
Abstract
Nonsuicidal self-injury (NSSI) is a serious public health concern among adolescents. Identifying risk factors of NSSI is important to effectively prevent or reduce such behavior. Child maltreatment is one of the most widely recognized risk factors for NSSI. How child maltreatment and NSSI is related, however, is still unclear. The present study tested the temporal relationship between physical and emotional abuse and NSSI, with distress intolerance as the potential mediator. Potential gender differences on these associations were also tested. We assessed all study variables among 2259 Chinese adolescents (53.8% females; Mage = 15.11 years, SD = 1.57) for three times at 6-month intervals. The results showed that distress intolerance only mediated the relationship between emotional abuse and NSSI, but not between physical abuse and NSSI. In addition, this mediation effect of distress intolerance was significant only for females. The findings of this study can help researchers and practitioners understand pathways by which child maltreatment impacts adolescent NSSI. Implications for preventions and interventions of NSSI were discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Adolescence, defined as the stage of growth between 10 and 19 years of age (World Health Organization 2018), is not only the crucial phase of physical maturation and psychological development, but also the peak of the occurrence of mental disorders (Lerner and Steinberg 2009). Nonsuicidal self-injury (NSSI), defined in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) as the direct and deliberate bodily harm in the absence of suicidal intent (American Psychiatric Association 2013), is a major public health concern among adolescents. Lifetime prevalence estimates suggest that approximately 18% of community adolescents have engaged in NSSI (Muehlenkamp et al. 2012; Plener et al. 2015). In inpatient settings, over 40% of adolescents suffer from NSSI. The high incidence of NSSI during adolescence has also become a public health concern in China. A national meta-analysis shows the 12-month prevalence of NSSI among Chinese adolescents is 29% (Tang et al. 2018). In addition, this behavior is accompanied by various psychiatric disorders, such as borderline personality disorder, substance use, and depression, and acts as a robust risk factor for future suicidal behaviors (Nock 2010; You and Lin 2015). Given the prevalence and clinical significance of NSSI among adolescents, identifying risk factors for NSSI is important to effectively prevent such behavior. Extant models of NSSI emphasize the roles of both distal environmental and proximal intrapersonal risk factors in the development and maintenance of this behavior (Nock 2010; Yates 2004). In the current study, we investigated two potential risk factors for adolescent NSSI: one environmental factor of child maltreatment and one intrapersonal factor of distress intolerance, with a sample of Chinese adolescents. Specifically, we examined the mediating role of distress intolerance in the relationship between child maltreatment and NSSI, as well as the potential gender differences on these associations.
Child Maltreatment and NSSI
Child maltreatment has been considered an important risk factor for NSSI. Child maltreatment has different forms including physical abuse, emotional abuse, sexual abuse, and neglect (Liu et al. 2018). Physical abuse refers to assault and harsh physical punishment; emotional abuse refers to verbal abuse, rejecting, terrorizing, abandonment, and psychological unavailability; sexual abuse refers to incest, sexual assault, and exposure to sexual activity; and neglect refers to a broad range of inadequate parental care such as failing to provide or ensure food, clothing, shelter, medical care, or education (Bolger and Patterson 2001). Two theoretical models have suggested the relationship between child maltreatment and NSSI.
According to Yates’s (2004) developmental psychopathology framework, in the process of positive self-adaptation, individuals develop critical competencies that form the foundation of subsequent adaptive functioning. These competences originate early in childhood and develop throughout one’s lifetime. Early traumatic experiences, such as child maltreatment, may undermine the development of these critical adaptive competencies. Without adaptive competencies, NSSI may develop as a maladaptive compensatory strategy to address normal and abnormal stressors and accompanying negative emotions.
Similarly, in the biosocial model explaining the development of borderline personality disorder, Linehan (1993) also emphasized the role of early childhood experiences in the development of NSSI. Particularly, she argued that the interaction between biological vulnerabilities to intense emotionality and an invalidating environment, such as being abused by parents, may result in NSSI. Common to both theories is the notion that child maltreatment may precipitate the development of NSSI.
Indeed, empirical research has provided extensive support for the risk effect of child maltreatment for NSSI. According to a recent systematic review of more than 70 studies, child maltreatment and all its subtypes (i.e., physical abuse, emotional abuse, sexual abuse, and physical neglect), except for emotional neglect, were significantly associated with NSSI across a range of age groups and populations (Liu et al. 2018). In addition, one longitudinal study demonstrated that histories of child maltreatment were predictors of subsequent NSSI (Garisch and Wilson 2015). Many cross-sectional studies aiming at investigating the mediating effects of diverse variables on the relationship between child maltreatment and NSSI also revealed their significant association, after controlling for those mediating variables (e.g., Auerbach et al. 2014; Swannell et al. 2012). These studies demonstrated that child maltreatment makes a direct contribution to the development of NSSI.
The existing literatures, however, are limited in several areas. First, the relationships between different forms of child maltreatment and NSSI are still unclear. Most studies have examined only one type of child maltreatment, which precludes the comparisons between the effects of different forms of maltreatment on NSSI across studies. In order to explore whether different forms of maltreatment play different roles in NSSI or whether some kind of maltreatment plays a more important role, we need to examine the relations between specific forms of child maltreatment and NSSI within a single study. Second, all studies investigating the specific mechanism behind the relationship between child maltreatment and NSSI used the cross-sectional design (e.g., Auerbach et al. 2014; Buser and Hackney 2012; Swannell et al. 2012). To explore their temporal relationship, as well as the potential mechanism behind this relationship, we need longitudinal studies. Taken together, further research is needed to gain more sights into the association between child maltreatment and NSSI.
The Mediating Role of Distress Intolerance
Individuals who engage in NSSI often do so years after their maltreatment experiences (Arens 2012); thus, child maltreatment may affect the development of individual characteristics that confer more proximal risks for NSSI. Some emotion-related variables, such as difficulties in emotion regulation, emotion inexpressivity, emotional coping, and alexithymia, were examined as mediators behind the relationship between child maltreatment and NSSI in previous studies (Buckholdt et al. 2009; Peh et al. 2017; Swannell et al. 2012; Thomassin et al. 2016). We believe that distress intolerance, a meta-emotion construct, may also play a role in the relationship between child maltreatment and NSSI. As compared to other emotion-related constructs, distress intolerance is a higher-order construct that consists of four aspects related to one’s inability to experience and withstand negative psychological states: “(1) tolerability and aversiveness, (2) appraisal and acceptability, (3) tendency to absorb attention and disrupt functioning, and (4) regulation of emotions, specifically, the consequent strength of action tendencies to either avoid or immediately attenuate the experience” (Simons and Gaher 2005; pp. 83, 84). Given that adolescence is a critical period for emotional development (Ahmed et al. 2015; Silvers et al. 2012), distress intolerance, which develops early in life, may emerge as a relatively stable and dispositional characteristic during adolescence (Cummings et al. 2013), and eventually result in adverse health consequences in later lives (Zvolensky and Hogan 2013). Thus, examining distress intolerance as the mediator may provide additional information for our understanding of the relationship from child maltreatment to NSSI.
With regard to the mediating role of distress intolerance, on the one hand, child maltreatment may result in distress intolerance. From the perspective of developmental psychopathology framework (Yates 2004), child maltreatment may thwart children’s development of integrative, symbolic, and reflective affect processing capacities. Additionally, according to Linehan’s (1993) biosocial model, biological irregularities combined with invalidating environments, as well as their interaction and transaction over time, may contribute to the development of emotion dysregulation and finally result in difficulties in distress tolerance. Several empirical studies have provided support for the role of child maltreatment in poor tolerance for distress. Across these studies, greater trauma severity was associated with lower perceived distress tolerance in college students (Arens et al. 2014) and clinical adults (Banducci et al. 2014; Gratz et al. 2007).
On the other hand, distress intolerance is also hypothesized to play an important role in the development and maintenance of NSSI (Tull and Aldao 2015). According to the pragmatic hypothesis of integrated theoretical model of NSSI (Nock 2010), individuals with poorer distress tolerance may be more likely to engage in NSSI because it is a rapid, effective, and pragmatic strategy to regulate and release distress. The experiential avoidance model proposed by Chapman et al. (2006) argued that NSSI is often used as an avoidance method to escape from intolerable internal experiences or distress. The emotional cascade model also suggested that individuals who engage in maladaptive behaviors, such as NSSI, do so to cope with highly intense distress resulting from the reciprocal relationship between negative affect and ruminative process (Selby et al. 2013). This relation between distress intolerance and NSSI has also been investigated empirically. For example, in a lab study, Nock and Mendes (2008) found that self-injurers displayed lower levels of distress tolerance (i.e., less capable of withstanding intense distress) than their non-self-injuring counterparts during a distressing task. Other studies also suggested that distress intolerance is positively associated with the frequency of NSSI (e.g., Anestis et al. 2014; Anestis et al. 2013a; 2013b). Moreover, a one-year follow-up study revealed that NSSI was significantly predicted by distress intolerance (Lin et al. 2017).
Building on these literatures, we proposed that distress intolerance might be an important characteristic that mediates the association between child maltreatment and NSSI. We located only one relevant study: Arens (2012) with a sample of 694 western undergraduates found that poor distress tolerance mediated the concurrent association between maltreatment and NSSI. This study was limited in several areas. First, the result of this study may not apply to adolescents, because developmental differences exist between young adults and adolescents. Second, this study did not distinguish between different types of child maltreatment. Third, this study was conducted with a western sample, but parenting style and parent-child relationship may differ across cultures. Specifically, the western culture advocates non-violent parenting, emphasizing closeness, warmth, reasoning, and negotiation in the parent-child relationship (Van Campen and Russell 2010), whereas the Chinese culture advocates filial piety, allowing parents to control and punish their children. When children make mistakes, Chinese parents often punish them by verbal abuse or physical punishment (Shen 2009). In this sense, maltreatment is relatively more accepted within Chinese society than within western society. Child maltreatment, especially emotional and physical abuses, is highly prevalent in China (Cui and Liu 2018).
Further, Chinese parents may also show different attitudes toward males and females (Xing et al. 2011). For males, strict education, such as corporal punishment, is advocated (Cui et al. 2016; Xing et al. 2011). Males are encouraged to tolerate pain and distress. But for females, liberal and protective education is advocated (Xing et al. 2011). Females are expected to tolerate less pain. Additionally, NSSI is more prevalent among females than males (Bresin and Schoenleber 2015). Thus, we proposed that there may be gender differences in the effects of child maltreatment on NSSI through distress intolerance.
The Current Study
Taken together, the temporal relationship between child maltreatment and NSSI needs to be clarified. Also, whether distress intolerance mediates these relationships and whether there are gender differences in these relationships are still questions. Based on previous developmental psychopathology theories (Linehan 1993; Yates 2004) and NSSI literatures, we assumed that abusive experiences are more likely to lead to difficulties in distress tolerance, which then increases the likelihood of engaging in NSSI. The current study was undertaken to explore this question, as no study to date had explored these temporal relationships. Thus, we hypothesized that: (a) both physical and emotional abuses would significantly and positively predict subsequent NSSI; and (b) distress intolerance would mediate the relationship between the two types of child maltreatment and NSSI. As for the gender differences, no specific hypothesis was made given that this question is exploratory.
Method
Participants
Participants were recruited from six high schools in Hong Kong and were surveyed semiannually for three times. The schools were randomly selected from the list of available schools in Hong Kong. At the baseline assessment (Wave 1), 3555students (52.0% females) participated. Thanks to the cooperation of school authorities, overall student participation rates were close to 99% in all schools. Participants aged between 12 and 19 years (Mage = 15.63 years, SD = 1.67) at baseline.
Participants were re-assessed after a 6-month (Wave 2) and a 12-month (Wave 3) interval, respectively. At the Wave 2 assessments, 2621 (53.5% females; Mage = 15.28 years, SD = 1.50) of the Wave 1 participants were retained; and at the Wave 3 assessment, 2259 (53.8% females; Mage = 15.11 years, SD = 1.57) of the Wave 1 participants were retained. The participant retention rates were 73.73% and 63.54% for the Wave 2 and Wave 3 assessments, respectively. Attrition were mainly due to students transferring to other schools and being absent from school on the day of assessment. Comparisons among participants who participated in Wave 1 assessment only, those who participated in both Wave 1 and Wave 2 assessments, and those who participated in all three assessments revealed no significant differences on all studied variables and demographic variables (ps > .05).
Procedure
Data collection was completed during regular class time with the assistance of school teachers. Before that, students’ assent to participate and parental passive informed consent were obtained. During each assessment, the same set of questionnaires was group administered in classrooms under the supervision of school personnel. At the beginning of each assessment, teachers were required to inform students that they could hand in the questionnaires whenever they wanted, and they did not need to finish all the items if they felt uncomfortable. A unique ID number for each student was created for data-matching purposes. Participants were assured of strict confidentiality of the collected data and that only research personnel had access to the questionnaires. All testing materials and the procedures were approved by the ethical board of the Chinese University of Hong Kong and the participating schools’ authorities.
Measures
Child maltreatment
The Personal Report of Childhood Abuse Scale (PRCAS; Zhu et al. 2006) is a retrospective self-report scale that includes four subscales: physical abuse, emotional abuse, sexual abuse, and neglect. In the current study, we only used physical and emotional abuse subscales of PRCAS to assess the experiences of maltreatment for the past 6 months. Four items measure physical abuse (e.g., “Did your parents ever scratch, bite, or slap you?”) and five items measure emotional abuse (e.g., “Did your parents ever belittle, laugh at, or despise you?”). Responses were made on a 5-point scale, ranging from 1 = almost never to 5 = almost always. A higher score reflects more frequent child maltreatment. The PRCAS demonstrated sufficient internal consistency and test-retest reliability over a 4-week interval. Moreover, the PRCA showed good convergent, discriminant, and criterion validity (Zhu et al. 2006). For the Wave 1 data, the Cronbach’s alpha values for the subscales of physical and emotional abuse were .82 and .87. Please note that only reliability information for the waves at which the scales were used in the current analyses is reported.
Distress Intolerance
The Distress Tolerance Scale (DTS; Simons and Gaher 2005) is a 15-item self-report questionnaire that assesses the capacity to experience and withstand negative psychological states. The DTS included four subscales: Tolerance (3 items, e.g., “I can’t handle feeling distress or upset”), Absorption (3 items, e.g., “When I feel distressed or upset, all I can think about is how bad I feel”), Appraisal (6 items, e.g., “My feeling of distress or being upset are not acceptable”), and Regulation (6 items, e.g., “I’ll do anything to stop feeling distressed or upset”). Items on DTS were rated on a 5-point scale, ranging from 1 = strongly disagree to 5 = strongly agree. A higher score on DTS indicates a lower distress tolerance ability. The total DTS and its four subscales demonstrated sufficient internal consistency and test-retest reliability over a 6-month interval. Moreover, the DTS showed good convergent, discriminant, and criterion validity among adolescents (Simons and Gaher 2005). In the present study, the DTS also showed good internal consistency. The Cronbach’s alpha values for the total scale and the subscales of Tolerance, Absorption, Appraisal, and Regulation were .95, .87, .89, .89, and .75 for the Wave 1 data, and .91, .86, .88, .88, and .74 for the Wave 2 data.
NSSI
The Nonsuicidal Self-Injury Scale is a frequency measure that assesses seven NSSI behaviors, including self-cutting, burning, biting, punching, scratching skin, inserting sharp objects to the nail or skin, and banging the head or other parts of the body against the wall. These behaviors were derived from the Revised Diagnostic Interview for Borderlines (DIB-R; Zanarini et al. 1989) and have been used in previous studies among Chinese adolescents (You and Leung 2012). At all three waves’ assessments, participants were asked, “In the past 6 months, have you engaged in the following behaviors to deliberately harm yourself, but without suicidal intent?” These items were rated on a 5-point scale, ranging from 0 = never, 1 = once, 2 = twice to five times, 3 = six times to eleven times, to 4 = twelve times or more. This scale has demonstrated sufficient concurrent and overtime validity via its relationships to other psychopathology measures (You and Leung 2012). In the current study, we classified those who have reported at least one incidence of any type of NSSI as self-injurers in the descriptive analyses and summed up scores on the seven NSSI items as an NSSI total score in model testing. This scale had a Cronbach’s alpha value of .80, .82, and .74 for Wave 1, Wave 2, and Wave 3 data, respectively.
Data analyses
First, descriptive analyses of the prevalence of NSSI were conducted. Chi-square analysis was conducted when comparing gender differences between those who had engaged in NSSI (NSSI group) and those who had not (Non-NSSI group). Bivariate correlations between all study variables were then performed separately by gender. Correlations between two continuous variables were computed by Person’s product-moment correlation. Then, skewness and kurtosis of emotional abuse, physical abuse, and NSSI total score were examined before the mediational analyses. Only the NSSI total score was significantly skewed, so we log-transformed it to reduce its skewness. All the above analyses were performed with SPSS 19.0 (Arbuckle 2010).
Second, we tested the hypothetical mediation model using Mplus Version 7.0 (Muthén and Muthén 2012). Missing data were handled with the full information maximum-likelihood estimation procedure (FIML). We also ran the analyses using listwise deletion as the sensitivity check. Model fit was assessed using a number of indexes. In the case of a large sample size, the chi-square (χ2) statistic is likely to overestimate the lack of fit and will always suggest a lack of fit (Bollen 1989). Therefore, multiple complementary fit indices were used to evaluate model fit (Hu and Bentler 1999). These indices included the comparative fit index (CFI), Tucker-Lewis index (TLI), standardized root mean square residual (SRMR), and the root mean square error of approximation (RMSEA). The cut-off criteria for a well-specified model are: CFI > .95, TLI > .95, SRMA < .06, and RMSEA < .06, and the cut-off criteria for an acceptable model are: CFI > .90, TLI > .90, SRMA < .08, and RMSEA < .08 (Browne and Cudeck 1993). To examine the mediation effect, we used the bootstrap procedure with 1000 iterations. The bootstrap method could provide estimates of both direct and indirect effects simultaneously (Preacher and Hayes 2008). For the estimate of the direct and indirect effect, the 95% bias-corrected (BC) confidence interval (CI) excluding zero indicates the significance of the mediational pathways.
Finally, in order to test the gender differences in the hypothesized model, we conducted a series of multiple group analysis following three steps (Arbuckle 1997). At Step 1, we tested the model fit separately in females and in males. At Step 2, we combined the samples of both genders and tested the model fit in the combined sample with all paths being freely estimated in each sample. The χ2 statistic and its corresponding degree of freedom (df) yielded from the model at Step 2 served as the basis for the following model comparisons. At Step 3, we constrained each of the model paths to be equal across genders one by one and compared each of the resulted χ2 and its df with the ones yielded at Step 2. A significant chi-square difference statistic (∆χ2) and its corresponding degrees of freedom (∆df) indicate a significant difference in that particular path across genders.
Results
Descriptive Analyses
In the current sample, the proportion of adolescents reporting having engaged in NSSI was 13.8% (n = 246) at Wave 1, 12.4% (n = 211) at Wave 2, and 11.5% (n = 190) at Wave 3. Females were more likely than males to engage in NSSI at Wave 1 (16.6%, n = 163% vs. 10.4%, n = 83; χ2[1, N = 2259] = 14.40, p < .001), at Wave 2 (14.4%, n = 135% vs. 9.9%, n = 76; χ2[1, N = 2259] = 7.777, p < .01), and at Wave 3 (13.7%, n = 127% vs. 8.7% n = 63; χ2[1, N = 2259] = 9.88, p < .01). Among the participants engaging in NSSI, cutting was the most prevalent method (n = 152, 61.8% at Wave 1; n = 138, 65.4% at Wave 2; and n = 126, 66.3% at Wave 3). In addition, 50.4 % (n = 124) of self-injurers at Wave 1, 44.1 % (n = 93) at Wave 2, and 42.6 % (n = 81) at Wave 3 reported using only one method, and 49.6 % (n = 122) of self-injurers at Wave 1, 55.9 % (n = 118) at Wave 2, and 57.4 % (n = 109) at Wave 3 reported using more than one method. As for the child maltreatment, the prevalence of physical and emotional abuse at Wave 1 was 32.2% (n = 723) and 52.2% (n = 1180), respectively. Gender differences were not significant on physical abuse (male: 33.8%, n = 350 vs. female: 30.8%, n = 373; χ2[1, N = 2259] = 2.19, p = .14) or emotional abuse (male: 52.7%, n = 548 vs. female: 52.5%, n = 632; χ2[1, N = 2259] = .01, p = .91).
Table 1 presents the means and standard deviations of all study variables, as well as the bivariate correlations between them separately by gender. Except for Wave 1 physical abuse, Wave 1 emotional abuse, and Wave 1 regulation that were not significantly related to Wave 3 NSSI among males, all the other variables were significantly and positively associated with NSSI at all three waves for both genders (ps < .01). This pattern of correlations provided an initial support for the hypothesized mediation process.
Mediation Analyses
Before we tested the mediation model, the direct effects of physical and emotional abuse on NSSI were first examined without distress intolerance in the model. The results indicated that subsequent NSSI was significantly predicted by emotional abuse (β = .10, p < .01), but not by physical abuse (β = .11, p > .05).
Then, we examined the longitudinal mediation model with Wave 1 physical abuse and emotional abuse as predicting variables, Wave 2 distress intolerance as the latent mediators with four indicators: regulation, tolerance, appraisal, and absorption, and Wave 3 NSSI as the outcome variable. Age, participating schools (the six schools were coded as five dummy variables)Footnote 1, Wave 1 distress intolerance, Wave 1 NSSI, and Wave 2 NSSI served as controls variables. The mediation model demonstrated a good fitFootnote 2, χ2(N = 2259) = 372.37, df = 106, p < .001, CFI = .99, TLI = .98, SRMR = .02, and RMSEA = .06. As for individual paths, the direct paths from Wave 1 physical abuse (β = −.01, p = .87) and Wave 1 emotional abuse (β = −.01, p = .83) to Wave 3 NSSI were both non-significant. The path from Wave 1 emotional abuse to Wave 2 distress intolerance (β = .07, p < .05) and the path from Wave 2 distress intolerance to Wave 3 NSSI (β = .04, p < .05) were both significant; whereas the path from Wave 1 physical abuse to Wave 2 distress intolerance (β = .01, p = .84) was non-significant. The bootstrap procedure revealed a significant indirect effect with distress intolerance as a mediator between emotional abuse and NSSI (β = .003, SE = .002, BC 95% CI [.001, .010], p = .02), but not between physical abuse and NSSI (β = .001, SE = .002, BC 95% CI [−.003, .004], p = .86). This suggests that distress intolerance only mediated the relationship between emotional abuse and NSSI, but not between physical abuse and NSSI. The whole model accounted for 70.8% of the total variance in Wave 3 NSSI.
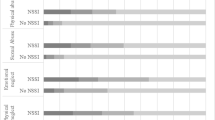
Finally, we examined gender differences in our model. At Step 1, the model fit the data well in females (χ2 = 218.73, df = 87, p < .001, CFI = .99, TLI = .98, SRMR = .02, and RMSEA = .06) and in males (χ2 = 203.28, df = 87, p < .001, CFI = .98, TLI = .98, SRMR = .02, and RMSEA = .04)Footnote 3. The standardized path coefficients for the model are presented separately by gender in Fig. 1. All the paths were non-significant (ps > .05) in males, suggesting that both direct and indirect effects of physical abuse and emotional abuse on NSSI were non-significant in males. In females, both the direct paths from Wave 1 physical abuse and Wave 1 emotional abuse to Wave 3 NSSI were non-significant (ps > .05). Both the paths from Wave 1 emotional abuse to Wave 2 distress intolerance and from Wave 2 distress intolerance to Wave 3 NSSI were significant (ps < .01), whereas the path from Wave 1 physical abuse to Wave 2 distress intolerance was non-significant (p > .05). The bootstrap procedure revealed a significant indirect effect with distress intolerance as a mediator between emotional abuse and NSSI (β = .005, SE = .004, BC 95% CI [.001, .016], p = .02), but not between physical abuse and NSSI (β = −.001, SE = .002, BC 95% CI [−.007, .002], p = .54). The whole model accounted for 65.8% of the total variance in Wave 3 NSSI. Since the direct and indirect effects of physical and emotional abuse on NSSI were all non-significant in males, there is no need for further testing of gender differences. Thus, we didn’t conduct Step 2 and Step 3 of the gender difference analyses.

Standardized Path Coefficients for the Longitudinal Mediation Models of NSSI with emotional and physical abuse as predictor variables. REG the regulation subscale for the DTS; TOL the tolerance subscale for the DTS; APP the appraisal subscale for the DTS; ABS the absorption subscale for the DTS; NSSI nonsuicidal self-injury. The subscriptions indicate the assessment waves. Standardized path coefficients for females are presented on the left, and data for males are present on the right. Significant paths are depicted with black lines and non-significant paths are depicted with gray lines. The path coefficients that are significant are presented with asterisks, and the path coefficients that are not significant are presented without asterisks. To avoid confusion, control variables were not shown. **p < .01; ***p < .001
Discussion
NSSI is a serious public health concern that can result in many negative consequences among adolescents. Identifying risk factors of NSSI is important to effectively prevent or reduce such behavior. Researchers have developed models that emphasize the role of child maltreatment in developing and maintaining NSSI. The developmental psychopathology framework and the biosocial theory provide excellent explanatory frameworks for understanding NSSI in this context (Linehan 1993; Yates 2004). Many studies investigating the relationship between child maltreatment and NSSI, however, are cross-sectional, and the potential mechanism behind the association is still unclear. Given the negative effects of child maltreatment on psychological development (Jaffee 2017), the influence of child maltreatment on NSSI should be further explored, as well as explanatory variables for this relationship. The purpose of the current study was to explore the temporal relationship between child maltreatment and NSSI, with distress intolerance as the potential mediator. We also examined potential gender differences on these associations among Chinese adolescents.
The first finding of our study was that only emotional abuse was indirectly related to NSSI through distress intolerance. The developmental psychopathology model (Yates 2004) and the biosocial model (Linehan 1993) have provided similar explanations to this finding. Both models emphasize the importance of family environment on the development of adolescents. In warm, tolerant, and harmonious families, parents provide sensitive and empathic responses to children’ emotions. Children may then believe that emotions can be shareable and tolerable. In contrast, in families with emotional abuse, parents chronically neglect and invalidate children’ emotions, especially negative emotions. Also in Chinese families, remarks or behaviors that may be regarded as emotional abuse, such as threat, terrorism, criticism, and humiliation, directed at children by parents, are common phenomena (Glaser 2002). As such, Chinese children may on the one hand frequently experience intense negative emotions, and on the other hand fail to express these feelings appropriately or to develop adaptive emotion regulation skills. Eventually, these children may become unable to tolerate overwhelming distress, and tend to use quick, effortless, and impulsive strategies, such as NSSI, to avoid intense negative emotional states (Lin et al. 2017; Nock and Mendes 2008).
It is noteworthy that our finding is inconsistent with Arens’s (2012) study, in which distress intolerance did not mediate the relationship between child maltreatment and NSSI. One reason for the inconsistency may be the measurement differences of child maltreatment. The Arens’s study treated child maltreatment as a latent variable with three indicators: sexual abuse, punishment, and neglect, while our study treated emotional abuse and physical abuse as two separate predictors. In Arens’s study, the significant effect of one specific form of child maltreatment on NSSI may be offset by the non-significant effects of others. Another possible reason may be that the sample of Arens’s study was adults, while the sample of our study was adolescents. Adolescence is a critical period for emotional development, especially the development of emotion regulation strategies and abilities (Ahmen et al. 2015; Silvers et al. 2012). As compared to those of adults, emotional regulation strategies of adolescents, especially of adolescents with abusive experiences, are deficient. Adolescents with abusive experiences are not only more prone to experience emotional distress, but also more likely to use maladaptive strategies to release distress than adults (Silvers et al. 2012).
As for the gender differences, we found that distress intolerance played a mediating role in the relationship between emotional abuse and NSSI only in females, but not in males. This pattern of gender difference is in line with the result of another Chinese study (Chen et al. 2017). This finding may be explained in the Chinese cultural context. In China, different role expectations exist across genders. Compared to females, males are expected to undertake more responsibilities and bear more pressures from family and society (Cui et al. 2016; Xing et al. 2011). Even making the same mistake, males may suffer more criticism and blame than females. Eventually, males may develop higher distress tolerance abilities than females (Cui et al. 2016). In addition, this gender difference may also be accounted for by differences in biological and psychosocial vulnerabilities across genders. Specifically, females are more sensitive to social relationship stress and are more likely to have intensified emotional reactivity than males (Lewis et al. 2015; Nolen-Hoeksema 2012). Thus, in the face of frequent insults, threats, and ridicules from parents, females may feel more intolerant of distress and are more likely to engage in NSSI as a fast and convenient emotion regulation method.
There were several limitations of the present study. First, the generalizability of the findings is limited by the inclusion of only Chinese adolescents in Hong Kong. Future studies should help elucidate whether these results are replicable among adolescents in clinical or other cultural samples. Second, due to shared method variance, the use of self-report data may inflate the associations among variables. Future research will benefit from including interview and/or observational data to reduce the influence of shared method variance. Third, we only examined the effects of physical and emotional abuses on NSSI. Future studies should use all types of child maltreatment to explore whether and why some types of abuse, but not others, are related to the engagement in NSSI. Finally, given that students were nested within schools, using a multilevel framework to examine adolescents within schools may provide important information. But in this study, we did not include any school level variable that is necessary for constructing a hierarchical linear model.
Conclusion
This study represents an important contribution to the literature. Theoretically, this is the first study to examine the temporal relationship between child maltreatment, distress intolerance, and NSSI among Chinese adolescents. This study may help us obtain a more thorough understanding of NSSI from a developmental perspective. Moreover, certain findings from the current longitudinal study are not consistent with those from cross-sectional ones, suggesting that some NSSI risk factors identified from cross-sectional studies may need to be re-examined in longitudinal research.
From a clinical standpoint, the finding that emotional abuse contributes the unique risk for NSSI above and beyond physical abuse and previous NSSI underscores the need for greater consideration of emotional abuse in the evaluation of risk for NSSI, particularly in community settings. Additionally, the study also highlights the importance of the mediational role of distress intolerance. Although the mediating effect is only significant in females, those who have difficulties in distress tolerance are at a particularly high risk for NSSI. From an emotion regulation perspective, we can regard distress intolerance as a transdiagnostic factor to the prevention and treatment of NSSI. Further, gender differences revealed in this study may shed light on the identification of female self-injurers, as well as on the development of NSSI prevention programs. Specifically, in order to decrease the prevalence of NSSI in female adolescents, it may be necessary to help them reduce emotional abuse, increase the ability to tolerate emotional distress, and learn effective emotion regulation strategies.
Notes
The differences in NSSI frequency across the six schools were non-significant at Wave 1 (F [5, 2259] = .59, p > .05), but were significant at Wave 2 (F [5, 2259] = 4.98, p < .001) and Wave 3 (F [5, 2259] = 5.19, p < .001).
The model using listwise deletion also demonstrated an acceptable fit, χ2(N = 2210) = 581.37, df =, p < .001, CFI = .98, TLI = .97, SRMR = .02, and RMSEA = .06. The significance pattern of the individual paths in the model using listwise deletion was the same as that in the model using full information maximum-likelihood for missing data. Thus, we reported only the results of the mean substitution model. Interested readers may contact the correspondence author for the results of the listwise deletion model.
The multi-group analyses using listwise deletion for dealing with missing data yielded the same pattern of results. Thus, we did not present the results of the listwise deletion analyses. Interested readers may contact the correspondence author for these results.
References
Ahmed, S. P., Bittencourt-Hewitt, A., & Sebastian, C. L. (2015). Neurocognitive bases of emotion regulation development in adolescence. Developmental Cognitive Neuroscience, 15, 11–25. https://doi.org/10.1016/j.dcn.2015.07.006.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders. 5th edn. Washington, DC: American Psychiatric Association
Anestis, M. D., Kleiman, E. M., Lavender, J. M., Tull, M. T., & Gratz, K. L. (2014). The pursuit of death versus escape from negative affect: An examination of the nature of the relationship between emotion dysregulation and both suicidal behavior and non-suicidal self-injury. Comprehensive Psychiatry, 55, 1820–1830. https://doi.org/10.1016/j.comppsych.2014.07.007.
Anestis, M. D., Knorr, A. C., Tull, M. T., Lavender, J. M., & Gratz, K. L. (2013a). The importance of high distress tolerance in the relationship between nonsuicidal self-injury and suicide potential. Suicide and Life Threatening Behavior, 43, 663–675. https://doi.org/10.1111/sltb.12048.
Anestis, M. D., Pennings, S. M., Lavender, J. M., Tull, M. T., & Gratz, K. L. (2013b). Low distress tolerance as an indirect risk factor for suicidal behavior: considering the explanatory role of non-suicidal self-injury. Comprehensive Psychiatry, 54, 996–1002. https://doi.org/10.1016/j.comppsych.2013.04.005.
Arens, A. M. (2012). Psychological mechanisms linking child maltreatment and non-suicidal self-injury. Vermillion: University of South Dakota.
Arens, A. M., Gaher, R. M., Simons, J. S., & Dvorak, R. D. (2014). Child maltreatment and deliberate self-harm: a negative binomial hurdle model for explanatory constructs. Child Maltreatment, 19, 168–177. https://doi.org/10.1177/1077559514548315.
Arbuckle, J. L. (1997). Amos users guide: Version3. Chicago: SmallWaters Corporation.
Arbuckle, J. L. (2010). IBM SPSS Amos19 user’s guide. Chicago: IBM SPSS.
Auerbach, R. P., Kim, J. C., Chango, J. M., Spiro, W. J., Cha, C., Gold, J., & Nock, M. K. (2014). Adolescent nonsuicidal self-injury: examining the role of child abuse, comorbidity, and disinhibition. Psychiatry Research, 220, 579–584. https://doi.org/10.1016/j.psychres.2014.07.027.
Banducci, A. N., Hoffman, E. M., Lejuez, C., & Koenen, K. C. (2014). The impact of childhood abuse on inpatient substance users: Specific links with risky sex, aggression, and emotion dysregulation. Child Abuse and Neglect, 38, 928–938. https://doi.org/10.1016/j.chiabu.2013.12.007.
Bolger, K. E., & Patterson, C. J. (2001). Pathways from child maltreatment to internalizing problems: Perceptions of control as mediators and moderators. Development and Psychopathology, 13, 913–940.
Bollen, K. A. (1989). Structural equations with latent variables. New York: Wiley.
Bresin, K., & Schoenleber, M. (2015). Gender differences in the prevalence of nonsuicidal self-injury: a meta-analysis. Clinical Psychology Review, 38, 55–64. https://doi.org/10.1016/j.cpr.2015.02.009.
Browne, M. W., & Cudeck, R. (1993). Alternative ways of assessing model fit. Sociological Method and Research, 154, 132–162. https://doi.org/10.1177/004912419021002005.
Buckholdt, K. E., Parra, G. R., & Jobe-Shields, L. (2009). Emotion regulation as a mediator of the relation between emotion socialization and deliberate self-harm. American Journal of Orthopsychiatry, 79, 482–490. https://doi.org/10.1037/a0016735.
Buser, T. J., & Hackney, H. (2012). Explanatory style as a mediator between childhood emotional abuse and nonsuicidal self-Injury. Journal of Mental Health Counseling, 34, 154–169. https://doi.org/10.17744/mehc.34.2.j714850564663545.
Chapman, A. L., Gratz, K. L., & Brown, M. Z. (2006). Solving the puzzle of deliberate self-harm: the experiential avoidance model. Behaviour Research and Therapy, 44, 371–394. https://doi.org/10.1016/j.brat.2005.03.005.
Chen, Y., Liu, X., Huang, Y., Yu, H., Yuan, S., Ye, Y., & He, Q. (2017). Association between child abuse and health risk behaviors among Chinese college students. Journal of Child and Family Studies, 26, 1380–1387. https://doi.org/10.1007/s10826-017-0659-y.
Cui, N., & Liu, J. (2018). Physical abuse, emotional abuse, and neglect and childhood behavior problems: a meta-analysis of studies in mainland China. Trauma Violence Abuse, 1–19. https://doi.org/10.1177/1524838018757750
Cui, N., Xue, J., Connolly, C. A., & Liu, J. (2016). Does the gender of parent or child matter in child maltreatment in China? Child Abuse and Neglect, 54, 1–9. https://doi.org/10.1016/j.chiabu.2016.01.003.
Cummings, J. R., Bornovalova, M. A., Ojanen, T., Hunt, E., MacPherson, L., & Lejuez, C. (2013). Time doesn’t change everything: the longitudinal course of distress tolerance and its relationship with externalizing and internalizing symptoms during early adolescence. Journal of Abnormal Child Psychology, 41, 735–748. https://doi.org/10.1007/s10802-012-9704-x.
Garisch, J. A., & Wilson, M. S. (2015). Prevalence, correlates, and prospective predictors of non-suicidal self-injury among New Zealand adolescents: cross-sectional and longitudinal survey data. Child Adolescent Psychiatry and Mental Health, 9, 1–11. https://doi.org/10.1186/s13034-015-0055-6.
Glaser, D. (2002). Emotional abuse and neglect (psychological maltreatment): a conceptual framework. Child Abuse and Neglect, 26, 697–714. https://doi.org/10.1016/S0145-2134(02)00342-3.
Gratz, K. L., Bornovalova, M. A., Delany-Brumsey, A., Nick, B., & Lejuez, C. W. (2007). A laboratory-based study of the relationship between childhood abuse and experiential avoidance among inner-city substance users: The role of emotional nonacceptance. Behavior Therapy, 38, 256–268. https://doi.org/10.1016/j.beth.2006.08.006.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. https://doi.org/10.1080/10705519909540118.
Jaffee, S. R. (2017). Child maltreatment and risk for psychopathology in childhood and adulthood. Annual Review of Clinical Psychology, 13, 525–551. https://doi.org/10.1146/annurev-clinpsy-032816-045005.
Lerner, R. M., & Steinberg, L. (2009). Handbook of adolescent psychology. 3rd edn. Hoboken, NJ: Wiley.
Lewis, A. J., Kremer, P., Douglas, K., Toumborou, J. W., Hameed, M. A., & Patton, G. C., et al. (2015). Gender differences in adolescent depression: Differential female susceptibility to stressors affecting family functioning. Australian Journal of Psychology, 67, 131–139. https://doi.org/10.1111/ajpy.12086.
Lin, M.P., You, J., Wu, Y.W., & Jiang, Y. (2017). Depression mediates the relationship between distress tolerance and nonsuicidal self-Injury among adolescents: one-year follow-up. Suicide and Life-Threatening Behavior, 1–12. https://doi.org/10.1111/sltb.12382.c
Linehan, M. M. (1993). Cognitive-behavioral treatment of borderline personality disorder. New York: Guilford Press.
Liu, R. T., Scopelliti, K. M., Pittman, S. K., & Zamora, A. S. (2018). Childhood maltreatment and non-suicidal self-injury: a systematic review and meta-analysis. The Lancet Psychiatry, 5, 51–64. https://doi.org/10.1016/s2215-0366(17)30469-8.
Muehlenkamp, J. J., Laurence, C., Lindsey, H., & Plener, P. L. (2012). International prevalence of adolescent non-suicidal self-injury and deliberate self-harm. Chinese Medicine, 6, 1–9. https://doi.org/10.1186/1753-2000-6-10.
Muthén, L. K., & Muthén, B. O. (2012). Mplus user’s guide. 7th edn. Los Angeles, CA: Muthén and Muthén.
Nock, M. K. (2010). Self-injury. Annual Review of Clinical Psychology, 6, 1–25. https://doi.org/10.1146/annurev.clinpsy.121208.131258.
Nock, M. K., & Mendes, W. (2008). Physiological arousal, distress tolerance, and social problem solving deficits among adolescent self-injurers. Journal of Consulting and Clinical Psychology, 76, 28–38. https://doi.org/10.1037/0022-006X.76.1.28.
Nolen-Hoeksema, S. (2012). Emotion regulation and psychopathology: the role of gender. Annual Review of Clinical Psychology, 8, 161–187. https://doi.org/10.1146/annurev-clinpsy-032511-143109.
Peh, C. X., Shahwan, S., Fauziana, R., Mahesh, M. V., Sambasivam, R., Zhang, Y., & Subramaniam, M. (2017). Emotion dysregulation as a mechanism linking child maltreatment exposure and self-harm behaviors in adolescents. Child Abuse and Neglect, 67, 383–390. https://doi.org/10.1016/j.chiabu.2017.03.013.
Plener, P. L., Schumacher, T. S., Munz, L. M., & Groschwitz, R. C. (2015). The longitudinal course of non-suicidal self-injury and deliberate self-harm: a systematic review of the literature. Borderline Personality Disorder and Emotion Dysregulation, 2, 1–11. https://doi.org/10.1186/s40479-014-0024-3.
Preacher, K., & Hayes, A. F. (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 20, 879–891. https://doi.org/10.3758/BRM.40.3.879.
Selby, E. A., Franklin, J., Carson-Wong, A., & Rizvi, S. L. (2013). Emotional cascades and self-injury: Investigating instability of rumination and negative emotion. Journal of Clinical Psychology, 69, 1213–1227. https://doi.org/10.1002/jclp.21966.
Shen, A. C. T. (2009). Long-term effects of interparental violence and child physical maltreatment experiences on PTSD and behavior problems: A national survey of Taiwanese college students. Child Abuse and Neglect, 33, 148–160. https://doi.org/10.1016/j.chiabu.2008.7.006.
Silvers, J. A., McRae, K., Gabrieli, J. D., Gross, J. J., Remy, K. A., & Ochsner, K. N. (2012). Age-related differences in emotional reactivity, regulation, and rejection sensitivity in adolescence. Emotion, 12, 1235–1247. https://doi.org/10.1037/a0028297.
Simons, J. S., & Gaher, R. M. (2005). The distress tolerance scale: development and validation of a self-report measure. Motivation and Emotion, 29, 83–102. https://doi.org/10.1007/s11031-005-7955-3.
Swannell, S., Martin, G., Page, A., Hasking, P., Hazell, P., Taylor, A., & Protani, M. (2012). Child maltreatment, subsequent non-suicidal self-injury and the mediating roles of dissociation, alexithymia and self-blame. Child Abuse and Neglect, 36, 572–584. https://doi.org/10.1016/j.chiabu.2012.05.005.
Tang, J., Li, G., Chen, B., Huang, Z., Zhang, Y., Chang, H., & Yu, Y. (2018). Prevalence of and risk factors for non-suicidal self-injury in rural China: results from a nationwide survey in China. Journal of Affective Disorders, 226, 188–195. https://doi.org/10.1016/j.jad.2017.09.051.
Thomassin, K., Shaffer, A., Madden, A., & Londino, D. L. (2016). Specificity of childhood maltreatment and emotion deficit in nonsuicidal self-injury in an inpatient sample of youth. Psychiatry Research, 244, 103–108. https://doi.org/10.1016/j.psychres.2016.07.050.
Tull, M. T., SpringerAmpamp; Aldao, A. (2015). Editorial overview: new directions in the science of emotion regulation. Current Opinion in Psychology, 3, 4–10. https://doi.org/10.1016/j.copsyc.2015.03.009.
Van Campen, K. S., & Russell, S. T. (2010). Cultural differences in parenting practices: What Asian American families can teach us (Frances McClelland Institute for Children, Youth, and Families Research Link, Vol. 2, No. 1). Tucson, AZ: The University of Arizona.
World Health Organization. (2018). Maternal, newborn, child and adolescent health: adolescent development. http://www.who.int/maternal_child_adolescent/adolescence/en/.
Xing, X., Wang, M., Zhang, Q., He, X., & Zhang, W. (2011). Gender differences in the reciprocal relationships between parental physical aggression and children’s externalizing problem behavior in China. Journal of Family Psychology, 25, 699–708. https://doi.org/10.1037/a0025015.
Yates, T. (2004). The developmental psychopathology of self-injurious behavior: Compensatory regulation in posttraumatic adaptation. Clinical Psychology Review, 24, 35–74. https://doi.org/10.1016/j.cpr.2003.10.001.
You, J., & Leung, F. (2012). The role of depressive symptoms, family invalidation and behavioral impulsivity in the occurrence and repetition of non-suicidal self-injury in Chinese adolescents: A 2-year follow-up study. Journal of Adolescence, 35, 389–395. https://doi.org/10.1016/j.adolescence.2011.07.020.
You, J., & Lin, M. P. (2015). Predicting suicide attempts by time-varying frequency of nonsuicidal self-injury among Chinese community adolescents. Journal of Consulting and Clinical Psychology, 83, 524–533. https://doi.org/10.1037/a0039055.
Zanarini, M. C., Gunderson, J. G., Frankenburg, F. R., & Chauncey, D. L. (1989). The revised diagnostic interview for borderlines: Discriminating BPD from other axis II disorders. Journal of Personality Disorders, 3, 10–19. https://doi.org/10.1521/pedi.1989.3.1.10.
Zhu, X. H., Li, J., Yang, Y. J., Wei, X. Y., Tian, Y. X., Qiao, J., & Zuo, X. W. (2006). Personal report of childhood abuse reliability and validity in a community. Chinese Journal of Behavioral Medicine Science, 11, 10451047.
Zvolensky, M. J., & Hogan, J. (2013). Distress tolerance and its role in psychopathology. Cognitive Therapy and Research, 37, 419–420. https://doi.org/10.1007/s10608-013-9533-4.
Acknowledgements
This manuscript’s data will not be deposited.
Authors’ Contributions
N.K. conceived of the study, participated in its design and coordination and drafted the manuscript; Y.J. participated in the design of the study, performed the measurement, and drafted the manuscript; Y.R. participated in data collection and prepared the initial draft of introduction and discussion; T.G. performed the measurement, conducted statistical analyses, and interpreation of data; X.L. participated in the review of the literature and revised the manuscript; F.L. participated in the design of the study and provided critical revisons of the manuscript; J.Y. participated in its design and coordination and helped to draft the manuscript. All authors contributed to the writing of the manuscript. All authors read and approved the final manuscript.
Funding
This research was supported by the National Natural Science Foundation of China (Grant No. 31771228), National Social Science Foundation of China (Grant No. 14ZDB159), Major Projects of the Humanities and Social Science Research Base of Ministry of Education (17JJD190001 and 16JJD190001), Research Center for Crisis Intervention and Psychological Service of Guangdong Province, South China Normal University, and the base of psychological services and counseling for “Happiness” in Guangzhou. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Data
This manuscript’s data will not be deposited.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Approval
All testing materials and the procedures were approved by the ethical board of the Chinese University of Hong Kong and the participating schools’ authorities.
Informed Consent
Informed consent was obtained from all participants included in the study.
Rights and permissions
About this article

Cite this article
Kang, N., Jiang, Y., Ren, Y. et al. Distress Intolerance Mediates the Relationship between Child Maltreatment and Nonsuicidal Self-Injury among Chinese Adolescents: A Three-Wave Longitudinal Study. J Youth Adolescence 47, 2220–2230 (2018). https://doi.org/10.1007/s10964-018-0877-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-018-0877-7