöv P, Bergkvist A, Bondesson A, Eriksson T, Höglund P. Medication errors when transferring elderly patients between primary health care and hospital care. Pharm World Sci. 2005;27(2):116–20.
Bondesson A, Hellström L, Eriksson T, Höglund P. A structured questionnaire to assess patient compliance and beliefs about medicines taking into account the ordered categorical structure of data. J Eval Clin Pract. 2009;15(4):713–23.
Bergkvist A, Midlöv P, Höglund P, Larsson L, Bondesson A, Eriksson T. Improved quality in the hospital discharge summary reduces medication errors–LIMM: landskrona integrated medicines management. Eur J Clin Pharmacol. 2009;65(10):1037–46.
Bergkvist A, Midlöv P, Höglund P, Larsson L, Eriksson T. A multi-intervention approach on drug therapy can lead to a more appropriate drug use in the elderly. LIMM-Landskrona integrated medicines management. J Eval Clin Pract. 2009;15(4):660–7.
Hellström LM, Bondesson A, Höglund P, Midlöv P, Holmdahl L, Rickhag E, et al. Impact of the Lund integrated medicines management (LIMM) model on medication appropriateness and drug-related hospital revisits. Eur J Clin Pharmacol. 2011;67(7):741–52.
Scarsi KK, Fotis MA, Noskin GA. Pharmacist participation in medical rounds reduces medication errors. Am J Health Syst Pharm. 2002;59(21):2089–92.
Mills PR, McGuffie AC. Formal medicine reconciliation within the emergency department reduces the medication error rates for emergency admissions. Emerg Med J. 2010;27(12):911–5.
Acknowledgments
We would like to thank the staff at the Department of Internal Medicine at Landskrona Hospital and the nurses in the community health care.
Funding
We are grateful to the Governmental Funding of Clinical Research within the NHS (ALF) and the National Board of Health and Welfare for funding the study.
Conflicts of interest
There are no conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Midlöv, P., Bahrani, L., Seyfali, M. et al. The effect of medication reconciliation in elderly patients at hospital discharge. Int J Clin Pharm 34, 113–119 (2012). https://doi.org/10.1007/s11096-011-9599-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11096-011-9599-6