
Abstract
Postoperative cognitive dysfunction (POCD) is diagnosed in up to 30% patients after anaesthesia. The causative role of anaesthetic toxicity remains unclear. Using clinical tests, no clear-cut differences have been observed between anaesthetics so far. The aim of this trial was to compare the incidence of POCD diagnosed by a battery of neuropsychologic tests after propofol and sevoflurane anaesthesia. Secondary goal was to examine possible relationship between POCD positivity and changes in auditory event-related potentials (ERPs). Sixty patients undergoing lumbar discectomy were prospectively randomized to receive depth-controlled sevoflurane (SEVO) or propofol (PROP) based anaesthesia. The neuropsychological examination and auditory event-related potentials (N1, P3a and P3b components) recording was performed preoperatively and on days 1, 6 and 42 after surgery. POCD was defined as a decline of more than one standard deviation in three or more tests. In 43 patients (20 in PROP and 23 in SEVO group) all selected tests were performed and used for the evaluation. POCD was present in 48%/60%, 18%/20% and 17%/11% (SEVO/PROP) of patients on days 1, 6 and 42 after surgery, with no significant intergroup difference. Among neuropsychologic tests, the most significant decline was observed in Semantic Verbal Fluency and Letter-Number Sequencing Test scores, congruently in both groups on days 1 and 6, with full recovery on the last control. Transient deteriorations in other tests were observed as well. No association of POCD positivity and ERPs changes was found, although long-term modifications of P3a and P3b components were observed, mainly in SEVO group. In our study, sevoflurane and propofol anaesthesia was associated with the similar incidence of POCD. Cognitive decline, mainly affecting executive functions, was temporary in most of the patients. Prolonged ERPs alterations after the anaesthesia seem not to have any relationship with the impairment registered by the neuropsychological examination and may represent subclinical changes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Postoperative cognitive dysfunction (POCD) is a mild cognitive decline following anaesthesia, which can be found in about 30% patients 1 week after the operation, particularly affecting attention, executive functions and some subtypes of memory [1]. Despite 20 years of intensive research, most details about POCD remain unclear and we still lack any preventive or therapeutic approach. Large observational studies identified successfully prevalence and risk factors [2, 3] for the development of cognitive decline. According to the current knowledge, anaesthesia type does not play any role in the pathophysiology of POCD [4]—less early cognitive dysfunction had been observed soon after regional anaesthesia [5], but the frequency measured later did not differ. With regards to the particular anaesthetics, results of the studies are conflicting as well—two studies in cardiac surgery [6, 7] found better cognitive outcome after volatile anaesthetics, one large randomized clinical trial [8] stated better short-term outcome after propofol in non-cardiac surgical patients. No influence of anaesthetics´ choice was observed in others [9].
Event-related potentials (ERPs) are one of the available methods to objectively examine specific parts of the cognitive process [10]. In the auditory ERPs, several components can be distinguished, each representing a different stage of information processing. Component N1 is related to initial readout of information from sensory analysers. Another component P3a (earlier part of P3) is connected with attention mechanisms and P3b (late P3) represents working memory and the stimulus evaluation [11]. The specific changes in morphology of long-latency auditory evoked potential—especially P3 component correlates—are associated with many neurological and psychiatric disorders [12, 13]. These components are also used for prognostication of comatose patients, mainly after cardiac arrest, where P3 component presence correlates with a high probability of restoration of consciousness [14]. The influence of general anaesthesia on ERPs parameters is unexplored, especially in the longer period after anaesthesia. Only a few studies have been done [15, 16], finding mainly a decrease of amplitude of P3 component [17]. The possible relationship between POCD and ERPs changes has never been studied.
Therefore, we have conducted this prospective randomised clinical trial to study the magnitude of cognitive decline after sevoflurane and propofol anaesthesia in the adult population in middle-risk neurosurgical procedures and to examine the possibility of a relationship between POCD and ERPs changes after surgery.
2 Methods
This prospective, investigator-initiated, one centre, parallel group randomized clinical trial was performed at the Department of Anaesthesia and Intensive Care Medicine and the Department of Neurosurgery of the University Hospital Plzen, Czech Republic. The study was registered in primary WHO registry (Australian New Zealand Clinical Trials Registry), Reg. No. ACTRN12613000362796, and it was approved by the local ethical committee (Institutional Review Board of the University Hospital in Plzen). All patients undergoing elective single space lumbar disc hernia resection were assessed for eligibility to be included in the study during the years 2012–2015. We excluded all patients who weren’t native Czech speakers in order to avoid bias posed by language barrier during psychological examinations. To exclude age-dependent cognitive decline, we have restricted the age of participants to 18–65 years. In accordance with previous POCD studies [1], we have also excluded patients with any other disease affecting central nervous system, those with previous cognitive impairment, psychoactive medication (incl. hypnotics), psychiatric disease, addiction, obstructive sleep apnoea syndrome and with any sensory impairment limiting examination. Normal results of preoperative neuropsychological and electrophysiological examination and signed informed consent were also prerequisite for inclusion.
Patients were equally randomized (single 1:1 randomization) into two groups—inhalational anaesthesia using sevoflurane (SEVO) and total intravenous anaesthesia with propofol (PROP)—using the sealed opaque envelopes technique by the treating anaesthesiologist. All other research team members (neurophysiologist, psychologist, treating neurosurgeon and the ward staff) were unaware of the patient’s group allocation. All patients were examined with a battery of neuropsychological and electrophysiological tests on the day before surgery, first, 6th and 42nd days after surgery. POCD was defined predicated on the neuropsychological test results according to our protocol. A significant difference in POCD occurrence between SEVO and PROP group was considered as the primary outcome of the study. Correlation of neuropsychological changes with the results of electrophysiological findings was defined as a secondary outcome. Patients were screened for any symptoms of clinically manifest cognitive decline throughout the postoperative course up to discharge.
2.1 Anaesthesia protocol
The patients had been anaesthetized by an only limited group of anaesthesiologists (JK, JP) familiar with bispectral index (BIS) guided approach. BIS Vista™ (Covidien, Boulder, CA) monitor was used in the study. Both groups of patients were premedicated with intramuscular morphine in dose 0.1 mg/kg. The use of benzodiazepines, anticholinergic drugs and antipsychotics was avoided. Anaesthesia for patients allocated to the SEVO group was induced with a single dose of propofol (2 mg/kg) and maintained with sevoflurane in air and oxygen mixture, starting at 1.0 age-corrected minimal alveolar concentration (MAC), adjusted to keep BIS between 45 and 60. In the PROP arm, patients were induced with single-dose of propofol (1 mg/kg), immediately followed by continuous administration according to Roberts’ infusion scheme ([18], the “10-8-6” method). After saturation of compartments, the dose was adjusted to reach the same BIS target. Analgesics (sufentanil, ketoprofen, paracetamol), muscle relaxants (atracurium or rocuronium) and antiemetic (ondansetron) were used in both groups as needed without limitations. The patients were protectively ventilated (tidal volume 6–8 ml/kg of predicted body weight, with positive end-expiratory pressure 5–10 cm H2O) to maintain normocapnia. All other physiological variables were maintained in patient’s normal values through anaesthesia. Patients were awakened from anaesthesia in the operation room immediately after the end of the surgery. The postoperative care, including analgesia, was managed by the treating neurosurgeon.
2.2 Neuropsychological testing
Because of the lack of standardised neuropsychological test battery, which can be used for POCD diagnostics, we have selected a set of tests based on previous publications [1] and the decision of psychologist specialised in cognitive function assessment (PB). Important for the choice of the test was also focus on attention and working memory, which can be linked to specific ERPs components. Tests are listed in Table 1. Neuropsychological tests were administered by professional psychologists in selected time points (preoperatively, on day 1, 6 and 42 after surgery) with exclusion of the Digit Span Backward, Trail Making Test, and Word and Colour variant of Stroop Test, which were omitted on the first postoperative day due to the extensive length of examination or movement limitations. Different test versions were used at each time point to reduce the practice effect. POCD positivity was defined as a decline of more than one standard deviation (SD) in more than three tests in certain time point—except first-day post operation, where one SD decline in two tests was accepted for diagnosis due to the reduced number of tests. For further statistical analysis, we also defined “overall POCD positivity”, indicating that the patient was POCD positive in at least one-time point.
2.3 Event-related potentials
ERPs were recorded at the same time points as neuropsychological tests. The examination took place in conditions of the electrophysiologic laboratory. The standard auditory active oddball protocol was used; patients were exposed to two types of auditory stimuli in randomized order, which were delivered binaurally via earphones. Patients were instructed to count deviant stimuli. Three series of stimuli were applied, each containing 400 ones. The frequency of stimulation was 1.1 Hz, 80% of stimuli were standard (750 Hz tone burst), 20% deviant (2000 Hz). EEG was registered using a low-density EEG montage, composed of midline scalp electrodes (Fz, Cz, Pz according to the international 10–20 system). Localization of electrodes for each measurement was chosen based on the local maxima—recording of N1 component from Fz or Cz, P3 component from Fz, Cz or Pz, like in other similar studies [19, 20]. The reference electrode was placed on the forehead, grounding one on the shoulder. The signal was amplified, digitized (560 Hz sampling), recorded and averaged online using Nicolet EEG System (Natus Medical Inc., Pleasanton, USA). For further offline EEG analysis, the epochs containing artefacts > 100 µV were excluded. For each patient, the EEG epoch lasting from 50 to 800 ms was averaged automatically. Then, ERPs peaks were then analysed offline by two independent electrophysiologists. Latencies and amplitudes of N1, P3a and P3b components were recorded for statistical analysis (Fig. 1).

ERPs traces for standard and deviant stimuli obtained from one of the patients
2.4 Statistical analysis
Software SAS 9.4 (Cary, NC, USA) and STATISTICA (StatSoft, Inc., Tulsa, OK, USA) were used for data analysis, which was performed by an independent statistician (see acknowledgements). The means, medians, standard deviations and confidence intervals were calculated where appropriate. The Shapiro–Wilk Test was used for normality assessment. The Wilcoxon Two-Sample Test or the Two-Sample Median Test was used for comparison of distributions of particular parameters within groups and subgroups. The factor influence was tested with Chi-squared test or Fisher Exact Test in case of low frequencies. Changes in measured parameters in time were analysed with repeated measures ANOVA or Friedman test, depending on distributions. The significance level was set at 0.05.
3 Results
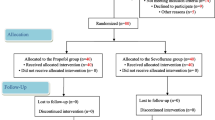
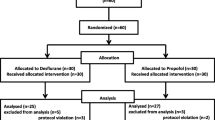
During the study period, 63 patients were found eligible for inclusion. After the refusal of three patients, 60 patients were included and randomized into this trial. All included patients signed the informed consent. From these, 43 patients (23 in SEVO and 20 in PROP group) were included in the final analysis. Drop-outs were caused mainly by lost to follow up in the neuropsychologic (n = 8) and electrophysiological testing (n = 4). Other reasons included the use of drugs restricted by protocol (n = 2), anaesthesia during follow-up (n = 1), patient refusal to continue (n = 1) and cancellation of surgery after randomization by a neurosurgeon (n = 1). Details of the participants flow through the trial are displayed in Fig. 2. There were no significant intergroup differences in the baseline characteristics (Table 2).

CONSORT flow diagram
Using the methods described above, POCD was diagnosed in 48% patients in SEVO and 60% in PROP group on the day 1 (difference between groups p = 0.42), 18% versus 20% on day 6 (p = 0.86) and 17% versus 11% on day 42 (p = 0.63). The overall POCD positivity of 48% in SEVO and 60% in PROP did not differ (p = 0.88). No clinically apparent cognitive decline was observed or self-reported by any of those subjects. Overall POCD positives and negatives did not differ in any of suggested risk factors such as age, gender, duration of anaesthesia nor analgesia management—details are given in Table 3.
3.1 Changes in neuropsychological tests
Significant changes in test scores were observed in both anaesthesia groups. The main finding, which was uniform in both arms, was an early transient drop of the score in Semantic Verbal Fluency Test (on day 1, 6 and 42 after the operation: 20.5 (18.2–22.7)—15.0 (13.1–17.0)—15.8 (14.0–17.7)—21.9 (19.3–24.4) in SEVO and 22.0 (20.4–23.6)—16.8 (14.8–18.7)—18.1 (15.6–20.5)—22.7 (20.7–24.6) in PROP arm; mean score preoperatively, 95% CI). In Letter-Number Sequencing Test was found nearly the same process (9.1 (8.4–9.8)—8.0 (7.2–8.7)—8.8 (7.4–10.2)—8.4 (7.7–9.2) for SEVO and 10.1 (9.1–11.0)—8.2 (7.4-9.0)—10.1 (9.2–10.9)—10.2 (9.2–11.2) for PROP group; mean score in corresponding time points, 95% CI). Scores for these two tests are visualised on Figs. 3 and 4. In the PROP group, an isolated drop of Backward Digit Span was observed on the day 6 following surgery. Lastly, it is possible to observe improvement of scores of Stroop Colour, Stroop Word-Colour and TMT B. The detailed view of all tests development is provided in Table 5 in Appendix.

Development of scores of Semantic Verbal Fluency and Letter-Number Sequencing Test in particular groups
3.2 Association of POCD with changes in ERPs
The possible relationship between the POCD positivity and changes of amplitudes and latencies of N1, P3a and P3b components was analysed with ANOVA, repeated measures design. There was no significant result indicating any POCD–ERPs change interaction (Table 4). However, we found highly significant changes in P3a and P3b amplitude and latency, which were long lasting and were more profound after sevoflurane anaesthesia compared to propofol (Figs. 5, 6; Table 6 in Appendix).
4 Discussion
In our study, the POCD incidence, as measured by our chosen clinical tests, was similar after intravenous propofol and sevoflurane anaesthesia in adult patients undergoing lumbar disc hernia resection. The positivity of POCD in both PROP and SEVO arms on 6th day post operation was about 20%, which is congruent with other large studies [1, 2]. Limited data for incidence on the 42nd day are available, but our results (17% in SEVO resp. 11% in PROP group) are slightly above incidence usually reported after 3 months. Overall POCD occurrence was similar in both groups. Except one case, all patients with POCD were positive on the first day post-operation, with subsequent normalisation. Only one subject had a late onset in the last time point—this could be either caused by other external factors influencing patient before the last control or this can be due to imperfect sensitivity of our POCD criteria since we are not currently aware of a report of late-onset POCD.
During neuropsychological testing, significant drops in tests examining executive functions and visual–spatial working memory were found in the first days, with full normalization on the last control. Like in other studies, there was an improvement in some tests (TMT-B, Stroop Test subtests) focused on visual attention and task-switching. Both tests have very well described practice effect [21], which is nearly impossible to eliminate, despite the use of different versions—the task pattern is still the same. The most affected, symmetrically in both groups, was Verbal Fluency (only Semantic variant) which examines executive functions, the ability of recall from semantic memory. Nowadays, this test is considered to be very sensitive to even small cognitive impairment and it is a stable item in test batteries for diagnostics of cognitive impairment. Second affected was Letter-Number Sequencing Test, which provides a measure of processing speed and visual-spatial working memory. Test scores were significantly worsened, without full normalization on day 6. This allows us to state, that in the first days after surgery, there is a relevant decrease in executive functions and memory processing. This fact is well known, although routinely neglected—discussion about the ability to drive in the first days after anaesthesia is led currently [22].
In the results of ERPs testing, a significant decrease of P3a and P3b amplitude occurred after anaesthesia, but this was not associated with POCD positivity or clinically apparent cognitive decline. No link between changes in ERPs parameters and diagnosed POCD was found. ERPs were also decreased with both anaesthesia types, without a full return to preoperative values in some parameters. The drop in the amplitude and prolongation of the latency was non-significantly more common after sevoflurane. These changes were described earlier [17, 23], but there is no study with follow up lasting 6 weeks or longer, so the time to normalisation is unfortunately unknown. The reason of slow dynamics of ERPs changes, which do not copy results of the neuropsychological tests, as well as its pathophysiology, remains unclear. Although without clinical correlate, this phenomenon will need a further research and may represent a long-term subtle decrease of attention and affection of the working memory. Our explanation is, that the sensitivity of ERPs is much higher than neuropsychological tests. More profound statistical analysis of ERPs changes is limited because of lack of well-defined and accepted normal age-adjusted values. We conclude, therefore, that ERPs in current setting cannot be used for POCD assessment.
The cognitive decline was not associated with any of presumed risk factors, including the length of anaesthesia, pain scores or opioid consumption. This finding corresponds with other studies mentioned above. Age of patient, which is widely recognized as a risk factor for POCD, was non-significantly higher in the POCD positive group.
4.1 Limitations
A major limitation of our study, but commonly shared among most of POCD studies published so far, is the sample size calculation. No study except [8] showed differences in the POCD incidence after different anaesthetics in non-cardiac surgery, so empiric calculation is impossible. We decided to include 60 patients, randomized 1:1 into two groups. Other trials used this or even smaller sample size [24, 25]. Only 43 patients completed follow-up, thus drop-off rate was about 28%, which is slightly above other studies. This was caused by rather ambitious design of syncing the ambulatory controls in electrophysiology lab and psychologist, mainly at the last time point. The small sample size was also a cause of impossibility to perform logistic regression. Limited funding and human resources for testing were also a minor factor. The design of testing can also be a source of limitations. Although, the wide acceptance of the use of composite scores of test batteries, related to the control group for diagnostics of POCD, we decided to omit the control group for the calculation and use criterion “one SD in three tests” instead. This method is the strictest one according to a published review of diagnostic approaches [21], allowing some simplification of the study protocol.
5 Conclusion
To summarize, in our study incidence of POCD was similar after propofol and sevoflurane general anaesthesia. Patients had measurable slowing of executive functions and memory processing in the first days after anaesthesia. Significant, long-lasting ERPs changes were observed, but without any relationship with POCD and without any clinically apparent correlate.
Preliminary analysis of this study was presented at EuroNeuro 2016 congress. Patients included in this study were part of a larger cohort, in which electrophysiological study in perioperative setting was done. Results, focused only on the in-depth analysis of ERPs, were already published in [26].
References
Moller J, Cluitmans P, Rasmussen L, Houx P, Rasmussen H, Canet J, et al. Long-term postoperative cognitive dysfunction in the elderly: ISPOCD1 study. Lancet 1998;351(9106):857–61.
Monk T, Weldon B, Garvan C, Dede D. Predictors of cognitive dysfunction after major noncardiac surgery. Anesthesiology 2008;108(1):18–30.
Funder KS, Steinmetz J. Post-operative cognitive dysfunction—lessons from the ISPOCD studies. Trends Anaesth Crit Care. 2012;2(3):94–7.
Evered L, Scott DA, Silbert B, Maruff P. Postoperative cognitive dysfunction is independent of type of surgery and anesthetic. Anesth Analg. 2011;112(5):1179–85.
Rasmussen LS, Johnson T, Kuipers HM, Kristensen D, Siersma VD, Vila P, et al. Does anaesthesia cause postoperative cognitive dysfunction? A randomised study of regional versus general anaesthesia in 438 elderly patients. Acta Anaesthesiol Scand. 2003;47(3):260–6.
Royse CF, Andrews DT, Newman SN, Stygall J, Williams Z, Pang J, et al. The influence of propofol or desflurane on postoperative cognitive dysfunction in patients undergoing coronary artery bypass surgery. Anaesthesia 2011;66(6):455–64.
Schoen J, Husemann L, Tiemeyer C, Lueloh A, Sedemund-Adib B, Berger K-U, et al. Cognitive function after sevoflurane- vs propofol-based anaesthesia for on-pump cardiac surgery: a randomized controlled trial. Br J Anaesth. 2011;106(6):840–50.
Cai Y, Hu H, Liu P, Feng G, Dong W, Yu B. Association between the apolipoprotein E4 and postoperative cognitive dysfunction in elderly patients undergoing intravenous anesthesia and inhalation anesthesia. Anesthesiology 2012;116(1):84–93.
Rohan D, Buggy DJ, Crowley S, Ling FKH, Gallagher H, Regan C, et al. Increased incidence of postoperative cognitive dysfunction 24 hr after minor surgery in the elderly. Can J Anesth. 2005;52(2):137–42.
Woodman GF. A brief introduction to the use of event-related potentials (ERPs) in studies of perception and attention. Atten Percept Psychophysiol. 2010;72(8):1–29.
Remijn GB, Hasuo E, Fujihira H, Morimoto S. An introduction to the measurement of auditory event-related potentials (ERPs). Acoust Sci Technol. 2014;35(5):229–42.
Pulvermüller F, Lutzenberger W, Müller V, Mohr B, Dichgans J, Birbaumer N. P3 and contingent negative variation in Parkinson’s disease. Electroencephalogr Clin Neurophysiol. 1996;98(6):456–67.
Bonanni L, Franciotti R, Onofrj V, Anzellotti F, Mancino E, Monaco D, et al. Revisiting P300 cognitive studies for dementia diagnosis: early dementia with Lewy bodies (DLB) and Alzheimer disease (AD). Neurophysiol Clin. 2010;40(5–6):255–65.
De Giorgio CM, Rabinowicz AL, Gott PS. Predictive value of P300 event-related potentials compared with EEG and somatosensory evoked potentials in non-traumatic coma. Acta Neurol Scand. 1993;87(5):423–7.
van Hooff JC, de Beer N, Brunia CH, Cluitmans PJ, Korsten HH. Event-related potential measures of information processing during general anesthesia. Electroencephalogr Clin Neurophysiol. 1997;103(2):268–81.
Heinke W, Kenntner R, Gunter TC, Sammler D, Olthoff D, Koelsch S. Sequential effects of increasing propofol sedation on frontal and temporal cortices as indexed by auditory event-related potentials. Anesthesiology 2004;100(3):617–25.
Reinsel R, Veselis R, Wronski M, Marino P. The P300 event-related potential during propofol sedation: a possible marker for amnesia? Br J Anaesth. 1995;74(6):674–80.
Roberts FL, Dixon J, Lewis GTR, Tackley RM, Prys-Roberts C. Induction and maintenance of propofol anaesthesia. Anaesthesia 1988;43(s1):14–7.
Mueller SC, Swainson R, Jackson GM. ERP indices of persisting and current inhibitory control: a study of saccadic task switching. Neuroimage 2009;45(1):191–7.
Tomé D, Barbosa F, Nowak K, Marques-Teixeira J. The development of the N1 and N2 components in auditory oddball paradigms: a systematic review with narrative analysis and suggested normative values. J Neural Transm. 2015;122(3):375–91.
Rasmussen LS, Larsen K, Houx P, Skovgaard LT, Hanning CD, Moller JT. The assessment of postoperative cognitive function. Acta Anaesthesiol Scand. 2001;45(3):275–89.
Powell LM, Molyneux M. Should patients be advised not to drive for 4 days after isoflurane anaesthesia? Anaesthesia 2017;72(6):682–5.
Mracek J, Holeckova I, Chytra I, Mork J, Stepanek D, Vesela P. The impact of general versus local anesthesia on early subclinical cognitive function following carotid endarterectomy evaluated using P3 event-related potentials. Acta Neurochir (Wien). 2012;154(3):433–8.
Papaioannou A, Fraidakis O, Michaloudis D, Balalis C, Askitopoulou H. The impact of the type of anaesthesia on cognitive status and delirium during the first postoperative days in elderly patients. Eur J Anaesthesiol. 2005;22(7):492–9.
Nemeth E, Vig K, Racz K, Koritsanszky KB, Ronkay KI, Hamvas FP, et al. Influence of the postoperative inflammatory response on cognitive decline in elderly patients undergoing on-pump cardiac surgery: a controlled, prospective observational study. BMC Anesthesiol. 2017;17(1):113.
Holečková I, Kletečka J, Štěpánek D, Žídek S, Bludovský D, Pouska J, et al. Cognitive impairment measured by event-related potentials during early and late postoperative period following intravenous or inhalation anaesthesia. Clin Neurophysiol. 2018;129(1):246–53.
Acknowledgements
The authors would like to acknowledge the work performed by independent statistician ing. Kormunda and all staff involved in this study.
Funding
The study was funded by the Charles University research funds PRVOUK P36 and PROGRES Q39.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.

Rights and permissions
About this article

Cite this article
Kletecka, J., Holeckova, I., Brenkus, P. et al. Propofol versus sevoflurane anaesthesia: effect on cognitive decline and event-related potentials. J Clin Monit Comput 33, 665–673 (2019). https://doi.org/10.1007/s10877-018-0213-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10877-018-0213-5