
This study examined whether the impact of contextual-level socioeconomic disadvantage on adolescent mental health is contingent upon individual-level perceptions of social support. Data are from the National Longitudinal Study of Adolescent Health (Add Health), a panel survey of a nationally representative United States sample (analytic N=18,417) of students in 7th through 12th grade. Effects of social support and social context on both internalizing problems (depressive symptoms) and externalizing problems (minor delinquency and violent behavior) are analyzed. Contextual-level socioeconomic disadvantage is positively associated with depressive symptoms, negatively associated with minor delinquency, and not directly associated with violent behavior. High perceived support from family, friends, and other adults offsets poor mental health, but is most protective in areas of low socioeconomic disadvantage. The mental health benefits of perceived social support are dampened in socioeconomically disadvantaged areas, compared to advantaged areas. Results suggest that interventions targeting only individual- or family-level processes within disadvantaged contexts may be inadequate at stemming psychological distress among adolescents.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
INTRODUCTION
The overwhelming majority of studies linking low socioeconomic status (SES) to poor adolescent mental health have focused only on the individual or the family. Consistent with a family systems framework (e.g., Kreppner and Lerner, 1989), the family, in particular, has been seen as the most proximal and important context for examining SES differentials in adolescent health because it is typically the parents, rather than the individual adolescent, who earn an income. However, a growing body of research supports the value of assessing the mental health impact of larger social contexts (e.g., neighborhoods or communities) by revealing contextual-level SES effects in general (Adler et al., 1994; Anderson and Armstead, 1995; Leventhal and Brooks-Gunn, 2000; Sampson et al., 2002; Taylor et al., 1997; Williams and Collins, 1995), as well as for adolescent emotional well-being in particular (Aneshensel and Sucoff, 1996; Brooks-Gunn et al., 1993; Goodman et al., 2003; Wheaton and Clarke, 2003; Wickrama and Chalandra, 2003; Wight et al., 2005). Still, there is little research into the mechanisms that may generate this effect. In addition, most research focuses solely on one mental health outcome, even though any single indicator is not an adequate proxy for all disorders (Aneshensel et al., 1991; Thoits, 1995). This article uses data from a large nationally representative United States (U.S.) sample of adolescents to explore the role of perceived social support in moderating the association between socioeconomic context and both internalizing problems (depressive symptoms) and externalizing problems (minor delinquency and violent behavior).
This examination is driven by a multilevel approach that incorporates the simultaneous effects of the contextual-level and the individual-level. As a structural model, it emphasizes: (a) The structural properties of geographic contexts, economic stratification in particular; and (b) The location of the adolescent within systems of stratification (e.g., ethnicity, household structure, household income). This multilevel model is a major advance over most previous research on mental health among adolescents, which generally treats individual-level characteristics in isolation from social contexts, or treats contextual-level characteristics as if they are attributes of the person. The structural model is extended to incorporate cross-level interactions between contextual- and individual-level effects, thereby creating an ecological model. That is, the possibility that the effects of the social context in which the individual lives are contingent upon his or her personal characteristics is tested. This ecological model conceptually enhances the structural model, which contains the hidden assumption that contextual-level effects are the same for all individuals.
The recognition that socioeconomic context is relevant to mental health dates to Faris and Dunham (1960/1939), who documented associations between rates of mental disorder and areas characterized by social disorganization in Chicago. Recent interest in neighborhood and mental health flows in large part from the work of Wilson (1987, 1991) and Massey and Denton (1993), especially their descriptions of the emergence of hyper-segregated underclass urban communities. Wilson (1991) suggests that social isolation in concentrated poor neighborhoods has negative psychological consequences for the ability to plan, for efficacy, and for organization. Massey and Denton (1993) contend that the physical deterioration of the environment influences the social behavior of residents in that community. Specifically, the presence of ambient hazards such as abandoned housing lead to visible deviance such as public drunkenness, prompting residents to withdraw and spend more time indoors, thus focusing social interactions on family and close friends, and decreasing involvement in the larger community. This self-sustaining cycle lessens social control and leads to greater social disorganization.
Work conducted within this framework (the structural approach), is concerned with the idea that neighborhood disadvantage adversely affects all residents. In analytic terminology, this approach posits main effects of neighborhood characteristics on individual outcomes. From this perspective, variation in individual responses to neighborhood conditions is attributed to differences in exposure to these neighborhood conditions, or to differences in other risk factors (Crane, 1991). In contrast, social ecological theory adopts a social psychological perspective that emphasizes the intersection of neighborhood and person, especially risk (e.g., physical decay) and protective factors (e.g., social support) that enable some youth in adverse settings to attain more successful outcomes than most other youth (Jessor, 1992, 1993). The ecological model is concerned with the junction of person and environment, as embodied in the phrase “person-environment fit.” This model, therefore, is inherently conditional, that is, in analytic terminology, it posits an interaction between neighborhood and individual attributes.
There is scant previous research assessing the impact of socioeconomic context on internalizing problems among adolescents. Overall, the association between depressive symptoms and contextual-level SES appears to be negative: Adolescents residing in areas of low SES are at heightened risk for depressive symptomatology (Aneshensel and Sucoff, 1996; Brooks-Gunn et al., 1993; Goodman et al., 2003; Leventhal and Brooks-Gunn, 2003; Wickrama and Chalandra, 2003; Wight et al., 2005). The distressing impact of contextual-level socioeconomic disadvantage in childhood even appears to be sustained into young adulthood. Wheaton and Clarke (2003) found that current neighborhood disadvantage has no effect on early adult internalizing problems when childhood neighborhood disadvantage is controlled, negating a contextual continuity hypothesis positing that neighborhood contexts are sufficiently stable over time that any effect of the past is mediated by the present context. Thus, socioeconomic context in adolescence has both proximal and distal effects on emotional health.
At the individual-level, risk factors for adolescent internalizing problems, depressive symptoms in particular, have been comprehensively examined. The most extensive work concerns gender and age, with both clinical and community studies finding more symptoms of depression among older than younger teens, and among girls than boys by mid-adolescence (e.g., Aneshensel and Sucoff, 1996; Cryanoski et al., 2000; Nolen-Hoeksema and Girgus, 1994; Peterson et al., 1993; Resnick et al., 1997). A growing body of research examines the association between ethnicity and depressive symptoms, finding that minority teens have higher symptom levels than non-Hispanic Whites (e.g., Garrison et al., 1989; Schraedley et al., 1999; Rushton et al., 2002; Wight et al., 2005). However, some existing studies tend to confound ethnicity with socioeconomic status because African-American and Hispanic adolescents are substantially more likely to be living below the poverty line than non-Hispanic White adolescents (McClanahan and Casper, 1995), and living in disadvantaged financial circumstances, in turn, is positively associated with depressive symptoms (Dornbusch et al., 1991; Garrison et al., 1989; Gore et al., 1992; Hammack et al., 2004; Wilson, 1987). The depressive effect of family living arrangement is somewhat mixed in that some studies have found no impact of family structure (Aneshensel and Sucoff, 1996; Eamon, 2002; Gerard and Buehler, 2004) whereas others have found that living in homes without both biological parents is a risk factor for depressive symptoms (Rushton et al., 2002; Wight et al., 2005).
Findings for the impact of socioeconomic context on violent behavior and minor delinquency are somewhat ambiguous and many studies combine elements of these two constructs to create a composite measure. For example, one study found no main effect of neighborhood affluence on externalizing behavior, but an indirect effect such that males were at increased risk in neighborhoods of low affluence (Beyers et al., 2003). Yet, another study found that male adolescents in high SES neighborhoods are significantly less likely than male adolescents in low SES neighborhoods to engage in violent behavior (Beyers et al., 2001). Hoffman (2003) found that adolescents residing in areas of high male joblessness who experience stressful life events or little parental supervision are especially likely to exhibit serious delinquent behavior such as fighting or being arrested. Aneshensel and Sucoff (1996) found that symptoms of conduct disorder are especially low among Hispanics living in impoverished neighborhoods, whereas symptoms of oppositional defiant disorder are somewhat high in middle class communities. Thus, whereas it is clear that low contextual-level SES increases the risk for depressive symptomatology, its impact on delinquency and violent behavior appears to be complex.
Findings concerning individual-level risk factors for externalizing problems are also not entirely consistent, making it difficult to identify a particular risk profile. It is generally recognized that older male teens are at the highest risk for delinquent and violent behavior (e.g., Aneshensel and Sucoff, 1996; Beyers et al., 2001; Ellickson and McGuigan, 2000; Gerard and Buehler, 2004; Hoffman, 2003; Rankin and Kern, 1994). Regarding ethnicity, some studies find that non-Hispanic White youth are at highest risk for externalizing problems (Hoffman, 2003; Rankin and Kern, 1994), whereas others find Hispanic youth to be at greatest risk (Aneshensel and Sucoff, 1996; Gerard and Buehler, 2004). Findings from studies that specifically examine violent behavior are similarly mixed, in that some determine African-American youth to be at greatest risk (Sampson et al., 2005) and others find no significant impact of ethnicity (Ellickson and McGuigan, 2000). Family SES often fails to significantly predict adolescent externalizing problems (Aneshensel and Sucoff, 1996; Gerard and Buehler, 2004), but some researchers have found low SES to be a risk factor (Beyers et al., 2003), especially for violent behavior (Heimer, 1997). Inconsistencies are also apparent in the research on the impact of family structure. Living with both biological parents is protective of externalizing problems in some samples (Gerard and Buehler, 2004; Hoffman, 2003; Sampson et al., 2005), whereas this living arrangement has no externalizing impact in other samples (Aneshensel and Sucoff, 1996; Beyers et al., 2003; Ellickson and McGuigan, 2000).
The availability of social support from friends, parents, and other adults has well-established protective connections to adolescent mental health, whether operationalized as internality or externality (Beyers et al., 2003; Cornwell, 2003; Kaltiala-Heino et al., 2001; Marcotte et al., 2002; Sheeber et al., 1997; Stice et al., 2004; Wiesner and Windle, 2004). Social support can broadly be defined as those interpersonal social resources that involve either the presence or the implication of stable human relationships (Turner and Turner, 1999). Perceptions of social support have been shown to more strongly influence mental health than the actual receipt of support (Dunkel-Schetter and Bennett, 1990; Turner and Turner, 1999). Whether social support helps to account for the association between contextual-level SES and adolescent mental health, however, is largely uncharted waters. It is reasonable to expect that social support will have some impact on this association, given that studies have found support to “buffer” the deleterious effect of many other forms of stressors on emotional distress (Aneshensel, 1992; Pearlin, 1989; Thoits, 1995; Turner and Turner, 1999). According to the buffering perspective, the mental health impact of socioeconomic disadvantage should decrease as social support increases.
Thus, the goals of this article are three-fold: (1) To assess the nature of the association between contextual-level socioeconomic disadvantage and adolescent internalizing and externalizing problems; (2) To examine if and how social support impacts or moderates these associations; and (3) To assess the contemporaneous mental health impact of other risk factors. Based on previous research, we expect to find that contextual-level socioeconomic disadvantage is positively associated with depressive symptomatology. However, due to inconsistent findings concerning associations between contextual-level disadvantage and both minor delinquency and violent behavior, we make no a priori claims about the pattern of results we expect to uncover. We hypothesize that social support will be beneficial to adolescents, will offset any mental health deficits that stem from living in disadvantaged circumstances, and that the impact of support will vary across residence areas. At the individual-level, we predict that females, ethnic minorities, older teens, those not living in nuclear families, and those living in households with low income to be at highest risk for internalizing problems. We expect similar findings for externalizing problems, with the notable exception being that males will be at the highest risk. Analysis of this large nationally representative sample offers a unique opportunity to representatively investigate whether social support buffers the mental health impact of adverse social contexts among U.S. adolescents.
METHOD
The Sample
Data are from the National Longitudinal Study of Adolescent Health, “Add Health” (Bearman et al., 2005; Resnick et al., 1997), a nationally representative, school-based sample of 20,745 adolescents in grades 7 through 12 surveyed during the 1994–1995 academic year. The sampling frame consisted of all high schools in the United States (U.S.). A total of 80 high schools were selected with probabilities proportional to size. A sample of 52 feeder middle schools was attached to the sample of high schools. A total of 134 schools participated in the baseline study, with a response rate of 78.9%. A complete enumeration of all students was generated from student participation in an in-school questionnaire, combined with a student roster provided by the school. The sample for a detailed, in-home interview selected from this listing consists of a core sample and three supplemental over-samples included in these analyses (members of ethnic minority groups, disabled teens, and a complete sampling of two high schools and 14 small schools). The analytic sample size is 18,417 (omitting persons with missing or corrupted data). Grand sample weights adjust for the sample design and survey response rates.
Data about the adolescent and his or her family are from adolescent self-reports to an in-school questionnaire, a personal interview conducted at the adolescent's home, and a parental interview. In addition, a contextual database provides information about Census tract characteristics using 1990 U.S. Census data.
Individual-Level Measures
All scales were developed with principal-components analysis (varimax rotation).
Depressive symptoms were assessed with items from the Center for Epidemiologic Studies—Depression Scale (Radloff, 1977). The full CES-D consists of 20 items that ascertain depressive symptoms (e.g., felt depressed, sad, lonely, fearful) for the previous week. Add Health utilized 16 of the 20 items (three other measured symptoms are not CES-D items and are excluded here). Response categories ranged from (0) never or rarely to (3) most or all of the time. Four positively worded items were reverse scored. Possible scores for a summated measure range from 0 to 48 and the scale demonstrates very good reliability in this sample (α=.85).
Minor delinquency was assessed with five items that ascertained the frequency of various delinquent activities that adolescents may have engaged in over the previous 12 months (damaged property, lied about whereabouts, shoplifted, stole something of modest value, acted unruly in public). Response categories ranged from (0) never to (3) five or more times. Possible scores for the summated measure range from 0 to 15, and the scale demonstrates good reliability in this sample (α=.75).
Violent behavior was assessed with three items that ascertained the frequency of physically aggressive activities over the previous 12 months (got into a serious physical fight, seriously hurt someone, group fighting). Response categories ranged from (0) never to (3) five or more times. Possible scores for the summated measure range from 0 to 9, and this scale also demonstrates good reliability in this sample (α=.75).
Social support was assessed with a 7-item scale measuring the degree to which adolescents felt cared about by adults, teachers, parents, and friends, in addition to the degree to which they perceived that their family has fun together, pays attention to them, and understands them. Response categories ranged from (1) not at all to (5) very much. Possible scores for a summated measure range from 7 to 35, and the scale demonstrates good reliability in this sample (α=.79).
Other risk factors controlled in the analysis include those that have been empirically established in past research (Broidy et al., 2003; Costello et al., 2003; Overbeek et al., 2001; Wight et al., 2003): sex, age (categorized because of its known non-linear association with adolescent mental health [Kessler and Walters, 1998; Lewinsohn et al., 1998]), ethnicity [African-American, Asian-Pacific Islander (API), Hispanic, Non-Hispanic White (NHW), and “Other”], family living arrangement (lives with both biological parents versus all other living arrangements), and household income (scored in thousands of dollars and logged). Multiplicative age/sex interactions are included to assess the differential impact of age between males and females.
Contextual-Level Measure
Socioeconomic disadvantage is comprised of a single factor derived from principal components analysis of five Census tract variables: proportion of households (HH) receiving public assistance, proportion of individuals living below the poverty level, proportion of individuals aged 25+ without a high school diploma, proportion of individuals aged 25+ without a college degree, and unemployment rate.
For these analyses, contextual data are collapsed from the Census tract to the level of the primary sampling unit (high schools, N=80), operationalized as “sampling areas.” Census tract data are aggregated for all sampled students within a particular sampling area by averaging tract variables within areas [the average number of tracts per sampling area is 66 (SD=60)]. Sampling areas are mainly composed of one high school plus a feeder middle school (N=52 areas), with the remainder being composed of either one sampled school that includes grades 7 through 12 (N=22 areas) or one sampled school that includes only grades 9 through 12 (N=6 areas). There are no sampling areas that contain data from more than one high school. Thus, contextual characteristics are not attributes of the individual, the school, or of the Census tract per se, but the average attributes of the Census tracts that feed into the high school, conceptually comparable to “high school attendance areas.” Aside from providing an approximation of neighborhood “spillover” into the larger community in which teens live, this approach addresses design imbalance concerns. Nearly 50% of Add Health Census tracts (N=1,049) contain only one adolescent, thereby precluding the estimation of within-Census tract variation. The sampling areas are not ideally balanced (range of sampled individuals = 37 to 1,795, median = 222), but there are no singleton sampling areas and within-area variation can be estimated with some confidence. We believe the benefits of assessing contextual effects of a larger geographical unit, for which there is very little research, outweigh the costs of potentially misestimating social processes within singleton Census tracts.
Analysis
The analytic goal is to assess whether the mental health impact of contextual-level socioeconomic disadvantage varies over levels of adolescents’ perceived social support, which typically has a protective effect. Parallel analyses are conducted for depressive symptoms, minor delinquency, and violent behavior. Due to non-normal distributions, the square-root of each of the three dependent variables is used in multivariate analysis. Social support is transformed into quartiles due to non-linearity. Two-level hierarchical linear models are estimated with HLM software, version 5.05 (Raudenbush et al., 2000). To facilitate cross-level interactions, individual-level variables are group centered and the contextual-level variable is grand mean centered. Centered and uncentered models produce similar results. We do not present three-level models that further account for the nesting of some adolescents within families (occurring when more than one adolescent per family was interviewed, 18% of the sample) because most are single adolescent families and removing this level of clustering by randomly selecting one adolescent from multi-participant families had no impact.
First, the gross variance in each of the dependent variables that is associated with contexts is estimated with a null model that contains only random intercepts (γ00) and random variation in the intercept (τ 00). Second, the main effect of contextual-level socioeconomic disadvantage on the average level of each dependent variable is tested. Third, the impact of individual-level social support and the cross-level interaction between social support and contextual-level socioeconomic disadvantage is added. Fourth, individual-level risk factors (age, sex, ethnicity, household living arrangement, and income) are controlled. Slopes for both lower-order and higher-order social support terms are allowed to vary over contexts (i.e., assigned a random error term) to investigate whether there is significant variability in social support slopes across sampling areas. For all analyses, normalized grand sample weights are applied so that findings can be extrapolated to the population of U.S. adolescents. Deviance statistics assess model fit, and sequential differences between models are assessed with the likelihood ratio test. A statistical significance criterion of .10 is used in reporting sampling area effects (i.e., random slopes) due to the small number of degrees of freedom at the contextual-level (df=78).
RESULTS
Sample Characteristics
Table I shows individual-level characteristics of the analytic sample. As shown, NHW teens make up two-thirds of the weighted sample, sex and age are evenly distributed, over half reside with both biological parents, and median household income is somewhat higher than the median annual household income in the United States for 1995 (U.S. Census Bureau, 2005). Social support perceived from friends and family is relatively high, given the possible range of responses. The mean depressive symptom score falls within the lower 20th percentile of possible scores. The mean delinquency and violent behavior scores indicate that most adolescents do not engage in these behaviors.
Socioeconomic disadvantage is diverse across sampling areas, ranging from a principal component score of −1.28 to 1.24. Items comprising the principal component indicate socioeconomic diversity at the contextual-level.
Relationship Between Contextual-Level Characteristics, Social Support and Mental Health
Table II presents sequential HLM models that demonstrate how social support impacts the relationships between sampling area characteristics and adolescent mental health. As shown, each model represents a significant improvement in fit over the previous model. Models A1, B1, and C1 are compared to the null model, which is not shown.
Depressive Symptoms
The null model indicates significant variation in adolescent depressive symptoms across the sampling areas [γ 00=2.84 (SE=.03), p < .001; τ 00=.04, p < .001]. The intra-class correlation (ρ) is small (.03), indicating that most of the variation in symptoms is at the individual level. Model A1 indicates that high socioeconomic disadvantage is associated with high depressive symptomatology. As shown in Model A2, perceiving sub-optimal social support is also associated with high symptomatology, in comparison to perceiving the highest amount of support. In addition, the depressive impact of socioeconomic disadvantage is contingent upon social support at the individual-level, meaning that the impact of disadvantage varies across levels of perceived support. Significant variability in depressive symptoms across areas persists (τ 00=.05, p < .001), net of social support, and there is significant variability in terms of the social support slopes across sampling areas.
Individual-level risk factors are added in Model A3. As shown, the depressive impact of sub-optimal social support is sustained. Hispanic, African-American, and API teens experience depressive symptoms, on average, more often than NHW teens. One of the coefficients for the sex/age interactions is significant: Depressive symptoms increase steadily among males from early to late adolescence, increase more steeply among females than males from early to middle adolescence, but level off between middle and late adolescence. This conditional association is consistent with previous research, in which both clinical and community studies find more symptoms of depression among girls than boys by mid-adolescence, suggesting that both developmental and social mechanisms may generate this pattern (Nolen-Hoeksema and Girgus 1994; Peterson et al., 1993). Living with both biological parents and household income are negatively associated with depressive symptoms.
Minor Delinquency
The null model indicates significant variation in minor delinquency across the sampling areas [γ 00=1.21 (SE=.02), p < .001; τ 00=0.05, p < .001]. As with depressive symptoms, the intra-class correlation (ρ) is small (.05), indicating that most of the variation in delinquency is at the individual level. In contrast to depressive symptoms, however, Model B1 indicates that high socioeconomic disadvantage at the contextual-level is associated with low delinquency. Perceiving any sub-optimal social support is associated with high delinquency (Model B2). In addition, the delinquent impact of socioeconomic disadvantage is contingent upon social support at the individual-level. Significant variability in delinquency across areas persists, (τ 00=.03, p < .001), suggesting there is variation yet to be explained, and there is significant variability in terms of the slopes for low and low-medium support (in comparison to high support) across sampling areas.
The delinquent impact of sub-optimal social support is sustained when the individual-level risk factors are controlled (Model B3), and its effect continues to vary significantly across sampling areas. Hispanic teens are higher on delinquency, on average, compared to NHW teens. There is no significant contingency between age and sex, but being aged 11 to 14 years is significantly associated with high delinquency, in comparison to being aged 17 years or more. Minor delinquency is negatively associated with living with both biological parents, but in contrast to depressive symptoms, is positively associated with household income.
Violent Behavior
The null model indicates significant variation in adolescent violent behavior across the sampling areas [γ 00=.58 (SE=.02), p < .001; τ 00=0.02, p < .001], and the intra-class correlation (ρ) is small (.03), similar to findings for depressive symptoms and minor delinquency. However, Model C1 indicates that this variation is largely unaffected by contextual-level socioeconomic disadvantage. The coefficient for socioeconomic disadvantage does approach significance (p=.12), and in subsequent models we continue to investigate whether socioeconomic disadvantage explains variation in the slopes for social support. Model C2 indicates that perceiving any sub-optimal social support is associated with high violent behavior. There is a significant cross-level interaction between low social support and socioeconomic disadvantage. Significant variability in violent behavior across areas persists (τ 00=.02, p < .001), net of social support, and there is significant variability in terms of the slopes for sub-optimal support (in comparison to high support) across sampling areas.
When the individual-level risk factors are added (Model C), the impact of sub-optimal social support on violent behavior is sustained, and its effects continue to vary significantly across sampling areas. Violent behavior is positively associated with being Hispanic and African-American (compared to being NHW), as well as with being male and in the youngest age group (Model C3). There are no significant contingencies between gender and age. Living with both biological parents is negatively associated with violent behavior, and in contrast to minor delinquency, low household income is associated with high violent behavior.
Cross-Level Interactions
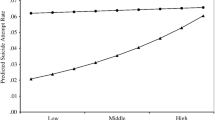
The significant cross-level interactions between social support and contextual-level socioeconomic disadvantage are illustrated in Fig. 1. For contextual-level socioeconomic disadvantage, the mean (0) plus and minus 1 standard deviation (1) is substituted into the regression equation. For age, gender, parental living arrangement, and household income, 0 is the value substituted into the regression equation.

Effects of individual-level social support on the association between adolescent mental health and contextual-level socioeconomic disadvantage (Cross-Level Interactions).
As shown in Fig. 1A, depressive symptoms for teens perceiving sub-optimal social support are the highest, somewhat irrespective of sampling area socioeconomic disadvantage. However, among teens perceiving high support, depressive symptoms are higher in the most disadvantaged areas, compared to the least disadvantaged areas. In the least disadvantaged areas, depressive symptoms are much more distinguishable between high and both low-medium and low-support adolescents. Thus, high support is emotionally protective in socioeconomically advantaged areas, but confers less mental health benefit in disadvantaged areas.
As shown in Fig. 1B, similar to depressive symptoms, minor delinquency is progressively lower for teens perceiving low, low-medium, medium-high, and high support, respectively. However, delinquency is lower in disadvantaged areas compared to advantaged areas. In addition, the effect of support on delinquency varies considerably by socioeconomic disadvantage at the sampling area-level. Among teens living in high disadvantaged areas, social support has a noticeable but slight impact on minor delinquency. Among those living in low disadvantaged areas, support has a sizable impact on delinquency, with those perceiving low support reporting the most delinquency and those perceiving high support reporting much lower delinquency. In fact, teens with high support who live in the most advantaged areas are very similar on delinquency to teens with low support who live in the most disadvantaged areas. Thus, social support confers more benefit in areas of low disadvantage than in areas of high disadvantage.
Figure 1C illustrates the conditional impact of social support and socioeconomic disadvantage on violent behavior. As discussed above, only adolescents perceiving low social support significantly differ from those perceiving high social support. Among those perceiving low support, violent behavior varies only slightly across areas of different socioeconomic disadvantage. However, among those perceiving high support, socioeconomic disadvantage bears a noticeable impact: Violent behavior increases as socioeconomic disadvantage increases. Violent behavior is lowest among adolescents who live in advantaged areas and perceive high support, but high support is less protective for those who live in the most disadvantaged areas.
DISCUSSION
Findings from this research indicate that social context matters to adolescent mental health: High contextual-level socioeconomic disadvantage is significantly associated with high depressive symptomatology and low levels of minor delinquency. The main effect of disadvantage on adolescent violent behavior approaches significance. Perceived social support is protective for each mental health outcome in this sample and the impact of contextual-level socioeconomic disadvantage on mental health is contingent upon levels of support. In addition, the impact of social support varies randomly across geographical areas, further highlighting the mental health importance of social context. All of these associations are sustained after controlling for other individual-level risk factors, the effects of which are somewhat variable across mental health outcomes. Our findings support the ecological model, as opposed to the structural model, because the effects of contextual-level socioeconomic disadvantage are not simply additive across individuals. Rather, these effects vary across individuals who perceive different amounts of social support. That is, the structural model falls short of characterizing the observed pattern of associations because it shows only the main effect of disadvantage for most adolescents, not its conditional impact.
The finding that contextual-level socioeconomic disadvantage is positively associated with depressive symptoms, negatively associated with minor delinquency, and not directly associated with violent behavior highlights the importance of assessing both internalizing and externalizing problems when examining adolescent mental health. In addition, partitioning out the impact of socioeconomic context on competing forms of externalization indicates that there is no consistent “across the board” mental health effect of either individual- or contextual-level disadvantage on problem behavior. The divergent manner in which disadvantage at both of these levels impacts minor delinquency and violent behavior suggests that combining these two constructs, as is common in the field, may be problematic. The true externalizing impact of SES may be obfuscated if separate components of a composite measure effectively cancel each other out.
Our findings indicating that minor delinquency is more prevalent in areas of socioeconomic advantage than disadvantage, especially among teens perceiving low levels of social support, was somewhat unexpected. The finding that household income is also positively associated with minor delinquency drives home the point that this type of problem behavior is not necessarily a byproduct of economic disadvantage. Additional research is needed to more fully understand the nature of these associations. It may be, for example, that social norms or acculturation differentially influence the likelihood of minor delinquency across areas. Advantaged teens living in affluent areas may perceive fewer repercussions for engaging in these types of delinquent activities, where such behaviors may be minimized or characterized as “rebellious.” Conversely, teens living in disadvantaged areas may be all too aware of the punitive consequences of any such activities because they are more likely to be labeled as criminal or illegal, perhaps as a form of social control. Social support is particularly effective at offsetting minor delinquency in areas of socioeconomic advantage, suggesting that mental health interventions promoting the development of support networks may be especially successful in these areas.
Clearly, social support is protective of both internalizing and externalizing problems among adolescents and the development of supportive relationships should be promoted by health care professionals, educators, and parents (see U.S. Public Health Service, Report of the Surgeon General's Conference on Children's Mental Health, 2000). Yet it is generally the adolescents living in advantaged areas that appear to garner the most mental health benefit from high support. This is not to say that social support is in any way detrimental in disadvantaged areas, but support appears to be more successful at offsetting poor mental health outcomes in the more advantaged areas. Thus, in areas of socioeconomic disadvantage, mental health interventions that focus too heavily on developing support networks may face special challenges if they are to be successful because the benefits of social support may be attenuated in these areas. Net of aiming to improve the actual conditions in disadvantaged communities, a worthy, but lofty goal rife with challenges (Heymann and Fischer, 2003), interventionists could aim to foster, in essence, a protective internal environment for adolescents faced with a threatening external environment.
In terms of the individual-level risk factors analyzed, our original hypotheses are generally supported, although no single “poor mental health risk typology” emerges among these adolescents. Interventions that are age and gender-specific and tailored to the cultural needs of Hispanic and African-American teens may be particularly helpful, as may be those targeting teens living in single parent or reconstituted households. For example, older females are especially vulnerable to depressive symptoms, whereas younger teens and males are at high risk for externalizing problems, indicating divergent mental health needs. Ethnic minority teens would most likely benefit from mental health programs that take into consideration cultural variation in experiences of stigma, discrimination, and other such factors that distinguish their life experiences from those of non-Hispanic White teens. Similarly, a systematic understanding of family dynamics that characterize non-nuclear family households should be an integral part of any interventions aimed at ameliorating adolescent distress. Thus, the mental health effects of these factors, in particular, represent clear targets for intervention, but other unmeasured contextual factors appear to be driving much of the mental health impact of living in areas of high disadvantage. Future research should be directed at uncovering these factors.
There are limitations to our analyses to acknowledge. First, the sample is school-based and findings cannot be generalized to adolescents who are not in school. Second, selection effects related to unique characteristics of adolescents who reside in certain residential areas may have impacted results, although it is the parent who selects a residence, not the adolescent. Third, the potential for under-reporting of externalizing problems due to sensitivity or illegality exists, although these questions were administered with audio-CASI and were not interviewer-administered thus lessening social desirability reporting. And fourth, the cross-sectional nature of the analyses limits inferences about the direction of causal associations.
Still, these findings are of unique public health relevance because they highlight the fact that socioeconomic characteristics of a rather large geographic unit (the sampling area) do distinctively contribute to adolescent mental health, whether operationalized as internality or externality, and that adolescents’ perceptions of social support affect how this contribution is patterned. The good news is that social support confers mental health benefits to all adolescents across all socioeconomic contexts. Less encouraging is the finding that social support is more consequential in advantaged areas, compared to disadvantaged areas, where it seems that high support is most needed. Interventions aimed at alleviating adolescent psychological distress should systematically account for the socioeconomic characteristics of the communities in which they reside, in addition to individual- and family-level processes. The widespread individualization of risk is somewhat inappropriate because social contexts may override adolescents’ own psychosocial resources, and expecting youth to be able to counter multilevel risk factors in isolation from their environment is a misconception.
REFERENCES
Adler, N. E., Boyce, T., Chesney, M. A., Cohen, S., Folkman, S., Kahn, R. L., and Syme, S. L. (1994). Socioeconomic status and health. Am. Psychol. 49: 15–24.
Anderson, N. B., and Armstead, C. A. (1995). Toward understanding the association of socioeconomic status and health: A new challenge for the biopsychosocial approach. Psychosom. Med. 57: 213–225.
Aneshensel, C. S., Rutter, C. M., and Lachenbruch, P. A. (1991). Social structure, stress, and mental health: Competing conceptual and analytic models. Am. Sociol. Rev. 56: 166–178.
Aneshensel, C. S. (1992). Social stress: Theory and research. Annu. Rev. Sociol. 18: 15–38.
Aneshensel, C. S., and Sucoff, C. A. (1996). The neighborhood context of adolescent mental health: Competing conceptual and analytic models. Am. Sociol. Rev. 56: 166–178.
Bearman, P. S., Jones, J., and Udry, J. R. (2005). The National Longitudinal Study of Adolescent Health: Research Design. Available at: http://www.cpc.unc.edu/addhealth. Accessed January 5.
Beyers, J. M., Loeber, R., Wikstrom, P. H., and Stouthamer-Loeber, M. (2001). What predicts violence in better-off neighborhoods? J. Abnorm. Child Psychol. 29: 369–381.
Beyers, J. M., Bates, J. E., Pettit, G. S., and Dodge, K. A. (2003). Neighborhood structure, parenting processes, and the development of youths’ externalizing behaviors: A multilevel analysis. Am. J. Community. Psychol. 31: 35–53.
Broidy, L. M., Nagin, D. S., Tremblay, R. E., Bates, J. E., Brame, B., Dodge, K. A., Fergusson, D., Horwood, J. L., Loeber, R., Laird, R., Lynam, D. R., Moffitt, T. E., Pettit, G. S., and Vitaro, F. (2003). Developmental trajectories of childhood disruptive behaviors and adolescent delinquency: A six-site, cross-national study. Dev. Psychol. 39: 222–245.
Brooks-Gunn, J., Duncan, G. J., Klebanov, P. K., and Sealand, N. (1993). Do neighborhoods influence child and adolescent development? AJS 99: 353–395.
Cornwell, B. (2003). The dynamic properties of social support: Decay, growth, and staticity, and their effects on adolescent depression. Soc. Forces 81: 953–978.
Costello, E. J., Compton, S. N., Gordon, K., and Angold, A. (2003). Relationship between poverty and psychopathology: A natural experiment. JAMA 290: 2023–2029.
Crane, J. (1991). The epidemic theory of ghettos and neighborhood effects on dropping out and teenage childbearing. AJS 96: 1126–1159.
Cryanoski, J. J., Frank, E., Young, E., and Shear, M. K. (2000). Adolescent onset of the gender difference in lifetime rates of major depression. Arch. Gen. Psychiatry 57: 21–27.
Dornbusch, S. M., Mont-Reynaud, R., Ritter, P. L., Chen, Z., and Steinberg, L. (1991). Stressful life events and their correlates among adolescents of diverse backgrounds. In Colton, M. E., and Gore, S. (eds.), Adolescent Stress: Causes and Consequences. Aldine de Gruyter, New York, pp. 111–130.
Dunkel-Schetter, C., and Bennett, T. L. (1990). Differentiating the cognitive and behavioral aspects of social support. In Sarason, B. R., Sarason, I. G., and Pierce, G. R. (eds.), Social Support: An Interactional View. Wiley, Oxford, England, pp. 267–296.
Eamon, M. K. (2002). Influences and mediators of the effect of poverty on young adolescent depressive symptoms. J. Youth Adolesc. 3: 231–242.
Ellickson, P. L., and McGuigan, K. A. (2000). Early predictors of adolescent violence. Am. J. Public Health 90: 566–572.
Faris, R. E. L., and Dunham, H. W. (1960/1939). Mental Disorder in Urban Areas. Hafner Publishing Company, New York.
Garrison, C. Z., Schluchter, M. D., Schoenbach, V. J., and Kaplan, B. K. (1989). Epidemiology of depressive symptoms in young adolescents. J. Am. Acad. Child Adolesc. Psychiatry 28: 343–351.
Gerard, J. M., and Buehler, C. (2004). Cumulative environmental risk and youth problem behavior. J. Marriage Fam. 66: 702–720.
Goodman, E., Huang, B., Wade, T. J., and Kahn, R. S. (2003). A multilevel analysis of the relation of socioeconomic status to adolescent depressive symptoms: Does school context matter? J. Pediat. October, 451–456.
Gore, S., Aseltien, R. H., and Colton, M. E. (1992). Social structure, life stress and depressive symptoms in a high school-aged population. J. Health Soc. Behav. 33: 97–113.
Hammack, P., Robinson, W. L., Crawford, I., and Li, S. T. (2004). Poverty and depressed mood in urban African-American adolescents: A family stress perspective. J. Child Fam Stud. 13: 309–323.
Heimer, K. (1997). Socioeconomic status, subcultural definitions, and violent delinquency. Soc. Forces 75: 799–833.
Heymann, J., and Fischer, A. (2003). Neighborhoods, health research, and its relevance to public policy. In Kawachi, I., Berkman, L. F. (eds.), Neighborhoods and Health. Oxford University Press, New York, NY, pp. 335–347.
Hoffman, J. P. (2003). A contextual analysis of differential association, social control, and strain theories of delinquency. Soc. Forces 81: 753–785.
Jessor, R. (1992). Risk behavior in adolescence: A psychosocial framework for understanding and action. In Rogers, D. E., and Ginzburg, E. (eds.), Adolescents at Risk: Medical and Social Perspectives. Westview Press, Boulder, CO, pp. 19–34.
Jessor, R. (1993). Successful adolescent development among youth in high-risk settings. Am. Psychol. 48: 117–126.
Kaltiala-Heino, R., Rimpela, M., Rantanen, P., and Laippala, P. (2001). Adolescent depression: The role of discontinuities in life course and social support. J. Affect. Disord. 64: 155–166.
Kessler, R. C., and Walters, E. E. (1998). Epidemiology of DSM-III-R major depression and minor depression among adolescents and young adults in the National Comorbidity Survey. Depress. Anxiety. 7: 3–14.
Kreppner, K., and Lerner, R. (1989). Family systems and the life span development: Issues and perspectives. In Kreppner, K., and Lerner, R. (eds.), Family Systems and Life-Span Development. Lawrence Erlbaum Associates, Hillsdale, New Jersey, pp. 1–13.
Leventhal, T., Brooks-Gunn, J. (2000). The neighborhoods they live in: The effects of neighborhood residence on child and adolescent outcomes. Psychol. Bull. 126: 309–337.
Leventhal, T., and Brooks-Gunn, J. (2003). Moving to opportunity: An experimental study of neighborhood effects on mental health. Am. J. Public Health 93: 1576–1582.
Lewinsohn, P. M., Rohde, P., and Seeley, J. R. (1998). Major depressive disorder in older adolescents: prevalence, risk factors, and clinical implications. Clin. Psychol. Rev. 18: 765–794.
Marcotte, G., Marcotte, D., and Bouffard, T. (2002). The influence of familial support and dysfunctional attitudes on depression and delinquency in an adolescent population. Eur. J. Psychol. Educ. XVII: 363–376.
McClanahan, S. S., and Casper, L. (1995). Growing diversity and inequality in the American family. In Farley, R. (ed.), State of the Union: America in the 1990s. Russell Sage, New York.
Massey, D. S., and Denton, N. A. (1993). American Apartheid: Segregation and the Making of the Underclass. Harvard University Press, Cambridge, MA.
Nolen-Hoeksema, S., and Girgus, J. S. (1994). The emergence of gender differences in depression during adolescence. Psychol. Bull., 115: 424–443.
Overbeek, G., Vollebergh, W., Meeus, W., Engels, R., and Luijpers, E. (2001). Course, co-occurrence, and longitudinal associations of emotional disturbance and delinquency from adolescence to young adulthood: A six-year three-wave study. J. Youth Adolesc. 30: 401–426.
Pearlin, L. I. (1989). The sociological study of stress. J. Health Soc. Behav. 30: 241–256.
Peterson, A. C., Compas, B. E., Brooks-Gunn, J., Stemmler, M., and Grant, K. E. (1993). Depression in adolescence. Am. Psychol. 48: 155–168.
Radloff, L. S. (1977). The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psych. Meas. 1: 385–401.
Rankin, J. H., and Kern, R. (1994). Parental attachments and delinquency. Criminology 32: 495–515.
Raudenbush, S. W., Bryk, A. S., Cheong, Y. F., and Congdon, R. T. (2000). Hierarchical Linear and Nonlinear Modeling. Scientific Software International, Lincolnwood, IL.
Resnick, M. D., Bearman, P. S., Blum, R. W., Bauman, K. E., Harris, K. M., Jones, J., Tabor, J., Beuhring, T., Sieving, E. E., Shew, M., Ireland, M., Bearinger, L. H., and Udry, J. R. (1997). Protecting adolescents from harm: Findings from the National Longitudinal Study of Adolescent Health. JAMA 278: 823–832.
Rushton, J. L., Forcier, M., and Schectman, R. M. (2002). Epidemiology of depressive symptoms in the National Longitudinal Study of Adolescent Health. J. Am. Acad. Child Adolesc. Psychiatry 41: 199–105.
Sampson, R. J., Morenoff, J. D., and Gannon-Rowley, T. G. (2002). Assessing “neighborhood effects”: Social processes and new directions in research. Annu. Rev. Sociol. 28: 443–478.
Sampson, R. J., Morenoff, J. D., and Raudenbush, S. (2005). Social anatomy of racial and ethnic disparities in violence. Am. J. Public Health 95: 224–232.
Schraedley, P. K., Gotlib, I. H., and Hayward, C. (1999). Gender differences in correlates of depressive symptoms in adolescents. J. Youth Adolesc. 25: 98–108.
Sheeber, L., Hops, H., Alpert, A., Davis, B., and Andrews, J. (1997). Family support and conflict: Prospective relations to adolescent depression. J. Abnorm. Child Psychol. 25: 333–344.
Stice, E., Ragan, J., and Randall, P. (2004). Prospective relations between social support and depression: Differential direction of effects for parent and peer support? J. Abnorm. Psychol. 113: 155–159.
Taylor, S. E., Repetti, R. L., and Seeman, T. (1997). Health psychology: What is an unhealthy environment and how does it get under the skin? Annu. Rev. Psychol. 48: 411–447.
Thoits, P. A. (1995). Stress, coping, and social support processes: Where are we? What next? J. Health Soc. Behav. extra issue: 53–79.
Turner, R. J., and Turner, J. B. (1999). Social integration and support. In Aneshensel, C. S., and Phelan, J. C. (eds.), Handbook of the Sociology of Mental Health. Kluwer Academic/Plenum Publishers, New York, NY, pp. 301–320.
U.S. Public Health Service (2000). Report of the Surgeon General's Conference on Children's Mental Health: A National Action Agenda. Department of Health and Human Services, Washington, D.C.
U.S. Census Bureau. (2005). Income Improves, Poverty Levels Stabilize, Health Insurance Coverage Slips, Census Bureau Reports. Available at: http://www.census.gov/Press-Release/cb97-162.html. Accessed January 5.
Wheaton, B., and Clarke, P. (2003). Space meets time: Integrating temporal and contextual influences on mental health in early adulthood. Am. Sociol. Rev. 68: 680–706.
Wickrama, K. A. S., and Chalandra, M. B. (2003). Community context of social resources and adolescent mental health. J. Marriage Fam. 65: 850–866.
Wiesner, M., & Windle, M. (2004). Assessing covariates of adolescent delinquency trajectories: A latent growth mixture modeling approach. J. Youth and Adolescence 33: 431--442.
Wight, R. G., Sepulveda, J. E., and Aneshensel, C. S. (2003). Depressive symptoms: How do adolescents compare with adults? J. Adolesc. Health 34: 314–323.
Wight, R. G., Aneshensel, C. S., Botticello, A. L., and Sepulveda, J. E. (2005). A multilevel analysis of ethnic variation in depressive symptoms among adolescents in the United States. Soc. Sci. Med. 60: 2073–2084.
Williams, D. R., and Collins, C. (1995). U.S. socioeconomic and racial differences in health: Patterns and explanations. Annu. Rev. Sociol. 21: 349–386.
Wilson, W. J. (1987). The Truly Disadvantaged: The Inner City the Underclass and Public Policy. University of Chicago Press, Chicago.
Wilson, W. J. (1991). Studying inner-city social dislocations: The challenge of public agenda research. American Sociological Review 56: 1–14.
ACKNOWLEDGMENTS
This research was supported by a grant from the National Institute of Mental Health (R01 MH 60923, Carol S. Aneshensel, PhD, Principal Investigator). This research uses data from the Add Health project, a program project designed by J. Richard Udry (PI) and Peter Bearman, and funded by grant P01-HD31921 from the National Institute of Child Health and Human Development to the Carolina Population Center, University of North Carolina at Chapel Hill, with cooperative funding from 17 other agencies. Persons interested in obtaining data files from the National Longitudinal Study of Adolescent Health should contact Add Health, Carolina Population Center, 123 West Franklin Street, Chapel Hill, NC 27516-2524 (http://www.cpc.unc.edu/addhalth).
Author information
Authors and Affiliations
Corresponding author
Additional information
Richard G. Wight, Assistant Research Sociologist, conducts life course mental health research in the UCLA Department of Community Health Sciences. His work emphasizes the intersection of individual- and contextual-level factors that impact health within dyads, families, and neighborhoods.
Amanda L. Botticello is a doctoral student in the UCLA Department of Community Health Sciences, where her work addresses the reciprocal relationships between depressive symptoms and problem drinking among adolescents.
Carol S. Aneshensel is a Professor of Community Health Sciences at UCLA, where she applies principals of social stratification and life course theory to the analysis of quantitative data to better understand disparities in mental health risks.
Rights and permissions
About this article
Cite this article
Wight, R.G., Botticello, A.L. & Aneshensel, C.S. Socioeconomic Context, Social Support, and Adolescent Mental Health: A Multilevel Investigation. J Youth Adolescence 35, 109–120 (2006). https://doi.org/10.1007/s10964-005-9009-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-005-9009-2