
Abstract
Decades of research supports the presence of significant genetic influences on children’s internalizing (emotional), externalizing (acting out), and social difficulties, including victimization. Additionally, being victimized has been shown to relate to further behavioral problems. The current study assessed the nature of the gene–environment relationships between the DRD4 gene, peer victimization, and externalizing and internalizing difficulties in 6- to 10-year-old children. 174 children (56 % girls; 88.6 % Caucasian, 3.4 % African American, 8 % mixed race or Mayan) and their parents were administered victimization and problem behavior questionnaires, and DRD4 was genotyped for the children. An interaction between genes (DRD4) and environment (victimization) was significant and supported the differential susceptibility model for verbal victimization and child-reported externalizing behaviors. Children with the DRD4 7-repeat allele were differentially responsive to the verbal victimization environment, such that those experiencing little to no victimization reported significantly lower levels of externalizing behaviors, but if they experienced high amounts of victimization, they reported the highest levels of externalizing behaviors. Thus, consideration of how genes and environment affect children’s experiences of victimization prior to adolescence is essential for understanding the trajectory of both externalizing and internalizing behaviors during adolescent development.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Burgeoning research demonstrates the high frequency at which children and adolescents experience social difficulties, specifically victimization, and associated mental health challenges. As many as 50 % of children in the United States experience at least one form of victimization (Beaver et al. 2007), with prevalence rates as high as 20 % for children by age 6 (Shojaei et al. 2009). Similarly, 13–22 % of United States children and adolescents experience a mental health disorder every year, a rate that has been increasing over time (Costello et al. 2003; Merikangas et al. 2010). Not surprisingly, research suggests a relationship between victimization and behavioral or mental health concerns, including internalizing behaviors (Hawker and Boulton 2000), externalizing behaviors (Reijntjes et al. 2011), loneliness (Qualter et al. 2013), suicidal ideation and attempts (Gini and Espelage 2014), and later psychotic symptoms (Wolke et al. 2014). Middle childhood is an important developmental period for the study of victimization, as prevalence research shows that victimization becomes fairly common at about ages 6–9 years, with one quarter of children in this age range reporting emotional victimization (Turner et al. 2011). Middle childhood also represents an important period for the emergence of mental health difficulties that often continue into adolescence and adulthood, such as anxiety and impulse-control disorders (Costello et al. 2003; Kessler et al. 2005). Finally, the salience of the peer environment is increasing in this age group, as peer acceptance or rejection play an important role in psychological well-being (Werner and Crick 2004). Considerable research on these topics has suggested that a biopsychosocial framework is appropriate, with significant biological and environmental influences on both victimization and behavior problems in childhood. Moreover, recent research has illuminated the potential role of genes in an individual’s response to environmental risks for problem behaviors (Newsome and Sullivan 2014). Examining gene–environment interactions clarifies the ways in which genes and environment affect problem behaviors of young children.
Genetic Influences on Internalizing, Externalizing, and Social Difficulties
Decades of research supports the presence of significant genetic influences on children’s internalizing (emotional), externalizing (acting out), and social difficulties, with most estimates suggesting that 30–80 % of the variance within these difficulties can be attributed to genes (Kendler 2013). One large twin study utilizing the Child Behavior Checklist as a measure of parent-reported symptoms of externalizing and internalizing difficulties in 8- to 17-year-old twins found heritability estimates of 0.45–0.77 for the various subscales (Spatola et al. 2007). Similarly, receiving aggression from others, either within novel situations or within the repeated pattern of interpersonal aggression that we term peer victimization, appears heritable (Ball et al. 2008; Beaver et al. 2009; DiLalla and John 2014). This likely occurs due to genetically influenced behavioral or temperamental characteristics that may elicit bullying from others, such as aggression or a shy temperament.
This evidence of significant heritability has led to research examining which specific genes influence these difficulties. One widely researched gene is the dopamine DRD4 receptor gene. Although present throughout the body, this gene notably is found in prefrontal and subcortical brain regions that are associated with reward sensitivity, emotion processing, and complex thinking skills (Oak et al. 2010). There are several polymorphisms of this gene that are composed of variable number repeats. Shorter polymorphisms have been linked to more efficient binding of dopamine (Plomin and Rutter 1998). Conversely, longer DRD4 alleles (six or more repeats) have been associated with a variety of problem behaviors and “difficult” temperament characteristics (DiLalla et al. 2009). Specifically, DRD4 has been linked to externalizing and internalizing difficulties, including hyperactivity/impulsivity (Banaschewski et al. 2010), addictive behavior (McGeary et al. 2007), increased novelty-seeking (Ray et al. 2009), aggression (Farbiash et al. 2014), oppositional defiance (Kirley et al. 2004), increased victimization (Daigle 2010), and depressive/mood symptoms (López León et al. 2005; Xiang et al. 2008). Although a number of studies conceptualize DRD4 “risk” as having any “long” DRD4 alleles, other studies suggest that the DRD4-7R (7-repeat) allele may function differently from other long alleles, and thus may represent the true “risk” genotype for DRD4, although the 2R allele may be the comparable “risk” allele for Asian individuals (Jiang et al. 2013).
The Relationship Between Peer Victimization and Internalizing/Externalizing Difficulties
Peer victimization is heavily associated with difficulties in both internalizing and externalizing pathology. Experiencing peer victimization has been associated with anxiety, depression, loneliness, and low self-esteem (see reviews by Hawker and Boulton 2000; Reijntjes et al. 2010). Peer victimization also is related to increased aggression, argumentativeness, and the development of a hostile attribution bias (see review by Reijntjes et al. 2011). Interestingly, the relationship between peer victimization and mental health problems appears to be bidirectional, with each accounting for increases in the other over time (Reijntjes et al. 2010, 2011). Thus, children who are victimized represent a high-risk group who are often stuck on a trajectory that leads to increased mental health problems and more instances of victimization from peers. Indeed, developmental cascade models derived by Vaillancourt et al. (2013) indicate concurrent and predictive associations between internalizing, externalizing, and peer victimization difficulties across grades 3 through 8.
It is clear that the relationship between internalizing and externalizing difficulties and peer victimization is strong. The demonstrated heritability of each construct supports the need to examine potential genetic factors that may moderate the relationship between victimization and mental health difficulties. Specifically, given its association with internalizing and externalizing behaviors, as noted above, DRD4 is an excellent candidate gene to investigate further as a moderator for the relationship between peer victimization and emotional/behavioral symptoms.
Gene–Environment Interactions
Gene–environment interactions (G × E) occur when the effects of a given genotype (e.g., DRD4 status) depend on the environment (e.g., peer victimization) that the child experiences. It may be the case that certain youth are genetically sensitive to different peer environments; in other words, the effects of the peer environment may depend on the genotype of the child experiencing it. Two major G × E theories include diathesis-stress (Gottesman and Shields 1972) and differential susceptibility (Belsky and Pluess 2009).
The diathesis-stress model states that individuals with certain genetic predispositions may be at increased risk for negative outcomes when they experience a negative environment. This model has been supported with research on the MAO-A gene (Caspi et al. 2002), the serotonin 5-HTTLPR polymorphism (see review by Nugent et al. 2011), and the DRD4 gene (Bakermans-Kranenburg and van IJzendoorn 2006; DiLalla et al. 2009; Propper et al. 2007) when examining a wide range of negative environments. For example, when studying the 5-HTTLPR gene, Sugden et al. (2010) found that children with two short (S) alleles who were frequently bullied were at the greatest risk for emotional problems. Similarly, Benjet et al. (2010) found that peer victimization significantly predicted depressive symptoms only for preadolescent girls with the SS genotype. Regarding the DRD4 gene, DiLalla et al. (2009) found that preschoolers with a DRD4 allele with six or more repeats whose parents demonstrated more insensitive parenting were more likely to be rated as high on externalizing behaviors. Thus, children with the risk DRD4 genotype experienced more negative outcomes when they experienced insensitive parenting relative to children without this genotype who also experienced insensitive parenting. Conversely, in the same study, 5-year-old children with the “risk” DRD4 genotype were more aggressive than those without this genotype when they were paired with a non-aggressive peer, but all children who were paired with an aggressive peer showed increased aggression themselves, showing a gene–environment interaction in low-aggressive environments. Thus, for those children with genetic risk, the threshold for aggression was lower and they reacted aggressively even in a low-intensity situation. One other study examining G × E with the social environment and DRD4 found evidence for diathesis-stress when examining the relationship between disadvantaged neighborhoods and antisocial outcomes (Beaver et al. 2012).
Differential susceptibility theory suggests a different mechanism by which genes and environments may interact by examining the full environmental spectrum, including both negative and positive environments. Instead of conceptualizing certain genes as conferring only risk, differential susceptibility suggests that they should be viewed as markers of “plasticity” or “malleability” to the environment, both negative and positive (Belsky and Pluess 2009). Differential susceptibility states that a child with a “risk” gene who experiences a risky or negative environment is at the highest risk for a negative outcome, but if placed in a more positive environment, that child would actually display the most positive outcomes. This theory has been supported with DRD4 research in children examining the parenting environment (Bakermans-Kranenburg and van IJzendoorn 2006, 2011; Jiang et al. 2013; Knafo et al. 2011). For example, Nikitopoulos and colleagues (2014) found that DRD4 moderated the relationship between early maternal care and externalizing behavior during adolescence. Specifically, those with a DRD4 allele with 7 or more repeats (7+R) demonstrated greater difficulties when placed in a less responsive, less stimulating environment than those without 7+R. They also showed fewer externalizing difficulties when placed in a more responsive and stimulating early care environment than those with the shorter allele, providing some support for a differential susceptibility (versus diathesis-stress) conceptualization. Focusing on the peer environment, Iyer et al. (2013) found evidence for a differential susceptibility model examining 5-HTTLPR in the relationship between bullying and depression. They found that adolescents with at least one S allele demonstrated significantly higher levels of depression when they were highly victimized, but significantly lower levels of depression when they reported low levels of victimization. However, less is known about whether this same differential pattern would be found with DRD4 and peer victimization.
Compared to research on 5-HTTLPR, less G × E research in the context of peer victimization has focused on DRD4. One study of African American children examined parenting and neighborhood influences rather than peers specifically, but they did examine social environments interacting with genotype (Simons et al. 2012). They found that children with the short 5-HTTLPR allele and the DRD4-7R allele who experienced negative social environments were more likely to demonstrate high levels of aggression, anger, and a hostile view of relationships. In contrast, children with this genotype in positive social environments were significantly less likely to demonstrate these negative outcomes, suggesting differential susceptibility. In a Dutch longitudinal adolescent sample, Kretschmer et al. (2013) studied both positive and negative peer environments to determine whether DRD4 behaved in a differential susceptibility fashion, interacting with peer environments to affect adolescents’ risk of delinquency. Contrary to research supporting the DRD4-7R allele as the susceptibility allele, they found that adolescents with the DRD4-4R, versus DRD4-7R, allele were most susceptible to the impact of both victimization and positive peer interactions on future delinquent behavior.
Although these results provide interesting evidence for differential susceptibility and diathesis-stress regarding DRD4, the peer environment measures in these studies included extreme situations of exposure to violent peers or neighborhood violence, or the outcome was confined to delinquent behavior. It is important to examine whether these results would extend to more normative peer victimization environments and to both externalizing and internalizing difficulties, which were examined in the present study.
Current Study
The aim of the current study was to assess the nature of the gene–environment relationships between the DRD4 gene, peer victimization, and externalizing and internalizing difficulties in 6- to 10-year-old children. This age range was chosen in order to include youth in elementary school, as they were exposed to the school social situation but were not yet fully adolescents, in the hopes that we would be able to identify some important processes that precede the increased levels of victimization that occur in adolescence (Turner et al. 2011). Our goal was to consider social experiences in the time prior to adolescence, although of course it is possible that some of the older youth were entering puberty. This was not assessed directly, but age was included in analyses to determine if there was an age effect. Although the majority of G × E DRD4 research focuses on externalizing problems, we chose to assess externalizing as well as internalizing problems given that internalizing problems have been shown to be associated with both DRD4 (Xiang et al. 2008) and peer victimization (Hawker and Boulton 2000), as well as the fact that externalizing and internalizing problems often co-occur (Achenbach et al. 1991; Oland and Shaw 2005). This study extends the previous literature by including a widespread environmental stressor (peer victimization) within a differential susceptibility framework. Specifically, we hypothesized that children with the DRD4 “risk” genotype (DRD4-7R) would be rated as having the greatest number of externalizing and internalizing problems when experiencing high levels of verbal victimization (which we defined as negative verbal communication) and physical victimization (defined as physically negative events against the child or his or her property). However, it also was hypothesized that children with the DRD4-7R genotype who experienced no verbal and physical victimization would have the fewest externalizing and internalizing problems. Importantly, in order to demonstrate differential susceptibility, it also was hypothesized that children without the DRD4-7R genotype (DRD4-no7R) would not show different levels of problem behaviors as a function of verbal or physical victimization experienced.
Method
Participants were drawn from two rounds of data collection, both of which were part of the Southern Illinois Twins/Triplets and Siblings Study (SITSS; DiLalla 2002; DiLalla et al. 2013), a longitudinal twin study of child development that included twins who lived within about 2 h of a Midwestern university, all of whom were typically developing (i.e., no diagnoses of developmental delay). Twins were recruited via a number of methods, including flyers, newspaper birth announcements, daycare recruitment, word of mouth, and the lab’s social media page. One round of data collection yielded 120 children (60 twin pairs; 69 girls and 51 boys) aged 6–10 years old (mean = 8.05, SD = 1.52) and their parents. Another round of data collection three years earlier yielded an additional 55 children [from 29 twin pairs (1 child refused testing, 2 children’s data were incomplete); 29 girls and 26 boys] also aged 6–10 years old (mean = 8.82, SD = 1.28) and their parents. For families with triplets or quadruplets, only two randomly selected children were included in order to avoid giving extra weight to families with more children. The final combined sample utilized for this study consisted of children from 24 monozygotic (MZ) pairs, 41 same-sex dizygotic (DZ) pairs, and 22 opposite-sex DZ pairs of twins. 88.6 % of the families reported their children were Caucasian, 3.4 % reported that they were African American, and 8 % reported that they were either mixed race or Mayan. Some genetic studies attempt to include only participants of the same race. However, given that race was self-reported and not genetically ascertained, and also given that DRD4 behavioral effects have been differentially noted for Asian individuals but not other racial groups (Jiang et al. 2013), we maintained all children in this study. We did, however, examine race as a covariate. One child was not included in analyses because DNA data were not conclusive for her, resulting in a final sample size of 174 children from 89 families. This study was approved by the Human Subjects Committee prior to its advent.
Procedure
Upon expressing interest in participating, families were called and a date was scheduled for the children and at least one parent to come to a campus lab for approximately one hour to complete testing. Parents were given consent forms and children were given assent forms prior to the beginning of testing. They were informed of study goals, risks, benefits, and confidentiality before providing informed consent. There were two trained testers present at each study so that twins could always be tested simultaneously. In cases of triplets, there were three testers so all three children could be tested at the same time.
After providing informed assent, each child went into a separate room with a trained tester. Children were read questions and marked their answers on an answer sheet. For younger children or those who had difficulty with the answer sheet, trained testers would allow the children to provide verbal responses and the testers would mark the answers on the sheet. We utilized pictorial aids of Likert-type scales, such as gumball machines (with different levels of gumballs within the machine indicating how much the child agreed with a statement) to facilitate comprehension. A detailed testing protocol was utilized by each tester to ensure standardization, including specific prompts and alternative explanations for items that the children may not have understood, given their age. Each twin completed the same set of measures in the same order. For one study, each questionnaire was separated by a lab task (either a theory of mind task or an emotion recognition task, neither of which is included in the present study). For the other study, questionnaires were alternated with an operant eye gaze task that involved watching pictures on a computer. Testing room doors were not shut completely in order to assure child safety. Thus, to increase privacy during testing, ocean sounds were played in each testing room, which eliminated any voice sounds across rooms. After testing, each child was allowed to pick out a toy to take home from several toys arranged on shelves, to thank them for participating.
While the children were tested, one parent completed a battery of separate measures for each twin (Child Behavior Checklist and Multidimensional Peer-Victimization and Bullying Scale were utilized in this study, as described below). Although any parent was eligible to fill out the measures, 93 % were completed by mothers, as they were usually the parent to bring the children in. At the conclusion of the testing session, parents received a gift card or were mailed a check to compensate them for their participation.
Measures
Demographic Questionnaire
All families completed a basic demographic questionnaire that assesses background information such as race, family structure, family income, and parent age, occupation, and education level. In our sample, the median yearly income was $85,000–$90,000/year, ranging from less than $5,000 (2 %) to greater than $90,000 (40 %). Maternal and paternal education were rated on a 5-point scale (1 = no high school degree; 2 = high school degree; 3 = technical certificate; 4 = college degree; 5 = advanced training beyond a college degree). In our sample, the median for both maternal and paternal education was having a college degree. These values are high compared to those of this general region, where 89 % of adults have a high school degree and 36 % have at least a college degree, and the median family income is about $51,000 (Jackson Growth Alliance website: http://www.jacksonbiz.org/infocenter/demojc.html). However, that is not surprising and is fairly typical of families who are willing to donate their time for a research study.
DNA Collection
In order to obtain genetic data from children in the current study, buccal cells were collected either when children were tested at younger ages or during current testing if we had not been able to collect these earlier. Collection occurred three times during testing, separated by different phases of the testing protocol. Before collection, parents provided consent after being given information on the purpose of collecting genetic material, the potential risks and benefits, and our confidentiality process. Samples were collected by swabbing the inside of both cheeks and gums for 20 s three times during testing—once prior to testing, once after the first child was tested, and finally after testing was completed. This is standard protocol for collecting buccal samples from young children. Samples were stored in a freezer until they were ready to be sent for analysis. For this project, samples were analyzed for DRD4 genotype. Allele sizes were scored by two investigators independently; inconsistencies were reviewed and rerun if necessary. Children were grouped as either DRD4 “risk” (DRD4-7R), having at least one allele with 7 repeats (N = 57), or DRD4 “no risk” (DRD4-no7R), having no alleles with 7 repeats (N = 117). Only 10 children had 2 alleles with the 7R variant, and therefore we did not compare children with one versus two 7R alleles. The earliest studies on DRD4 grouped participants as either having fewer than seven repeats or having seven or more repeats, but more recent studies suggest that the 7R variant differs from other repeat alleles in function and that it is incorrect to combine them with alleles with more repeats (Jiang et al. 2013). Thus, we compared children with or without a 7R allele. This sample was in Hardy–Weinberg equilibrium, χ 2(1) = 0.90, p = .343.
Verbal and Physical Victimization
Two types of victimization, verbal and physical, were measured using the Multidimensional Peer-Victimization and Bullying Scale (MPVBS; Biebl et al. 2011), which is an adapted form of the Multidimensional Peer Victimization Scale (MPVS) created by Mynard and Joseph (2000). The original 16-item scale contains 4 subscales of victimization (physical victimization, social manipulation, verbal victimization, and attacks on property). The creators demonstrated good test–retest reliability for each subscale, with Cronbach’s alpha scores ranging from 0.73 to 0.85 (Mynard and Joseph 2000). The questionnaire asks the child to rate the frequency of each situation in his/her own life (0 = never, 1 = once, 2 = more than once). The altered version of the scale also includes parallel items that query for bullying. For example, a question asking “How often have you had property stolen from you by another child?” was later rephrased to read “How often have you stolen property from another child?” The Likert-type scale also was changed for the modified questionnaire to offer more options (0 = never, 1 = once, 2 = two to five times, 3 = six to ten times, and 4 = more than ten times). This adapted questionnaire yields the original 4 subscales of victimization (physical victimization, social manipulation, verbal victimization, and attacks on properties) and an additional 4 scales of bullying (physical bullying, social manipulation, verbal bullying, and attacks on properties).
For the present study, only the victimization items were examined. Two higher order subscales were created, one for verbal victimization (summing the social manipulation and verbal victimization items into a single scale) and one for physical victimization (summing physical victimization and attacks on properties). The two higher order subscales showed good reliability, Cronbach’s alpha = 0.82 and 0.85 for verbal and physical victimization, respectively.
Child-Rated Externalizing and Internalizing Problem Behaviors
Children were asked to rate themselves on the Strengths and Difficulties Questionnaire (SDQ; Goodman 1997, 2001) to provide assessments of externalizing and internalizing problem behaviors. The SDQ utilizes a three-point, Likert-type response scale to examine conduct problems, emotional symptoms, hyperactivity and inattention, peer relationship problems, and prosocial behaviors, totaling 25 items with 5 items per category. The SDQ has both parent and child versions, with the latter used in the current study. For each item, children were asked to indicate whether a behavior was not true, somewhat true, or certainly true of themselves.
The SDQ has been shown to have adequate internal consistency (average alpha of 0.73) and test–retest stability after 5 months (average alpha of 0.62) for both children and parent reports (Goodman 2001). In low-risk samples (such as the sample utilized in the current study), it has been suggested that combining the emotional and peer subscales into an internalizing scale and the conduct and hyperactivity subscales into an externalizing scale is most useful (Goodman et al. 2010). Goodman and Scott (1999) found that correlations between the internalizing and externalizing scales of the SDQ were lower than these correlations on the Child Behavior Checklist (CBCL; Achenbach and Rescorla 2001), suggesting more precise construct validity of the second-order scales. For the present sample, Cronbach’s alphas were adequate, 0.69 for externalizing and 0.74 for internalizing.
Parent Ratings of Child Externalizing and Internalizing
Parents completed the Child Behavior Checklist (CBCL; Achenbach and Rescorla 2001) to provide parent reports of children’s externalizing and internalizing problem behaviors. The CBCL is a widely used measure comprising 113 items listing possible problem behaviors, which parents endorse using a 3-point response scale, from 0 = this never applies to my child to 2 = this is often a problem. Externalizing includes aggression and rule breaking behaviors, and internalizing includes withdrawn, somaticizing, and anxious behaviors. Cronbach’s alphas for our sample were good for both scales, alpha = 0.87 for externalizing and 0.77 for internalizing.
Statistical Approach
Mixed model multilevel linear regression modeling in SPSS 20 was used to examine the effects of victimization and genotype status on children’s externalizing and internalizing behaviors. This method allows inclusion of siblings (twins) within a family as a nested factor and therefore allowed us to include two children from each family in the analyses. Although the number of families in this study is not large (89 families with 1 or 2 children from each), this number is sufficient to yield unbiased parameter estimates using this statistical method (Maas and Hox 2005).
Physical and verbal victimization scores were mean centered, as suggested by Aiken and West (1991), to allow for more interpretable results for the interaction analyses. Main effects of physical and verbal victimization and DRD4 status (dummy coded as 1 = DRD4-7R and 2 = DRD4-no7R) were examined first as fixed effects (Model 1). Second, age, race, sex, and zygosity were examined one at a time to determine whether they were significant covariates (Models 2–5). If they were significant, then the significant variable was included in the rest of the analyses. Third, the hierarchical nature of the data set (including siblings from the same family) was examined by including family as a random effect, allowing examination of whether y-intercepts vary across individual families (Model 6). Fourth, we examined whether adding random slopes for the victimization variables was beneficial to the models (Model 7). Doing this allows examination of whether the regression slopes (rather than intercepts) vary across families. Finally, interactions between physical victimization and DRD4 risk status and then between verbal victimization and DRD4 risk status were examined (Models 8 and 9). Maximum likelihood estimation was used so that models could be compared statistically (Field 2013). The best fitting models were those with significantly improved model fit based on Chi square comparison tests as well as lowest Aikike information criterion (AIC) test (Akaike 1974). The AIC is based on the Chi square but controls for number of estimated parameters. The AICc (AIC corrected) is similar but uses a correction for sample size (Hurvich and Tsai 1989) and therefore is a better test for small samples. An important advantage of the AICc test over the Chi square difference test is that non-nested models can be compared by using the AICc. The model with the lowest AICc value is considered the best-fitting model of those that are tested.
Results
Physical and verbal victimization scores and CBCL internalizing and externalizing were positively skewed; therefore, these variables were square root transformed to eliminate skew. SDQ internalizing and externalizing were normally distributed and did not require transformation. Descriptive statistics for all study variables are included in Table 1. Correlations between study variables are presented in Table 2.
Prior to determining the existence of G × E effects, Belsky et al. (2007) suggest that it is valuable to determine whether gene–environment correlations may be providing a confound that should be controlled during G × E analyses. They suggest that it is important to rule out significant correlations between the moderator (DRD4 in this case) and the independent variables (physical and verbal victimization here), and between the moderator and the outcome variables (internalizing and externalizing here). To do this, we calculated a Spearman’s ρ correlation between DRD4 group and each of the independent and dependent variables. There were no significant group differences between children with and without the 7-repeat allele for either verbal (ρ = 0.07, p = .395) or physical (ρ = −0.06, p = .426) victimization, nor for child-reported or parent-reported externalizing (ρ = 0.05, p = .518, and ρ = 0.07, p = .341, respectively) or child-reported or parent-reported internalizing (ρ = 0.07, p = .362, and ρ = 0.15, p = .055, respectively). Thus, these possible gene–environment correlation confounds were not problematic for this study.
Effects of Victimization and DRD4 Status on Child-Reported Behavior Problems
Externalizing Problem Behaviors
As can be seen in Table 3 (Models 2–5), neither age, sex, race, nor zygosity (MZ versus DZ) were significant predictors of SDQ externalizing behaviors. Model 6 included family status in the model as a random effect. Although this model was not significantly better fitting than Model 1, family status was maintained in the rest of the analyses because it is theoretically important to control for shared family status when including two children from the same family. Random slopes (Model 7) were not significant, nor was the physical victimization × DRD4 status interaction (Model 8). However, Model 9, which included verbal victimization × DRD4, provided a significantly better fit and was the best-fitting model, with the lowest AICc value of 908.191. Parameter estimates are provided in Table 4.
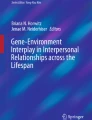
The verbal victimization × DRD4 interaction effect was probed by re-running Model 9 (without DRD4 as an IV) separately for the two DRD4 risk groups (see Table 5), as per Field (2013). These models showed that verbal victimization was significantly and positively predictive of SDQ externalizing for children with the 7-repeat DRD4 allele but not for children without the 7-repeat allele (see Fig. 1). Specifically, children with DRD4-7R who reported the most victimization showed the highest levels of externalizing behaviors, whereas DRD4-7R children who reported the least victimization had the lowest externalizing behavior scores. Importantly, note that the cross-over point in the graph is at approximately SDQ = 5.5, which is about the mean value for this sample and certainly within the range of interest for this measure (Roisman et al. 2012). Notably, victimization was not related to externalizing problem behaviors for DRD4-no7R children.

Interaction of DRD4 and verbal victimization predicting to SDQ externalizing problem behaviors. Variables are plotted without transformation (see Table 1 for means and ranges). The slope for the DRD4-7R group is significant; the slope for the DRD4-no7R group is not
Internalizing Problem Behaviors
The same analyses were repeated for children’s self-reported internalizing problem behaviors. As can be seen from Table 6, there was no significant effect of sex or race. However, age and zygosity were significant, with younger children and DZ twins reporting more internalizing behaviors. Thus, these covariates were maintained for the rest of the analyses, although zygosity was no longer significant after sibship was added to the model (Model 6). The hierarchical structure of our data set was modeled in Model 6 by including family (sibship) as a random effect, and this also yielded an improved model fit, meaning that the intercepts for the relationship between victimization and internalizing problem behaviors vary across families. Neither random slopes (Model 7) nor physical or verbal victimization × DRD4 interactions (Models 8 and 9) were significant. Although Model 9 had the lowest AICc, the Chi square difference test was not significant. Additionally, examination of the parameter estimates for this model showed that the interaction term was not significant. Thus, Model 6 was considered the best-fitting, most parsimonious model, with nearly the lowest AICc value of 903.037. Final model parameter estimates are presented in Table 4 and show that age, physical victimization, and verbal victimization were significant predictors of child-reported internalizing problems.
Effects of Victimization and DRD4 Status on Parent-Reported Behavior Problems
Externalizing Problem Behaviors
The same series of models were examined using parent-reported CBCL externalizing problem behaviors (see Table 7). There was no significant effect of sex, age, race, or zygosity, so these covariates were dropped from the rest of the models. The hierarchical structure of our data set was then included in Model 6 and yielded an improved model fit. When random slopes were added to the model (Model 7), there was no significant improvement in model fit. Similarly, when victimization × DRD4 interaction effects were added to the model (Models 8 and 9), no significant improvement in model fit was seen. Thus, the best fitting model was Model 6, with AICc = 549.912. Parameter estimates in Table 8 show that children who reported increased verbal victimization were rated by their parents as having more externalizing problem behaviors, although this did not differ by DRD4 status.
Internalizing Problem Behaviors
Finally, the same models were run examining parent-reported CBCL internalizing problem behaviors as the dependent variable (see Table 9). Neither age, sex, race, nor zygosity (Models 2–5) were significantly related to internalizing problem behaviors. Although the model fit improved when the hierarchical structure of the data set was added to the model (Model 6), there were no significant relationships observed between child-reported victimization and parent-reported problem behaviors and none of the interactions were significant (see Table 8). The best fitting model included adding family as a random effect (Model 6), with AICc = 495.735. Final parameter estimates are presented in Table 8.
Discussion
Being victimized can lead to a number of negative outcomes, including both externalizing and internalizing problem behaviors (Hawker and Boulton 2000; Reijntjes et al. 2010, 2011). However, as a function of their genotype, some children appear to be at increased risk for negative outcomes after being victimized. Specifically, in this study we showed that children with at least one copy of the 7-repeat allele of the DRD4 gene may be differentially susceptible to victimization exposure in terms of their externalizing behaviors. DRD4-7R children who were verbally victimized were significantly more likely to have self-reported externalizing problem behaviors compared to DRD4-7R children who were not verbally victimized. Conversely, children with this genotype showed the fewest externalizing problems in an environment without verbal victimization. Children without a 7-repeat allele of the DRD4 gene did not show differences in externalizing behaviors as a function of being victimized, suggesting that they may be protected from the negative effects of being victimized. However, they also did not exhibit significantly fewer problem behaviors when they were in a positive, non-victimizing environment, whereas the DRD4-7R children did. Thus, for externalizing problems, our study supports the basic tenets of differential susceptibility theory for the DRD4 genotype within a victimization environment. Interestingly, we did not show an interaction between DRD4 and victimization for internalizing problems, which appears to be consistent with other research (Bakermans-Kranenburg and van IJzendoorn 2006). Instead, both physical and verbal victimization put children at risk for internalizing problems regardless of children’s DRD4 status.
Developmental Implications
Our examination of children aged 6–10 years provides information about some of the important processes that put children at risk for the ill effects of early victimization at a time before they reach adolescence, at which time bullying behaviors are often associated with dangerous and more substantial consequences (Heilbron and Prinstein 2010; Laird et al. 2001). Our results demonstrate that negative peer experiences negatively impact behavior problems even at this younger age, and this may be true especially for children with certain biological dispositions to respond more negatively to that victimization. These early experiences may put youth at risk for more negative peer experiences in adolescence, suggesting the possibility of a negative trajectory from early victimization to greater problems in adolescence. This highlights the importance of understanding these processes developmentally, prior to adolescence. Given that victimization in childhood and adolescence predicts maladaptive outcomes into adulthood, an approach that appreciates both developmental periods likely provides the most comprehensive view of these difficulties (Klomek et al. 2010).
Gene–Environment Interaction Theories
Much research examining gene–environment interactions focuses on diathesis-stress theory. Although diathesis-stress is a well-supported theory, it conceptualizes certain genotypes as inherently “bad” (Belsky et al. 2009) and only examines negative environments. Instead, it may be useful to consider differential susceptibility theory, stating that certain genotypes are “susceptibility” rather than “risk” genotypes (Kennedy 2013). By assessing “susceptible” youth in both negative and positive environments, we may be able to identify the potential they may have for more positive outcomes if placed in environments that better fit their biological predispositions. Our findings are consistent with these differential susceptibility findings. Specifically, we showed that children with a DRD4-7R allele reported significantly fewer externalizing problem behaviors when they reported a peer environment devoid of verbal victimization, but they reported significantly more externalizing behaviors when they reported large amounts of verbal victimization from their peers. Children without this allele showed no differences in externalizing behaviors as a function of their peer victimization environment.
However, it is important to note that we did not assess overtly positive environments and outcome behaviors. In our study, the absence of victimization was meant to represent a positive environment and the absence of externalizing or internalizing problems was conceptualized as a positive outcome. Although we did not assess specific aspects of the positive, non-victimized environments, it is likely that these environments consisted of more positive peer relationships than environments characterized by high amounts of victimization, since friendships have been shown to protect against victimization (Hodges et al. 1999; Kendrick et al. 2012). Given that positive peer relationships have been linked with a number of positive outcomes such as happiness, improved attitudes towards school, and better adjustment (Holder and Coleman 2009; Majors 2012), we believe that an environment characterized by low amounts of victimization can be viewed as positive in this way. However, a more accurate assessment of the positive side of the environmental spectrum would include ratings of the presence of a specific positive environment, such as positive life events or the number of friendships a child has (Bakermans-Kranenburg and van IJzendoorn 2011). Additionally, although the lack of externalizing and internalizing problems is positive, future studies assessing the effects of the peer environment may consider assessing for more overtly positive outcome behaviors, such as prosociality. Recent research on the effects of parenting has suggested that DRD4-7R children exhibit the most prosocial behaviors when they experience secure attachments to their mothers (Bakermans-Kranenburg and van IJzendoorn 2011) or when they experience positive parenting during a parent–child interaction (Knafo et al. 2011), but show the least prosociality when experiencing insecure attachments or negative parenting, supporting differential susceptibility. However, prosocial behaviors have not been a target variable for studies examining victimization. Nevertheless, a differential susceptibility framework was supported in the current study, as we found differential responsivity, or susceptibility, to the environment as a function of genotype.
Differences in Types of Victimization
Interestingly, we only observed G × E effects for verbal victimization and not for physical victimization. One explanation for this may be that verbal victimization is more subjective than physical victimization. It is easier to misinterpret relational or verbal victimization than it is to misinterpret being physically harmed. Perhaps DRD4-7R children’s susceptibility to the environment could also translate into a perception bias related to verbal victimization. If children with this genotype have a perception bias (i.e., cognitive distortion) leading them to over-interpret events in an all-or-nothing fashion, then they might perceive everything as all good or all bad (see Beck et al. 1979, for a comprehensive description of cognitive distortions). Thus, when they perceive the environment to be good, they would perceive everything in a positive light, including both others’ behaviors as well as their own. Conversely, when they perceive the environment to be bad, they would perceive the environment as well as their own behaviors to be negative. Interestingly, the G × E results did not hold up for parent ratings. If children’s perception biases are responsible for the G × E results that we found, then indeed we would not expect to find this interaction when using parent reports as outcome measures. Thus, our results support the possibility that DRD4-7R children may have a perception bias toward viewing the world in an all-positive or all-negative light, whereas DRD4-no7R children may have a more balanced approach. The relationship between cognitive distortions and internalizing/externalizing difficulties has been well documented in community and clinical samples of children and adolescents (Barriga et al. 2000; Leung and Wong 1998). Further research examining the association between children’s perceptions and different genotypes would further elucidate this issue.
We also only observed G × E for externalizing and not internalizing behavior problems. This appears to be consistent with other studies (Bakermans-Kranenburg and van IJzendoorn 2006) and may be related to the fact that genetic influences on internalizing appear to be stronger in an environment without stressors or negativity (Hicks et al. 2009a). Hicks and colleagues demonstrated that nonshared environment becomes the most important predictor of internalizing problems in environments characterized by any of a number of stressors, such as antisocial peers or parent–child relationship problems. This did not hold true for externalizing problem behaviors (Hicks et al. 2009b). Thus, in a study examining victimization as the relevant environment in G × E, it is not surprising that this interaction was significant for externalizing problems and not significant for internalizing problems.
Strengths and Limitations
There are several strengths that this study brings to the examination of victimization and children’s problem behaviors in a pre-adolescent sample. One important strength of this study is the effort to broaden our current understanding of gene–environment relationships by examining the full range of a typically occurring environmental problem (peer victimization) and its association with genotype. Our research supports the growing need to examine gene–environment relationships beyond “risk” models such as diathesis-stress theory. Indeed, findings such as these help us to determine how to prevent maladaptive symptoms in children following stressful life events, underscoring the important risk or protective role that genotype may play. A second strength of our study is the inclusion of both children’s and parents’ reports of children’s behaviors, especially considering that we found different results depending on the reporter of the problem behaviors. We have previously shown that parents tend to report less victimization when compared to children’s self-report, especially verbal victimization, which is more difficult than physical victimization for parents to observe (John and DiLalla 2013). We now demonstrate also that parent reports of children’s problem behaviors, both externalizing and internalizing, do not show evidence of G × E, whereas children’s reports do. Consideration of children’s perceptions of both their environments and their own behaviors may yield important information about how genotype relates to perception biases.
There are several important limitations to this study that merit discussion. The primary limitation is the small sample size. Gene–environment interactions are difficult to ascertain in small samples because the power is so low, and therefore of course these results will require replication (Roisman et al. 2012). We maximized our sample by including all children in a mixed model multilevel linear regression model, but we still had very limited power to detect robust interactions. Nonetheless, the results we obtained were consistent with differential susceptibility theory and with previous research on externalizing problem behaviors. The problem with under-powered studies lies with the potential to accept the null hypothesis mistakenly (Type II errors), and we in fact have found a significant result, suggesting the possibility of having committed a Type I error, which is less of a concern with under-powered studies (Field 2013; Spybrook et al. 2011). However, because of our small sample size, we could not conduct analyses examining three-way interactions. Thus, for example, we did not explore whether there were any interactions with sex of child. Further research with a larger sample should address such issues. In addition, it is possible that with a larger sample we would have been able to identify G × E with parent reports. Further research with a larger sample will be necessary to explore this.
Additionally, our sample consisted primarily of upper to middle class Caucasian families, and thus generalizability is suspect. Replication across a more diverse sample would be beneficial. This is especially true because the impact of victimization may vary across different cultures. A third important limitation is that we included children across a fairly large age range, from 6 to 10 years. These children have in common that they are all in elementary school, which was our goal, but it also is true that some of the older children might have been beginning puberty, which would certainly affect their behaviors. Age was a significant predictor of internalizing, with younger children reporting more internalizing problems, but not of externalizing. It will be important to replicate this study with a much larger sample of youth of different ages to determine whether the very youngest children differ from the oldest.
Conclusion
We have demonstrated that, for externalizing problems, young school-age children are differentially susceptible to the victimization environment depending on their DRD4 genotype. Children with a 7-repeat allele who report high amounts of verbal victimization report high levels of externalizing problems, whereas children with the 7-repeat allele who report little or no verbal victimization report few externalizing behavior problems. Importantly, those without the 7-repeat allele do not report differences in problem behaviors as a function of being victimized. For internalizing problems, both physical and verbal victimization were significant predictors of child reported problems, but there was no evidence of G × E. Examining this age group helps to illuminate early risk for the negative trajectory of social consequences into adolescence and adulthood. Indeed, our research examining the factors involved in how school age youth respond to victimization at the beginning of this negative trajectory contributes to a more comprehensive view of the complex etiology of adolescent behavior problems.
References
Achenbach, T. M., Howell, C. T., Quay, H. C., & Conners, C. K. (1991). National survey of problems and competencies among four- to sixteen-year-olds: Parents’ reports for normative and clinical samples. Monographs of the Society for Research in Child Development, 56, 1–131.
Achenbach, T. M., & Rescorla, L. A. (2001). Manual for the ASEBA School-Age Forms and Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, and Families.
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions. Newbury Park: Sage.
Akaike, H. (1974). A new look at the statistical model identification. IEEE Transactions on Automatic Control, 19(6), 716–723. doi:10.1109/TAC.1974.1100705.
Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2006). Gene–environment interaction of the dopamine D4 receptor (DRD4) and observed maternal insensitivity predicting externalizing behavior in preschoolers. Developmental Psychobiology, 48(5), 406–409. doi:10.1002/dev.20152.
Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2011). Differential susceptibility to rearing environment depending on dopamine-related genes: New evidence and a meta-analysis. Development and Psychopathology, 23(1), 39–52. doi:10.1017/S0954579410000635.
Ball, H. A., Arseneault, L., Taylor, A., Maughan, B., Caspi, A., & Moffitt, T. E. (2008). Genetic and environmental influences on victims, bullies and bully-victims in childhood. Journal of Child Psychology and Psychiatry, 49(1), 104–112. doi:10.1111/j.14697610.2007.01821.x.
Banaschewski, T., Becker, K., Scherag, S., Franke, B., & Coghill, D. (2010). Molecular genetics of attention-deficit/hyperactivity disorder: An overview. European Child and Adolescent Psychiatry, 19, 237–257. doi:10.1007/s00787-010-0090-z.
Barriga, A. Q., Landau, J. R., Stinson, B. L., Liau, A. K., & Gibbs, J. C. (2000). Cognitive distortion and problem behaviors in adolescents. Criminal Justice and Behavior, 27(1), 36–56. doi:10.1177/0093854800027001003.
Beaver, K. M., Boutwell, B. B., Barnes, J. C., & Cooper, J. A. (2009). The biosocial underpinnings to adolescent victimization. Youth Violence and Juvenile Justice, 7(3), 223–238. doi:10.1177/1541204009333830.
Beaver, K. M., Gibson, C. L., DeLisi, M., Vaughn, M. G., & Wright, J. P. (2012). The interaction between neighborhood disadvantage and genetic factors in the prediction of antisocial outcomes. Youth Violence and Juvenile Justice, 10(1), 25–40. doi:10.1177/1541204011422085.
Beaver, K. M., Wright, J. P., DeLisi, M., Daigle, L. E., Swatt, M. L., & Gibson, C. L. (2007). Evidence of a gene × environment interaction in the creation of victimization: Results from a longitudinal sample of adolescents. International Journal of Offender Therapy and Comparative Criminology, 51, 620–645. doi:10.1177/0306624X07304157.
Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive therapy of depression. New York: Guilford.
Belsky, J., Bakermans-Kranenburg, M. J., & van IJzendoorn, M. H. (2007). For better and for worse: Differential susceptibility to environmental influences. Current Directions in Psychological Science, 16(6), 300–304.
Belsky, J., Jonassaint, C., Pluess, M., Stanton, M., Brummett, B., & Williams, R. (2009). Vulnerability genes or “malleability” genes? Molecular Psychiatry, 14, 746–754. doi:10.1038/mp.2009.44.
Belsky, J., & Pluess, M. (2009). Beyond diathesis-stress: Differential susceptibility to environmental influences. Psychological Bulletin, 135(6), 885–908. doi:10.1037/a0017376.
Benjet, C., Thompson, R. J., & Gotlib, I. H. (2010). 5-HTTLPR moderates the effect of relational peer victimization on depressive symptoms in adolescent girls. Journal of Child Psychology and Psychiatry, 51(2), 173–179. doi:10.1111/j.1469-7610.2009.02149.x.
Biebl, S. J. W., DiLalla, L. F., Davis, E. K., Lynch, K. A., & Shinn, S. O. (2011). Longitudinal associations among peer victimization and physical and mental health problems. Journal of Pediatric Psychology, 36, 868–877. doi:10.1093/jpepsy/jsr025.
Caspi, A., McClay, J., Moffitt, T. E., Mill, J., Martin, J., Craig, I. W., et al. (2002). Role of genotype in the cycle of violence in maltreated children. Science, 297, 851–854. doi:10.1126/science.1072290.
Costello, E. J., Mustillo, S., Erkanli, A., Keeler, G., & Angold, A. (2003). Prevalence and development of psychiatric disorders in childhood and adolescence. Archives of General Psychiatry, 60, 837–844. doi:10.1001/archpsyc.60.8.837.
Daigle, L. E. (2010). Risk heterogeneity and recurrent violent victimization: The role of DRD4. Biodemography and Social Biology, 56(2), 137–149. doi:10.1080/19485565.2010.524095.
DiLalla, L. F. (2002). Preschool social and cognitive behaviors: The Southern Illinois Twins. Twin Research, 5, 468–471.
DiLalla, L. F., Elam, K. K., & Smolen, A. (2009). Genetic and gene–environment interaction effects on preschoolers’ social behaviors. Developmental Psychobiology, 51(6), 451–464. doi:10.1002/dev.20384.
DiLalla, L. F., Gheyara, S., & Bersted, K. (2013). The Southern Illinois Twins and Siblings Study (SITSS): Description and update. Twin Research and Human Genetics, 16(1), 371–375.
DiLalla, L. F., & John, S. G. (2014). Genetic and behavioral influences on received aggression during observed play with unfamiliar preschool-aged peers. Merrill-Palmer Quarterly, 60(2), 168–192.
Farbiash, T., Berger, A., Atzaba-Poria, N., & Auerbach, J. G. (2014). Prediction of preschool aggression from DRD4 risk, parental ADHD symptoms, and home chaos. Journal of Abnormal Child Psychology, 42(3), 489–499. doi:10.1007/s10802-013-9791-3.
Field, A. (2013). Discovering statistics using IBM SPSS statistics (4th ed.). Los Angeles: SAGE Publications Ltd.
Gini, G., & Espelage, D. L. (2014). Peer victimization, cyberbullying, and suicide risk in children and adolescents. JAMA: Journal of the American Medical Association, 312(5), 545–546. doi:10.1001/jama.2014.3212.
Goodman, R. (1997). The Strengths and Difficulties Questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38, 581–586. doi:10.1111/j.1469-7610.1997.tb01545.x.
Goodman, R. (2001). Psychometric properties of the Strengths and Difficulties Questionnaire (SDQ). Journal of the American Academy of Child and Adolescent Psychiatry, 40, 1337–1345.
Goodman, A., Lamping, D. L., & Ploubidis, G. B. (2010). When to use broader internalising and externalising subscales instead of the hypothesised five subscales on the Strengths and Difficulties Questionnaire (SDQ): Data from British parents, teachers and children. Journal of Abnormal Child Psychology, 38, 1179–1191. doi:10.1007/s10802-010-9434-x.
Goodman, R., & Scott, S. (1999). Comparing the Strengths and Difficulties Questionnaire and the Child Behavior Checklist: Is small beautiful? Journal of Abnormal Child Psychology, 27, 17–24. doi:10.1023/A:1022658222914.
Gottesman, I. I., & Shields, J. (1972). Schizophrenia and genetics: A twin study vantage point. New York: Academic Press.
Hawker, D. J., & Boulton, M. J. (2000). Twenty years’ research on peer victimization and psychosocial maladjustment: A meta-analytic review of cross-sectional studies. Journal of Child Psychology and Psychiatry, 41(4), 441–455. doi:10.1111/1469-7610.00629.
Heilbron, N., & Prinstein, M. J. (2010). Adolescent peer victimization, peer status, suicidal ideation, and nonsuicidal self-injury. Merrill-Palmer Quarterly, 56(3), 388–419. doi:10.1353/mpq.0.0049.
Hicks, B. M., DiRago, A. C., Iacono, W. G., & McGue, M. (2009a). Gene–environment interplay in internalizing disorders: Consistent findings across six environmental risk factors. Journal of Child Psychology and Psychiatry, 50, 1309–1317. doi:10.1111/j.1469-7610.2009.02100.x.
Hicks, B. M., South, S. C., DiRago, A. C., Iacono, W. G., & McGue, M. (2009b). Environmental adversity and increasing genetic risk for externalizing disorders. Archives of General Psychiatry, 66, 640–648.
Hodges, E. E., Boivin, M., Vitaro, F., & Bukowski, W. M. (1999). The power of friendship: Protection against an escalating cycle of peer victimization. Developmental Psychology, 35(1), 94–101. doi:10.1037/0012-1649.35.1.94.
Holder, M. D., & Coleman, B. (2009). The contribution of social relationships to children’s happiness. Journal of Happiness Studies, 10(3), 329–349. doi:10.1007/s10902-007-9083-0.
Hurvich, C. M., & Tsai, C. L. (1989). Regression and time series model selection in small samples. Biometrika, 76(2), 297–307. doi:10.2307/2336663.
Iyer, P. A., Dougall, A. L., & Jensen-Campbell, L. A. (2013). Are some adolescents differentially susceptible to the influence of bullying on depression? Journal of Research in Personality, 47(4), 272–281. doi:10.1016/j.jrp.2013.02.004.
Jiang, Y., Chew, S. H., & Ebstein, R. P. (2013). The role of D4 receptor gene exon III polymorphisms in shaping human altruism and prosocial behavior. Frontiers in Human Neuroscience, 7, 1–7. doi:10.3389/fnhum.2013.00195.
John, S. G., & DiLalla, L. F. (2013). Explaining differential reporting of victimization between parents and children: A consideration of social biases. Behavioral Sciences: Special Issue on Functional Perspectives on Emotion, Behavior, and Cognition, 3, 473–491. doi:10.3390/bs3030473.
Kendler, K. S. (2013). What psychiatric genetics has taught us about the nature of psychiatric illness and what is left to learn. Molecular Psychiatry, 18, 1058–1066. doi:10.1038/mp.2013.50.
Kendrick, K., Jutengren, G., & Stattin, H. (2012). The protective role of supportive friends against bullying perpetration and victimization. Journal of Adolescence, 35(4), 1069–1080. doi:10.1016/j.adolescence.2012.02.014.
Kennedy, E. (2013). Orchids and dandelions: How some children are more susceptible to environmental influences for better or worse and the implications for child development. Clinical Child Psychology and Psychiatry, 18(3), 319–321.
Kessler, R., Berglund, P., Demier, O., Jin, R., & Walters, E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62, 593–602.
Kirley, A., Lowe, N., Mullins, C., McCarron, M., Daly, G., Waldman, I., et al. (2004). Phenotype studies of the DRD4 gene polymorphisms in ADHD: Association with oppositional defiant disorder and positive family history. American Journal of Medical Genetics: Neuropsychiatric Genetics, 131, 38–42. doi:10.1002/dev.20249.
Klomek, A. B., Sourander, A., & Gould, M. (2010). The association of suicide and bullying in childhood to young adulthood: A review of cross-sectional and longitudinal research findings. The Canadian Journal of Psychiatry/La Revue Canadienne de Psychiatrie, 55(5), 282–288.
Knafo, A., Israel, S., & Ebstein, R. P. (2011). Heritability of children’s prosocial behavior and differential susceptibility to parenting by variation in the dopamine receptor D4 gene. Development and Psychopathology, 23(1), 53–67. doi:10.1017/S0954579410000647.
Kretschmer, T., Dijkstra, J. K., Ormel, J., Verhulst, F. C., & Veenstra, R. (2013). Dopamine receptor D4 gene moderates the effect of positive and negative peer experiences on later delinquency: The Tracking Adolescents’ Individual Lives Survey study. Development and Psychopathology, 25(4), 1107–1117. doi:10.1017/S0954579413000400.
Laird, R. D., Jordan, K. Y., Dodge, K. A., Pettit, G. S., & Bates, J. E. (2001). Peer rejection in childhood, involvement with antisocial peers in early adolescence, and the development of externalizing behavior problems. Development and Psychopathology, 13, 337–354.
Leung, P. L., & Wong, M. T. (1998). Can cognitive distortions differentiate between internalising and externalising problems? Journal of Child Psychology and Psychiatry, 39(2), 263–269. doi:10.1017/S0021963097001868.
López León, S., Croes, E. A., Sayed-Tabatabaei, F. A., Stephan, C., Van Broeckhoven, C., & van Duijn, C. M. (2005). The Dopamine D4 receptor gene 48-base-pair-repeat polymorphism and mood disorders: A meta-analysis. Biological Psychiatry, 57(9), 999–1003. doi:10.1016/j.biopsych.2005.01.030.
Maas, C. J. M., & Hox, J. J. (2005). Sufficient sample sizes for multilevel modeling. Methodology, 1, 86–92.
Majors, K. (2012). Friendships: The power of positive alliance. In S. Roffey & S. Roffey (Eds.), Positive relationships: Evidence based practice across the world (pp. 127–143). New York, NY, US: Springer Science + Business Media.
McGeary, J., Esposito-Smythers, C., Spirito, A., & Monti, P. (2007). Associations of the dopamine D4 receptor gene VNTR polymorphism with drug use in adolescent psychiatric inpatients. Pharmacology, Biochemistry and Behavior, 86, 401–406. doi:10.1016/j.pbb.2006.11.001.
Merikangas, K. R., He, J., Burstein, M., Swanson, S. A., Avenevoli, S., Cui, L., et al. (2010). Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). Journal of the American Academy of Child and Adolescent Psychiatry, 49(10), 980–989. doi:10.1016/j.jaac.2010.05.017.
Mynard, H., & Joseph, S. (2000). Development of the multidimensional peer victimization scale. Aggressive Behavior, 26, 169–178. doi:10.1002/(SICI)1098-2337(2000)26:2<169:AID-AB3>3.3.CO;2-1.
Newsome, J., & Sullivan, C. J. (2014). Resilience and vulnerability in adolescents: Genetic influences on differential response to risk for delinquency. Journal of Youth and Adolescence, 43(7), 1080–1095. doi:10.1007/s10964-014-0108-9.
Nikitopoulos, J., Zohsel, K., Blomeyer, D., Buchmann, A. F., Schmid, B., et al. (2014). Are infants differentially sensitive to parenting? Early maternal care, DRD4 genotype and externalizing behavior during adolescence. Journal of Psychiatric Research, 59, 53–59. doi:10.1016/j.jpsychires.2014.08.012.
Nugent, N. R., Tyrka, A. R., Carpenter, L. L., & Price, L. H. (2011). Gene–environment interactions: Early life stress and risk for depressive and anxiety disorders. Psychopharmacology (Berl), 214(1), 175–196. doi:10.1007/s00213-010-2151-x.
Oak, J., Oldenhof, J., & Van Tol, H. (2010). The dopamine D4 receptor: One decade of research. European Journal of Pharmacology, 405, 303–327. doi:10.1016/S0014-2999(00)00562-8.
Oland, A. J., & Shaw, D. S. (2005). Pure versus co-occurring externalizing and internalizing symptoms in children: The potential role of socio-developmental milestones. Clinical Child and Family Psychology Review, 8, 247–270.
Plomin, R., & Rutter, M. (1998). Child development, molecular genetics, and what to do with genes once they are found. Child Development, 69, 1223–1242. doi:10.2307/1132371.
Propper, C., Willoughby, M., Halpern, C. T., Carbone, M. A., & Cox, M. (2007). Parenting quality, DRD4, and the prediction of externalizing and internalizing behaviors in early childhood. Developmental Psychobiology, 49(6), 619–632. doi:10.1002/dev.20249.
Qualter, P., Brown, S. L., Rotenberg, K. J., Vanhalst, J., Harris, R. A., Goossens, L., et al. (2013). Trajectories of loneliness during childhood and adolescence: Predictors and health outcomes. Journal of Adolescence, 36(6), 1283–1293. doi:10.1016/j.adolescence.2013.01.005.
Ray, L. A., Bryan, A., MacKillop, J., McGeary, J., Hesterberg, K., & Hutchison, K. E. (2009). The dopamine D4 receptor (4) gene exon III polymorphism, problematic alcohol use and novelty seeking: Direct and mediated genetic effects. Addiction Biology, 14(2), 238–244. doi:10.1111/j.1369-1600.2008.00120.x.
Reijntjes, A., Kamphuis, J. H., Prinzie, P., Boelen, P. A., van der Schoot, M., & Telch, M. J. (2011). Prospective linkages between peer victimization and externalizing problems in children: A meta-analysis. Aggressive Behavior, 37(3), 215–222. doi:10.1002/ab.20374.
Reijntjes, A., Kamphuis, J. H., Prinzie, P., & Telch, M. J. (2010). Peer victimization and internalizing problems in children: A meta-analysis of longitudinal studies. Child Abuse and Neglect, 34(4), 244–252. doi:10.1016/j.chiabu.2009.07.009.
Roisman, G. I., Newman, D. A., Fraley, R. C., Haltigan, J. D., Groh, A. M., & Haydon, K. C. (2012). Distinguishing differential susceptibility from diathesis-stress: Recommendations for evaluating interaction effects. Development and Psychopathology, 24, 389–409. doi:10.1017/S0954579412000065.
Shojaei, T., Wazana, A., Pitrou, I., Gilbert, F., & Kovess, V. (2009). Self-reported peer victimization and child mental health: Results of a cross-sectional survey among French primary school children. Journal of Developmental and Behavioral Pediatrics, 30, 300–309. doi:10.1097/DBP.0b013e3181ad1e1a.
Simons, R. L., Lei, M. K., Beach, S. R. H., Brody, G., Philbert, R. A., & Gibbons, F. X. (2012). Social environmental variation, plasticity genes, and aggression: Evidence for the differential susceptibility hypothesis. American Sociological Review, 76(6), 833–912. doi:10.1177/0003122411427580.
Spatola, C. M., Fagnani, C., Pesenti-Gritti, P., Ogliari, A., Stazi, M., & Battaglia, M. (2007). A general population twin study of the CBCL/6-18 DSM-oriented scales. Journal of the American Academy of Child and Adolescent Psychiatry, 46(5), 619–627. doi:10.1097/CHI.0b013e3180335b12.
Spybrook, J., Bloom, H., Congdon, R., Hill, C., Martinez, A., & Raudenbush, S. (2011). Optimal design for longitudinal and multilevel research: Documentation for the optimal design software version 3.0. Available from www.wtgrantfoundation.org.
Sugden, K., Arseneault, L., Harrington, H., Moffitt, T. E., Williams, B., & Caspi, A. (2010). Serotonin transporter gene moderates the development of emotional problems among children following bullying victimization. Journal of the American Academy of Child and Adolescent Psychiatry, 49(8), 830–840. doi:10.1016/j.jaac.2010.01.024.
Turner, H. A., Finkelhor, D., Hamby, S. L., Shattuck, A., & Ormrod, R. K. (2011). Specifying type and location of peer victimization in a national sample of children and youth. Journal of Youth and Adolescence, 40(8), 1052–1067. doi:10.1007/s10964-011-9639-5.
Vaillancourt, T., Brittain, H. L., McDougall, P., & Duku, E. (2013). Longitudinal links between childhood peer victimization, internalizing and externalizing problems, and academic functioning: Developmental cascades. Journal of Abnormal Child Psychology, 41(8), 1203–1215. doi:10.1007/s10802-013-9781-5.
Werner, N. E., & Crick, N. R. (2004). Maladaptive peer relationships and the development of relational and physical aggression during middle childhood. Social Development, 13(4), 495–514. doi:10.1111/j.1467-9507.2004.00280.x.
Wolke, D., Lereya, S. T., Fisher, H. L., Lewis, G., & Zammit, S. (2014). Bullying in elementary school and psychotic experiences at 18 years: A longitudinal, population-based cohort study. Psychological Medicine, 44(10), 2199–2211. doi:10.1017/S0033291713002912.
Xiang, L., Szebeni, K., Szebeni, A., Klimek, V., Stockmeier, C., Karolewicz, B., & Ordway, G. (2008). Dopamine receptor gene expression in human amygdaloid nuclei: Elevated D4 receptor mRNA in major depression. Brain Research, 120, 7214–7224. doi:10.1016/j.brainres.2008.02.009183719402008-05136-022.
Jackson Growth Alliance website: http://www.jacksonbiz.org/infocenter/demojc.html
Acknowledgments
Funding for this study was provided by grants from SIUC, the Southern Illinois University School of Medicine, and the Center for Integrative Neuroscience-Cognitive Neurosciences (CIR-CNS) awarded to the first author. The authors wish to thank Dr. Andrew Smolen for expert assistance with genotyping. We also wish to thank all the families who graciously gave their time for this study.
Author contributions
LD conceived of the study, participated in its design and coordination, performed the statistical analyses, and drafted the manuscript; KB conceived of the study, participated in interpretation of the data, and helped to draft the manuscript; SJ participated in the design and interpretation of the data and helped to draft the manuscript. All authors read and approved the final manuscript.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
DiLalla, L.F., Bersted, K. & John, S.G. Peer Victimization and DRD4 Genotype Influence Problem Behaviors in Young Children. J Youth Adolescence 44, 1478–1493 (2015). https://doi.org/10.1007/s10964-015-0282-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10964-015-0282-4