
Abstract
This paper reviews empirical studies conducted on the role of spirituality and religiosity (S/R) characteristics in 12-step recovery among program members followed up after substance abuse treatment and those assessed independent of formal treatment. Aspects of spiritual functioning that change in relation to program participation and those S/R characteristics that were found to mediate the association between program involvement and drinking-related outcomes are discussed. In addition, a review is provided of 12-step program studies investigating S/R-related predictors of clinical outcomes relevant to risk of relapse among members in long-term recovery. To further examine the role of S/R characteristics in recovery, a study was conducted on long-term AA members to assess the relationship of S/R characteristics and AA program involvement to craving for alcohol and emotional distress after controlling for relevant demographic variables. Feeling God’s presence daily, believing in a higher power as a universal spirit, and serving as an AA sponsor were all predictive of positive outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Spirituality is a multifaceted construct which has received increased attention with regard to its role in the maintenance of recovery from alcoholism. Spirituality has been defined as that which gives meaning and purpose in life (Puchalski 2003) as well as a sense of personal identity and transcendence that motivate individuals beyond the practicalities of daily living (Galanter et al. 2011). The search for meaning and personal identity may be expressed through participation in a religion, but it can be much broader than that encompassing involvement in family, humanism, or the arts (Puchalski and Ferrell 2010). In American culture, spirituality has come to be seen as a human dimension, particularly useful in bridging sectarian divisions common to religion (Galanter 2005).
Spirituality is central to Alcoholics Anonymous (AA) as demonstrated in the 12 steps that members apply in working the program as well as in the Twelve Traditions that pertain to the operation of the AA groups. The origins of AA can be traced to the influence of the Oxford Group, a Christian evangelical group which advocated self-examination, acknowledgment of character defects, restitution for harm done, and sharing with others (AA World Services 1957). Bill W., a New York stockbroker, was unable to attain sobriety despite repeated attempts to stop drinking. Receiving guidance from the Oxford Group, Bill was able to quit drinking after an intense spiritual experience he characterized in terms of a vision of a “white light.” Bill was influenced by a childhood friend in recovery from alcoholism. This friend advised him that he could only remain sober if he helped another alcoholic. Toward this end, Bill met Dr. Bob, a physician alcoholic who was able to achieve sobriety through Bill’s support. Together Bill and Dr. Bob founded AA in 1935, and within a few years, AA had a total of 100 members. Since that first meeting in 1935, there has been a tremendous increase in the spread of AA. Today the General Service Office of AA estimates that there are over 114,000 groups in operation in 170 countries with more than 2 million members worldwide (AA Fact File 2015). As interest in the movement spread on the part of alcoholics and non-alcoholics, it was decided that the movement be clearly separate from any organization. AA would have no affiliation with any religious or professional treatment organization nor would it receive any form of financial support. Being self-supporting was crucial for AA to minimize the likelihood of their groups being diverted from their primary mission, i.e., to carry the message to other alcoholics. It is suggested that no AA group be named after any individual so that members can “place principles before personalities.” In 1938, a book was published, Alcoholics Anonymous known as the “Big Book” to serve as the basic text. Meetings are open to anyone who has a desire to quit drinking and can consist of as few as 2–3 alcoholics gathered together with no other affiliation. Groups are run with the principle of rotation to ensure that group tasks in AA are shared. Group members are expected to do their fair share to foster AA’s three basic legacies: recovery, unity, and service. As a program of recovery, AA group leaders do not govern. They are regarded as trusted servants administering a program developed by and for persons with alcoholism. Alcoholics Anonymous as a spiritual recovery movement views addiction as an illness of the mind, body, and spirit, and requires a commitment to abstinence, and a working of the 12 steps.
Working the 12 steps is aimed at fostering an enhanced awareness and functionality of one’s personal orientation to God, with 6 of the 12 steps referring to God of the person’s own understanding: The first includes acceptance (step 2) followed by surrender (step 3), admission of wrongs (step 5), readiness to have God remove character defects (step 6), request to have God remove these defects (step 7), and finally of most relevance perhaps to the maintenance of sobriety and spiritual growth is the seeking through prayer and meditation to improve conscious contact with God (step 11). According to the AA program, working through the first 11 steps will lead to a spiritual awakening or new state of consciousness—one characterized by reliance on God and a joy of living, in which giving is its own reward.
The Twelve Traditions which embody the fellowship of sharing and support are principles applicable to the functioning of AA groups. The traditions are meant to serve as guidelines for AA groups to weather conflict and to function smoothly in the absence of a formal structured governing organization (Detar 2011). Tradition Two explicitly acknowledges the ultimate authority overseeing the group mission, which is “a loving God as He may express Himself in our group conscience.” Tradition Five, which addresses the primary function of the group, is intended to carry a specific message to other alcoholics: The ability to bring about recovery is a gift from God which is meant to be shared with others.
Engagement in the AA program may result in either a reactivation of a spiritual state which may have become dormant while the individual was actively using alcohol or the creation of a new spiritual identity with its attendant beliefs, practices, and experiences. The assessment of spirituality-related characteristics in relation to positive outcomes of AA program participation has been an active area of research especially in regard to the role such characteristics may play in early and long-term recovery. Even though a distinction can be made between AA spirituality and formal religion, certain AA beliefs and practices, such as belief in a deity and engaging in prayer practices, may be similar to those found in organized religion. Therefore, many of the studies conducted on spirituality in AA apply instruments used in the assessment of individual differences in religiosity as well as measures reflecting AA-specific spiritual principles and practices.
A number of cross-sectional and longitudinal studies which have assessed how relevant spiritual/religious (S/R) characteristics relate to AA program participation in terms of meeting attendance, 12-step work, sponsorship, and service will be reviewed below. Recent research on S/R characteristics, which may mediate the relationship between AA program participation and alcohol use in treatment-seeking samples, will also be reviewed. Finally, survey studies conducted on long-term, committed AA/NA members addressing S/R predictors of clinical outcomes relevant to relapse will be discussed. To further examine the role of S/R characteristics in recovery, we describe the results of a study on long-term AA members to assess the relationship of S/R characteristics and AA program involvement to craving for alcohol and emotional distress.
Carroll (1993) studied 100 members of AA recruited from 20 different AA groups with respect to spirituality, the extent of engagement in step 11 and step 12 practices, the number of AA meetings attended, and the length of sobriety. The indicator of spirituality in this study was selected to reflect perceived change in purpose and meaning in life. The measure, based on Crumbaugh and Maholick’s (1964) Purpose in Life (PIL) questionnaire, was adapted to assess individuals’ beliefs before and after achieving sobriety. Carroll found that PIL was positively associated with step 11 practice and number of AA meetings attended but unrelated to the length of sobriety.
Mathew et al. (1996) assessed a sample of 62 AA/NA members recovering from substance abuse with a minimum of 6 months of abstinence. For comparison purposes, a sample of 61 volunteers free of alcohol or drug use disorders was recruited. Mathew et al. administered the Mathew Materialism Spiritualism Scale (MMSS) and derived six empirically distinct subscales: (1) beliefs concerning God, (2) belief in the value of religious practices, (3) mystical experiences, (4) belief in the existence of spirits, (5) core character values (e.g., altruism), and (6) belief in paranormal phenomena. In order to better assess the potential range of spiritual experiences that may occur in 12-step program recovery, Mathew et al. developed a second instrument, the Cognitive Pattern Scale (CPS), which taps the ability to appreciate aesthetics such as art, music, poetry. The AA/NA members were asked to complete each measure twice, first with respect to their current status of continuous sobriety and then again with respect to their active substance abusing days. The comparison group subjects were asked to complete the measures only once to reflect their current state. With the exception of belief in the paranormal, the CPS and MMSS scores were higher after the achievement of abstinence in the AA/NA member group. With respect to most MMSS scores, the 12-step member sample was similar to the comparison group with the single exception of the mysticism scale where the AA/NA members exhibited higher scores.
Caldwell and Cutter (1998) assessed acceptance of a HP in a sample of 55 clients following 12-step-based treatment for alcohol use disorders in relation to the number of meetings attended during the 3 months following discharge. Their S/R measure was based on Gilbert’s (1991) Steps questionnaire which reflects elements of “came to believe” and “turning it over” as embodied in AA’s first three steps. Three levels of AA meeting attendance emerged: (1) low, unstable attenders with fewer than 20 meetings attended; (2) mid-level attenders with 20–59 meetings attended, and (3) on-schedule attendees, on track to fulfill the “90-in-90” AA program recommendation. The on-schedule attendees had greater acceptance of a HP than the mid- and low-level attendees. This finding highlights the importance of regular meeting attendance within the 3 months following formal treatment. Young (2013) measured a similar S/R construct in a study of AA member sponsorship. He administered an online survey instrument to 264 AA members which included Reinert’s (1997) Surrender Scale as well as items assessing frequency of prayer. The Surrender Scale embodies the concept of acknowledging one’s limitations, giving up control, and accepting a HP. Sponsored AA members engaged in daily prayer practice more often and experienced a greater level of surrender than did those without a sponsor.
Horstmann and Tonigan (2000) explored an aspect of spirituality involving the nature of the God relationship relative to AA program participation and abstinence. The authors drew from Pargament’s (1988) religious coping style model, which posits three styles: (1) “self-directing,” in which an individual addresses problems alone without turning to God/HP; (2) “deferring,” in which the person depends on God/HP for a solution; and lastly (3) “collaborative,” in which problems of adjustment are addressed jointly. Forty-seven study participants were recruited from two AA groups within the community. Scores on Pargament’s religious coping style questionnaire (short version) were assessed in relation to AA involvement as measured by the Alcoholics Anonymous Involvement (AAI) (Tonigan et al. 1996a) Scale. The AAI questionnaire includes items concerning meeting attendance, program practices, and step completion. No relationship was found between collaborative coping style and number of AA steps completed. However, a positive relationship emerged between collaborative coping style and abstinence.
Kelly and Moos (2003) assessed the relationship of religious affiliation to risk of 12-step program dropout among 2,778 male VA patients within the 12 months following intensive substance use disorder treatment. Two measures of religious affiliation were obtained: (1) formal religious self-designation with categories of Catholic, Jewish, Protestant, other, or none; and (2) frequency of attendance at religious services. Both self-identified formal religious affiliation and frequency of religious service attendance assessed at baseline were associated with lower dropout rates at 1 year after discharge. Tonigan et al. (2002) analyzed data from Project MATCH, a multisite randomized clinical trial of Twelve-Step Facilitation, Cognitive Behavior Therapy, and Motivational Enhancement with 1,726 clients to explore whether religious affiliation would predict AA program participation at 12-month follow-up. The primary S/R instrument administered in Project MATCH was the Religious Background and Behavior (RBB) questionnaire assessing S/R self-designation, God experiences/consciousness (GC), and formal practices (FP). With regard to S/R self-designation, respondents are asked to choose among the following categories: (1) atheist, (2) agnostic, (3) unsure, (4) spiritual (“I believe in God, but I’m not religious”, and (5) religious (“I believe in God and practice religion”). Clients describing themselves as either atheist or agnostic had lower AA meeting attendance compared to those with a spiritual or religious identification. However, no differences were found between the atheist–agnostic group and those who identified as spiritual or religious with respect to drinking outcome.
Zemore and Kaskutas (2004) administered a survey to 200 recovering alcoholics recruited directly from AA meetings in addition to formal treatment programs and the self-help organization Women for Sobriety. The Daily Spiritual Experiences (DSE) (Underwood 1999) Scale was administered to the clients. Underwood reported a unidimensional factor structure reflecting perceptions of one’s connection to God and life. However, in a factor analysis of DSE items in their sample, Zemore and Kaskutas derived two empirically distinct dimensions: Theism (perception of God experiences) and Self-Transcendence (feelings of connection to others and the universe). They assessed the pattern of interrelationships among the spirituality measures, three forms of helping (helping within recovery, within life, and within community), the length of sobriety, and AA program involvement as assessed by the Alcoholics Anonymous Affiliation (AAA) (Humphreys et al. 1998) Scale. The AAA Scale contains items assessing meeting attendance, sponsorship, and activities such as relying on AA members for assistance and reading AA literature. Zemore and Kaskutas conducted a factor analysis on these items and derived two dimensions which they labeled “AA involvement,” reflective of current status, and “AA achievement,” indicative of completion of the Twelve Steps and serving as a sponsor. Theism was positively correlated with AA involvement, AA achievement, recovery and life helping, and the length of sobriety. Self-Transcendence was positively related to the length of sobriety and to all forms of helping but had no association with any of the AAA measures.
There exists another body of research findings which deals with studies conducted mainly on treatment samples in early recovery. This research addresses the issue of whether certain S/R characteristics mediate the relationship between AA program participation and abstinence. Kaskutas et al. (2003) assessed a sample of 587 clients drawn from public and private treatment programs that had been studied by the Alcohol Research Group and followed them for a period of 3 years. Baseline S/R self-designation as assessed in the RBB was not associated with the number of AA meetings attended nor with the odds of achieving sobriety at third-year follow-up. At this follow-up, having had a spiritual awakening as a result of their involvement in AA (reflective of past year occurrence) was positively associated with clients’ continuous sobriety for that year. Using Project MATCH data with 952 clients, Tonigan (2003) found that AA participation as assessed by the AAI-AA practices component was associated with having had a spiritual awakening. Spiritual awakening was unrelated to abstinence at the 3-year follow-up.
Robinson et al. (2007) studied 123 outpatients to investigate the relationship of drinking outcomes to change in S/R characteristics from treatment entry to 6-month follow-up. A series of 5 instruments was administered to derive a total of ten S/R measures: (1) the Brief Multidimensional Measure of Religiousness and Spirituality (BMMRS, Fetzer Institute/NIA 1999), which generates two S/R scores, one score reflecting beliefs and values relating to sense of meaning in one’s life, responsibility for reducing one’s suffering, and God beliefs and a second S/R-related scores reflecting forgiveness involving self, others, and God; (2) RBB which generates a second pair of S/R scores—S/R self-designation and RBB FP component; (3) DSE scored in terms of a single dimension derived from a factor analysis conducted by Robinson et al.; (4) the Brief Religious Coping Scale adapted from Pargament’s (1998) original version which generates two S/R measures—positive religious coping and negative religious coping; (5) Loving and Controlling God Scales (Benson and Spilka 1973); and (6) the PIL questionnaire. The AAI measure used in this study was modified to include an item on AA service. Over the 6 months, there were increases in AAI scores accompanied by increases in DSE, forgiveness, positive religious coping, and PIL. Increases in DSE and PIL were associated with a decreased likelihood of heavy drinking at the 6-month follow-up.
Zemore (2007) found that increases in S/R as assessed by the RBB composite score (i.e., S/R designation + FP + GC) and occurrence of spiritual awakening mediated the relationship between 12-step participation (as measured by the AAA) and 1-month abstinence at the 12-month follow-up. The sample of 733 clients was drawn from participants in a clinical outcomes study of 733 patients in chemical dependency treatment. Oakes (2008) assessed PIL as a mediator among 78 participants drawn from AA clubs. Purpose in life was associated with AA participation as assessed by the AAI but was unrelated to the length of sobriety. In order to test for S/R variables which may mediate the effects of AA participation on alcohol use, Kelly et al. (2011) analyzed Project MATCH data with a sample of 1,726 adults. Assessments were collected at treatment intake and 3-, 9-, and 15-month follow-ups. The RBB composite scores combining S/R self-designation, GC, and FP components were used in the mediational analyses. Attendance in AA was consistently associated with improved subsequent alcohol drinking outcomes. This relationship was partially mediated by increases in RBB measures. On the basis of a meta-analysis of these aforementioned 6 studies, Tonigan et al. (2013) concluded that measures of AA participation were predictive of increased abstinence, with the magnitude of this effect similar to those reported in earlier meta-analytic studies (Emrick et al. 1993; Tonigan et al. 1996b). Overall, empirical support was demonstrated for S/R characteristics as partial mediators of the relationship between AA participation and increased abstinence.
Tonigan et al. (2013) noted that the Project MATCH sample used by Kelly et al. (2011) may have limited generalizability in that Kelly’s subjects were mostly non-Hispanic white males without comorbid substance use disorders. To address whether the Kelly et al. findings could be replicated with a broader sample, Tonigan et al. employed the same research design (i.e., fully time-lagged), in which they interviewed 130 12-step program attendees recruited from outpatient treatment centers, community shelters, and AA meetings. Clients were assessed at baseline and quarterly over a 9-month period in order to assess changes in S/R characteristics that may be predictive of abstinence. The target AA samples were those in early recovery (one had to be attending AA not more than 16 weeks). Changes in God consciousness experiences were measured by using a modified version of the original RBB-GC (MGC). Here meditation was scored as part of the God Consciousness dimension instead of the FP component as originally scored by Connors et al. These changes in the God consciousness experience predicted increased percent days abstinent even after controlling for concurrent formal treatment-seeking. The mediational analysis on 12-step meeting attendance and 9-month drinking outcome indicated that MGC accounted for 22 % of the direct effect of AA attendance on subsequent percent days abstinent.
In a sample of 364 clients drawn from participants in the Life Transitions Study, a 3-year longitudinal study of alcohol dependent individuals, Krentzman et al. (2013) tested potential mediating effects of multiple S/R characteristics. Six measures of spirituality were tested: (1) private religious practices (PRP representing composite measure of frequency of prayer, meditation, scripture reading, watching religious television programs, and saying grace before meals, Fetzer 1999), (2) DSE [single composite score per Underwood and Teresi (2002) original scoring], (3) forgiveness of others, and (4) forgiveness of self (Mauger, Forgiveness Scale 1992), (5) negative religious coping (Pargament et al. 1998), and (6) PIL. Participation in AA assessed in terms of meeting attendance and a modified version of the AAI questionnaire predicted increases in PRP, DSE, and forgiveness of others. Of these three potential S/R-mediating variables, only PRP (measured at 1-year follow-up) was found to mediate the relationship between AA involvement (measured at 6-month follow-up) and alcohol use at the 1.5-year follow-up.
This last set of studies assesses S/R characteristics and program functioning in relation to clinical outcomes relevant to relapse among long-term AA/NA members based in the community. These samples were assessed independent of their being followed up from any prior treatment. These cross-sectional studies were designed to be in accordance with the 12th AA Tradition, the need to preserve members’ anonymity. Therefore, the names of the participants were not obtained, and they were surveyed in such a way that they could not be individually identified by their responses. The major survey components included (1) S/R characteristics relevant to AA spirituality (e.g., belief in a personal God) and formal religious practices (frequency of church attendance); (2) program functioning characteristics (e.g., length of sobriety, level of affiliativeness to group members, sponsorship), and (3) clinical outcomes relevant to relapse (e.g., level of anxiety, craving for alcohol and/or drugs). In a sample of 144 physicians at a conference of doctors in AA recovery, 81 % reported a spiritual awakening (Galanter et al. 2013a). The majority (60 %) described themselves as spiritual and not religious. Having had a spiritual awakening was associated with a longer period of recent abstinence and with the absence of alcohol craving during the previous week.
In a study of Narcotics Anonymous conducted with the cooperation of the Narcotics Anonymous World Service Office (NAWSO), 527 NA members from 3 states were administered a survey similar to that employed with the AA member sample (Galanter et al. 2013b). Similar to the physician AA member sample, 84 % reported a spiritual awakening. Again, most viewed themselves as spiritual and not religious (65 %). Those reporting feeling God’s presence on a daily basis (54 % of the total sample) had a longer duration of abstinence, a lower level of depression, and were more likely to report the absence of craving for substances. In another study of NA members, in which the NAWSO agreed to select a diverse group of US meetings which were likely to have attendees who were veterans, a survey was administered to a total of 508 members in 5 states (Galanter et al. 2014b). Those having had a spiritual awakening (i.e., 82 %) had been sober longer, had a higher level of affiliative feelings toward group members, were more likely to have sponsored more than 5 fellow members, and experienced less craving for substances and lower depression in the week prior to survey completion. Sixty-four percent reported feeling God’s presence on a daily basis.
To further examine the role that God/HP experiences and beliefs may play in 12-step recovery, the relationship of feeling god’s presence to clinical outcomes relevant to risk of relapse was assessed relative to other S/R characteristics and program functioning. The source of survey data that were used in these analyses was drawn from a sample of AA members attending an annual conference of Young People in Alcoholics Anonymous (YPAA). The survey is described in detail in our earlier report on 266 respondents (mean age = 26.9, SD = 5.21) where those below age 25 were compared with those between age 25 and 39 on prior substance use, formal treatment experience, and AA program functioning-related variables (Galanter et al. 2012). At the YPAA conference, a total of 358 attendees volunteered at registration to complete the survey, 90 % of whom had complete data yielding a sample size of 322. The findings presented below are based on data collected on these 322 attendees (mean age = 32.8, SD = 8.81). Similar to the other community-based AA/NA member samples we studied, most had a spiritual awakening (94 %) and reported frequent meeting attendance in the year prior to completing the survey (mean = 230.6 meetings, SD = 138.9) and were abstinent on average 7.2 years (SD = 8.81). Their first encounter with AA was on average 10.6 years (SD = 9.4) prior to the completion of the survey. Two-thirds of the sample had sponsored multiple AA members. The two clinical outcomes relevant to risk of relapse that were assessed included the level of anxiety and alcohol craving. We first assessed the relationship of background variables to each outcome for potential use in our predictive models as covariates: age, gender, source of referral to AA, employment status, prior treatment for substance abuse, and general psychiatric problems. Of all the background variables assessed, only age and employment status were significantly related to the level of anxiety. Older AA members and those who were employed had lower anxiety. The only background variable related to alcohol craving was age, with older respondents reporting less craving. The S/R variables entered into the predictive models included feeling God’s presence daily, belief in a personal God, belief in a HP as a universal spirit, and weekly church attendance. The program functioning-related variables entered into the models included the length of abstinence, extent of affiliativeness with other AA members, and sponsorship of other AA members. After controlling for age and employment status, the following program related and S/R characteristics retained significance (F = 8.01, df = 9, 312, p < .0001, R 2 = .188): Serving as a sponsor (β = −219, p = .01), feeling God’s presence daily (β = −.147, p = .011), level of affiliativeness to AA members (β = −.114, p = .03), and belief in HP as a universal spirit (β = −.107, p = .04) were associated with lower anxiety. The results of a multiple logistic regression analysis indicated that sponsoring other AA members (adjusted OR 2.07, p = .02), belief in a HP as a universal spirit (adjusted OR 2.04, p = .01), and feeling God’s presence daily (adjusted OR 1.79, p = .05) emerged as significant unique predictors of the absence of craving. Weekly church attendance was not related to the level of anxiety or the absence of craving.
Discussion
In studies conducted on 12-step program members, a number of S/R characteristics have been shown to (1) increase after members have achieved sobriety, (2) correlate with specific aspects of program participation, (3) partially mediate the relationship between program involvement and drinking-related outcomes, and (4) predict clinical outcomes relevant to risk for relapse. The results from the Mathew et al. (1996) study suggest that, among AA members who achieve at least 6 months of abstinence, change occurs across multiple domains of spiritual functioning encompassing heightened God experiences, religious affiliation, mystical experiences, and appreciation of character values and aesthetics. These S/R characteristics are consistent with strengths associated with the core virtue of transcendence that underlies a basic sense of authentic happiness, fulfillment, and well-being in life (Peterson and Seligman 2004). Transcendence is one of the six core virtues that emerged from analyses of the literature of ancient philosophical and religious traditions across different historical periods and cultures (Dahlsgaard et al. 2005). As such, these core virtues may have biological and evolutionary bases for survival at both the group and societal levels. In theory and practice, the AA model articulates the basis for developing strengths associated with these core virtues. It is not unexpected that research on AA itself yielded empirical findings illustrative of the potential for the development of human strengths associated with these very core virtues.
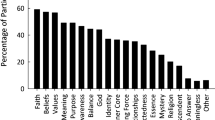
Compared to non-alcoholics, 12-step group members were found to be higher in mysticism, one key spiritual belief espoused in AA (Connors et al. 2008). Because quitting drinking may be perceived as nothing short of a miracle from God, it would be expected that 12-step program members who have maintained sobriety might experience increases in spirituality relating to the attachment to God and mystical experiences. Rather than reflecting good luck or chance occurrence, attainment of sobriety in AA is viewed as originating from what has been referred to as a “transcendental intervention” reflecting a larger purpose or reality (Connors et al. 2008). The practice of step 11, involving prayer and meditation to improve one’s conscious contact with God may move one toward such an awareness. Carroll (1993) found that application of step 11 was associated with greater PIL. Step 12 refers to having a spiritual awakening and carrying the message on to other alcoholics. The spiritual awakening experience in and of itself may contribute to an enhanced sense of PIL. In a study of spiritual awakening in AA, Galanter et al. (2014a) reported that personal meaning was one of the dimensions underlying members’ characterization of their first spiritual awakening.
Another S/R characteristic which was found to correlate with specific aspects of program participation was that of surrender, which refers to turning one’s will over to God/HP, with the acknowledgment that one is powerless over the use of alcohol. Acceptance of surrender to a HP was greater among those members with a pattern of meeting attendance that approximated 90 meetings in 90 days following alcoholism treatment (Caldwell and Cutter 1998) and among those AA members with a sponsor (Young 2013). Newcomers to 12-step programs are encouraged to obtain a sponsor early in the program. Young reported that having a sponsor was also associated with a higher frequency of one’s engaging in prayer or meditation. An AA sponsor may promote a supportive context for engaging in prayer and meditation and one’s readiness to surrender to God or to a HP.
Using a broader measure of AA program involvement encompassing attendance at meetings, sponsorship, and other activities such as reading AA literature, Zemore and Kaskutas (2004) found that such involvement was correlated with a heightened perception of God-related experiences. As measured by a component derived from the DSE instrument, self-transcendence was unrelated to aspects of AA program involvement. Zemore and Kaskutas found, however, that self-transcendence was associated with AA members helping in recovery and with non-recovery-related matters and helping within the community at large. A full sense of transcendence may be more likely to evolve over the course of helping other AA members in recovery combined with helping those outside the AA program.
Consistent with prior research, Robinson et al. (2007) found, that with increasing involvement in AA, members reported a higher level of daily spiritual experiences involving attachment to God and PIL. Positive religious coping and forgiveness, two other S/R characteristics, were found to increase over the 6-month assessment period. Positive religious coping entails a trust in God/HP for guidance and direction in abstaining from drinking as well as in maintaining attitudes and behaviors which facilitate recovery. Steps 4 through 10 of AA involve conducting a moral self-inventory, listing persons one has harmed and making amends to them, which often involves forgiveness of oneself and others. The precontemplation, contemplation, and action processes inherent in the practice of steps 8 and 9 relate to various dimensions of forgiveness and reconciliation (Hart 1999). The significance of forgiveness increasing over the course of AA program participation can also be viewed from the perspective of the core human virtue of temperance (Peterson and Seligman 2004; Dahlsgaard et al. 2005). Forgiveness is considered to be a strength which can safeguard against excesses in life and promote tolerance.
The S/R characteristics found to partially mediate the relationship between 12-step program participation and drinking outcomes reflect God consciousness experiences, S/R practices, or a combination of both (e.g., RBB composite and component measures). Empirical support for the mediating effects on recovery of a spiritual awakening and the spirituality variables as measured by the DSE and PIL instruments was mixed. Given the variability that exists with regard to the underlying dimensions of a spiritual awakening as well as differences in type of onset (i.e., sudden vs. gradual), and the likelihood that individuals may experience more than one episode over the course of AA participation, spiritual awakening may not have been found to be a mediator in all cases. With respect to mediational tests using the DSE and PIL questionnaire measures (Krentzman et al. 2013; Oakes 2008; Robinson et al. 2007), the inconsistency in findings may be due in part to differences in the AA member study samples, mediational test procedures, and the time frames employed in these studies.
A broader issue requiring further investigation regards the testing of the mediators involving meditation within 12-step programs. It is unclear whether meditation embodies a state of God consciousness or rather denotes a spiritual practice as suggested by Connors et al. in their original scoring of the RBB. Prayer and meditation are sometimes referred to as talking and listening, respectively (AA 2003). As meditation may embody a state as well as an action, future investigations addressing the manner in which AA members come to understand and experience meditation as a process and end-state may advance addiction treatment providers’ knowledge of spiritual processes in AA recovery.
The S/R characteristics that may play a role in long-term recovery among AA members who have maintained sobriety include feeling God’s presence on a daily basis, believing in the universality of a HP, and program involvement in the form of sponsoring fellow AA members. The frequency of church attendance was unrelated to clinical outcomes. Church attendance per se may not reflect aspects of religious involvement such as intrinsic motivation (Salsman et al. 2005) that promote recovery. According to Connors et al. (2008), one fundamental belief in AA is the need for spiritual renewal on a daily basis. Feeling God’s presence on a day-to-day basis may facilitate such renewal and also prevent the realization of the miracle of sobriety from fading from one’s awareness. A sense of gratitude, which embodies appreciation for the gift of sobriety, may be central to the renewal process. Belief in the universality of a HP and provision of fellowship support may enable long-term AA members to sustain what has been referred to as “living the program.” Here, through the recognition of the universal spirit linking all humanity, members develop a kinship to others both within and outside the program. It is through this ongoing AA fellowship involvement that members may continue to fulfill a larger purpose in society.
References
Alcoholics Anonymous World Services. (1957). Alcoholics Anonymous comes of age: A brief history of A.A. New York, NY: Alcoholism Anonymous World Services.
Alcoholics Anonymous World Services. (2015). A. A. Fact File. New York, NY: Alcoholics Anonymous World Services. Accessed February 5, 2015, http://www.aa.org/assets/en_US/aa-literature/m-24-aa-fact-file.
Alcoholics Anonymous (AA). (2003). Spiritual awakening: Journeys of the spirit from the pages of the AA Grapevine. New York, NY: AA Grapevine.
Benson, P., & Spilka, B. (1973). God image as a function of self-esteem and locus of control. Journal for the Scientific Study of Religion, 12, 297–310.
Caldwell, P. E., & Cutter, H. S. (1998). Alcoholics Anonymous affiliation during early recovery. Journal of Substance Abuse Treatment, 15(3), 221–228.
Carroll, S. (1993). Spirituality and purpose in life in alcoholism recovery. Journal of Studies on Alcohol, 54(3), 297–301.
Connors, G. J., Walitzer, K. S., & Tonigan, J. S. (2008). Spiritual change in recovery. In M. Galanter & L. A. Kaskutas (Eds.), Recent developments in alcoholism (pp. 209–227). Totowa, NJ: Humana Press.
Crumbaugh, J. C., & Maholick, L. T. (1964). An experimental study in existentialism: The psychometric approach to Frankl’s concept of noogenic neurosis. Journal of Clinical Psychology, 20, 200–207.
Dahlsgaard, K., Peterson, C., & Seligman, M. E. P. (2005). Shared virtue: The convergence of valued human strengths across culture and history. Review of General Psychology, 9(3), 203–213.
Detar, D. T. (2011). Alcoholics Anonymous and other twelve-step programs in recovery. Primary Care Clinical Office Practice, 38(1), 143–148.
Emrick, C. D., Tonigan, J. S., Montgomery, H. A., & Little, L. (1993). Alcoholics Anonymous: What is currently known? In B. S. McCrady & W. R. Miller (Eds.), Research on Alcoholics Anonymous: Opportunities and alternatives (pp. 41–76). Piscataway, NJ: Rutgers Center for Alcohol Studies.
Fetzer Institute/National Institute on Aging. (1999). Multidimensional measurement of religiousness/spirituality for use in health research: A report of the Fetzer Institute/National Institute on Aging Working Group, with additional psychometric data. Kalamazoo, MI: Fetzer Institute.
Galanter, M. (2005). Spirituality and the healthy mind. Science, therapy, and the need for personal meaning. New York, NY: Oxford University Press.
Galanter, M., Dermatis, H., Post, S., & Sampson, C. (2013a). Spirituality-based recovery from drug addiction in the twelve-step fellowship of Narcotics Anonymous. Journal of Addiction Medicine, 7(3), 189–195.
Galanter, M., Dermatis, H., & Sampson, C. (2014a). Spiritual awakening in Alcoholics Anonymous: Empirical findings. Alcoholism Treatment Quarterly, 32(2–3), 319–334.
Galanter, M., Dermatis, H., & Sampson, C. (2014b). Narcotics Anonymous: A comparison of military veterans and non-veterans. Journal of Addictive Diseases, 33, 187–195.
Galanter, M., Dermatis, H., & Santucci, C. (2012). Young people in Alcoholics Anonymous: The role of spiritual orientation and AA member affiliation. Journal of Addictive Diseases, 31(2), 173–182.
Galanter, M., Dermatis, H., Stanievich, J., & Santucci, C. (2013b). Physicians in long-term recovery who are members of Alcoholics Anonymous. The American Journal on Addiction, 22(4), 323–328.
Galanter, M., Dermatis, H., Talbot, N., McMahon, C., & Alexander, M. J. (2011). Introducing spirituality into psychiatric care. Journal of Religion and Health, 50, 81–91.
Gilbert, F. S. (1991). Development of a “Steps Questionnaire”. Journal of Studies on Alcohol and Drugs, 52(4), 353–360.
Hart, K. E. (1999). A spiritual interpretation of the 12-steps of Alcoholics Anonymous: From resentment to forgiveness to love. Journal of Ministry in Addiction & Recovery, 6(2), 25–39.
Horstmann, M. J., & Tonigan, J. S. (2000). Faith development in Alcoholics Anonymous (AA): A study of two AA groups. Alcoholism Treatment Quarterly, 18(4), 75–84.
Humphreys, K., Kaskutas, L. A., & Weisner, C. (1998). The Alcoholics Anonymous Affiliation Scale: Development, reliability, and norms for diverse treated and untreated populations. Alcoholism: Clinical and Experiential Research, 22, 974–978.
Kaskutas, L. A., Turk, N., Bond, J., & Weisner, C. (2003). The role of religion, spirituality and Alcoholics Anonymous in sustained sobriety. Alcoholism Treatment Quarterly, 21(1), 1–16.
Kelly, J. F., & Moos, R. (2003). Dropout from 12-step self-help groups: Prevalence, predictors, and counteracting treatment influences. Journal of Substance Abuse Treatment, 24(3), 241–250.
Kelly, J. F., Stout, R. L., Magill, M., Tonigan, J. S., & Pagano, M. E. (2011). Spirituality in recovery: A lagged mediational analysis of Alcoholics Anonymous’ principal theoretical mechanism of behavior change. Alcoholism: Clinical and Experimental Research, 35(3), 454–463.
Krentzman, A. R., Cranford, J. A., & Robinson, E. A. (2013). Multiple dimensions of spirituality in recovery: A lagged meditational analysis of Alcoholics Anonymous’ principal theoretical mechanism of behavior change. Substance Abuse, 34(1), 20–32.
Mathew, R. J., Georgi, J., Wilson, W. H., & Mathew, V. G. (1996). A retrospective study of the concept of spirituality as understood by recovering individuals. Journal of Substance Abuse Treatment, 13(1), 67–73.
Mauger, P. A., Perry, J. E., Freeman, T., & Grove, D. C. (1992). The measurement of forgiveness: Preliminary research. Journal of Psychology and Christianity, 11, 170–180.
Oakes, K. E. (2008). Purpose in life: A mediating variable between involvement in Alcoholics Anonymous and long-term recovery. Alcoholism Treatment Quarterly, 26(4), 450–463.
Pargament, K. I., Kennell, J., Hathaway, W., Grevengoed, N., Newman, J., & Jones, W. (1988). Religion and the problem-solving process: Three styles of coping. Journal for the Scientific Study of Religion, 27(1), 90–104.
Pargament, K. I., Smith, B. W., Koenig, H. G., & Perez, L. (1998). Patterns of positive and negative religious coping with major life stressors. Journal for the Scientific Study of Religion, 37, 710–724.
Peterson, C., & Seligman, M. E. (2004). Character strengths and virtues: A classification and handbook. Washington, DC: American Psychological Association.
Puchalski, C. M. (2003). The spiritual dimension: The healing force for body and mind. In C. M. Puchalski (Ed.), Caregiving book series (pp. 174–195). Americus, GA: Rosalyn Carter Institute for Human Development, Georgia Southwestern State University.
Puchalski, C., & Ferrell, B. (2010). Making health care whole: Integrating spirituality into patient care. West Conshohocken: Templeton Press.
Reinert, D. F. (1997). The Surrender Scale: Reliability, factor structure, and validity. Alcoholism Treatment Quarterly, 15(3), 15–32.
Robinson, E. A., Cranford, J. A., Webb, J. R., & Brower, K. J. (2007). Six-month changes in spirituality, religiousness, and heavy drinking in a treatment-seeking sample. Journal of Studies on Alcohol and Drugs, 68(2), 282–290.
Salsman, J. M., Brown, T. L., Brechting, E. H., & Carlson, C. R. (2005). The link between religion and spirituality and psychological adjustment: The mediating role of optimism and social support. Personality and Social Psychology Bulletin, 31, 522–535.
Tonigan, J. S. (2003). Changing AA practices and outcomes: Project MATCH three-year follow-up. Alcoholism: Clinical and Experimental Research, 27(3), 526–528.
Tonigan, J. S., Connors, G. J., & Miller, W. R. (1996a). Alcoholics Anonymous involvement (AAI) scale: Reliability and norms. Psychology of Addictive Behaviors, 10(2), 75–80.
Tonigan, J. S., Miller, W. R., & Schermer, C. (2002). Atheists, agnostics and Alcoholics Anonymous. Journal on Studies of Alcohol and Drugs, 63(5), 534–541.
Tonigan, J. S., Rynes, K. N., & McCrady, B. S. (2013). Spirituality as a change mechanism in 12-step programs: A replication, extension, and refinement. Substance Use and Misuse, 48(12), 1161–1173.
Tonigan, J. S., Toscova, R., & Miller, W. R. (1996b). Meta-analysis of the literature on Alcoholics Anonymous: Sample and study characteristics moderate findings. Journal of Studies on Alcohol, 57(1), 65–72.
Underwood, L. G. (1999). Daily spiritual experiences: Multidimensional measurement of religiousness/spirituality for use in health research. A report of the Fetzer Institute/National Institute on Aging Working Group (pp. 11–18). Kalamazoo, MI: Fetzer Institute.
Underwood, L. G., & Teresi, J. A. (2002). The Daily Spirituality Experience Scale: Development, theoretical description, reliability, exploratory factor analysis, and preliminary construct validity using health-related data. Annuals of Behavioral Medicine, 24, 22–33.
Young, L. B. (2013). Characteristics and practices of sponsored members of Alcoholics Anonymous. Journal of Groups in Addiction & Recovery, 8(2), 149–164.
Zemore, S. E. (2007). A role for spiritual change in the benefits of 12-step involvement. Alcoholism: Clinical and Experiential Research, 31(S3), 76S–79S.
Zemore, S. E., & Kaskutas, L. A. (2004). Helping, spirituality and Alcoholics Anonymous in recovery. Journal on Studies of Alcohol and Drugs, 65(3), 383–391.
Acknowledgments
This study was undertaken with support from The John Templeton Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dermatis, H., Galanter, M. The Role of Twelve-Step-Related Spirituality in Addiction Recovery. J Relig Health 55, 510–521 (2016). https://doi.org/10.1007/s10943-015-0019-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10943-015-0019-4