
Abstract
Adolescent sleep research has focused heavily on duration and quality with less work examining chronotype, defined as individual differences in sleep–wake timings driven by the circadian rhythm. This study filled a gap in the literature by utilizing actigraphy-based sleep estimates in an accelerated longitudinal design in order to better understand the developmental trajectory and individual stability of chronotype during adolescence, as well as the associations between chronotype with risky behaviors, substance use, and depressive symptoms. A total of 329 adolescents (57% female; 21% Asian American, 31% European American, 41% Latino, 7% other ethnicity) provided actigraphy-based estimates of sleep and completed questionnaires at up to three time points, two years apart, beginning at 14–17 years of age. Multilevel modeling revealed a non-linear developmental trend in chronotype whereby eveningness increased from 14 to 19 years of age followed by a trend toward morningness. Individual differences in chronotype exhibited modest stability during adolescent development. Furthermore, greater evening chronotype was associated with more risky behaviors and substance use among males, and more substance use among older adolescents, whereas depressive symptoms were not associated with chronotype. The findings from this study may have practical implications for adolescent behavioral health interventions targeted at reducing risky behaviors and substance use among youth.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Whereas much of the growing research on adolescent sleep has focused heavily on duration and quality, less attention has been given to chronotype, an influential characteristic of human sleep–wake activity (Buysse, 2014). Circadian rhythms are known to regulate various bodily functions including sleep and wake timings (Takahashi et al., 2018), and individual variations result in morning chronotypes who engage in early bed and wake times and evening chronotypes whose nightly sleep begins and ends later (Roenneberg et al., 2003). Prior studies have suggested a general shift toward eveningness during adolescence, but there have been few longitudinal studies to support such developmental trends or to allow for the estimation of the stability of individual differences in chronotype. Additionally, most previous studies have utilized self-reports of preferring morning or evening activities and sleep timings whereas few have estimated chronotype from objectively-assessed actual sleep behaviors. The current study utilized actigraphy-based sleep estimates in an accelerated longitudinal design in order to better understand the developmental trajectory and individual stability of chronotype during adolescence. Actigraphy also allowed for an examination of whether previously-observed associations between self-reported chronotype and risk-taking, substance use, and depressive symptoms were supported by the use of a more objective measure of sleep. Finally, the current study examined potential age and sex variations in the association of chronotype with adjustment due to the differential base rates in behavioral and mental health difficulties according to these factors.
Chronotype Changes and Stability during Adolescence
Prior cross-sectional research demonstrates that most individuals evidence greater morningness (i.e., morning chronotype) during childhood, shift toward eveningness (i.e., evening chronotype) during adolescence, and slowly revert back toward morningness starting in the late teens and early 20s through adulthood (Fischer et al., 2017). Both biological maturation, such as puberty and brain development, and changes in social and structural constraints such as school, work, and family schedules, are thought to drive these developmental changes (Hagenauer & Lee, 2012).
Interestingly, surprisingly few longitudinal assessments have confirmed these developmental trends and most studies have relied upon self-reports of preferences for evening or morning activities (e.g., studying, socializing) and sleep times (e.g., Duarte et al., 2014; Fisher et al., 2017; Randler, 2011; Roenneberg et al., 2004). The only exception was a recent study of approximately 100 adolescents who wore wrist actigraphs, well-validated devices that estimate sleep timing from movement (Sadeh et al., 1994), that observed greater eveningness from 8 to 17 years of age (Kuula et al., 2018). The current study combined an accelerated longitudinal design with the use of wrist actigraphs to estimate changes in chronotype from 14 to 22 years of age. Bed and wake time estimates from the actigraphs on days with relatively unconstrained wake times (e.g., weekends) can be used to estimate chronotype from the midsleep point (MSP), the halfway point between an individual’s bed and wake time, after correcting for any accumulated sleep debt on previous days (Roenneberg et al., 2004). An earlier MSP is indicative of greater “morningness” (i.e., earlier bed and wake times) while a later MSP is indicative of greater “eveningness” (i.e., later bed and wake times). MSP correlates well with commonly-used chronotype preference questionnaires, but it has the unique value of being an estimate of chronotype from actual sleep behavior rather than idealized sleep schedules and activity preferences (Santisteban et al., 2018).
In addition to providing more empirical support for overall developmental trends, longitudinal objective estimates of chronotype would provide insight into the degree and timing of group differences during the adolescent years. It has been suggested that due to earlier pubertal timing, females begin the shift toward eveningness earlier than males, but males may catch up and show greater eveningness in the later years of adolescence (Hagenauer & Lee, 2012). Additionally, there have been virtually no studies of ethnic differences in chronotype during adolescence. Reports of group differences in sleep as well as bed and wake times among adolescents suggest that some ethnic groups, such as Asian Americans, may evidence greater eveningness at an earlier age than other groups potentially due to study time or family activities (Adam et al., 2007; Fuligni & Hardway, 2006), but the existing evidence base is fairly thin. As such, both sex and ethnic differences in the levels and changes in chronotype during adolescence were examined in the current study.
Longitudinal data allow for the assessment of actual developmental change in chronotype as well as the ability to estimate the stability of individual differences in chronotype. An assumption of stability of chronotype comes from genetics research that has shown links between chronotype and the CLOCK and PERIOD genes as well as other genetic variants (Kalmbach et al., 2017; Merikanto et al., 2018). However, few studies have utilized longitudinal data to examine the actual stability of individual differences in chronotype across time during adolescence, and recent formulations of chronotype have suggested that changing situational constraints across age may produce only modest stability (Roenneberg et al., 2019). One study reported that chronotype as estimated by the MSP of self-reported sleep and wake times was correlated at 0.45 across a one-year period during high school (Bai et al., 2020). An additional study of individuals aged 18–56 that revealed moderate stability (r = 0.56) across a seven-year period of time (Druiven et al., 2020), although this study did not include adolescents and used self-reports of preferred activities and sleep times. The current study utilized actigraphy-based estimates of actual sleep to determine the amount of stability in individual differences in chronotype during the adolescent years. Given the potential association of chronotype with aspects of adjustment, the degree of stability versus change in individual differences could inform potential interventions to improve mental and behavioral health through sleep routines (Harvey et al., 2018).
Chronotype and Adjustment during Adolescence
A large body of research has documented associations between chronotype and indicators of behavioral and mental health among adults, with greater eveningness generally being associated with higher levels of risky behavior, substance use, and internalizing problems (Au & Reece, 2017; Taylor & Hasler, 2018). Those with more evening chronotypes have circadian rhythms that are out of synch with the early morning expectations of school, work, and family life, a concept termed as social jet-lag (Wittmann et al., 2006). This discordance could create difficulties with emotion and mood regulation that leads to greater internalizing problems and a tendency to self-medicate with greater substance use. Additionally, being awake at later hours is seen as providing more opportunity to engage in risk-taking and substance use in late-night social settings (Staff et al., 2010).
Much less work has examined the association between chronotype and adjustment during the teenage years, and as noted earlier, research has been limited by the almost exclusive use of self-report measures of morning and evening preferences. Obtaining a more definitive understanding of the potential role of chronotype in relation to other aspects of sleep such as duration and quality is important given that the teenage years is a period of increased risk for behavioral and mental health problems for some youth (Paus et al., 2008). Additionally, the possibility that eveningness presents greater risk for different sexes and ages who have differential rates of risky behavior, substance use, and internalizing problems should be explored.
Chronotype may be particularly consequential for risky behavior and substance use during the adolescent years. One of the hallmarks of adolescence is an increased tendency to engage in risky behaviors as youth explore their environment and novel situations (e.g., Duell et al., 2018). The tendency to do so may be greater among those with more evening chronotypes because of the ease of engaging in such behaviors in the evening hours away from adult supervision, particularly on nights before unscheduled days when they can sleep later (Díaz-Morales et al., 2014). Indeed, a number of studies using self-report measures of chronotype have documented a link between eveningness and a tendency toward impulsivity and poor emotion regulation abilities (Taylor & Hasler, 2018). The similar findings for a variety behaviors, including substance use, suggest that the association may have more to do with a general tendency toward riskiness or thrill-seeking among more evening chronotypes.
Adolescents’ chronotype also may play a role in their experiences with depressive symptoms, which like risky behavior and substance use, also rise during the teenage years for some youth (Clayborne et al., 2019). Many adolescents experience sleep problems during high school through the transition to young adulthood (Park et al., 2019), and multiple indicators of poor sleep (e.g., shorter duration, poorer quality, and greater variability) have been associated with increased reports of depressive symptoms (Lemola et al., 2015; Raniti et al., 2017). As such, there has been some interest in whether a more evening chronotype is also a risk factor for internalizing problems, but findings have been inconsistent. Cross-sectional results based upon self-report measures of preference for morning and evening activities suggest that eveningness is associated with more depressive symptoms among adolescents (Haraden et al., 2017), but other studies using MSP derived from self-reported bed and wake times have not found a link with depressive and other internalizing symptoms (Bai et al., 2020).
The emerging research base of the role of chronotype in adolescent adjustment would benefit from several additions. First, understanding the role of chronotype in adolescent adjustment requires the use of more objective assessments of eveningness in order to avoid the shared method variance evident in much of the previous research in which participants self-reported both their morning and evening preferences and their behavioral and mental health. Second, studies should take into consideration the differential rates by which youths of different ages and sexes evidence behavioral and psychological difficulties. Specifically, it would be important to test whether the association of chronotype with risky behavior and substance use is greater for older and male youths who are more likely to engage in such behaviors (Duell et al., 2018). Similarly, greater eveningness may be linked with depressive symptoms more strongly for older and female adolescents who experience higher levels of internalizing problems (Alloy et al., 2016). Finally, estimates of the association between chronotype and adjustment should take into account the potential role of other sleep parameters known to predict behavioral and mental health. Sleep duration and quality are consistently associated with risky behavior, substance use, and depressive symptoms. Including such measures would allow provide key information as to whether efforts to improve sleep during adolescence should pay attention to chronotype along with sleep duration and quality.
Current Study
Prior research on chronotype development has left a gap by focusing primarily on self-report preference scales of sleep–wake timing. Using an accelerated longitudinal design and objective estimates of sleep behavior, this study examined the developmental trajectory and individual stability of chronotype, as well as its association with risky behavior, substance use, and depressive symptoms as a function of age and sex. The first aim of this study was to assess whether chronotype differed as a function of age during adolescence. In light of previous research, it was hypothesized that there would be intraindividual shifts in chronotype toward eveningness as adolescents aged, with eveningness peaking around 19–20 years of age followed by a shift toward morningness. The second aim was to assess the rank order stability of individual differences in chronotype during this developmental transition. It was hypothesized that individual differences in chronotype would be moderately stable such that those with an evening chronotype at wave 1 would be more likely to evince an evening chronotype at the follow-up waves. The final aim was to evaluate whether chronotype is associated with substance use, risky behaviors, and depressive symptoms as a function of age and sex. It was hypothesized that evening chronotype would be associated with greater risky behavior and substance use, particularly among older adolescents and males, whereas as the association with depressive symptoms would be stronger for older youth and females. The associations between chronotype and adjustment were expected to exist over and above the impact of sleep duration and quality.
Methods
Participants
A total of 350 10th and 11th grade high school students were recruited to participate in a three-wave accelerated longitudinal study, each wave occurring at 2-year intervals, that took place from 2011 to 2016. Of this total, 329 participants had sufficient actigraphy-based sleep data to compute chronotype during at least one of the three waves. Those with only one wave of sleep data were included in the analyses of age trends and associations with adjustment, but not in estimates of the stability of individual differences.
The 329 (57% female) ethnically-diverse (21% Asian American, 31% European American, 41% Latino, 7% other ethnicity) adolescents were recruited from four public high schools in the Los Angeles metropolitan area. Participants’ primary caregivers reported education levels for themselves and for their spouse (1 = some elementary school; 2 = completed elementary school; 3 = some junior high school; 4 = completed junior high school; 5 = some high school; 6 = graduated from high school; 7 = trade or vocational school; 8 = some college; 9 = graduated from college; 10 = some medical, law, or graduate school; 11 = graduated from medical, law, or graduate school). Averaging across both caregivers’ level of education suggested that caregivers averaged slightly above trade or vocational school (M = 7.29, SD = 1.85).
At wave 1, 282 of 316 participants had sufficient sleep data (i.e., at least one full night of sleep onset and offset time) to compute chronotype. At wave 2, 214 of the original 316 participants returned the study sample was replenished by recruiting 34 additional participants who were matched for age. A total of 194 participants had sufficient data to compute chronotype at the second wave. At wave 3, 180 adolescents who participated in one or both of the first two waves returned, and 135 had sufficient data to compute chronotype. Across the 3 waves, 138 participants contributed one estimate of chronotype (41.9%), 100 participants contributed two estimates of chronotype (30.4%), and 91 participants contributed all three estimates of chronotype (27.7%).
Papers previously published from this dataset have examined developmental changes in sleep duration (Park et al., 2019) as well as the links of sleep with inflammation (Park et al., 2016), HPA-axis functioning (Chiang et al., 2016), discrimination (Huynh et al., 2016), mood (Chiang et al., 2017), and family stress (Tsai et al., 2018) in high school. No published papers have examined chronotype.
Procedure
During a home visit at each wave, participants completed questionnaires tapping various psychological and health outcomes and were instructed on how to wear an actigraph watch while a primary caregiver participated in an interview in which they provided demographic information. Adolescent participants were compensated with $50 at wave 1, $75 at wave 2, and $120 at wave 3. All procedures were approved by the Institutional Review Board at the University of California, Los Angeles.
Measures
Chronotype
Participants were instructed to wear actigraphs (Micro Motionlogger Sleep Watch, Ambulatory Monitoring, Inc.; Ardsley, NY) on their non-dominant wrist for eight consecutive nights at each wave of data collection; participants provided an average of 6.30 days (SD = 1.53) of actigraphy data across the waves. They were instructed to press the “event marker” button on the actigraph during the following instances: (1) when they turned out the light to go to bed, (2) if they got out of bed in the middle of the night (i.e., to use the restroom), and (3) when they got out of bed in the morning. Actigraphy data was coded and scored using Action4 software (Ambulatory Monitoring Inc.; Ardsley, NY). Sleep onset was defined as the first three minutes of uninterrupted sleep and sleep offset was the last five or more minutes of uninterrupted sleep.
Chronotype was computed by calculating participants’ average midsleep point (i.e., midway time between sleep onset and offset, scaled in hours past midnight) on free days (M = 2.82 days, SD = 1.47) correcting for sleep debt accrued on scheduled days (abbreviated as MSFc, see formula below), (M = 4.24 days, SD = 1.14) (Roenneberg et al., 2004). Free days were defined as non-school days (i.e., summer, school holidays, weekend days) when participants were attending high school, and as weekend days (i.e., Friday, Saturday night) when participants were post-high school. Free days provide a more accurate measure of an individual’s chronotype since individuals typically do not have restricted bed and wake times due to predetermined school or work schedules. The formula is as follows:
MSFC = MSF – 0.5 (SDF – SDavg)
MSF stands for midsleep point on free days and SDF is indicative of sleep duration on free days. SDavg represents average sleep duration across free and scheduled days.
Risky behavior
Risky behavior was measured using 11 items adapted from the Domain-Specific Risk-Taking Scale (DOSPERT) and the Adolescent Risk Taking Scale (Alexander et al., 1990; Weber et al., 2002). Participants rated how frequently they engaged in risky behaviors (e.g., “Stealing or shoplifting from a store;” “Passing off someone else’s work for your own;” “Doing something risky or dangerous on a dare”) on a scale from 1 to 6 (1 = never, 2 = once in my life, 3 = twice in my life, 4 = a few times (3–5), 5 = many times, 6 = frequently/all the time). Responses were averaged to compute a mean score of risky behavior. To distinguish this measure from substance use, items referring to substances (e.g., getting drunk at a party) were removed. The internal consistency of this measure was high at each wave (α range = 0.77–0.81).
Substance use
Lifetime substance use was measured through a modified version of the Youth Risk Behavior Survey (CDC, 2010). Seven items assessed adolescents’ lifetime substance use ranging from alcohol to illicit drugs (e.g., “If you have ever used smoked more than one or two puffs of a cigarette, how old were you when you smoked that much for the first time?”). If participants reported first trying a drug at a certain age, that substance was coded as being used by that adolescent. The number of substances used was summed to determine lifetime substance use at each wave. The internal consistency of this measure was moderate to high at each wave (α range = 0.60–0.73).
Depressive symptoms
Depressive symptoms were assessed by the Center for Epidemiologic Studies Depression Scale (CES-D) (Andresen et al., 1994; Radloff, 1991). The scale contains 20 items (e.g., “I felt lonely”) and participants were asked to rate each item on a scale from 0 to 3 (0 = rarely or none of the time, 1 = some or little of the time, 2 = moderately or much of the time, 3 = most or almost all the time) accounting for the past month. In order to avoid a confound between chronotype and the measure of depressive symptoms, one item (i.e., “My sleep was restless”) was removed, thus an average was taken of the remaining 19 items. The internal consistency of the CES-D was high at each wave (α range = 0.90–0.91).
Sleep duration
Actigraphy data were used to compute sleep duration by subtracting sleep onset time from sleep offset time.
Sleep quality
Sleep quality was measured using the Pittsburgh Sleep Quality Index (Buysse et al., 1989). Youth completed 19 items regarding their sleep over the past month. Following traditional and well-validated scoring methods, global scores of sleep quality were computed from the seven component scores. Participants received a score ranging from 0 to 21, wherein higher scores indicated worse sleep quality. The internal consistency of the PSQI was moderate to high at each wave (α range = 0.68–0.75).
Analytic Strategy
Descriptive statistics by age are presented in Table 1. Bivariate correlations and intraclass correlation coefficients (ICCs) were computed to estimate the within-person stability of chronotype. Multilevel growth curve models, with waves nested within individuals, were estimated to examine the association between age and chronotype, controlling for sex, ethnicity, and parental education. Age and parent education were grand-mean centered while sex (Male = 0) and ethnicity (European American = 0) were dummy-coded. Linear, quadratic, and cubic age trends were estimated given the hypothesized quadratic trend in the development of chronotype.
Multilevel modeling was also employed to estimate concurrent associations of chronotype with risky behaviors, substance use, and depressive symptoms, controlling for age, sex, ethnicity, and parent education. Initial models estimated the main effect of chronotype on the outcomes of interest, with subsequent models examining the interaction of chronotype with age and sex. Chronotype was included as a random slope in all models. Analyses were run on STATA 15.1 (College Station, TX). Given previously established links between sleep and the outcomes of interest, sleep duration and sleep quality were entered as additional control variables in the models.
Results
Participation Analyses
Some participants began at wave 2 and some wave 1 participants missed wave 2 but returned at wave 3, therefore participation and attrition rates were estimated by computing the percent of possible waves in which youth could have participated over the course of the study. On average, youth participated in 60% (SD = 31%) of their possible waves (i.e., three possible waves for those who started at wave 1 and two possible waves for those who started at wave 2). Participation rates varied by ethnicity (F(3, 325) = 3.66, p = 0.013) such that Asian Americans participated in fewer waves than the other three ethnic groups. Rate of participation did not differ by sex (t(322) = −1.67, p = 0.095) nor parental education (r = 0.07, p = 0.230). Chronotype was not associated with participation rate (b = 0.49, SE = 0.21, p = 0.211) when controlling for age and sex. Similarly, neither risky behaviors (b = −0.21, SE = 0.17, p = 0.320), substance use (b = −0.15, SE = 0.34, p = 0.668), nor depressive symptoms (b = 0.00, SE = 0.12, p = 0.989) were associated with participation rate when controlling for age and sex. Sleep quality was not associated with participation rate (b = −0.15, SE = 0.34, p = 0.668), but more sleep duration was associated with greater participation (b = 0.73, SE = 0.25, p = 0.003) when controlling for age and sex.
Age Differences in Chronotype
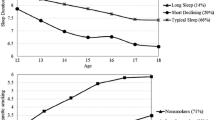
The multilevel growth curve model revealed a significant cubic trend (b = −0.04, SE = 0.01, p < 0.001) of age (Table 2) whereby chronotype shifted toward eveningness across adolescence until approximately 19 years of age, after which it shifted back toward morningness (Fig. 1). Chronotype became later by 1 h and 54 min between ages 14 and 19. Additionally, a significant ethnic difference emerged indicating that Asian American adolescents had a 28 minute later chronotype compared to their European American peers (b = 0.48, SE = 0.19, p = 0.010) at the mean-centered age of the sample (i.e., 17 years, 11 months) (Table 2).

Chronotype by age
Stability of Individual Differences in Chronotype
Analyses yielded small to medium-sized correlations between the chronotype (MSFc) estimates across the three waves suggesting a modest degree of stability in chronotype within individuals across the two and four-year intervals. The correlation value between waves 1 and 2 was r = 0.19 (p = 0.018), r = 0.35 (p < 0.001) between waves 2 and 3, and r = 0.30 (p = 0.002) between waves 1 and 3. The ICC, derived from the multilevel growth curve model, was 0.23 which suggests that 23% of the variance in MSFc was due to between-person differences.
Risky Behaviors, Substance Use, and Depressive Symptoms
Initial main effect multilevel models did not indicate direct associations between chronotype and the outcome variables of interest: risky behaviors, substance use, and depressive symptoms (see Table 3). However, subsequent models examining moderations by age and sex revealed a significant chronotype × sex interaction in predicting risky behavior whereby an evening chronotype was associated with more risky behavior among males but not females (Fig. 2a). Furthermore, a significant chronotype × sex interaction was also observed for substance use. Males with more of an evening chronotype reported more substance use but the same was not found for females (Fig. 2b). Additionally, older adolescents with more of an evening chronotype reported more substance use compared to younger and mid-aged adolescents (Fig. 3). Follow-up sensitivity analyses suggested that the chronotype × sex interactions predicting risky behaviors and substance use maintained statistical significance after controlling for sleep duration and quality, but the chronotype × age interaction was reduced to become non-significant due to a slightly inflated standard error from introducing additional covariates into the model as opposed to a reduced coefficient (Table 4).

a Risky behavior by chronotype and sex. b Substance use by chronotype and sex

Substance use by chronotype and age. Simple slopes were derived at centered age (17.95 years) and 1 SD above (19.68 years) and below (16.22) the mean
Discussion
Prior research demonstrates that chronotype, individual differences in bed and wake times determined by the circadian rhythm, shows developmental shifts throughout the life course with a notable delay toward evening chronotype (i.e., late bed and wake times) during adolescence contrasted with greater morning chronotype (i.e., early bed and wake times) during childhood and adulthood. The majority of this work, however, has utilized cross-sectional, self-report surveys to estimate developmental change. In addition, little work has examined the rank order stability of individual differences in chronotype. Lastly, although prior research suggests that evening chronotype adolescents evince poorer adjustment, less is known about how age and sex may moderate the link between chronotype with substance use, risky behaviors, and depressive symptoms. This study used actigraphy-based sleep measurement in an accelerated longitudinal design to provide several insights into the developmental patterns and behavioral implications of chronotype during the transition from adolescence to young adulthood.
First, results showed that chronotype developed in a non-linear pattern with increased eveningness from 14 to 19 years of age followed by a shift back toward morningness in young adulthood. Second, chronotype exhibited only modest stability in individual differences across this development phase, suggesting a potential malleability that may be responsive to intervention efforts. Finally, chronotype was differentially associated with risky behavior and substance use as a function of sex and age, but was not associated with depressive symptoms.
Consistent with prior cross-sectional data (Duarte et al., 2014; Fisher et al., 2017; Kuula et al., 2018; Randler, 2011; Roenneberg et al., 2004) and what the current study hypothesized, the results indicated that chronotype shifted toward eveningness until approximately 19 years of age and then shifted back toward morningness. The evening shift in adolescence is consistent with maturational accounts of later chronotype after puberty (Tarokh et al., 2019), and the move back toward morningness in the twenties could be due to increased responsibilities and work schedules typical in adulthood as well as the reduction in social jetlag (Paine et al., 2006; Roenneberg et al., 2019). Although not a part of the a priori hypotheses, results also showed that Asian American adolescents may have a later chronotype at an earlier age as compared to their European American peers. This finding is supported by prior research showing that Asian American adolescents experience poorer sleep compared to their Asian international counterparts (Karan & Park, 2020) possibly because of greater time spent studying in the evenings (Fuligni & Hardway, 2006). Given that there is limited research assessing ethnic differences in chronotype, future work should seek to replicate this finding and uncover how ethnic differences manifest in sleep timing preferences.
The modest stability of individual differences in chronotype during the transition from adolescence to young adulthood suggests a degree of malleability, despite existing research on the genetic underpinnings of sleep-timing (Kalmbach et al., 2017; Merikanto et al., 2018). Previous findings suggested more within-person stability in chronotype based on self-report measures of preference (Kuula et al., 2018). The use of an objective measure of sleep in this study, as well as the developmental period of transition, could have resulted in more variability in chronotype across time. Furthermore, the day of obtaining data may have contributed to the modest within-person stability since school days preclude the body’s natural rhythm due to set schedules and weekends typically allow for natural sleep with less scheduled activities. Additional studies of actual sleep behaviors across more days over a longer period of time should be conducted in order to obtain a fuller understanding of the individual stability of chronotype in everyday life. Clearer results may be obtained from studies examining the stability of chronotype among twins using actigraphy. Nevertheless, this finding is consistent with recent re-conceptualizations of chronotype as more of a state than a trait due to the powerful influence of environmental cues (i.e., zeitgebers) and other situational factors influencing on sleep-timing and the circadian rhythm (Roenneberg et al., 2019).
In terms of mental health, results suggested that a later chronotype may be associated more with externalizing-type behaviors, such as risk-taking and substance use, than with internalizing behaviors, such as depressive symptoms, and more so for males and older youth. The links with risk-taking and substance use should not be surprising, given previous findings (Hasler et al., 2017; Haynie et al., 2018) and the probability that these behaviors are more likely to occur during the evening hours when parental supervision is reduced (Randler et al., 2009; Staff et al., 2010). A more evening chronotype, therefore, provides greater opportunity to engage in such behaviors, however, more research is needed to clarify the directionality of the association. Finally, although studies have observed a link between evening chronotype and heightened depressive symptoms among adolescents, they have predominantly employed self-report scales of circadian preference thus associations with internalizing symptoms could be a result of common method-variance and reporter bias (Alvaro et al., 2014; Chiu et al., 2017; Haraden et al., 2017; Pabst et al., 2009). This may explain why the current study did not see a link between depressive symptoms and chronotype as hypothesized.
Few previous studies have tested for such differential associations according to sex, but the present findings are consistent with those from a study that found that adult males with an evening chronotype engaged in more risky decisions compared to females (Wang & Chartrand, 2015). To our knowledge, no other studies have examined variations in the association of chronotype with substance use by age in adolescence thus future work would need to replicate the finding of a link between eveningness and substance use among older youth. Taken together, the moderations observed in this study suggest that chronotype may be more predictive of risky behavior and substance use among subgroups of youth who are already more likely to engage in higher levels of these behaviors, such as males and older youth (Choi et al., 2018; Duell et al., 2018).
The results from this investigation should be considered in conjunction with study limitations and future directions. Although weekend days and holidays were used to compute MSFc, the current study lacked data on activities that may have influenced participant bed and wake times on free days. Future research should ensure that MSFc is computed using days on which subjects’ bed and wake times are free from all scheduled activities. Extracurricular activities such as volunteering and sports may artificially induce early wake times among adolescents, therefore ensuing research should collect information on weekend activities that may influence MSFc computations. Attrition was another limitation; however, attrition did not differ according to the key constructs of the study and multilevel modeling was used with maximum likelihood estimations that account for missing data. Work examining age-related changes and individual stability in chronotype among younger developmental age groups, such as children along with adolescents, would help fill remaining gaps in the literature. Furthermore, although the current study did not find an association between depressive symptoms and chronotype, prior research demonstrates an association; however, future research examining chronotype and depression among adolescents should seek to measure chronotype using an objective indictor such as MSP and a self-report measure to assess the role of common method-variance and report bias in the link between chronotype and depression. Additionally, research should focus on investigating the mediating processes through which chronotype might influence risky behaviors, substance use, and depressive symptoms to further shed light on promising intervention efforts to improve these behaviors through chronotype.
The present study’s findings have important implications for behavioral health interventions that aim to prevent substance use and reduce other risky behaviors in adolescence, however, it is important to note that the current study cannot make directional claims about chronotype and risk-taking during adolescence with the current data. Nonetheless, many interventions focus on sleep duration or disturbance (Blake et al., 2019), but the current study found that chronotype is associated with risky behaviors over and above sleep duration. Moreover, when measured objectively, chronotype was only modestly stable across time. Therefore, chronotype could be a key component of sleep health assessments, which should be developmentally-informed and interpreted in the context of an individual’s biological maturation. More importantly, chronotype may be a malleable target of intervention (Harvey et al., 2018) that when changed, could reduce adolescent risk-taking behaviors. Additionally, the consistent links between chronotype and substance use, over and above sleep duration, indicate that a later chronotype is implicated in the risk for substance use. As such, interventions that target sleep to reduce substance use (e.g., Britton et al., 2010; Conroy & Arnedt, 2014) may be improved with a specific focus on chronotype in addition to sleep duration and quality.
Conclusion
Prior studies have demonstrated a development toward eveningness during adolescence, but there have been few longitudinal studies to support such developmental trends or to allow for the estimation of the stability of individual differences in chronotype. Additionally, most previous studies have administered self-reports of preferring morning or evening activities and sleep timing and relatively few have computed chronotype from objectively-assessed sleep. The current study makes important contributions to the adolescent sleep literature by utilizing an objective measure of chronotype to examine developmental trends and individual stability in adolescence and young adulthood. Furthermore, associations between chronotype and risky behaviors, substance use, and depressive symptoms were assessed with respect to age and sex differences, expanding upon prior studies that have found associations between chronotype and these outcomes. Results supported prior studies of self-reported chronotype and age by demonstrating a non-linear trend of chronotype by age wherein adolescents demonstrate more eveningness followed by a shift toward morningness in young adulthood. Chronotype was modestly stable among individuals during this developmental period. Furthermore, greater evening chronotype was associated with more risky behaviors and substance use among males, and more substance use among older adolescents, whereas depressive symptoms were not associated with chronotype. Findings were maintained when controlling for sleep duration and sleep quality, suggesting a unique role of chronotype in risk-taking among adolescents. Taken together, chronotype is a malleable construct that is associated with adolescent adjustment and it should be further studied to leverage as a meaningful agent of intervention.
References
Adam, E. K., Snell, E. K., & Pendry, P. (2007). Sleep timing and quantity in ecological and family context: a nationally representative time-diary study. Journal of Family Psychology, 21(1), 4 https://doi.org/10.1037/0893-3200.21.1.4.
Alexander, C. S., Kim, Y. J., Ensminger, M., Johnson, K. E., Smith, B. J., & Dolan, L. J. (1990). A measure of risk taking for young adolescents: Reliability and validity assessments. Journal of Youth and Adolescence, 19(6), 559–569. https://doi.org/10.1007/BF01537176.
Alloy, L. B., Hamilton, J. L., Hamlat, E. J., & Abramson, L. Y. (2016). Pubertal development, emotion regulatory styles, and the emergence of sex differences in internalizing disorders and symptoms in adolescence. Clinical Psychological Science, 4(5), 867–881. https://doi.org/10.1177/2167702616643008.
Alvaro, P. K., Roberts, R. M., & Harris, J. K. (2014). The independent relationships between insomnia, depression, subtypes of anxiety, and chronotype during adolescence. Sleep Medicine, 15(8), 934–941. https://doi.org/10.1016/j.sleep.2014.03.019.
Andresen, E. M., Malmgren, J. A., Carter, W. B., & Patrick, D. L. (1994). Screening for depression in well older adults: Evaluation of a short form of the CES-D. American Journal of Preventive Medicine, 10(2), 77–84. https://doi.org/10.1016/S0749-3797(18)30622-6.
Au, J., & Reece, J. (2017). The relationship between chronotype and depressive symptoms: A meta-analysis. Journal of Affective Disorders, 218, 93–104. https://doi.org/10.1016/j.jad.2017.04.021.
Bai, S., Karan, M., Gonzales, N. A., & Fuligni, A. J. (2020). A daily diary study of sleep chronotype among Mexican-origin adolescents and parents: Implications for adolescent behavioral health. Development and Psychopathology, 1, 10. https://doi.org/10.1017/S0954579419001780.
Blake, M. J., Latham, M. D., Blake, L. M., & Allen, N. B. (2019). Adolescent-sleep-intervention research: Current state and future directions. Current Directions in Psychological Science, 28(5), 475–482. https://doi.org/10.1177/0963721419850169.
Britton, W. B., Bootzin, R. R., Cousins, J. C., Hasler, B. P., Peck, T., & Shapiro, S. L. (2010). The contribution of mindfulness practice to a multicomponent behavioral sleep intervention following substance abuse treatment in adolescents: A treatment-development study. Substance Abuse, 31(2), 86–97. https://doi.org/10.1080/08897071003641297.
Buysse, D. J. (2014). Sleep health: Can we define it? Does it matter? Sleep, 37(1), 9–17. https://doi.org/10.5665/sleep.3298.
Buysse, D. J., Reynolds, III, C. F., Monk, T. H., Berman, S. R., & Kupfer, D. J. (1989). The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Research, 28(2), 193–213. https://doi.org/10.1016/0165-1781(89)90047-4.
Centers for Disease Control and Prevention. 2010 Youth Risk Behavior Survey Questionnaire. Available at: www.cdc.gov/yrbs.
Chiang, J. J., Kim, J. J., Almeida, D. M., Bower, J. E., Dahl, R. E., Irwin, M. R., & Fuligni, A. J. (2017). Sleep efficiency modulates associations between family stress and adolescent depressive symptoms and negative affect. Journal of Adolescent Health, 61(4), 501–507. https://doi.org/10.1016/j.jadohealth.2017.04.011.
Chiang, J. J., Tsai, K. M., Park, H., Bower, J. E., Almeida, D. M., Dahl, R. E., & Fuligni, A. J. (2016). Daily family stress and HPA axis functioning during adolescence: The moderating role of sleep. Psychoneuroendocrinology, 71, 43–53. https://doi.org/10.1016/j.psyneuen.2016.05.009.
Chiu, W. H., Yang, H. J., & Kuo, P. H. (2017). Chronotype preference matters for depression in youth. Chronobiology International, 34(7), 933–941. https://doi.org/10.1080/07420528.2017.1327441.
Choi, H. J., Lu, Y., Schulte, M., & Temple, J. R. (2018). Adolescent substance use: Latent class and transition analysis. Addictive Behaviors, 77, 160–165. https://doi.org/10.1016/j.addbeh.2017.09.022.
Clayborne, Z. M., Varin, M., & Colman, I. (2019). Systematic review and meta-analysis: Adolescent depression and long-term psychosocial outcomes. Journal of the American Academy of Child & Adolescent Psychiatry, 58(1), 72–79. https://doi.org/10.1016/j.jaac.2018.07.896.
Conroy, D. A., & Arnedt, J. T. (2014). Sleep and substance use disorders: An update. Current Psychiatry Reports, 16(10), 487 https://doi.org/10.1016/j.psyneuen.2016.05.009.
Díaz-Morales, J. F., Escribano, C., Jankowski, K. S., Vollmer, C., & Randler, C. (2014). Evening adolescents: The role of family relationships and pubertal development. Journal of Adolescence, 37(4), 425–432. https://doi.org/10.1016/j.adolescence.2014.03.001.
Druiven, S. J., Hovenkamp‐Hermelink, J. H., Knapen, S. E., Kamphuis, J., Haarman, B. C., Penninx, B. W., & Riese, H. (2020). Stability of chronotype over a 7‐year follow‐up period and its association with severity of depressive and anxiety symptoms. Depression and Anxiety, 37(5), 466–474. https://doi.org/10.1002/da.22995.
Duarte, L. L., Menna-Barreto, L., Miguel, M. A. L., Louzada, F., Araújo, J., Alam, M., & Pedrazzoli, M. (2014). Chronotype ontogeny related to gender. Brazilian Journal of Medical and Biological Research, 47(4), 316–320. https://doi.org/10.1590/1414-431X20143001.
Duell, N., Steinberg, L., Icenogle, G., Chein, J., Chaudhary, N., Di Giunta, L., & Pastorelli, C. (2018). Age patterns in risk taking across the world. Journal of Youth and Adolescence, 47(5), 1052–1072. https://doi.org/10.1007/s10964-017-0752-y.
Fischer, D., Lombardi, D. A., Marucci-Wellman, H., & Roenneberg, T. (2017). Chronotypes in the US–influence of age and sex. PLoS One, 12(6), e0178782 https://doi.org/10.1371/journal.pone.0178782.
Fuligni, A. J., & Hardway, C. (2006). Daily variation in adolescents’ sleep, activities, and psychological well‐being. Journal of Research on Adolescence, 16(3), 353–378. https://doi.org/10.1111/j.1532-7795.2006.00498.x.
Hagenauer, M. H., & Lee, T. M. (2012). The neuroendocrine control of the circadian system: Adolescent chronotype. Frontiers in Neuroendocrinology, 33(3), 211–229. https://doi.org/10.1016/j.yfrne.2012.04.003.
Haraden, D. A., Mullin, B. C., & Hankin, B. L. (2017). The relationship between depression and chronotype: A longitudinal assessment during childhood and adolescence. Depression and Anxiety, 34(10), 967–976. https://doi.org/10.1002/da.22682.
Harvey, A. G., Hein, K., Dolsen, M. R., Dong, L., Rabe-Hesketh, S., Gumport, N. B., & Smith, R. L. (2018). Modifying the impact of eveningness chronotype (“Night-Owls”) in youth: A randomized controlled trial. Journal of the American Academy of Child & Adolescent Psychiatry, 57(10), 742–754. https://doi.org/10.1016/j.jaac.2018.04.020.
Hasler, B. P., Casement, M. D., Sitnick, S. L., Shaw, D. S., & Forbes, E. E. (2017). Eveningness among late adolescent males predicts neural reactivity to reward and alcohol dependence 2 years later. Behavioural Brain Research, 327, 112–120. https://doi.org/10.1016/j.bbr.2017.02.024.
Haynie, D. L., Lewin, D., Luk, J. W., Lipsky, L. M., O’Brien, F., Iannotti, R. J., & Simons-Morton, B. G. (2018). Beyond sleep duration: Bidirectional associations among chronotype, social jetlag, and drinking behaviors in a longitudinal sample of US high school students. Sleep, 41(2), 1–14. https://doi.org/10.1093/sleep/zsx202.
Huynh, V. W., Guan, S. S. A., Almeida, D. M., McCreath, H., & Fuligni, A. J. (2016). Everyday discrimination and diurnal cortisol during adolescence. Hormones and Behavior, 80, 76–81. https://doi.org/10.1016/j.yhbeh.2016.01.009.
Kalmbach, D. A., Schneider, L. D., Cheung, J., Bertrand, S. J., Kariharan, T., Pack, A. I., & Gehrman, P. R. (2017). Genetic basis of chronotype in humans: Insights from three landmark GWAS. Sleep, 40(2). https://doi.org/10.1093/sleep/zsw073.
Karan, M., & Park, H. (2020). Sleep quality and cultural orientation among Chinese and Korean undergraduates in the United States. Journal of American College Health, 1-5. https://doi.org/10.1080/07448481.2020.1763368.
Kuula, L., Pesonen, A. K., Merikanto, I., Gradisar, M., Lahti, J., Heinonen, K., & Räikkönen, K. (2018). Development of late circadian preference: Sleep timing from childhood to late adolescence. The Journal of Pediatrics, 194, 182–189. https://doi.org/10.1016/j.jpeds.2017.10.068.
Lemola, S., Perkinson-Gloor, N., Brand, S., Dewald-Kaufmann, J. F., & Grob, A. (2015). Adolescents’ electronic media use at night, sleep disturbance, and depressive symptoms in the smartphone age. Journal of Youth and Adolescence, 44(2), 405–418. https://doi.org/10.1007/s10964-014-0176-x.
Merikanto, I., Lahti, J., Kuula, L., Heinonen, K., Räikkönen, K., Andersson, S., & Pesonen, A. K. (2018). Circadian preference and sleep timing from childhood to adolescence in relation to genetic variants from a genome-wide association study. Sleep Medicine, 50, 36–41. https://doi.org/10.1016/j.sleep.2018.04.015.
Pabst, S. R., Negriff, S., Dorn, L. D., Susman, E. J., & Huang, B. (2009). Depression and anxiety in adolescent females: the impact of sleep preference and body mass index. Journal of Adolescent Health, 44(6), 554–560. https://doi.org/10.1016/j.jadohealth.2008.11.012.
Paine, S. J., Gander, P. H., & Travier, N. (2006). The epidemiology of morningness/eveningness: Influence of age, gender, ethnicity, and socioeconomic factors in adults (30-49 years). Journal of Biological Rhythms, 21(1), 68–76. https://doi.org/10.1177/0748730405283154.
Park, H., Chiang, J. J., Irwin, M. R., Bower, J. E., McCreath, H., & Fuligni, A. J. (2019). Developmental trends in sleep during adolescents’ transition to young adulthood. Sleep Medicine, 60, 202–210. https://doi.org/10.1016/j.sleep.2019.04.007.
Park, H., Tsai, K. M., Dahl, R. E., Irwin, M. R., McCreath, H., Seeman, T. E., & Fuligni, A. J. (2016). Sleep and inflammation during adolescence. Psychosomatic Medicine, 78(6), 677 https://doi.org/10.1097/PSY.0000000000000340.
Paus, T., Keshavan, M., & Giedd, J. N. (2008). Why do many psychiatric disorders emerge during adolescence? Nature Reviews Neuroscience, 9(12), 947–957. https://doi.org/10.1038/nrn2513.
Radloff, L. S. (1991). The use of the Center for Epidemiologic Studies Depression Scale in adolescents and young adults. Journal of Youth and Adolescence, 20(2), 149–166. https://doi.org/10.1007/BF01537606.
Randler, C. (2011). Association between morningness–eveningness and mental and physical health in adolescents. Psychology, Health & Medicine, 16(1), 29–38. https://doi.org/10.1080/13548506.2010.521564.
Randler, C., Bilger, S., & Díaz-Morales, J. F. (2009). Associations among sleep, chronotype, parental monitoring, and pubertal development among German adolescents. The Journal of Psychology, 143(5), 509–520. https://doi.org/10.3200/JRL.143.5.509-520.
Raniti, M. B., Allen, N. B., Schwartz, O., Waloszek, J. M., Byrne, M. L., Woods, M. J., & Trinder, J. (2017). Sleep duration and sleep quality: Associations with depressive symptoms across adolescence. Behavioral Sleep Medicine, 15(3), 198–215. https://doi.org/10.1080/15402002.2015.1120198.
Roenneberg, T., Kuehnle, T., Pramstaller, P. P., Ricken, J., Havel, M., Guth, A., & Merrow, M. (2004). A marker for the end of adolescence. Current Biology, 14(24), R1038–R1039. https://doi.org/10.1016/j.cub.2004.11.039.
Roenneberg, T., Pilz, L. K., Zerbini, G., & Winnebeck, E. C. (2019). Chronotype and social jetlag: A (self-) critical review. Biology, 8(3), 54 https://doi.org/10.3390/biology8030054.
Roenneberg, T., Wirz-Justice, A., & Merrow, M. (2003). Life between clocks: Daily temporal patterns of human chronotypes. Journal of Biological Rhythms, 18(1), 80–90. https://doi.org/10.1177/0748730402239679.
Sadeh, A., Sharkey, M., & Carskadon, M. A. (1994). Activity-based sleep-wake identification: An empirical test of methodological issues. Sleep, 17(3), 201–207. https://doi.org/10.1093/sleep/17.3.201.
Santisteban, J. A., Brown, T. G., & Gruber, R. (2018). Association between the Munich Chronotype Questionnaire and wrist actigraphy. Sleep Disorders, 2018, 1–7. https://doi.org/10.1155/2018/5646848.
Staff, J., Schulenberg, J. E., Maslowsky, J., Bachman, J. G., O’Malley, P. M., Maggs, J. L., & Johnston, L. D. (2010). Substance use changes and social role transitions: Proximal developmental effects on ongoing trajectories from late adolescence through early adulthood. Development and Psychopathology, 22(4), 917 https://doi.org/10.1017/S0954579410000544.
Takahashi, M., Tahara, Y., Tsubosaka, M., Fukazawa, M., Ozaki, M., Iwakami, T., & Shibata, S. (2018). Chronotype and social jetlag influence human circadian clock gene expression. Scientific Reports, 8(1), 1–10. https://doi.org/10.1038/s41598-018-28616-2.
Tarokh, L., Short, M., Crowley, S. J., Fontanellaz-Castiglione, C. E., & Carskadon, M. A. (2019). Sleep and circadian rhythms in adolescence. Current Sleep Medicine Reports, 5(4), 181–192. https://doi.org/10.1007/s40675-019-00155-w.
Taylor, B. J., & Hasler, B. P. (2018). Chronotype and mental health: Recent advances. Current Psychiatry Reports, 20(8), 59 https://doi.org/10.1007/s11920-018-0925-8.
Tsai, K. M., Dahl, R. E., Irwin, M. R., Bower, J. E., McCreath, H., Seeman, T. E., & Fuligni, A. J. (2018). The roles of parental support and family stress in adolescent sleep. Child Development, 89(5), 1577–1588. https://doi.org/10.1111/cdev.12917.
Wang, L., & Chartrand, T. L. (2015). Morningness–eveningness and risk taking. The Journal of Psychology, 149(4), 394–411. https://doi.org/10.1080/00223980.2014.885874.
Weber, E. U., Blais, A. R., & Betz, N. E. (2002). A domain‐specific risk‐attitude scale: Measuring risk perceptions and risk behaviors. Journal of Behavioral Decision Making, 15(4), 263–290. https://doi.org/10.1002/bdm.414.
Wittmann, M., Dinich, J., Merrow, M., & Roenneberg, T. (2006). Social jetlag: Misalignment of biological and social time. Chronobiology International, 23(1-2), 497–509. https://doi.org/10.1080/07420520500545979.
Author information
Authors and Affiliations
Contributions
M. K. developed the study concept, performed analyses, and drafted the manuscript. A. J. F. developed the study concept, collected data, and provided extensive input on analyses and the manuscript. S. B. provided extensive input on analyses and the manuscript. D. M. A. was involved in data collection, provided input on analyses and the manuscript. M. R. I. was involved in data collection, provided input on analyses and the manuscript. H. M. was involved in data collection, provided input on analyses and the manuscript. All authors interpreted the results, and read and approved of the final manuscript.
Funding
This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01-HD062547); the UCLA California Center for Population Research, which was supported by the National Institute of Child Health and Human Development (R24-HD041022); and the UCLA Older Americans Independence Center, which was supported by the National Institute on Aging (P30-AG017265 and P30-AG028748) awarded to A. J. F. Preparation of this manuscript was supported in part by a National Institute of Child Health and Human Development T32 Fellowship awarded to M. K. (5T32HD091059).
Data Sharing and Declaration
This manuscript’s data will not be deposited.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethical Approval
All procedures in this study complied with ethical standards of the University of California, Los Angeles Institutional Review Board (IRB #14-000404)
Informed Consent
Informed consent was obtained from all adult participants and minor participants’ parents, and assent was obtained from all minor participants.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Karan, M., Bai, S., Almeida, D.M. et al. Sleep–Wake Timings in Adolescence: Chronotype Development and Associations with Adjustment. J Youth Adolescence 50, 628–640 (2021). https://doi.org/10.1007/s10964-021-01407-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-021-01407-1