
Abstract
Multilevel research on whether and how contextual socioeconomic disadvantage affects adolescent suicidal behaviors is scarce. Using data from the first two waves (1994/95 and 1996) of the National Longitudinal Study of Adolescent to Adult Health (N = 13,335; 49.63% girls; Mage = 15.02 years), this study examined (1) the association between area-level socioeconomic disadvantage and adolescent suicide attempts over and above individual-level socioeconomic factors, (2) the moderating role of gender, and (3) the mediating roles of contextually relevant stressors and available psychosocial resources. The results revealed that area-level socioeconomic disadvantage increased the risk of attempting suicide even after adjusting for individual-level socioeconomic status, especially for boys. Consistent with the stress process perspective, reports of exposure to violence and lack of safety explain this contextual effect. National suicidal behavior prevention strategies across the U.S. should recognize the strong association with the socioeconomic context, along with individual-level risk factors.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Suicidal behaviors are prevalent among adolescents (Evans et al. 2005), and they represent the most prominent precursors of a completed suicide (Cash and Bridge 2009; Nock et al. 2013). Identifying the risk factors associated with adolescent suicidal behaviors is an important endeavor for developing appropriate intervention and prevention methods. The majority of the previous research in this area focused on individual-level precursors such as psychopathology and familial problems (Bridge et al. 2006; Nock et al. 2008). Conversely, since Durkheim’s (1897/1951) seminal work, social researchers of suicide have emphasized the relevance of more distal risk factors that are not necessarily the attributes of the individuals, but rather of those larger social contexts in which they live such as their neighborhood or community environment (Wray et al. 2011). Interest in contextual risk factors has increased, especially with the development of multilevel modeling techniques that enable researchers to analyze data on multiple levels simultaneously (Maimon et al. 2010; Thorlindsson and Bernburg 2009). Following this trend, researchers have found that area-level measures of residential mobility (Thorlindsson and Bernburg 2009), collective efficacy (Maimon et al. 2010), and religious participation (Maimon and Kuhl 2008) all influenced adolescent suicidality over and above individual-level risk factors.
Despite this growing attention to the context, however, multilevel research on whether area-level socioeconomic disadvantage—the concentration of lower socioeconomic status individuals (Hill and Maimon 2013)—affects adolescent suicidal behaviors over and above individual-level socioeconomic disadvantage has been scarce. There are also considerable gaps in the literature regarding the potential gender differences and underlying mechanisms of the process. Using one of the largest sample of American adolescents, this study investigated the association between area-level socioeconomic status and adolescent suicide attempts by considering the potential moderating role of gender. Moreover, drawing on decades of neighborhood context and stress process literature (Aneshensel 2009), possible mediating roles of contextually relevant stressors and psychosocial resources were assessed.
Area-level Socioeconomic Disadvantage and Adolescent Suicidal Behaviors
It is a well-known phenomenon that individuals from low socioeconomic backgrounds are at increased risk of suicide and suicidal behaviors (Pirkis et al. 2017). Personal income, education level, and employment in adults; and parental education and household income in adolescents are consistently and inversely associated with suicide risk (see Platt 2016 for review). These individual-level socioeconomic factors are certainly important, as they index individuals’ positions in relation to the unequal distribution of money, resources, goods, and quality of life (Mirowsky and Ross 2003); all may affect suicidality via a myriad of pathways (Denney et al. 2009). However, a growing body of research has shown that the socioeconomic characteristics of the contexts in which individuals live (e.g., neighborhood, community) might also influence their risk level. Much of the empirical evidence for this claim comes from European ecological studies examining the relationship between area-level socioeconomic factors such as unemployment and suicide rates (see Cairns et al. 2017 for review). These studies have fairly consistently determined that suicide deaths tend to geographically cluster in places with a higher concentrations of people from lower socioeconomic positions (Exeter and Boyle 2007). A majority of these studies, however, have ignored non-fatal suicidal behaviors, and focused on either adult populations or all age groups together (Rehkopf and Buka 2006). More importantly, these studies were based on area-level data only, and thus were unable to assess whether differences in suicide rates across multiple areas were merely a reflection of the socioeconomic positions of the people residing in those areas (i.e., compositional effect), or if area-level socioeconomic factors actually predicted suicide risk regardless of the contribution of the individual-level socioeconomic elements (i.e., contextual effect).
In order to parse out the effects of individual-level socioeconomic factors, recent research has examined adult suicides, using both area- and individual-level data (Agerbo et al. 2007; Denney et al. 2015; Martikainen et al. 2004). These studies found that suicide risk among adults was indeed influenced by socioeconomic characteristics of the areas (Denney et al. 2015), even though adjusting for individual-level factors partly attenuated the contextual associations (Agerbo et al. 2007). To our knowledge, however, very few studies have used a multilevel framework to investigate whether area-level socioeconomic disadvantage is related to adolescent non-fatal suicidal behaviors, and those that have produced inconsistent findings (Allen and Goldman-Mellor 2017; Dupéré et al. 2009). Dupéré and colleagues’ (2009) study on a representative sample of Canadian adolescents found that area-level poverty was associated with a higher risk of suicidal behaviors, irrespective of socioeconomic status. Conversely, Allen and Goldman-Mellor (2017) found that objective measures of neighborhood characteristics, including neighborhood socioeconomic disadvantage, were no longer significant predictors of California adolescents’ risk of suicidal behaviors after controlling for parental education and income. The reason for these inconsistent findings might be related to their differing samples, methods, and statistical measures; regardless, given the limited amount of research on this topic, additional multilevel work is needed.
Gender Differences
Another gap in the literature that deserves attention is whether the effects of area-level socioeconomic disadvantage differ for boys and girls. Gender plays a significant and complex role in suicide and the suicidal behaviors of adolescents. For instance, while more boys than girls die by suicide, yet girls are more likely to report suicidal thoughts and attempts (McLoughlin et al. 2015). Impacts of some risk and protective factors have also been shown to vary by gender (Donker et al. 2014). Despite these gender differences, however, previous multilevel research has failed to consider the possible differential effect of socioeconomic context on the suicidal behaviors of boys and girls. Even though we might expect a higher overall risk of suicide attempts among female adolescents, there are several reasons to posit that socioeconomic context might be more salient for boys. First of all, while an empirical answer for this pattern is lacking in previous literature, gender-stratified ecological studies have shown that the association between area-level poverty and suicide rates were stronger for men than women (Brock et al. 2006; Cairns et al. 2017; Sher 2005). Second, with some notable exceptions (Brazil and Clark 2017; Clampet-Lundquist et al. 2011), evidence shows that adolescent boys’ mental health is relatively more vulnerable to the impacts of socioeconomic factors in general (McLeod and Owens 2004) and contextual socioeconomic disadvantage in particular (Boticello 2009; Kroneman et al. 2004). Based on these findings, it is reasonable to expect that boys’ suicidal behaviors might be more susceptible to the effects of contextual socioeconomic disadvantage.
Explaining the Contextual Effect of Area-level Socioeconomic Disadvantage on Adolescent Suicidal Behaviors
Why might area-level socioeconomic disadvantage affect adolescent suicidal behaviors over and above individual-level disadvantage? An empirical answer to this question has not been provided by previous suicide research, but the stress process perspective in mental health literature could lead us to a possible explanation (Pearlin 1989). Consistent with the basic tenets of social disorganization theory (Sampson and Groves 1989), decades of stress process research have shown that individuals living in socioeconomically disadvantaged contexts are more likely to be exposed to a greater number of stressors due to the decayed social order and weakened social control mechanisms in such areas (Aneshensel and Sucoff 1996; Cutrona et al. 2006; Hill and Maimon 2013). Stressful life events such as criminal victimization and exposure to violence occur with greater frequency (Boardman et al. 2001; Ross and Mirowsky 2009; Sampson 1985), and chronic stressors such as fear of crime and feeling unsafe are more common among adolescents living in these contexts (Ross and Mirowsky 2001; Mirowsky and Ross 2003). Social disorder in disadvantaged contexts not only increases the exposure to these acute and chronic stressors, but also undermines individuals’ psychological and social resources by invoking general feelings of mistrust and negative appraisal (Mirowsky and Ross 2003). Living in disadvantaged neighborhoods was associated with lower self-esteem (Behnke et al. 2011; Hill and Maimon 2013) and less perceived social support (Schieman 2005; Cutrona et al. 2006). The buffering effects of these resources against stressors were also dampened in socioeconomically disadvantaged areas (Wight et al. 2005).
Even though it has yet to be tested, indirect evidence suggests that the stress process model could be useful in explaining the possible area-level effects of socioeconomic disadvantage on adolescent suicidal behaviors. First of all, stress process mechanisms have been useful in explaining the relationship between area-level disadvantage and mental and behavioral health problems such as depression (Cutrona et al. 2006; Kim 2010; Ross 2000) and substance use (Boardman et al. 2001; Hill and Angel 2005), which are similar to suicidal behaviors with respect to their variations across area-level characteristics. These mental and behavioral health problems are closely associated with suicidal behaviors (Galaif et al. 2007), suggesting there might be some common underlying mechanisms. Furthermore, contextual stressors such as community problems (Zhou and Zhang 2014) and exposure to violence (Bennett and Joe 2015; Van Orden et al. 2010; Yildiz and Solakoglu 2017), and psychosocial resources such as self-esteem (Sharaf et al. 2009) and social support (Farrell et al. 2015; Miller et al. 2015) have also been individually associated with suicidal behaviors in youth. Therefore, from the stress process perspective, it is reasonable to anticipate that the contextual effects of socioeconomic disadvantage on adolescent suicidal behaviors will be mediated by differential exposure to stressors and/or access to psychosocial resources.
The Current Study
Previous studies have suggested a possible association between area-level socioeconomic disadvantage and adolescent suicidal behaviors, but it seems that further multilevel research is needed to assess whether this effect is contextual or compositional. Further investigation is also needed to explore the possible gender differences and the underlying mechanisms, as previous studies were limited in these regards. This research aims to deepen our understanding of the association between area-level socioeconomic disadvantage and adolescent suicide attempts primarily by filling these gaps in the literature. Several key research questions guide this research. First, does area-level socioeconomic disadvantage contribute to the risk of suicide attempts, net of individual-level socioeconomic factors? Second, does the effect of area-level socioeconomic disadvantage on the risk of adolescent suicide attempts differ for boys and girls? Finally, do differential exposure to stressors (exposure to physical violence and perceived lack of safety) and/or access to psychosocial resources (self-esteem and social support) account for the contextual effects of socioeconomic disadvantage? These questions were addressed by applying multilevel modeling techniques to test the direct, indirect, and interactive effects among our variables of interest. It is expected that adolescents, especially boys, who lived in socioeconomically disadvantaged contexts would have a higher risk of suicide attempts, even after controlling for individual-level socioeconomic factors. Based on the stress process perspective, it is also expected that the aforementioned stressors and psychosocial resources would mediate this effect.
Methods
The Sample
Data for this study were obtained from the first two waves (1994/95 and 1996) of the National Longitudinal Study of Adolescent Health (Add Health). Add Health is a nationally representative study of American adolescents in seventh through twelfth grade, in 134 middle and high schools in 80 different sampling areas. The overall response rate for the 134 participating schools was 79% (See Bearman et al. 1997 for further information on study design). The individual-level measures were based on in-home interviews of adolescents and corresponding parent questionnaires. Area-level data came from the appended 1990 U.S. Census data.
Several sample selection filters were used to produce the analytic sample. To control for the temporal order of study variables and benefit from the longitudinal nature of the Add Health data, this study used the outcome variable of suicide attempts measured in Wave 2; all other explanatory variables were measured in Wave 1. Thus, the sample was restricted to the respondents who participated in both Wave 1 and Wave 2 of Add Health (N = 14,738). Among these, respondents who didn’t have valid sample weights and/or corresponding census data were excluded. Finally, since this study was interested in the area-level effects, adolescents who moved to a different address between Waves 1 and 2 were excluded from the sample. These restrictions reduced the analytic sample to 13,335 adolescents. Of this final sample, almost half were female (49.63%). The largest race category was Non-Hispanic White (65.52%), followed by African American (15.48%), Hispanic (12.11%), Asian (3.92%), and Native American (2.02%). The mean age was 15.02 (SD = 1.61), and more than half of the sample lived with both parents (56.38%) at Wave 1. Missing data on the individual-level variables were imputed using “ICE” procedures in Stata (Royston 2005).
Measures
Suicide attempt
Adolescents’ Wave 2 self-reports of suicide attempts were used as the dependent variable. Adolescents were asked: “During the past 12 months, how many times did you actually attempt suicide?” Responses ranged from zero to four times. Consistent with prior studies using Add Health data (Maimon and Kuhl 2008), we operationalized adolescents’ suicide attempts as a count variable. Since suicide attempts were rare and the variance of the measure larger than its mean, we employed a Poisson distribution and specified overdispersion in the analytic models.
Area-level socioeconomic disadvantage
Area-level socioeconomic disadvantage was comprised of a single composite factor derived from a principal component analysis (PCA) of four census tract items: “proportion of households receiving public assistance,” “proportion of individuals living below the poverty level,” “proportion of individuals aged 25 + without a high school diploma,” and “unemployment rate” (Sampson et al. 2002). Following previous studies that analyzed Add Health data (Wight et al. 2005, 2006), the PCA scores were then collapsed from the census tract to the level of each primary sampling area, or what we simply refer to here as “areas.” Each of these areas (N = 80) were generally comprised of one high school and one corresponding feeder middle school. Operationalizing areas in this way offered some advantages over using official census tracts as the primary contextual unit (Wight et al. 2005, 2006). First, whereas official census tracts represent the adolescents’ local contexts, areas capture their local and extra-local surroundings. In other words, the collapsed data provided an approximation of the larger social context in which these adolescents resided, went to school, and interacted with others beyond their proximal environment. Second, this approach overcame a methodological issue in the Add Health study. In almost 50% of the Add Health census tracts, there is only one sampled adolescent; this impedes any statistical estimation of within-census tract variation. The areas were not perfectly balanced (range of sampled adolescents = 37 to 1,795, median = 222); however, since there were no areas with just one sampled adolescent, within-area variation could be estimated with some confidence.
Stressors
Measures of exposure to violence and perceived lack of safety were included to capture contextually relevant stressors in adolescence. Both measures were previously used for samples of U.S. adolescents where they displayed modest reliability (Benson 2014; Johnson and Mollborn 2009).
Exposure to violence
This stressor was assessed based on adolescents’ reports of witnessing or experiencing violence. Each respondent was asked: “During the past 12 months, how often did each of the following things happen? (1) Someone shot you (2) Someone cut or stabbed you (3) Saw someone shoot or stab another person (4) You were jumped.” The response options included never, once, or more than once. Scores to these four examples of violence were summed to form a scale that ranged from never (0) to five times and more (5); the result produced an acceptable level of reliability (α = 0.65; minimum and mean factor loadings are 0.33 and 0.51, respectively).
Perceived lack of safety
This stressor was constructed by combining two items addressing whether or not adolescents usually felt safe at their school (strongly agree to strongly disagree) and in their neighborhood (yes or no). Adolescents who strongly disagreed with the assertion that they felt safe at school and/or answered “no” to feeling safe in their neighborhoods were coded as “1” for a perceived lack of safety.
Psychosocial resources
Measures of social support and self-esteem were included to capture adolescents’ psychosocial resources. The measures were previously validated with samples of U.S. adolescents and displayed strong reliability (Benson 2014; Wight et al. 2005).
Social support
Social support was assessed by responses to the seven questions asking about the extent to which adolescents felt cared for by their parents, other adults, friends, and teachers, as well as if their family paid attention to them, understood them, and if they had fun together. Response categories ranged from “1” indicating not at all, to “5” representing very much. Scores were averaged to form a social support measure ranging from 1 to 5 (α = 0.78).
Self-esteem
The Rosenberg Self-Esteem Scale (Simmons et al. 1973) was used to measure this construct. Adolescents were asked to indicate whether they liked themselves the way they were, had a lot to be proud of, felt socially accepted; felt like they were doing everything just right, felt loved and wanted, and had a lot of good qualities. Response categories ranged from strongly disagree (0) to strongly agree (4). Scores were averaged to create a self-esteem measure ranging from 0 to 4 (α = 0.84).
Demographic variables
Individual-level demographics in the analysis included household income (scored in thousands of dollars and logged), parental education (ranging from 0 = never went to school to 9 = higher education beyond 4-year college; maximum value in the case of two parents), gender (coded “1” for female and “0” for male), age (in years), race/ethnicity (Non-Hispanic White, African-American, Hispanic, Asian, Native American, and Other), and family living arrangement (coded “1” for respondents living with both biological parents and “0” for all other living arrangements). Although household income and parental education are not attributes of adolescents, they were treated as individual-level indicators of socioeconomic status since they were assessed for each individual adolescent (Wight et al. 2005).
Analytic Strategy
The analyses began with a presentation of the descriptive statistics for all of the variables included in our study (see Table 1). We then performed a series of multilevel analyses to assess the simultaneous effects of area- and individual-level predictors on adolescent suicide attempts (Gelman and Hill 2014). The multilevel modeling approach allows for more elaborative and precise analyses of the behaviors of individuals clustered within larger units (e.g., areas). Overall, this method was able to overcome the limitations of applying ordinary regression techniques to clustered data. First, it provided more accurate estimates of coefficients and standard errors by adjusting for interdependence among individuals within higher-level units. Second, it enabled us to estimate the effects of variables across higher-level units (e.g., area-level socioeconomic disadvantage). Finally, it allowed for an assessment of the interactive effects of variables at different levels (e.g., area-level socioeconomic disadvantage and gender). In this study, we employed a two-level random-intercept Poisson model. All analyses were weighted using “SVY” commands in Stata to adjust for the complex sampling design of the Add Health study (Chen and Chantala 2014).
In these multilevel analyses, an unconditional random-intercept model (without any predictors) was first estimated to test whether suicide attempt rates varied significantly across all areas. Next, area-level socioeconomic disadvantage, gender, and a cross-level interaction term between the two were included. This model tested whether there was a significant relationship between socioeconomic context and adolescent suicide attempts, and whether this relationship differed for boys and girls. Third, individual-level socioeconomic indicators (parental education and household income) and other demographic controls such as race/ethnicity, age, and family living arrangements were included. This model tested whether a significant residual relationship remained between area-level socioeconomic disadvantage and suicide attempts after controlling for individual-level socioeconomic and demographic characteristics (i.e., whether the effect was contextual vs. compositional). Finally, in the subsequent models, piecewise blocks of predictor variables were added to assess the degree to which each of the variables of interest— psychosocial resources and stressors—helped explain the remaining relationship between area-level socioeconomic disadvantage and suicide attempts.
Results
Descriptive Statistics
The descriptive statistics for all of the variables in our analyses are presented in Table 1. The mean number of suicide attempts was .06 (SD = 0.32). Overall, 3.37% (N = 450) of the adolescents reported attempting suicide during the 12 months before Wave 2; most (62%) attempted suicide only once. The measures of individual-level socioeconomic status revealed that the average household income for adolescents was close to $47,000 and the average parental education level was between high school diploma and college degree. Given the possible range of responses, the mean social support (M = 4.05; SD = 0.59) and self-esteem (M = 3.13; SD = 0.59) scores were relatively high. The mean value for exposure to violence was low (M = 0.39; SD = 0.88), but a substantial minority of adolescents perceived a lack of safety in their personal contexts (18.99%). Finally, area-level socioeconomic disadvantage was diverse across the various areas, with PCA scores ranging from −1.05 to 2.31 (M = −0.01; SD = 0.68). The descriptive statistics for the individual items forming this scale showed socioeconomic diversity at the area level.
Multilevel Analyses
The results from the multilevel Poisson regression analyses are presented in Table 2. First, in order to assess the degree of variation in suicide attempt rates among the areas, we estimated an unconditional model with no included predictors (not shown). This preliminary analysis showed that suicide attempt rates among adolescents varied significantly across the areas (γ00 = −3.05, p < 0.001; τ00 = 0.24, p < 0.001); however, the interclass correlation coefficient (ρ) was small (0.03), suggesting that most of the variation occurred at the individual level.
Next, the effects of area-level socioeconomic disadvantage and gender, as well as a cross-level interaction between the two with regards to adolescent suicide attempts were estimated (see Table 2, Model 1). Note that the coefficient of the cross-level interaction term represented the difference in the effects of area-level socioeconomic disadvantage for boys and girls. Due to this interaction term, the coefficient of area-level socioeconomic disadvantage was not a general (main) effect, but rather the effect of area-level socioeconomic disadvantage on boys (i.e., when female = 0). Similarly, the coefficient for female represented the effect of a female gender when area-level socioeconomic disadvantage was 0 (i.e., around the mean; M = −0.01). The first model indicated that area-level socioeconomic disadvantage significantly increased the risk of suicide attempts, but the effect differed for boys (β = 0.28; p < 0.05) and girls (β = 0.28 –0.25 = 0.03, p < 0.05). Specifically, females were far less severely influenced by the socioeconomic context than were boys. On average, a one-unit increase in PCA score for area-level socioeconomic disadvantage was expected to increase the incidence rate of suicide attempts by 32% for boys (IRR = 1.32), whereas it did so by only 2% (IRR = 1.32 × 0.78 = 1.02) for girls. Nevertheless, girls were found to be significantly more likely to attempt suicide than boys (β = 0.72; IRR = 2.02; p < 0.001), when the area-level socioeconomic disadvantage was at its average.
Model 2 added the individual-level socioeconomic and demographic factors to evaluate whether area-level socioeconomic disadvantage might affect the suicide attempts of adolescents over and above these factors. Coefficients of both area-level socioeconomic disadvantage (β = .27; p < 0.05) and the cross-level interaction term (β = −0.25; p < 0.05) remained almost the same without losing any significance, indicating that these effects were not simply due to the summation of the socioeconomic characteristics of the individuals who lived in those areas (i.e., compositional), but instead reflected the emergence of a higher-level process (i.e., contextual). Higher parental education level significantly protected against suicide attempt risk (β = −0.04; p < 0.05), whereas household income did not have a significant impact. Among the other individual-level variables, being of either the Hispanic (β = 0.25; p < 0.05) or Native American (β = 0.57; p < 0.05) races was significantly associated with a higher risk of suicide attempts, while being of the African American race (β = −0.25; p < 0.05), being older (β = −0.06; p < 0.05), and living with both biological parents (β = −0.29; p < 0.001) were all associated with a lower risk of attempting suicide.
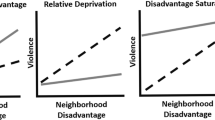
Figure 1 illustrates the effects of area-level socioeconomic disadvantage on boys’ and girls’ suicide attempts, using the results from Model 2. When area-level socioeconomic disadvantage was low (1 standard deviation below the mean), a dramatic difference existed between boys’ and girls’ predicted suicide attempt rates (2% vs. 6%, respectively). This difference decreased, however, as the area-level socioeconomic disadvantage increased. When the area-level socioeconomic disadvantage was high (1 standard deviation above the mean), there was almost no difference between boys’ and girl’s predicted suicide attempt rates. In other words, even though boys are, overall, generally less likely to attempt suicide, in the highly disadvantaged areas tested in this research, boys were at almost equal risk with girls, due to the differential effect of socioeconomic context on each.

The effect of area-level socioeconomic disadvantage on adolescent suicide attempts by gender (cross-level interaction based on model 2)
Finally, in Models 3 and 4 we entered piecewise blocks of psychosocial resources and stressors, respectively, to test whether these mechanisms might help to explain the effects of area-level socioeconomic disadvantage on suicide attempts. Examination of Model 3 revealed that both of the psychosocial resources—social support (β = −0.64; p < 0.001) and self-esteem (β = −0.55; p < 0.001)—were significantly associated with a lower risk of suicide attempts. However, controlling for psychosocial resources did not decrease the estimated effect of area-level socioeconomic disadvantage, suggesting that the effect was not mediated by these resources.
Conversely, the results in Model 4 indicated that both stressors—exposure to violence (β = 0.43; p < 0.001) and perceived lack of safety (β = 0.35; p < 0.001)—were significantly associated with a higher risk of suicide attempts, and inclusion of these stressors reduced the magnitude and significance levels of the coefficients of both area-level socioeconomic disadvantage and the interaction term. Elimination of the original relationship between area-level socioeconomic disadvantage and suicide attempts was a strong indication of the mediating effects of these stressors.
Sensitivity Analyses
Statistically, for mediation to occur, significant associations also needed to be present between our main independent variable, area-level socioeconomic disadvantage, and the mediators exposure to violence and perceived lack of safety (Baron and Kenny 1986). To test for this condition, the binary associations among area-level socioeconomic disadvantage and the stressors were examined. Due to the nature of the measures, we conducted a Spearman’s nonparametric correlation test for the relationship between area-level socioeconomic disadvantage and exposure to violence (0–4), and simple logistic regression for the connection between area-level socioeconomic disadvantage and perceived lack of safety (0–1). These supplementary analyses (see Table 3) revealed that both exposure to violence and perceived lack of safety were indeed significantly higher among adolescents living in socioeconomically disadvantaged contexts. The bivariate associations were also slightly stronger for boys than girls.
Upon reviewers’ suggestions, multilevel analyses were re-conducted with official census tracts instead of primary sampling areas. We were unable to find any significant within-census tract variation in suicide attempt rates, probably because the half of the census tracts contained only one sampled adolescent. Additionally, to support our assumption that socioeconomically disadvantaged areas had higher levels of social disorganization and decay, we checked whether the crime rates were higher in lower socioeconomic status areas. Findings of these supplementary analyses indicated that crime rates were indeed higher in socioeconomically disadvantaged areas (R = 0.31***), and adjusting for area-level crime rates reduced the coefficient of area-level socioeconomic status (from IRR = 1.31*** to IRR = 1.21*). This remaining effect became insignificant after controlling for individual-level stressful experiences (exposure to violence and perceived lack of safety).
Discussion
Multilevel research on the effects of area-level socioeconomic disadvantage on adolescent suicidal behaviors is scarce, despite the enduring interest of social researchers in contextual risk factors of suicide. Moreover, there are considerable gaps in the literature regarding the gender differences and underlying mechanisms. Using Add Health data, this study examined the association between area-level socioeconomic disadvantage and suicide attempts among adolescents, focusing on the potential moderating role of gender and the mediating roles of contextually relevant stressors and psychosocial resources. Building on previous suicide research, it was expected that adolescents, especially boys, who live in socioeconomically disadvantaged contexts would be at a higher risk of attempting suicide, even after controlling for individual-level socioeconomic factors. Drawing on stress process theory, it was also expected that stressors of exposure to violence and perceived lack of safety, as well as the psychosocial resources of social support and self-esteem, would mediate this effect.
The findings indicate that suicide attempt risk among adolescents varied significantly across the sampled areas, even though most of the variation occurred at the individual level. Socioeconomic status at the area level was significantly associated with adolescent suicide attempts, and gender was a significant moderator. Specifically, even though area-level socioeconomic disadvantage increased suicide attempt risk in adolescents of both gender, the effect was much stronger for boys than girls. The differential effect of socioeconomic context on boys and girls was robust to the inclusion of individual-level socioeconomic factors, suggesting that the effect was mostly contextual rather than compositional. In other words, the association between area-level socioeconomic disadvantage and suicide attempts was not due to the socioeconomic characteristics of adolescents who live such contexts; rather, there were higher-level processes affecting those adolescents irrespective of their socioeconomic characteristics. This contextual effect is consistent with Dupéré et al. (2009), a multilevel study on Canadian adolescents, and further advances the current literature by providing evidence from a U.S. adolescent sample. The findings regarding the gender differences also enhance the knowledge produced by previous multilevel studies, many of which contained the hidden assumption that socioeconomic context would influence all adolescents in the same way. Female disadvantage in risk of suicide attempts is a well-known phenomenon (Canetto 2008) that was confirmed by this study, but the finding that gender difference almost vanished in highly disadvantaged contexts is a unique contribution to suicide research.
The findings also shed light on the mechanisms through which area-level socioeconomic disadvantage increased adolescent suicide attempt risk. As predicted by the logic of the stress process paradigm, the contextual effect was explained by the fact that adolescents from socioeconomically disadvantaged areas encounter more stressors (i.e., experience higher levels of exposure to violence and perceive a greater lack of safety) than others. This finding is concordant with previous neighborhood and mental health literature, which has shown that the effects of objective measures of the neighborhood context on various adolescent mental health outcomes are mediated by subjective neighborhood experiences (Hill and Maimon 2013). Consistent with social disorganization theory (Sampson and Grooves 1989), low socioeconomic status areas are often characterized by few social control mechanisms, which may increase the likelihood of exposure to violence and feeling unsafe. From the stress process perspective, living in a socioeconomically disadvantaged context can also be considered a primary stressor, which may then lead to the emergence of additional, secondary stressors such as exposure to violence and lack of safety (Pearlin 1989). Even though stressors have been used to explain the effects of contextual factors on various mental and behavioral health problems (Cutrona et al. 2006; Hill and Angel 2005; Kim 2010), to the best of our knowledge, this study is the first one to examine the mediating role of stressors on the relationship between area-level socioeconomic disadvantage and adolescent suicidal behaviors.
Contrary to expectations, however, the higher risk of suicide attempts in low socioeconomic status contexts did not appear to result from deficits in psychosocial resources such as social support or self-esteem. Although perceived social support and self-esteem protected adolescents against attempting suicide, no evidence was found to suggest that these resources mediate the effect of socioeconomic context. Instead of mediating, it is possible that these psychosocial factors buffer the effects of area-level socioeconomic disadvantage and/or stressors on adolescent suicidal behaviors (Wight et al. 2006). Thus, we recommend future researchers in this area to build upon the current analyses, especially in form of more elaborated models that integrate psychosocial resources as moderators (rather than mediators) in the process.
Why does socioeconomic context have a stronger effect on boys’ suicidal behaviors? Even though a detailed answer is beyond the scope of this research, our findings suggest one possible answer. Since exposure to stressors accounted for the relationship between contextual disadvantage and suicide attempts, one could argue that boys are more sensitive to their socioeconomic context because they have a higher chance of being exposed to contextual stressors. Boys spend more time immersed in their community environment (Ramirez-Valles et al. 2002), and have higher risk-taking tendencies, including becoming involved in street fighting, neighborhood gangs, and possessing firearms (Esbensen et al. 1999). Conversely, adolescent girls spend more time at home than in the neighborhood and are more likely to be closely supervised by their parents (Kroneman et al. 2004). Therefore, their socioeconomic context might not be as influential on them as on boys. Consistent with this argument, we found that the cross-level interaction term that represented the difference between boys and girls in terms of the effect of socioeconomic context was no longer significant once we controlled for stressors. We also found stronger bivariate relationships among area-level socioeconomic disadvantage and stressors for boys than for girls. However, we fully acknowledge that further research is needed to support this argument. Future research should continue to investigate why boys appear to be more sensitive to the effects of socioeconomic factors in general, and to contextual socioeconomic factors in particular. Our study provides the first step towards this goal.
This study has several methodological strengths. First, we analyzed data from a large-scale representative sample of American adolescents, which increased the generalizability of our findings to adolescents throughout the country. Second, we benefited from the longitudinal nature of the data by using the suicide attempt question at Wave 2 as our outcome measure. This gave us the confidence to infer directionality among the study variables. Third, instead of measuring it dichotomously, we constructed suicide attempts as a count variable, and thus also statistically captured adolescents who attempted suicide more than once in a single year. Fourth, by using multiple items from the census data, we created a composite, objective, and informative measure of area-level socioeconomic disadvantage, which may have helped in uncovering the contextual effects. Finally, our operationalization of the area overcame methodological problems associated with using official census tracts and provided a more relevant context conceptually, since it captured adolescents’ neighborhoods and the surrounding areas. Note that Allen and Goldman-Mellor (2017), who operationalized context as the official census tracts, was unable to find any contextual effect for socioeconomic disadvantage.
This study also suffers from some limitations that need to be mentioned. First of all, while the sample was large and representative, suicide attempts are still a relatively rare outcome; this may have caused decline in statistical power. Second, researchers and policy makers should be cautious in generalizing findings to completed suicides. Even though suicide attempts are the most significant predictor of subsequent completed suicides, many of the adolescents who die by suicide lack a history of suicidal behaviors (Bridge et al. 2006). Third, due to the data limitations, suicide attempt was measured by one item question asking how many times respondents have attempted suicide in the preceding 12 months. Although this measure of suicide attempt was previously used by many researchers (e.g. Maimon et al. 2010; Thorlindsson and Bernburg 2009), we acknowledge that better-constructed dimensional tools (e.g. Beck et al. 1979) would provide a better capture of suicidal behaviors of adolescents.
Fourth, we omitted from the current analyses some important individual-level risk factors regarding adolescents’ mental and behavioral health status, including depression and substance use (Galaif et al. 2007). The reason why we did so is because inclusion of such factors could obscure the effects of area-level socioeconomic disadvantage and the mediating role of stressors, given previous findings indicating that the effects of stressors on adolescent suicidal behaviors were mostly manifested through negative emotions and risky behavior (Yildiz and Solakoglu 2017). We leave further examination of this issue to future research. Fifth, our social support scale captures support from adults, teachers, parents, and friends, but it does not directly capture support from neighbors. This might be why we could not find any significant mediating effect for this psychosocial resource. It is possible that increased feelings of mistrust and negative appraisals among residents in disadvantaged contexts might significantly harm supportive relationships among neighbors (Mirowsky and Ross 2003). Thus, future studies should consider using better social support measures that also capture support from neighbors. Finally, the data is somehow outdated, considering that the adolescents who participated in the Add Health survey are now adults. However, even though the characteristics of participants and their contextual areas in our study might have changed over time, we don’t have any reason to believe that there has been a change in the nature of the relationship between socioeconomic context and adolescent suicidal behaviors. Our findings are still relevant, since socioeconomic inequalities among such contexts continue to exist.
In terms of policy implications, it is crucial that national suicide intervention strategies across the U.S. recognize the significant association with area-level socioeconomic disadvantage. Suicide prevention schemes should be provided across the country, but with a scale and intensity that is proportionate to the degree of socioeconomic disadvantage at the area-level (Cairns et al. 2017). Clinically speaking, health policymakers should be aware that adolescents reporting negative neighborhood or school experiences may be an especially vulnerable subgroup in need of mental health services. Thus, more attention should be paid to reduce stressors resulting from living in disadvantaged contexts. Efforts to regain social order through community organizations may be an effective way of reducing stressors such as violent crime victimization and feelings of unsafety (Latkin and Curry 2003). The robust gender differences should also be taken into account, since this may help organize gender-specific strategies for preventing incidents of suicide. Finally, the findings have some implications for researchers of theoretical model development for suicide. Even though the social disorganization and the stress process perspectives were frequently used to understand the effects of social context on various mental and behavioral health outcomes (Cutrona et al. 2006; Sampson and Groves 1989), this study shows that they are also well-suited to understand the underlying mechanisms of the contextual disadvantage-suicidal behavior association. Future social researchers should benefit more from these theoretical frameworks to improve explanatory models of youth suicidal behaviors.
Conclusion
Previous research on the effect of contextual socioeconomic disadvantage on adolescent suicidal behaviors was scarce, despite the enduring interest of social researchers in studying the contextual risk factors of suicide. Further multilevel studies were needed to determine whether the effect was compositional or contextual, and to uncover potential gender differences and underlying mechanisms. The present study aimed to fill these gaps by applying multilevel techniques on the data gathered from a representative sample of American adolescents. The findings showed that adolescents living in socioeconomically disadvantaged areas were at a higher risk of suicide attempts, regardless of their socioeconomic status. Gender was a significant moderator—boys were more vulnerable than girls to the effects of socioeconomic context. Consistent with the stress process perspective, the contextual effect of area-level socioeconomic disadvantage was explained by differential exposure to contextual stressors. The findings underscore the importance of contextual characteristics on adolescent suicidality and suggest that appropriate prevention strategies should be developed to reduce suicidal behaviors that might result from living in disadvantaged contexts.
References
Agerbo, E., Sterne, J. A., & Gunnell, D. J. (2007). Combining individual and ecological data to determine compositional and contextual socio-economic risk factors for suicide. Social Science & Medicine, 64(2), 451–461.
Allen, K., & Goldman-Mellor, S. (2017). Neighborhood Characteristics and Adolescent Suicidal Behavior: Evidence from a Population-based Study. Suicide and Life-Threatening Behavior. Advance online publication. 10.1111/sltb.12391
Aneshensel, C. S. (2009). Neighborhood as a social context of the stress process. In W. R. Avison, C. S. Aneshensel, S. Schieman & B. Wheaton (Eds.), Advances in the Conceptualization of the Stress Process (pp. 35–52). New York: Springer.
Aneshensel, C. S., & Sucoff, C. A. (1996). The neighborhood context of adolescent mental health. Journal of Health and Social Behavior, 37(4), 293–310.
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. Journal of personality and Social Psychology, 51(6), 1173.
Beck, A. T., Kovacs, M., & Weissman, A. (1979). Assessment of suicidal intention: the Scale for Suicide Ideation. Journal of consulting and Clinical Psychology, 47(2), 343.
Behnke, A. O., Plunkett, S. W., Sands, T., & Bámaca-Colbert, M. Y. (2011). The relationship between Latino adolescents’ perceptions of discrimination, neighborhood risk, and parenting on self-esteem and depressive symptoms. Journal of Cross-Cultural Psychology, 42(7), 1179–1197.
Bearman, P. S., Jones, J., & Udry, R. J. (1997). The National Longitudinal Study of Adolescent Health: Research Design. Chapel Hill: Carolina Population Center, University of North Carolina at Chapel Hill. http://www.cpc.unc.edu/projects/addhealth/design.
Bennett, Jr, M. D., & Joe, S. (2015). Exposure to community violence, suicidality, and psychological distress among African American and Latino youths: findings from the CDC Youth Violence Survey. Journal of Human Behavior in the Social Environment, 25(8), 775–789.
Benson, J. E. (2014). Reevaluating the “subjective weathering” hypothesis: subjective aging, coping resources, and the stress process. Journal of Health and Social Behavior, 55(1), 73–90.
Boardman, J. D., Finch, B. K., Ellison, C. G., Williams, D. R., & Jackson, J. S. (2001). Neighborhood disadvantage, stress, and drug use among adults. Journal of Health and Social Behavior, 42(2), 151–165.
Botticello, A. L. (2009). School contextual influences on the risk for adolescent alcohol misuse. American Journal of Community Psychology, 43(1-2), 85–97.
Brazil, N., & Clark, W. A. (2017). Individual mental health, life course events and dynamic neighbourhood change during the transition to adulthood. Health & Place, 45, 99–109.
Bridge, J. A., Goldstein, T. R., & Brent, D. A. (2006). Adolescent suicide and suicidal behavior. Journal of Child Psychology and Psychiatry, 47(3-4), 372–394.
Brock, A., Baker, A., Griffiths, C., Jackson, G., Fegan, G., & Marshall, D. (2006). Suicide trends and geographical variations in the United Kingdom, 1991–2004. Health Statistics Quarterly, 31(6), 6–22.
Canetto, S. S. (2008). Women and suicidal behavior: a cultural analysis. American Journal of Orthopsychiatry, 78(2), 259–266.
Cash, S. J., & Bridge, J. A. (2009). Epidemiology of youth suicide and suicidal behavior. Current Opinion in pediatrics, 21(5), 613.
Cairns, J. M., Graham, E., & Bambra, C. (2017). Area-level socioeconomic disadvantage and suicidal behaviour in Europe: A systematic review. Social Science & Medicine, 192, 102–111.
Chen, P., & Chantala, K. (2014). Guidelines for analyzing Add Health data (p. 1-53). Chapel Hill, NC: Carolina Population Center, the University of North Carolina at Chapel Hill.
Clampet-Lundquist, S., Edin, K., Kling, J. R., & Duncan, G. J. (2011). Moving teenagers out of high-risk neighborhoods: how girls fare better than boys. American Journal of Sociology, 116(4), 1154–89.
Cutrona, C. E., Wallace, G., & Wesner, K. A. (2006). Neighborhood characteristics and depression: an examination of stress processes. Current directions in psychological Science, 15(4), 188–192.
Denney, J. T., Rogers, R. G., Krueger, P. M., & Wadsworth, T. (2009). Adult suicide mortality in the United States: marital status, family size, socioeconomic status, and differences by sex. Social Science Quarterly, 90(5), 1167–1185.
Denney, J. T., Wadsworth, T., Rogers, R. G., & Pampel, F. C. (2015). Suicide in the city: do characteristics of place really influence risk? Social Science Quarterly, 96(2), 313–329.
Donker, T., Batterham, P. J., Van Orden, K. A., & Christensen, H. (2014). Gender-differences in risk factors for suicidal behaviour identified by perceived burdensomeness, thwarted belongingness and acquired capability: cross-sectional analysis from a longitudinal cohort study. BMC Psychology, 2(1), 20.
Dupéré, V., Leventhal, T., & Lacourse, E. (2009). Neighborhood poverty and suicidal thoughts and attempts in late adolescence. Psychological Medicine, 39(8), 1295–1306.
Durkheim, E. (1951). Suicide, a study in sociology (J. A. Spaulding & G. Simpson, Trans.). New York: Free Press. (Original work published in 1897).
Esbensen, F. A., Deschenes, E. P., & Winfree, Jr, L. T. (1999). Differences between gang girls and gang boys: results from a multisite survey. Youth & Society, 31(1), 27–53.
Evans, E., Hawton, K., Rodham, K., & Deeks, J. (2005). The prevalence of suicidal phenomena in adolescents: a systematic review of population-based studies. Suicide and Life-Threatening Behavior, 35(3), 239–250.
Exeter, D. J., & Boyle, P. J. (2007). Does young adult suicide cluster geographically in Scotland? Journal of Epidemiology & Community Health, 61(8), 731–736.
Farrell, C. T., Bolland, J. M., & Cockerham, W. C. (2015). The role of social support and social context on the incidence of attempted suicide among adolescents living in extremely impoverished communities. Journal of Adolescent Health, 56(1), 59–65.
Galaif, E. R., Sussman, S., Newcomb, M. D., & Locke, T. F. (2007). Suicidality, depression, and alcohol use among adolescents: a review of empirical findings. International Journal of Adolescent Medicine and Health, 19(1), 27–36.
Gelman, A., & Hill, J. (2014). Data Analysis Using Regression and Multilevel/Hierarchical Models. New York: Cambridge University Press.
Hill, T. D., & Angel, R. J. (2005). Neighborhood disorder, psychological distress, and heavy drinking. Social Science & Medicine, 61(5), 965–975.
Hill, T. D., & Maimon, D. (2013). Neighborhood context and mental health. In C. S. Aneshensel, J. C. Phelan & A. Bierman (Eds.), Handbook of the sociology of mental health (pp. 479–501). Dordrecht: Springer.
Johnson, M. K., & Mollborn, S. (2009). Growing up faster, feeling older: hardship in childhood and adolescence. Social Psychology Quarterly, 72(1), 39–60.
Kim, J. (2010). Neighborhood disadvantage and mental health: the role of neighborhood disorder and social relationships. Social Science Research, 39(2), 260–271.
Kroneman, L., Loeber, R., & Hipwell, A. E. (2004). Is neighborhood context differently related to externalizing problems and delinquency for girls compared with boys? Clinical Child and Family Psychology Review, 7(2), 109–122.
Latkin, C. A., & Curry, A. D. (2003). Stressful neighborhoods and depression: a prospective study of the impact of neighborhood disorder. Journal of health and social behavior, 44(1), 34-44.
Maimon, D., Browning, C. R., & Brooks-Gunn, J. (2010). Collective efficacy, family attachment, and urban adolescent suicide attempts. Journal of Health and Social Behavior, 51(3), 307–324.
Maimon, D., & Kuhl, D. C. (2008). Social control and youth suicidality: situating Durkheim's ideas in a multilevel framework. American Sociological Review, 73(6), 921–943.
Martikainen, P., Mäki, N., & Blomgren, J. (2004). The effects of area and individual social characteristics on suicide risk: a multilevel study of relative contribution and effect modification. European Journal of Population, 20(4), 323–350.
McLeod, J. D., & Owens, T. J. (2004). Psychological well-being in the early life course: variations by socioeconomic status, gender, and race/ethnicity. Social Psychology Quarterly, 67(3), 257–278.
McLoughlin, A. B., Gould, M. S., & Malone, K. M. (2015). Global trends in teenage suicide: 2003–2014. QJM: An International Journal of Medicine, 108(10), 765–780.
Miller, A. B., Esposito-Smythers, C., & Leichtweis, R. N. (2015). Role of social support in adolescent suicidal ideation and suicide attempts. Journal of Adolescent Health, 56(3), 286–292.
Mirowsky, J., & Ross, C. E. (2003). Social causes of psychological distress (2nd ed). Hawthorne: Aldine de Gruyter.
Nock, M. K., Borges, G., Bromet, E. J., Alonso, J., Angermeyer, M., & Beautrais, A., et al. (2008). Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. The British Journal of Psychiatry, 192(2), 98–105.
Nock, M. K., Green, J. G., Hwang, I., McLaughlin, K. A., Sampson, N. A., & Zaslavsky, A. M., et al. (2013). Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents: results from the National Comorbidity Survey Replication Adolescent Supplement. JAMA Psychiatry, 70(3), 300–310.
Pearlin, L. I. (1989). The sociological study of stress. Journal of Health and Social Behavior, 30(3), 241–256.
Platt, S. (2016). Inequalities and suicidal behavior. In R. O’Connor & J. Pirkis (Eds.), The International Handbook of Suicide Prevention (pp. 258–284). Chichester: Wiley.
Pirkis, J., Currier, D., Butterworth, P., Milner, A., Kavanagh, A., & Tibble, H., et al. (2017). Socio-economic position and suicidal ideation in men. International Journal of Environmental Research and Public Health, 14(4), 365.
Ramirez-Valles, J., Zimmerman, M. A., & Juarez, L. (2002). Gender differences of neighborhood and social control processes: a study of the timing of first intercourse among low-achieving, urban, African American youth. Youth & Society, 33(3), 418–441.
Rehkopf, D. H., & Buka, S. L. (2006). The association between suicide and the socio-economic characteristics of geographical areas: a systematic review. Psychological Medicine, 36(2), 145–157.
Ross, C. E. (2000). Neighborhood disadvantage and adult depression. Journal of Health and Social Behavior, 41(2), 177–187.
Ross, C. E., & Mirowsky, J. (2001). Neighborhood disadvantage, disorder, and health. Journal of Health and Social Behavior, 42(3), 258–276.
Ross, C. E., & Mirowsky, J. (2009). Neighborhood disorder, subjective alienation, and distress. Journal of Health and Social Behavior, 50(1), 49–64.
Royston, P. (2005). Multiple imputation of missing values: update. Stata Journal, 5(2), 188.
Sampson, R. J. (1985). Neighborhood and crime: the structural determinants of personal victimization. Journal of Research in Crimean and delinquency, 22(1), 7–40.
Sampson, R. J., & Groves, W. B. (1989). Community structure and crime: testing social-disorganization theory. American Journal of Sociology, 94(4), 774–802.
Sampson, R. J., Morenoff, J. D., & Gannon-Rowley, T. (2002). Assessing “neighborhood effects”: social processes and new directions in research. Annual Review of Sociology, 28(1), 443–478.
Schieman, S. (2005). Residential stability and the social impact of neighborhood disadvantage: a study of gender-and race-contingent effects. Social Forces, 83(3), 1031–1064.
Sharaf, A. Y., Thompson, E. A., & Walsh, E. (2009). Protective effects of self-esteem and family support on suicide risk behaviors among at-risk adolescents. Journal of Child and Adolescent Psychiatric Nursing, 22(3), 160–168.
Sher, L. (2005). Per capita income is related to suicide rates in men but not in women. Journal of Men’s Health and Gender, 3(1), 39–42.
Simmons, R. G., Rosenberg, F., & Rosenberg, M. (1973). Disturbance in the self-image at adolescence. American Sociological Review, 38(5), 553–568.
Thorlindsson, T., & Bernburg, J. G. (2009). Community structural instability, anomie, imitation and adolescent suicidal behavior. Journal of Adolescence, 32(2), 233–245.
Van Orden, K. A., Witte, T. K., Cukrowicz, K. C., Braithwaite, S. R., Selby, E. A., & Joiner, Jr, T. E. (2010). The interpersonal theory of suicide. Psychological Review, 117(2), 575.
Wight, R. G., Aneshensel, C. S., Botticello, A. L., & Sepúlveda, J. E. (2005). A multilevel analysis of ethnic variation in depressive symptoms among adolescents in the United States. Social Science & Medicine, 60(9), 2073–2084.
Wight, R. G., Botticello, A. L., & Aneshensel, C. S. (2006). Socioeconomic context, social support, and adolescent mental health: a multilevel investigation. Journal of Youth and adolescence, 35(1), 109.
Wray, M., Colen, C., & Pescosolido, B. (2011). The sociology of suicide. Annual Review of Sociology, 37, 505–528.
Yildiz, M., & Solakoglu, Ö. (2017). Strain, negative emotions, and suicidal behaviors among adolescents: testing general strain theory. Youth & Society. Advance online publication. doi: ?10.1177/0044118X17700318
Zhou, R., & Zhang, J. (2014). Effects of community stress and problems on residents’ psychopathology. Psychiatry Research, 215(2), 394–400.
Acknowledgements
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R. Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth). No direct support was received from grant P01-HD31921 for this analysis.
Authors’ Contributions
MY conceived of the study, accessed data, participated in statistical analyses and interpretations, and drafted the manuscript. ED developed the measures, participated in the design of the study, and drafted the manuscript. SG helped to draft the manuscript and participated in the interpretations of the results. All authors read and approved the final manuscript.
Funding
The authors received no specific funding for this work.
Data Sharing and Declaration
The restricted-use datasets analyzed during the current study are not publicly available but are available by contractual agreement through Add Health contracts team. (https://www.cpc.unc.edu/projects/addhealth/documentation/restricteduse).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
The data set was approved by Louisiana State University Institutional Review Board (IRB# 3529). This work was conducted in accordance with general ethical standards.
Informed Consent
Add Health participants provided written informed consent for participation in all aspects of Add Health in accordance with the University of North Carolina School of Public Health Institutional Review Board guidelines.
Rights and permissions
About this article

Cite this article
Yildiz, M., Demirhan, E. & Gurbuz, S. Contextual Socioeconomic Disadvantage and Adolescent Suicide Attempts: A Multilevel Investigation. J Youth Adolescence 48, 802–814 (2019). https://doi.org/10.1007/s10964-018-0961-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-018-0961-z