
Abstract
The greatest risk factor for development of the deadly neurodegenerative disorder known as Alzheimer’s disease (AD) is advancing age. Currently unknown is what mediates the impact of advanced age on development of AD. Also unknown is what impact activity alterations in the entorhinal cortex (EC) has on the spread of AD pathology such as pathological tau through the brain as AD progresses. This review focuses on evidence in the literature that describes how one potential age-related change, that of glutamate-mediated increases in neuronal activity, may ultimately increase the risk of developing AD and promote the spread of tau pathology in AD-affected brains from the EC to later regions such as the hippocampus and prefrontal cortex. A better understanding of these detrimental alterations may allow for earlier detection of AD, offering a better prognosis for affected individuals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Alzheimer’s disease (AD) is the most common form of dementia, accounting for 60 to 80 percent of all dementia cases (Atri 2019). AD is characterized by three main biological hallmarks, extracellular beta-amyloid plaques, intracellular neurofibrillary tangles containing hyperphosphorylated tau protein, and neuronal death (Hyman et al. 2012). Though there are many risk factors for the development of AD, the greatest is advancing age (Lindsay et al. 2002). The connection between increasing age and AD is of interest because of the aging baby boomer population, which is expected to exacerbate the medical burden of age-related changes in cognition as well as age-related neurodegenerative disorders like AD (Rajan et al. 2021).
While AD ultimately proves fatal for affected individuals, of additional concern is the negative functional impact that the development of AD has on quality of life for these individuals and their caretakers (Isik et al. 2019). Over time, AD affects multiple brain regions as pathology spreads throughout the neocortex, entorhinal cortex, hippocampus, and prefrontal cortex (Braak and Braak 1991). Some of the functional changes that occur, such as deficits in spatial, working, or episodic memory, can be tied to network alterations in the entorhinal cortex (EC) and the hippocampal formation, which consists of the subiculum, the dentate gyrus (DG), and the hippocampus proper (Baddeley et al. 1991; deIpolyi et al. 2007; Greene et al. 1996). The hippocampus in particular has been greatly studied for its role in the progression of AD. In fact, current diagnostic tasks utilized for the detection of AD, such as the mini-mental status exam (MMSE), focus on deficits that become apparent when the functional integrity of the hippocampus and prefrontal cortex has been compromised (Sabuncu et al. 2011). Less understood is the role that the EC plays in the development of AD. This shortcoming is significant because the EC is one of the first areas impacted by tau pathology in the progression of AD and tau pathology beginning in the EC ultimately spreads to the hippocampus and prefrontal cortex as the disease progresses (Braak and Braak 1991). Thus, it is critical to understand the cognitive alterations resulting from pathology in the EC, so as to better detect cognitive deficits resulting from disease-related alterations in this region. Understanding cognitive deficits that result from pathology in this region may help identify potential novel therapeutic targets to attenuate the spread of tau pathology throughout the brain. This review will focus on animal and human work that delves into the relationship among aging, AD, and the EC.
Aging and AD
Evidence from the literature suggests that aging is one of the greatest risk factors for the development of AD (Harman 2006; Munoz and Feldman 2000; Xia et al. 2018). There quite a few age-related changes in brain function and activity that likely mediate this risk, one of which regards changes in network activity. Indeed, late-stage AD is associated with a variety of physiological changes but is frequently associated with neuron loss and subsequent network deficits in neuronal activity (de Haan et al. 2012; Hatanpää et al. 1996; Palop et al. 2007). However, there is evidence to suggest that in normal aging, as well as very early stages of AD, some brain regions are hyperactive instead. For example, aging has been associated with increases in hippocampal hyperactivity in both human and rodent models (El-Hayek et al. 2013; Reagh et al. 2018; Yassa et al. 2011). Neuronal hyperactivity, as measured by blood-oxygen level dependent (BOLD) functional magnetic resonance imaging (fMRI), is also a characteristic of amnestic mild cognitive impairment (aMCI) (Yassa et al. 2011), a measurable decline in cognitive function that is considered by some to be a risk factor for the development of AD (Mauri et al. 2012). Increased neuronal activity in patients with aMCI is indicative of the rate and possibility of development of AD in these individuals (10 to 15% progression rate annually in clinical samples) (Bakker et al. 2008; Oltra-Cucarella et al. 2018). In addition, hyperexcitability has been associated with cognitive deficits even in older adults that had normal scores on the MMSE (Yassa et al. 2011).
Neuronal hyperactivity is also associated with a number of maladaptive changes in human subjects as well as rodents, including cognitive decline (Reagh et al. 2018), enhanced seizure susceptibility (Cloyd et al. 2006; Stover et al. 2017), and the accumulation of tau but not beta-amyloid (Huijbers et al. 2019). Moreover, reducing neuronal hyperactivity in humans and rodents is sufficient to reduce cognitive deficits (Bakker et al. 2012; Hunsberger et al. 2015b; Koh et al. 2010; Sanchez et al. 2012), suggesting not only an association but a causative relationship between hyperactivity and cognitive decline. Of additional concern is evidence suggesting increased neuronal activity can also lead to excitotoxicity, a pathological process in which neurons are killed due to overactivation (Rudy et al. 2015). Therefore, detrimental changes in neuronal activity levels could serve as potential therapeutic targets to halt or slow the progression from normal aging or aMCI to AD. Of great interest, then, is understanding potential mechanisms that may contribute to these activity alterations and how they may be permissive for the development of AD.
One of the mechanisms that may underlie alterations in neuronal activity is dysregulation of glutamatergic neurotransmission. There is increasing evidence that aging results in enhanced glutamatergic signaling, suggesting one mechanism by which aging might increase the risk for AD. Several animal studies have indicated enhanced glutamate release and/or reduced glutamate clearance in aged rodents (Saransaari and Oja 1995; Stephens et al. 2011). These observations might be due to underlying increases in VGLUT, promoting increased release of glutamate into the synapse (Cheng et al. 2011). In addition, aging is associated with reductions in levels of EAATs, such as GLT-1, resulting in less glutamate clearance from the synapse (Potier et al. 2010; Zoia et al. 2004) leading to increased resting, or tonic, glutamate levels in some cases (Velasco and Tapia 2002). However, other studies have found the opposite, such that aged rodents exhibit decreased glutamate release and/or enhanced glutamate clearance (Mullany et al. 1996). The discrepancies that have been observed may be due to varied ages in the animal models as well as the methods utilized to measure glutamatergic alterations.
In disease states such as AD, glutamatergic signaling also becomes disrupted and these changes have been associated with the presence of tau pathology. Using enzyme-based microelectrode array, our laboratory has observed tau-associated increases in glutamate release and decrease in glutamate clearance in the rTg4510 mouse line, which overexpresses the mutant P301L form of human tau (Hunsberger et al. 2014, 2015a, b). Increases in glutamate release were associated with increased levels of VGLUT, while reductions in glutamate clearance were associated with reductions in levels of GLT-1. Using riluzole to restore these alterations resulted in attenuated cognitive deficits and pathology, which suggests a causative role for increased glutamatergic signaling and cognitive impairment.
These glutamatergic alterations can lead to excess extracellular glutamate, which can initiate cell death-signaling pathways by “spill-over” activation of extrasynaptic NMDARs (Gouix et al. 2009; Potier et al. 2010). Furthermore, an increase in activation of extrasynaptic NMDARs leads to increased tau phosphorylation, which can be reduced by blocking extrasynaptic NMDARs and their associated receptor subunits (Allyson et al. 2010).
Ultimately, enhanced excitatory neurotransmission may create an excitotoxic environment with greater susceptibility to the development and progression of AD. This is critical, because increasing evidence suggests that hyperexcitability can exacerbate the severity of tau pathology and promote its spread in AD.
Tau and AD
While much of the research over the past few decades has focused on beta-amyloid pathology as a therapeutic target for the treatment of AD, therapeutic interventions focusing solely on beta-amyloid have proven largely unsuccessful (Higuchi et al. 2005; Holmes et al. 2008; Honig et al. 2018; Rosenblum 2014; Salloway et al. 2014; Vellas et al. 2013). Additionally, many reports have indicated that the presence of tau pathology more closely correlates with the rate of cognitive decline than does beta-amyloid (Arriagada et al. 1992; Gómez-Isla et al. 1997; Nelson et al. 2012). Though beta-amyloid is thought to initiate tau pathology (Hardy and Higgins 1992; Kowalska 2004), tau pathology once initiated may be self-perpetuating and beta-amyloid independent (Ashe and Zahs 2010; Guo and Lee 2013). Thus, it is equally important to investigate tau as a therapeutic target in the treatment of AD.
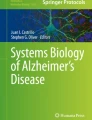
One of the aspects that makes tau a unique therapeutic target is the pattern of its progression. Early tau pathology is more localized than early beta-amyloid pathology, beginning in the entorhinal cortex before spreading to the hippocampus and prefrontal cortex as the disease progresses (see Fig. 1) (Braak and Braak 1991; Braak and Del Tredici 2018; Liu et al. 2012). The mechanisms behind this spread are still not well understood. However, increasing evidence suggests that increases in excitatory neurotransmission may mediate the spread of tau pathology across synaptically connected circuits, a process termed trans-synaptic spread. Additionally, there is evidence from the literature that suggests that the presence of pathological tau also results in excess excitatory neurotransmission, indicating a feedback loop between the two phenomena (Bi et al. 2017; Siano et al. 2019). In agreement, knocking down or knocking out tau in rodent or drosophila models resulted in protection from kainic acid-induced seizures, indicating that tau itself plays a role in excitotoxicity in the absence of beta-amyloid (Pallo et al. 2016; Palop et al. 2007; Roberson et al. 2011). Thus, the importance of better understanding the role that tau pathology plays in the progression of the disease and as a potential therapeutic target is clear. An overview of tau protein and the ways in which it becomes dysfunctional in tauopathies like Alzheimer’s disease will be discussed below.

In comparison to early beta-amyloid pathology, early tau pathology is more localized in most patients. Stages I-II consists of early tau pathology primarily deposited in the EC (LEC, specifically). In stages III-IV, tau pathology has begun to spread to the hippocampus and prefrontal cortex. In stages V-VI, tau pathology has spread into the neocortex. By the time tau pathology reaches these areas, it is severe in the origin areas. Darker shading/coloration indicates more severe pathology progression
Tau is a protein important for the assembly and stabilization of microtubules (Weingarten et al. 1975), which earns it the name microtubule-associated protein tau (or MAPT). Tau is a phosphoprotein, which means it is post-translationally modified by the addition of phosphate groups in a process known as phosphorylation (Mawal-Dewan et al. 1994). Its longest isoform (containing 441 amino acids) has 80 serine or threonine sites on which it can be phosphorylated, though tau protein can be phosphorylated on tyrosine sites as well (Goedert et al. 1989). While tau is highly phosphorylated in fetal brains, this phosphorylation generally decreases throughout development and as the brain ages (Goedert et al. 1989). Changes in the amount of tau phosphorylation as the brain ages are due to alterations in the levels of kinases, enzymes that phosphorylate proteins, and phosphatases, enzymes that dephosphorylate proteins (Mawal-Dewan et al. 1994).
Tau is normally an intracellular protein primarily found in neurons, specifically in the axons (Wood et al. 1986). Besides stabilization of the microtubule, tau is thought to have some other functional roles in a healthy brain. Intracellularly, tau is important for axonal transport of signaling molecules via motor proteins such as kinesin and dynein (Chaudhary et al. 2018). Tau is also critical for neuronal development, as it plays a role in neurite outgrowth (Wang and Mandelkow 2016). Additionally, though the presence of extracellular tau has been indicated as a major player in tauopathies such as AD (Delacourte and Defossez 1986; Grundke-Iqbal et al. 1986), there is evidence that tau can be found extracellularly in the absence of disease. For example, tau has been found in the interstitial fluid of wild-type mice (Yamada et al. 2011) and in human cerebral spinal fluid (CSF) in the absence of any measurable cognitive changes (Fagan et al. 2009; Handoko et al. 2013; Laws et al. 2017). This evidence appears to suggest that there is a normal, physiological role for extracellular tau. As such, it has been proposed that tau may play an important role in inter-neuronal signaling (Chaudhary et al. 2018). In disease states, however, tau protein becomes dysfunctional in a myriad of ways.
In AD, tau aggregates into paired-helical filaments (PHF), which are the main structural element of neurofibrillary tangles (Goedert et al. 1989). Increased tau phosphorylation, generally termed as hyperphosphorylation, was found to be a key player in the formation of PHFs (Goedert 1993). Additional research determined that in AD, tau is hyperphosphorylated at a rate about three to fourfold higher than in normal brains (Kenessey and Yen 1993; Köpke et al. 1993), which may be due to increased levels of kinases and decreased levels of phosphatases. There are several consequences of these changes in phosphorylation. Hyperphosphorylation of tau negatively impacts its ability to bind to microtubules (Lindwall and Cole 1984). This hyperphosphorylation of tau has been observed to cause mislocalization of tau from axons to somatodendritic compartments leading to synaptic deficits and mediating beta-amyloid toxicity (Hoover et al. 2010; Ittner et al. 2010). In addition to changes in phosphorylation, tau protein can also become misfolded in AD (Tai et al. 2012). This conformational change results in increased propensity of aggregation into neurofibrillary tangles (Tai et al. 2012).
Tau is normally an intracellular protein; however, after pathological tau results in neuronal death, it can accumulate extracellularly as ghost tangles (Bancher et al. 1989). Because of this, it had been assumed that the increased neuronal death that occurs in the disease state may underlie the release of tau into the extracellular space and findings of increased tau in cerebral spinal fluid (CSF) as the disease progresses. However, multiple studies have indicated that the neuron need not die for tau to be released into the extracellular space, and the presence of extracellular tau does not seem to be correlated with markers of cell damage such as LDH activity (Chai et al. 2012; Yamada et al. 2014; Yamada and Iwatsubo 2018). Tau can also be found in interstitial spinal fluid and CSF prior to neurodegeneration (Barten et al. 2012; Yamada et al. 2011). Additionally, the spread of tau seeds precedes neurodegeneration and neither the presence of hyperphosphorylated tau nor tau aggregates are immediately toxic to neurons (Hallinan et al. 2018).
Once tau reaches the extracellular space, regardless of the mechanism, it can be taken up by neighboring neurons, ultimately compromising them as well (Wu et al. 2016). It is in this way that pathological tau is thought to behave in a prion-like fashion along synaptically connected neural networks (Frost and Diamond 2009; Guo and Lee 2011; Kfoury et al. 2012). Prions are misfolded proteins with the ability to transmit their misfolded shape onto normal variants of the same protein. Supporting the prion tau-spread theory, human pluripotent stem-cell models have been utilized to demonstrate that pathological tau released from initially infected cells into the medium can thereafter be taken in by previously unaffected recipient cells. Further, aberrant tau can be released by these recipients and taken in by new recipients, indicating a cell-to-cell propagation (Wu et al. 2016). The prion-like propagation of tau pathology has also been demonstrated in vivo. Injection of brain homogenates from mice expressing mutant tau into mice expressing wild-type tau results in the assembly of the wild-type tau into NFTs and neuropil threads (NTs), and this pathology spreads to synaptically connected brain regions (Clavaguera et al. 2015). Additionally, injection of brain extract from older mice expressing mutated tau (Ahmed et al. 2014; Peeraer et al. 2015), or synthetic pre-formed fibrils from full-length or truncated tau (Iba et al. 2013) into the brains of younger mice expressing mutant tau (prior to expression of tau pathology) also resulted in enhanced prion-like spread of tau pathology along synaptically connected circuits.
The latter finding, that of the spread of tau from brain region to brain region, has also been of great focus in the literature. Tau can spread along mono-synaptic (across one synapse) or trans-synaptic (across more than one synapse) circuits (Liu et al. 2012). Mice expressing mutant P301L tau restricted to layer II of the EC also exhibit propagation to connected regions such as hippocampal subregions and the cingulate cortex (de Calignon et al. 2012). This spread of tau is not limited to pathological or mutant tau, as wild-type tau also can spread along axonal connections to distal brain regions (Dujardin et al. 2014). The trans-synaptic pathology spread suggests that propagation of tau pathology is an active process that is synaptically-linked and not solely limited to targeting nearby neurons.
The entorhinal cortex, tau, and AD
The literature suggests that the EC is one of the first regions in the brain to develop tau pathology (Braak and Braak 1991; Kaufman et al. 2018; Welikovitch et al. 2018). However, compared to the hippocampus, the functional role of the EC in cognition as well as in the progression of AD is relatively poorly understood. In order to target maladaptive alterations that are EC-dependent, this region needs to be further studied. An overview of the EC and its role in the spread of tau in AD is discussed further, below.
The entorhinal cortex, so named because it is partially enclosed by the rhinal sulcus, is located in the medial temporal lobe between the transentorhinal area and the hippocampal formation. In mice, the EC consists of the medial and lateral entorhinal cortices (MEC and LEC, respectively), whereas in humans, the EC is divided into the anterolateral (front and to the side) and posteromedial (to the back and at the center) entorhinal areas (Maass et al. 2015).
The EC can be separated into six layers. Layer I of the entorhinal cortex receives olfactory input and projects to the presubiculum, peririhinal cortices, and amygdala. Layer II projects to the dentate gyrus (DG) and cornu ammonis 3 (CA3) subregions of the hippocampus, whereas Layer III projects to the cornu ammonis 1 (CA1) and subiculum subregions of the hippocampus. The Layer II and III hippocampal projections are referred to as the perforant pathway. In turn, the deeper layers (Layers IV and V) of the EC receive input from the CA1, a pathway called the third synaptic connection (see Fig. 2). Information processed via the third synaptic connection eventually projects to the striatum, amygdala, and thalamus. Layer VI is still not well understood (Canto and Witter 2012). The projections between the EC and hippocampus are impacted in both early AD and aMCI, causing disruptions in neuronal signaling (see Fig. 2).

The entorhinal cortex projects to the dentate gyrus (DG) and CA1 hippocampal subregions (referred to as the perforant pathway). The dentate gyrus projects to the CA3 hippocampal subregion (referred to as the mossy fiber pathway). The CA3 has autoassociative (or recurrent) tracts that project onto itself. The CA3 also projects to the CA1 via the Schaffer collateral pathway, and the CA1 projects back to the entorhinal cortex (third synaptic connection). Evidence from the literature suggests that alterations such as hypoactivity (blue arrow) in the EC are associated with increases in activity (red arrows) in the DG and CA3
Generally, the hippocampus is most commonly denoted as the neurobiological source for episodic memory (Desgranges et al. 1998). However, it is also clear that the entorhinal cortex plays a significant role in episodic memory (Wilson et al. 2013b). Memory tasks that assess performance in regard to this type of contextual information have been purported to represent a rodent model of episodic memory (Eacott and Easton 2010). Briefly, components of this model include information regarding objects within a given environment, information regarding the spatial aspects of the objects in that environment, and aspects of the environment itself.
The combination of processing non-spatial and spatial information as described above is important for a type of memory known as associative memory. Associative memory tasks involve altering two or more aspects (object recognition, object location, and contextual properties) of the environment in order to assess an animal’s ability to detect novelty. For example, a task may involve exposing the animal to a specific environment and then either altering the objects within the environment, the locations of said objects, the context itself, or some combination thereof. The combinations are thus referred to as associative memory, as proper performance on these tasks requires the animal to remember the association between the object, locations, and context to which the animal has been previously exposed. Lesion studies have determined that while LEC-lesioned rodents are able to detect changes in object or object location alone, these animals are unable to detect changes in tasks that involve associative memory, such as object-object location, object location-context, or object-object location-context combinations (Hunsaker et al. 2013; Wilson, et al. 2013a, b).
To our knowledge, there are no currently existing animal studies examining the impact of tau (or beta-amyloid) pathology within the EC on EC-dependent cognition. However, evidence from human literature sheds some light on what impact AD-associated changes, such as alterations in excitotoxicity has on EC-dependent cognitive performance. For example, hypoactivity in the EC and hyperactivity of hippocampal DG and CA3 subregions, as identified by changes in fMRI blood-oxygen level dependent (BOLD) activation, is associated with a shift toward responses indicating pattern completion rather than pattern separation (Bakker et al. 2012), which is not observed when the task has a spatial component (i.e. objects within a specific location in an environment) (Reagh et al. 2018). Recent studies have identified the anterolateral entorhinal cortex (alEC), rather than the posteromedial entorhinal cortex (pmEC), as the specific subregion of the entorhinal cortex that is hypoactive in older adults (Berron et al. 2019; Reagh et al. 2018) and that this dysfunction is associated with higher levels of tau in cerebrospinal fluid.
The functional imbalance observed in these cases may well have to do with the projections from EC to DG and CA3 hippocampal subregions via the perforant pathway. The projections between the EC and hippocampus are impacted in both early AD and aMCI, causing disruptions in neuronal signaling (see Fig. 2). What is unknown is the directionality of these alterations in human studies. That is, whether it is the EC hypoactivity that is causing DG/CA3 hyperactivity, or the reverse. It has been theorized that CA3/DG hyperactivity could lead to retrograde degeneration of the perforant pathway in human subjects (Reagh et al. 2018). It has been also been theorized that the disrupted EC signaling leads to inadvertent activation of the CA3 recurrent tracts, promoting a state of hyperexcitability (Reagh et al. 2018). Studies assessing the role of early EC activity in humans are lacking, potentially due to the degradation of this region by the time hippocampal-dependent changes are apparent.
Volumetric changes in the alEC are also predictive of ability to process repeated versus similar objects (Yeung et al. 2017). As volume decreases are also observed in the LEC in preclinical AD (Yeung et al. 2017), these region-specific changes and resultant impact on object-recognition memory may represent a precise target for development of a diagnostic task sensitive to early AD alterations.
In addition, because hippocampal subregions receive major excitatory input from Layer II of the EC, it has been proposed that changes observed in cognitive aging and aMCI are likely resultant from a disruption in EC-hippocampal afferents (Smith et al. 2000). Indeed, evidence has shown that input from Layer II of the EC is reduced with increasing age (Geinisman et al. 1992; Scheff et al. 2006). Additionally, synapses that project from Layer II of the EC to the CA1 hippocampal subregion undergo degeneration in AD mouse models (Shih et al. 2016). The EC is also one of the first areas to undergo neuronal loss in early AD. For example, by the time individuals affected by cognitive aging or aMCI have progressed to even mild AD, they can exhibit 60% neuron loss in Layer II of the EC compared to a normal individual (Gómez-Isla et al. 1996; Kordower et al. 2001). In conjunction, the EC is significantly atrophied in AD compared to other brain regions (Kordower et al. 2001; Van Hoesen et al. 1991).
While there are several studies examining the role of EC in cognition via EC-lesions, as well as studies assessing the impact of EC activity alterations on cognition, there is a gap in the literature regarding the impact of pathological tau in the EC on EC-dependent cognitive tasks.
Conclusion
The key to better understanding the pathophysiology of AD, and therefore offering a better prognosis for affected individuals, is understanding one of the major regions that AD pathology originates from. It is clear from the evidence in the literature, as disseminated in this review, that aging and early AD result in alterations in network activity in the EC and hippocampus. These alterations create an environment of excitotoxicity which is then permissive to promote and propagate the spread of tau pathology. In turn, pathological tau deposition, once initiated, begets further tau pathology as well as mediating both beta-amyloid toxicity and exacerbated excitatory neurotransmission. While these observations have been documented in the literature, not much focus has been given to the impact of early AD pathology within the entorhinal cortex on EC-related cognitive function. This review hopes to offer a comprehensive starting point in terms of the currently known information and the gaps that need to currently be filled. In addition, understanding what changes that occur in this region lead to the spread of pathological tau, such as hyperactivity, is fundamental in the advancement of the field.
References
Ahmed Z, Cooper J, Murray TK, Garn K, McNaughton E, Clarke H, … Jackson S (2014) A novel in vivo model of tau propagation with rapid and progressive neurofibrillary tangle pathology: the pattern of spread is determined by connectivity, not proximity. Acta Neuropathol 127(5):667–683
Allyson J, Dontigny E, Auberson Y, Cyr M, Massicotte G (2010) Blockade of NR2A-containing NMDA receptors induces Tau phosphorylation in rat hippocampal slices. Neural Plast 2010:340168. https://doi.org/10.1155/2010/340168
Arriagada PV, Growdon JH, Hedley-Whyte ET, Hyman BT (1992) Neurofibrillary tangles but not senile plaques parallel duration and severity of Alzheimer’s disease. Neurology 42(3 Pt 1):631–639. https://doi.org/10.1212/wnl.42.3.631
Ashe KH, Zahs KR (2010) Probing the biology of Alzheimer’s disease in mice. Neuron 66(5):631–645. https://doi.org/10.1016/j.neuron.2010.04.031
Atri A (2019) The Alzheimer’s disease clinical spectrum: Diagnosis and management. Medical Clinics 103(2):263–293
Baddeley AD, Bressi S, Della Sala S, Logie R, Spinnler H (1991) The decline of working memory in Alzheimer’s disease. A Longitudinal Study. Brain 114(Pt 6):2521–2542. https://doi.org/10.1093/brain/114.6.2521
Bakker A, Kirwan CB, Miller M, Stark CE (2008) Pattern separation in the human hippocampal CA3 and dentate gyrus. Science 319(5870):1640–1642. https://doi.org/10.1126/science.1152882
Bakker A, Krauss GL, Albert MS, Speck CL, Jones LR, Stark CE, … Gallagher M (2012) Reduction of hippocampal hyperactivity improves cognition in amnestic mild cognitive impairment. Neuron 74(3):467–474. https://doi.org/10.1016/j.neuron.2012.03.023
Bancher C, Brunner C, Lassmann H, Budka H, Jellinger K, Seitelberger F, … Wisniewski HM (1989) Tau and ubiquitin immunoreactivity at different stages of formation of Alzheimer neurofibrillary tangles. Prog Clin Biol Res 317:837–848
Barten DM, Fanara P, Andorfer C, Hoque N, Wong PA, Husted KH, … Liu V (2012) Hyperdynamic microtubules, cognitive deficits, and pathology are improved in tau transgenic mice with low doses of the microtubule-stabilizing agent BMS-241027. J Neurosci 32(21):7137–7145
Berron D, Cardenas-Blanco A, Bittner D, Metzger CD, Spottke A, Heneka MT, … Wagner M (2019) Higher CSF tau levels are related to hippocampal hyperactivity and object mnemonic discrimination in older adults. J Neurosci 39(44):8788–8797
Bi M, Gladbach A, Van Eersel J, Ittner A, Przybyla M, Van Hummel A, … Müller J (2017) Tau exacerbates excitotoxic brain damage in an animal model of stroke. Nat Commun 8(1):1–15
Braak H, Braak E (1991) Neuropathological stageing of Alzheimer-related changes. Acta Neuropathol 82(4):239–259. https://doi.org/10.1007/bf00308809
Braak H, Del Tredici K (2018) Spreading of tau pathology in sporadic Alzheimer’s disease along cortico-cortical top-down connections. Cereb Cortex 28(9):3372–3384
Canto CB, Witter MP (2012) Cellular properties of principal neurons in the rat entorhinal cortex. I. The Lateral Entorhinal Cortex. Hippocampus 22(6):1256–1276. https://doi.org/10.1002/hipo.20997
Chai X, Dage JL, Citron M (2012) Constitutive secretion of tau protein by an unconventional mechanism. Neurobiol Dis 48(3):356–366
Chaudhary AR, Berger F, Berger CL, Hendricks AG (2018) Tau directs intracellular trafficking by regulating the forces exerted by kinesin and dynein teams. Traffic 19(2):111–121. https://doi.org/10.1111/tra.12537
Cheng XR, Yang Y, Zhou WX, Zhang YX (2011) Expression of VGLUTs contributes to degeneration and acquisition of learning and memory. Neurobiol Learn Mem 95(3):361–375. https://doi.org/10.1016/j.nlm.2011.01.010
Clavaguera F, Hench J, Goedert M, Tolnay M (2015) Invited review: Prion-like transmission and spreading of tau pathology. Neuropathol Appl Neurobiol 41(1):47–58
Cloyd J, Hauser W, Towne A, Ramsay R, Mattson R, Gilliam F, Walczak T (2006) Epidemiological and medical aspects of epilepsy in the elderly. Epilepsy Res 68(Suppl 1):S39-48. https://doi.org/10.1016/j.eplepsyres.2005.07.016
de Calignon A, Polydoro M, Suárez-Calvet M, William C, Adamowicz DH, Kopeikina KJ, … Hyman BT (2012) Propagation of tau pathology in a model of early Alzheimer’s disease. Neuron 73(4):685–697. https://doi.org/10.1016/j.neuron.2011.11.033
de Haan W, Mott K, van Straaten EC, Scheltens P, Stam CJ (2012) Activity dependent degeneration explains hub vulnerability in Alzheimer’s disease. PLoS Comput Biol 8(8):e1002582. https://doi.org/10.1371/journal.pcbi.1002582
deIpolyi AR, Rankin KP, Mucke L, Miller BL, Gorno-Tempini ML (2007) Spatial cognition and the human navigation network in AD and MCI. Neurology 69(10):986–997. https://doi.org/10.1212/01.wnl.0000271376.19515.c6
Delacourte A, Defossez A (1986) Alzheimer’s disease: Tau proteins, the promoting factors of microtubule assembly, are major components of paired helical filaments. J Neurol Sci 76(2–3):173–186. https://doi.org/10.1016/0022-510x(86)90167-x
Desgranges B, Baron JC, Eustache F (1998) The functional neuroanatomy of episodic memory: the role of the frontal lobes, the hippocampal formation, and other areas. Neuroimage 8(2):198–213. https://doi.org/10.1006/nimg.1998.0359
Dujardin S, Lécolle K, Caillierez R, Bégard S, Zommer N, Lachaud C, … Winderickx J (2014) Neuron-to-neuron wild-type Tau protein transfer through a trans-synaptic mechanism: relevance to sporadic tauopathies. Acta Neuropathol Commun 2(1):1–14
Eacott MJ, Easton A (2010) Episodic memory in animals: remembering which occasion. Neuropsychologia 48(8):2273–2280. https://doi.org/10.1016/j.neuropsychologia.2009.11.002
El-Hayek YH, Wu C, Ye H, Wang J, Carlen PL, Zhang L (2013) Hippocampal excitability is increased in aged mice. Exp Neurol 247:710–719. https://doi.org/10.1016/j.expneurol.2013.03.012
Fagan AM, Mintun MA, Shah AR, Aldea P, Roe CM, Mach RH, … Holtzman DM (2009) Cerebrospinal fluid tau and ptau(181) increase with cortical amyloid deposition in cognitively normal individuals: implications for future clinical trials of Alzheimer’s disease. EMBO Mol Med 1(8–9):371–380. https://doi.org/10.1002/emmm.200900048
Frost B, Diamond MI (2009) The expanding realm of prion phenomena in neurodegenerative disease. Prion 3(2):74–77. https://doi.org/10.4161/pri.3.2.8754
Geinisman Y, deToledo-Morrell L, Morrell F, Persina IS, Rossi M (1992) Age-related loss of axospinous synapses formed by two afferent systems in the rat dentate gyrus as revealed by the unbiased stereological dissector technique. Hippocampus 2(4):437–444. https://doi.org/10.1002/hipo.450020411
Goedert M (1993) Tau protein and the neurofibrillary pathology of Alzheimer’s disease. Trends Neurosci 16(11):460–465. https://doi.org/10.1016/0166-2236(93)90078-z
Goedert M, Spillantini MG, Jakes R, Rutherford D, Crowther RA (1989) Multiple isoforms of human microtubule-associated protein tau: sequences and localization in neurofibrillary tangles of Alzheimer’s disease. Neuron 3(4):519–526. https://doi.org/10.1016/0896-6273(89)90210-9
Gómez-Isla T, Price JL, McKeel DW Jr, Morris JC, Growdon JH, Hyman BT (1996) Profound loss of layer II entorhinal cortex neurons occurs in very mild Alzheimer’s disease. J Neurosci 16(14):4491–4500. https://doi.org/10.1523/jneurosci.16-14-04491.1996
Gómez-Isla T, Hollister R, West H, Mui S, Growdon JH, Petersen RC, … Hyman BT (1997) Neuronal loss correlates with but exceeds neurofibrillary tangles in Alzheimer’s disease. Ann Neurol 41(1):17–24. https://doi.org/10.1002/ana.410410106
Gouix E, Léveillé F, Nicole O, Melon C, Had-Aissouni L, Buisson A (2009) Reverse glial glutamate uptake triggers neuronal cell death through extrasynaptic NMDA receptor activation. Mol Cell Neurosci 40(4):463–473. https://doi.org/10.1016/j.mcn.2009.01.002
Greene JD, Baddeley AD, Hodges JR (1996) Analysis of the episodic memory deficit in early Alzheimer’s disease: evidence from the doors and people test. Neuropsychologia 34(6):537–551. https://doi.org/10.1016/0028-3932(95)00151-4
Grundke-Iqbal I, Iqbal K, Tung YC, Quinlan M, Wisniewski HM, Binder LI (1986) Abnormal phosphorylation of the microtubule-associated protein tau (tau) in Alzheimer cytoskeletal pathology. Proc Natl Acad Sci U S A 83(13):4913–4917. https://doi.org/10.1073/pnas.83.13.4913
Guo JL, Lee VM (2011) Seeding of normal Tau by pathological Tau conformers drives pathogenesis of Alzheimer-like tangles. J Biol Chem 286(17):15317–15331. https://doi.org/10.1074/jbc.M110.209296
Guo JL, Lee VM (2013) Neurofibrillary tangle-like tau pathology induced by synthetic tau fibrils in primary neurons over-expressing mutant tau. FEBS Lett 587(6):717–723. https://doi.org/10.1016/j.febslet.2013.01.051
Hallinan, G. I., Vargas-Caballero, M., West, J., & Deinhardt, K. (2018). Efficient propagation of misfolded Tau between individual neurons occurs in absence of degeneration. bioRxiv, 372029.
Handoko M, Grant M, Kuskowski M, Zahs KR, Wallin A, Blennow K, Ashe KH (2013) Correlation of specific amyloid-β oligomers with tau in cerebrospinal fluid from cognitively normal older adults. JAMA Neurol 70(5):594–599. https://doi.org/10.1001/jamaneurol.2013.48
Hardy JA, Higgins GA (1992) Alzheimer’s disease: the amyloid cascade hypothesis. Science 256(5054):184–185. https://doi.org/10.1126/science.1566067
Harman D (2006) Alzheimer’s disease pathogenesis: role of aging. Ann N Y Acad Sci 1067(1):454–460
Hatanpää K, Brady DR, Stoll J, Rapoport SI, Chandrasekaran K (1996) Neuronal activity and early neurofibrillary tangles in Alzheimer’s disease. Ann Neurol 40(3):411–420. https://doi.org/10.1002/ana.410400310
Higuchi M, Iwata N, Matsuba Y, Sato K, Sasamoto K, Saido TC (2005) 19F and 1H MRI detection of amyloid beta plaques in vivo. Nat Neurosci 8(4):527–533. https://doi.org/10.1038/nn1422
Holmes C, Boche D, Wilkinson D, Yadegarfar G, Hopkins V, Bayer A, … Nicoll JA (2008) Long-term effects of Abeta42 immunisation in Alzheimer’s disease: follow-up of a randomised, placebo-controlled phase I trial. Lancet 372(9634):216–223. https://doi.org/10.1016/s0140-6736(08)61075-2
Honig LS, Vellas B, Woodward M, Boada M, Bullock R, Borrie M, … Siemers E (2018) Trial of Solanezumab for mild dementia due to Alzheimer’s Disease. N Engl J Med 378(4):321–330. https://doi.org/10.1056/NEJMoa1705971
Hoover BR, Reed MN, Su J, Penrod RD, Kotilinek LA, Grant MK, … Liao D (2010) Tau mislocalization to dendritic spines mediates synaptic dysfunction independently of neurodegeneration. Neuron 68(6):1067–1081. https://doi.org/10.1016/j.neuron.2010.11.030
Huijbers W, Schultz AP, Papp KV, LaPoint MR, Hanseeuw B, Chhatwal JP, … Sperling RA (2019) Tau accumulation in clinically normal older adults is associated with hippocampal hyperactivity. J Neurosci 39(3):548–556. https://doi.org/10.1523/jneurosci.1397-18.2018
Hunsaker MR, Chen V, Tran GT, Kesner RP (2013) The medial and lateral entorhinal cortex both contribute to contextual and item recognition memory: a test of the binding of items and context model. Hippocampus 23(5):380–391. https://doi.org/10.1002/hipo.22097
Hunsberger HC, Rudy CC, Weitzner DS, Zhang C, Tosto DE, Knowlan K, … Reed MN (2014) Effect size of memory deficits in mice with adult-onset P301L tau expression. Behav Brain Res 272:181–195. https://doi.org/10.1016/j.bbr.2014.06.057
Hunsberger HC, Rudy CC, Batten SR, Gerhardt GA, Reed MN (2015a) P301L tau expression affects glutamate release and clearance in the hippocampal trisynaptic pathway. J Neurochem 132(2):169–182. https://doi.org/10.1111/jnc.12967
Hunsberger HC, Weitzner DS, Rudy CC, Hickman JE, Libell EM, Speer RR, … Reed MN (2015b) Riluzole rescues glutamate alterations, cognitive deficits, and tau pathology associated with P301L tau expression. J Neurochem 135(2):381–394. https://doi.org/10.1111/jnc.13230
Hyman BT, Phelps CH, Beach TG, Bigio EH, Cairns NJ, Carrillo MC, … Montine TJ (2012) National Institute on Aging-Alzheimer’s Association guidelines for the neuropathologic assessment of Alzheimer’s disease. Alzheimers Dement 8(1):1–13. https://doi.org/10.1016/j.jalz.2011.10.007
Iba M, Guo JL, McBride JD, Zhang B, Trojanowski JQ, Lee VM-Y (2013) Synthetic tau fibrils mediate transmission of neurofibrillary tangles in a transgenic mouse model of Alzheimer’s-like tauopathy. J Neurosci 33(3):1024–1037
Isik AT, Soysal P, Solmi M, Veronese N (2019) Bidirectional relationship between caregiver burden and neuropsychiatric symptoms in patients with Alzheimer’s disease: a narrative review. Int J Geriatr Psychiatry 34(9):1326–1334
Ittner LM, Ke YD, Delerue F, Bi M, Gladbach A, van Eersel J, … Götz J (2010) Dendritic function of tau mediates amyloid-beta toxicity in Alzheimer’s disease mouse models. Cell 142(3):387–397. https://doi.org/10.1016/j.cell.2010.06.036
Kaufman SK, Del Tredici K, Thomas TL, Braak H, Diamond MI (2018) Tau seeding activity begins in the transentorhinal/entorhinal regions and anticipates phospho-tau pathology in Alzheimer’s disease and PART. Acta Neuropathol 136(1):57–67
Kenessey A, Yen SH (1993) The extent of phosphorylation of fetal tau is comparable to that of PHF-tau from Alzheimer paired helical filaments. Brain Res 629(1):40–46. https://doi.org/10.1016/0006-8993(93)90478-6
Kfoury N, Holmes BB, Jiang H, Holtzman DM, Diamond MI (2012) Trans-cellular propagation of Tau aggregation by fibrillar species. J Biol Chem 287(23):19440–19451. https://doi.org/10.1074/jbc.M112.346072
Koh MT, Haberman RP, Foti S, McCown TJ, Gallagher M (2010) Treatment strategies targeting excess hippocampal activity benefit aged rats with cognitive impairment. Neuropsychopharmacology 35(4):1016–1025. https://doi.org/10.1038/npp.2009.207
Köpke E, Tung YC, Shaikh S, Alonso AC, Iqbal K, Grundke-Iqbal I (1993) Microtubule-associated protein tau. Abnormal phosphorylation of a non-paired helical filament pool in Alzheimer disease. J Biol Chem 268(32):24374–24384
Kordower JH, Chu Y, Stebbins GT, DeKosky ST, Cochran EJ, Bennett D, Mufson EJ (2001) Loss and atrophy of layer II entorhinal cortex neurons in elderly people with mild cognitive impairment. Ann Neurol 49(2):202–213
Kowalska A (2004) The beta-amyloid cascade hypothesis: a sequence of events leading to neurodegeneration in Alzheimer’s disease. Neurol Neurochir Pol 38(5):405–411
Laws SM, Gaskin S, Woodfield A, Srikanth V, Bruce D, Fraser PE, … Verdile G (2017) Insulin resistance is associated with reductions in specific cognitive domains and increases in CSF tau in cognitively normal adults. Sci Rep 7(1):9766. https://doi.org/10.1038/s41598-017-09577-4
Lindsay J, Laurin D, Verreault R, Hébert R, Helliwell B, Hill GB, McDowell I (2002) Risk factors for Alzheimer’s disease: a prospective analysis from the Canadian Study of Health and Aging. Am J Epidemiol 156(5):445–453. https://doi.org/10.1093/aje/kwf074
Lindwall G, Cole RD (1984) Phosphorylation affects the ability of tau protein to promote microtubule assembly. J Biol Chem 259(8):5301–5305
Liu L, Drouet V, Wu JW, Witter MP, Small SA, Clelland C, Duff K (2012) Trans-synaptic spread of tau pathology in vivo. PLoS ONE 7(2):e31302. https://doi.org/10.1371/journal.pone.0031302
Maass A, Berron D, Libby LA, Ranganath C, Düzel E (2015) Functional subregions of the human entorhinal cortex. Elife 4:e06426. https://doi.org/10.7554/eLife.06426
Mauri M, Sinforiani E, Zucchella C, Cuzzoni MG, Bono G (2012) Progression to dementia in a population with amnestic mild cognitive impairment: clinical variables associated with conversion. Funct Neurol 27(1):49–54
Mawal-Dewan M, Henley J, Van de Voorde A, Trojanowski JQ, Lee VM (1994) The phosphorylation state of tau in the developing rat brain is regulated by phosphoprotein phosphatases. J Biol Chem 269(49):30981–30987
Mullany P, Connolly S, Lynch MA (1996) Ageing is associated with changes in glutamate release, protein tyrosine kinase and Ca2+/calmodulin-dependent protein kinase II in rat hippocampus. Eur J Pharmacol 309(3):311–315. https://doi.org/10.1016/0014-2999(96)00464-5
Munoz DG, Feldman H (2000) Causes of Alzheimer’s Disease. Cmaj 162(1):65–72
Nelson PT, Alafuzoff I, Bigio EH, Bouras C, Braak H, Cairns NJ, … Beach TG (2012) Correlation of Alzheimer disease neuropathologic changes with cognitive status: a review of the literature. J Neuropathol Exp Neurol 71(5):362–381. https://doi.org/10.1097/NEN.0b013e31825018f7
Oltra-Cucarella J, Sánchez-SanSegundo M, Lipnicki DM, Sachdev PS, Crawford JD, Pérez-Vicente JA … Initiative, A. s. D. N. (2018) Using base rate of low scores to identify progression from amnestic mild cognitive impairment to Alzheimer’s disease. J Am Geriatr Soc 66(7):1360–1366
Pallo SP, DiMaio J, Cook A, Nilsson B, Johnson GV (2016) Mechanisms of tau and Aβ-induced excitotoxicity. Brain Res 1634:119–131
Palop JJ, Chin J, Roberson ED, Wang J, Thwin MT, Bien-Ly N, … Mucke L (2007) Aberrant excitatory neuronal activity and compensatory remodeling of inhibitory hippocampal circuits in mouse models of Alzheimer’s disease. Neuron 55(5):697–711. https://doi.org/10.1016/j.neuron.2007.07.025
Peeraer E, Bottelbergs A, Van Kolen K, Stancu I-C, Vasconcelos B, Mahieu M, … Sluydts E (2015) Intracerebral injection of preformed synthetic tau fibrils initiates widespread tauopathy and neuronal loss in the brains of tau transgenic mice. Neurobiol Dis 73:83–95
Potier B, Billard JM, Rivière S, Sinet PM, Denis I, Champeil-Potokar G, … Dutar P (2010) Reduction in glutamate uptake is associated with extrasynaptic NMDA and metabotropic glutamate receptor activation at the hippocampal CA1 synapse of aged rats. Aging Cell 9(5):722–735. https://doi.org/10.1111/j.1474-9726.2010.00593.x
Rajan, K. B., Weuve, J., Barnes, L. L., McAninch, E. A., Wilson, R. S., & Evans, D. A. (2021). Population estimate of people with clinical Alzheimer's disease and mild cognitive impairment in the United States (2020–2060). Alzheimer's & Dementia.
Reagh ZM, Noche JA, Tustison NJ, Delisle D, Murray EA, Yassa MA (2018) Functional imbalance of anterolateral entorhinal cortex and hippocampal dentate/CA3 underlies age-related object pattern separation deficits. Neuron 97(5):1187-1198.e1184. https://doi.org/10.1016/j.neuron.2018.01.039
Roberson ED, Halabisky B, Yoo JW, Yao J, Chin J, Yan F, … Mucke L (2011) Amyloid-β/Fyn-induced synaptic, network, and cognitive impairments depend on tau levels in multiple mouse models of Alzheimer’s disease. J Neurosci 31(2):700–711. https://doi.org/10.1523/jneurosci.4152-10.2011
Rosenblum WI (2014) Why Alzheimer trials fail: removing soluble oligomeric beta amyloid is essential, inconsistent, and difficult. Neurobiol Aging 35(5):969–974
Rudy CC, Hunsberger HC, Weitzner DS, Reed MN (2015) The role of the tripartite glutamatergic synapse in the pathophysiology of Alzheimer’s disease. Aging Dis 6(2):131–148. https://doi.org/10.14336/ad.2014.0423
Sabuncu MR, Desikan RS, Sepulcre J, Yeo BT, Liu H, Schmansky NJ, … Fischl B (2011) The dynamics of cortical and hippocampal atrophy in Alzheimer disease. Arch Neurol 68(8):1040–1048. https://doi.org/10.1001/archneurol.2011.167
Salloway S, Sperling R, Fox NC, Blennow K, Klunk W, Raskind M, … Brashear HR (2014) Two phase 3 trials of bapineuzumab in mild-to-moderate Alzheimer’s disease. N Engl J Med 370(4):322–333. https://doi.org/10.1056/NEJMoa1304839
Sanchez PE, Zhu L, Verret L, Vossel KA, Orr AG, Cirrito JR, … Mucke L (2012) Levetiracetam suppresses neuronal network dysfunction and reverses synaptic and cognitive deficits in an Alzheimer’s disease model. Proc Natl Acad Sci U S A 109(42):E2895-2903. https://doi.org/10.1073/pnas.1121081109
Saransaari P, Oja SS (1995) Age-related changes in the uptake and release of glutamate and aspartate in the mouse brain. Mech Ageing Dev 81(2–3):61–71. https://doi.org/10.1016/0047-6374(95)01583-l
Scheff SW, Price DA, Schmitt FA, Mufson EJ (2006) Hippocampal synaptic loss in early Alzheimer’s disease and mild cognitive impairment. Neurobiol Aging 27(10):1372–1384. https://doi.org/10.1016/j.neurobiolaging.2005.09.012
Shih Y-H, Tsai S-F, Huang S-H, Chiang Y-T, Hughes M, Wu S-Y, … Kuo Y-M (2016) Hypertension impairs hippocampus-related adult neurogenesis, CA1 neuron dendritic arborization and long-term memory. Neuroscience 322:346–357
Siano G, Varisco M, Caiazza MC, Quercioli V, Mainardi M, Ippolito C, … Di Primio C (2019) Tau modulates VGluT1 expression. J Mol Biol 431(4):873–884
Smith TD, Adams MM, Gallagher M, Morrison JH, Rapp PR (2000) Circuit-specific alterations in hippocampal synaptophysin immunoreactivity predict spatial learning impairment in aged rats. J Neurosci 20(17):6587–6593. https://doi.org/10.1523/jneurosci.20-17-06587.2000
Stephens ML, Quintero JE, Pomerleau F, Huettl P, Gerhardt GA (2011) Age-related changes in glutamate release in the CA3 and dentate gyrus of the rat hippocampus. Neurobiol Aging 32(5):811–820. https://doi.org/10.1016/j.neurobiolaging.2009.05.009
Stover KR, Lim S, Zhou TL, Stafford PM, Chow J, Li H, … Zhang L (2017) Susceptibility to hippocampal kindling seizures is increased in aging C57 black mice. IBRO Rep 3:33–44. https://doi.org/10.1016/j.ibror.2017.08.001
Tai HC, Serrano-Pozo A, Hashimoto T, Frosch MP, Spires-Jones TL, Hyman BT (2012) The synaptic accumulation of hyperphosphorylated tau oligomers in Alzheimer disease is associated with dysfunction of the ubiquitin-proteasome system. Am J Pathol 181(4):1426–1435. https://doi.org/10.1016/j.ajpath.2012.06.033
Van Hoesen GW, Hyman BT, Damasio AR (1991) Entorhinal cortex pathology in Alzheimer’s disease. Hippocampus 1(1):1–8. https://doi.org/10.1002/hipo.450010102
Vellas B, Carrillo MC, Sampaio C, Brashear HR, Siemers E, Hampel H, … Aisen P (2013) Designing drug trials for Alzheimer’s disease: what we have learned from the release of the phase III antibody trials: a report from the EU/US/CTAD Task Force. Alzheimers Dement 9(4):438–444. https://doi.org/10.1016/j.jalz.2013.03.007
Velasco I and Tapia R (2002) High extracellular gamma-aminobutyric acid protects cultured neurons against damage induced by the accumulation of endogenous extracellular glutamate. J Neurosci Res 67(3):406–410. https://doi.org/10.1002/jnr.10114
Wang Y, Mandelkow E (2016) Tau in physiology and pathology. Nat Rev Neurosci 17(1):5–21. https://doi.org/10.1038/nrn.2015.1
Weingarten MD, Lockwood AH, Hwo S-Y, Kirschner MW (1975) A protein factor essential for microtubule assembly. Proc Natl Acad Sci 72(5):1858–1862
Welikovitch LA, Do Carmo S, Maglóczky Z, Szocsics P, Lőke J, Freund T, Cuello AC (2018) Evidence of intraneuronal Aβ accumulation preceding tau pathology in the entorhinal cortex. Acta Neuropathol 136(6):901–917
Wilson DI, Langston RF, Schlesiger MI, Wagner M, Watanabe S, Ainge JA (2013a) Lateral entorhinal cortex is critical for novel object-context recognition. Hippocampus 23(5):352–366. https://doi.org/10.1002/hipo.22095
Wilson DI, Watanabe S, Milner H, Ainge JA (2013b) Lateral entorhinal cortex is necessary for associative but not nonassociative recognition memory. Hippocampus 23(12):1280–1290. https://doi.org/10.1002/hipo.22165
Wood JG, Mirra SS, Pollock NJ, Binder LI (1986) Neurofibrillary tangles of Alzheimer disease share antigenic determinants with the axonal microtubule-associated protein tau (tau). Proc Natl Acad Sci U S A 83(11):4040–4043. https://doi.org/10.1073/pnas.83.11.4040
Wu JW, Hussaini SA, Bastille IM, Rodriguez GA, Mrejeru A, Rilett K, … Duff KE (2016) Neuronal activity enhances tau propagation and tau pathology in vivo. Nat Neurosci 19(8):1085–1092. https://doi.org/10.1038/nn.4328
Xia X, Jiang Q, McDermott J, Han JDJ (2018) Aging and Alzheimer’s disease: comparison and associations from molecular to system level. Aging Cell 17(5):e12802
Yamada K, Iwatsubo T (2018) Extracellular α-synuclein levels are regulated by neuronal activity. Mol Neurodegener 13(1):1–8
Yamada K, Cirrito JR, Stewart FR, Jiang H, Finn MB, Holmes BB, … Holtzman DM (2011) In vivo microdialysis reveals age-dependent decrease of brain interstitial fluid tau levels in P301S human tau transgenic mice. J Neurosci 31(37):13110–13117. https://doi.org/10.1523/jneurosci.2569-11.2011
Yamada K, Holth JK, Liao F, Stewart FR, Mahan TE, Jiang H, … Holtzman DM (2014) Neuronal activity regulates extracellular tau in vivo. J Exp Med 211(3):387–393. https://doi.org/10.1084/jem.20131685
Yassa MA, Lacy JW, Stark SM, Albert MS, Gallagher M, Stark CE (2011) Pattern separation deficits associated with increased hippocampal CA3 and dentate gyrus activity in nondemented older adults. Hippocampus 21(9):968–979. https://doi.org/10.1002/hipo.20808
Yeung LK, Olsen RK, Bild-Enkin HEP, D’Angelo MC, Kacollja A, McQuiggan DA, … Barense MD (2017) Anterolateral entorhinal cortex volume predicted by altered intra-item configural processing. J Neurosci 37(22):5527–5538. https://doi.org/10.1523/jneurosci.3664-16.2017
Zoia C, Cogliati T, Tagliabue E, Cavaletti G, Sala G, Galimberti G, … Ferrarese C (2004) Glutamate transporters in platelets: EAAT1 decrease in aging and in Alzheimer’s disease. Neurobiol Aging 25(2):149–157. https://doi.org/10.1016/s0197-4580(03)00085-x
Author information
Authors and Affiliations
Contributions
Sharay E. Setti performed the literature search and drafted the review. Miranda N. Reed critically revised the content of the review article.
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflict of interest.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Setti, S.E., Reed, M.N. Network activity changes in the pathophysiology of Alzheimer’s disease: the role of aging and early entorhinal cortex dysfunction. Metab Brain Dis 37, 289–298 (2022). https://doi.org/10.1007/s11011-021-00848-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11011-021-00848-8