
Abstract
Peer victimization experiences is suggested to play a mediating role in the transmission of depression symptoms between mothers and children. Childcare attendance has been found to reduce the association between mother and child depressive symptoms. However, it is not clear whether this protective effect unfolds via a reduction of peer victimization experiences in middle childhood. The aims of this study were to test (1) whether peer victimization in middle childhood mediated the association between exposure to maternal depressive symptomatology in early childhood and child depressive symptoms in late childhood, (2) whether childcare attendance moderate the direct associations between maternal depressive symptoms and children’s peer victimization experiences in middle childhood as well as depressive symptoms in late childhood and (3) whether childcare attendance moderates this mediated association. Data come from the Avon Longitudinal Study of Children and Parents (N = 5526) where exposure to maternal depressive symptoms and intensity of childcare attendance were assessed repeatedly during early childhood. Children’s peer victimization and depressive symptoms were self-reported at eight and 10 years of age, respectively. We used weighted structural equation modeling and found that the association between mothers and children’s depression was partially mediated by peer victimization. Childcare attendance did not moderate the indirect effect of maternal depression on child depressive symptoms via peer victimization. However, we found that for children who attended childcare, maternal depression was no longer associated child depressive symptoms in late childhood. In conclusion, peer victimization experiences partly explain the intergenerational transmission of depressive symptoms, but this mechanism is not altered by children’s childcare attendance. Future research should examine potential socio-emotional and school readiness mechanisms that may break the cycle of depressive symptomatology from mothers to children.
Highlights
-
Children’s peer victimization experiences partially explained the association mothers’ and children’s depressive symptoms.
-
Part-time childcare attendance decreased the association between mothers’ and children’s depressive symptoms.
-
We did not find that childcare attendance moderated the association between mother’s depressive symptoms and children’s peer victimization experiences.
-
The protective role of childcare attendance did not unfold via a reduction of peer victimization experiences, other intermediary psychosocial factors need to be explored.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Family experiences shape children’s capacity to adapt and cope with stress and challenges arising at school and are expected to impact children’s relationships with peers in many ways. Exposure to maternal depressive symptoms during early childhood has been associated cross-sectionally and longitudinally with children’s higher levels of peer difficulties and internalized symptoms (Goodman et al., 2011). This association between maternal depressive symptoms and her offspring’s social adjustment seems to withstand until late adolescence (Jaffee et al., 2021; Pearson et al., 2013). Several mechanisms have been suggested to explain the intergenerational transmission of depression from mothers to children (Goodman, 2007). Yet only few studies have investigated how this association emerges during childhood and what could be the intermediary experiences that underlie this intergenerational transmission of depressive symptoms from mothers to children. According to the Integrative Model for the Transmission of Risk (Goodman & Gotlib, 1999), children who have been exposed to maternal depression are at higher risk of social, cognitive or behavioral skills deficits which may put them at higher risk of developing depression later on. These deficits may be linked to mothers engaging in parenting practices of lower quality due to their depressive symptomatology (Goodman, 2007). In that sense, mothers with high depressive symptomatology may be unable to fulfill their children’s needs for social and emotional support (Cicchetti & Toth, 1998), which in turn, might negatively affect the child’s social and cognitive skills. Over time, these children may struggle to interact with peers, because of their lower levels of verbal, cognitive and socio-emotional skills, and become at higher risk of being peer victimized (Oncioiu et al., 2020; Perren et al., 2009).
Côté et al. (2018) reported that experiences of peer victimization play a complete mediating role in the association between mothers’ and adolescents’ depressive symptoms. Peer victimization can be defined as being the recipient of repeated and intentional aggression by (a) more powerful peer(s) (Olweus, 1993). Children exposed to maternal depression exhibit higher levels of emotional regulation problems and peer victimization (Apter-Levi et al., 2016; Azeredo et al., 2017), which in turn, put children at higher risk of experiencing mental health problems (Côté et al., 2018; Tsypes & Gibb, 2015). Using the Avon Longitudinal Study of Parents and Children (ALSPAC), the same dataset used in the present study, Zwierzynska et al. (2013) found that peer victimization in late childhood was associated with internalized problems in early adolescence. However, this study did not explore whether peer victimization explained, partially or entirely, the extent to which maternal depression predicted later internalized problems. Of note, the few studies that investigated the mediation hypothesis have targeted internalized problems in early or late adolescence (Côté et al., 2018; Tsypes & Gibb, 2015; Zwierzynska et al., 2013). In the present study, we investigated whether peer victimization mediated the intergenerational transmission of depressive symptoms between mothers and children as early as in late childhood. Intervening early on children who are living with depressive mothers and/or are peer victimized, before they enter the teenage years, would be a promising way to prevent internalized symptoms and its downward effects on adolescents’ academic and social functioning (Verboom et al., 2014).
Childcare Attendance as a Protective Factor
Some studies have reported that attending formal childcare before five years of age may be associated with reduced internalizing difficulties for children exposed to high levels of maternal depressive symptomatology (Giles et al., 2011; Goelman et al., 2014; Herba et al., 2013; Lee et al., 2006; Paquin et al., 2020). To date, studies that investigated this potential protective role have mainly focused on short-term associations (i.e., from early to middle childhood) and on internalized and externalized problems (Charrois et al., 2020; Giles et al., 2011; Goelman et al., 2014; Herba et al., 2013; Paquin et al., 2020). However, the mechanisms through which this potential protective effect unfolds as well as the specific protective effect of childcare attendance on the association between exposure to maternal depression and peer-related problems, like peer victimization, have not been examined. Several reasons might explain why childcare attendance buffers the effect of maternal depressive symptomatology on children’s psychosocial adjustment and mental health. For the mother, the perception of having good childcare choices where she lives has been associated with a reduced likelihood of clinical depressive symptoms (Johnson & Padilla, 2019). Also, childcare attendance for high-risk families had been associated with improvements in the home environment, such as a reduction in negative parenting practices and warmer mother-child interactions (McCartney et al., 2007). For the child, attending childcare might provide opportunities to interact and learn with peers and other adults, such as their educators, which may help to promote resilient mechanisms pertaining to mental health, such as social and emotion regulation (Schindler et al., 1987). Childcare attendance may thus offer daily social skills training through experiences, reinforcement, and exposure to prosocial models, which may in turn have lasting impact on children’s ability to interact socially with others (Berry et al., 2016) and maintain mental health (Larose et al., 2021; Orri et al., 2019; Zachrisson & Dearing, 2015). As shown by Charrois et al. (2017, 2020), high childcare quality mitigated the association between maternal depression and children’s externalizing symptoms (in early and middle childhood (Charrois et al., 2017, 2020) as well as with internalizing symptoms in middle childhood (Charrois et al., 2020). Both studies by Charrois et al. (2017, 2020) adjusted their regression models for child’s sex, maternal education, family income, single child, single parent, perceived social support, coercive parenting practices and the average number of hours per week spent in childcare.
Only two previous studies have investigated which childcare intensity (i.e., number of weekly hours) is required to alleviate the association between maternal depressive symptoms and later internalized and externalized problems. Giles et al. (2011) found that as little as four hours per week were beneficial for child development, whereas Lee et al. (2006) suggested that part-time attendance (i.e., approximately 15 h a week) reduced the risk of child internalized problems following exposure to maternal depressive symptoms. In contrast, full-time childcare attendance was reported to be required to cancel the association between mothers’ depressive symptoms and children’s internalized problems (Lee et al., 2006). More research is needed to determine the intensity of the childcare attendance required to prevent children’s depressive symptoms in late childhood following exposure to maternal depressive symptoms in early childhood. Of note, we decided to focus on maternal depression rather than paternal or parental depression, given the United Kingdom’s socio-political context in the early 1990s where mothers were more likely to be the primary caregiver during the day if their children did not attend childcare.
Objectives
Using data from the large-scale prospective British population-based cohort study Avon Longitudinal Study of Parents and Children (ALSPAC), we aimed to investigate (1) whether peer victimization in middle childhood mediates the association between exposure to maternal depressive symptomatology in early childhood and child depressive symptoms in late childhood, (2) whether childcare attendance moderates the direct associations between maternal depressive symptoms and children’s peer victimization experiences in middle childhood as well as depressive symptoms in late childhood and (3) whether childcare attendance moderates this mediated association. We expect that peer victimization experiences will partly explain the association between mothers’ and children’s depressive symptoms, that childcare attendance will moderate the associations between maternal depressive symptoms and children’s peer victimization as well as depressive symptomatology in late childhood, and that children who attended part-time or full-time childcare during early childhood would be prevented from this developmental cascade (i.e., moderated mediation).
Methods
Participants
ALSPAC is an ongoing epidemiological study of children born from 14,541 pregnancies to women residing in Avon, United Kingdom, with an expected delivery date between April 1991 and December 1992 (Boyd et al., 2013; Fraser et al., 2013). Informed consent to use the data collected via questionnaires and clinics was obtained from participants following the recommendations of the ALSPAC Ethics and Law Committee at the time. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Ethical approval for the study was obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees. Note that the study website contains details of all the data that are available through a fully searchable data dictionary: https://www.bristol.ac.uk/alspac/researchers/our-data/.
For this study, analyses were conducted on a subsample of 5526 children for whom data on maternal depression and childcare attendance in early childhood, peer victimization experiences in middle childhood and child-reported depressive symptoms in late childhood were available. As our sample is reduced from the original ALSPAC sample, because many children did not participate in the research clinics (i.e., on site instead of remote assessments) when peer victimization was assessed, we computed a population representativeness weight based on the socio-demographic characteristics associated with the likelihood of being included (or not) in the final analytical sample. More specifically, children from families whose parents had lower levels of parental education and occupation, and whose mothers were younger, were less likely to be included in the final analytical sample (see Table S1 in Supplementary Material for more details). This weight was then applied to the estimation of the mediation and moderation models. Also, considering that childcare attendance is subject to social selection, we controlled for the propensity of attending childcare by using propensity scores based on the socio-demographic characteristics (e.g., maternal age, second pregnancy, family social class) associated with the intensity of childcare attendance. Both population representativeness and propensity score weights for social selection into childcare were applied in our moderation and moderated mediation model.
Measures
Maternal depressive symptoms during early childhood
Maternal depressive symptoms were assessed using the Edinburgh Postnatal Depression Scale (EPDS) at two, eight, 21 and 33 months postpartum (Cox et al., 1987). The EPDS is a well-established and widely used assessment of depressive symptomatology in the postnatal period and captures the intensity of depressive symptoms over the preceding seven days. The EPDS has 10 items (e.g., “I have blamed myself unnecessarily when things went wrong”, “I have felt sad or miserable”) answered with various response options, varying from 0 to 3. At each assessment time, items were summed up yielding a minimum score of 0 and a maximum of 30 (αs = 0.82–83). We created a latent score of maternal depression during early childhood drawing on the scores obtained at the four time points using a confirmatory factor analysis where a higher score indicates greater severity of depression (RMSEA = 0.08, CFI = 0.99, SRMR = 0.015).
Childcare attendance
When the child was eight, 15, 24 and 38 months, mothers reported on childcare use and the weekly number of hours their child spent in childcare. Childcare was defined as a group-based care context where children are cared for by someone other than their parents or relatives outside of their home by someone who is paid for the care provided—which includes the following types of care: creche, day nursery and childminders. Our childcare variable is thus similar to the one presented by Gregg et al. (2005), with the exception that childminders were also considered as a group-based care. To ascertain the moderating impact of stable patterns of childcare attendance during early childhood, we estimated trajectories of childcare attendance using latent class growth analysis (Jung & Wickrama, 2008). To be included in the analysis, parents ought to report on at least on one occasion their use of childcare services. A three-group childcare attendance trajectory model was selected based on of model fit (i.e., Bayesian Information Criteria or BIC) and better group classification (entropy = 0.99) (see Table S3 in Supplementary Material for greater details about model selection). The BIC is a commonly used fit index in which lower values indicate a more parsimonious model. Entropy is a measure of classification accuracy with values closer to 1 indexing greater precision (range = 0–1) (McLachlan & Peel, 2004). Based on the mean number of hours children spent in childcare services, children were either exposed to full-time childcare (3.7%), part-time childcare (5.9%) or had low attendance of childcare (90.4%) (see Fig.1). Considering the high entropy, we used hard classification in childcare trajectories. The percentage of children in each trajectory is similar to the proportion reported in a British national report summarizing group-based childcare attendance at that time period (West & Noden, 2016). In the early 90’s, childcare attendance in the United Kingdom was highly fragmented due to the high costs of childcare services and limited governmental subsidies (i.e., market-based economy), therefore many children were under the care of grandparents, babysitters and other relatives (Gray, 2005).

Trajectories of childcare attendance from age 8 months to 3 years
Peer victimization experiences
Children were interviewed with the Bullying and Friendship Interview Schedule (Wolke et al., 2001) when they were on average eight years of age as part of a face-to-face interview. Trained psychology graduates asked the children nine questions concerning overt and relational bullying by peers that might have occurred over the previous six months and the frequency of its occurrence. Five items referred to overt victimization: 1) personal belongings taken; 2) threatened or blackmailed; 3) hit or beaten up; 4) tricked in nasty way; 5) called bad/nasty names, and four items referred to relational victimization: 1) exclusion; 2) coercive pressure to do things s/he didn’t want to do; 3) lies or nasty things said about him/her; 4) spoilt activities for him/her on purpose to make him/her upset. Children reported whether they had experienced peer victimization, responding ‘not at all’ = 0 to ‘very frequently’ = 3. Using a confirmatory factor analysis, we created a latent score of victimization experiences from the nine victimization items. This score had good fit indices (RMSEA = 0.051, CFI = 0.931, SRMR = 0.032) and the alpha and omega indices were acceptable (0.73 and 0.70, respectively). Of note, we also performed our analysis while creating two latent factors based on the type of peer victimization experienced (i.e., overt and relational), and found no meaningful differences in the results. Therefore, we report the results according to an overall latent score of peer victimization experiences
Child depressive symptoms in late childhood
The Short Moods and Feelings Questionnaire (SMFQ) (Angold et al., 1995) was administered to children when they were 10 years of age. The SMFQ is a 13-item questionnaire including questions relating to the occurrence of depressive symptoms over the past two weeks. For each question, the child answers on a 3-point scale where 0 refers to ‘not true’, 1 ‘sometimes true’, and 2 ‘true’. The scale included items such as: ‘I felt miserable or unhappy,” ‘I felt lonely’, and ‘I cried a lot.’ A cumulative score was created with higher scores indicating higher depressive symptoms levels (Cronbach’s alpha = 0.85).
Covariates for the main analysis
We included the following set of covariates in our main analyses: child sex, family adversity, paternal depressive symptoms during early childhood, children’s behavioral dysregulation problems in early childhood, and their cognitive abilities as well as bullying perpetration behaviors in middle childhood. Family adversity was assessed by mothers on three occasions (i.e., during the second trimester of mother’s pregnancy, between child birth and the children’s second anniversary and between children second and fourth year) using the Family Adversity Index questionnaire (Bowen et al., 2005). This scale assesses 18 contextual risks (e.g., early parenthood, housing adequacy, low parental education, financial difficulties, partnering status and relationship quality, parental substance abuse, involvement with crime and lack of social support) that the mother or child were exposed to (1) or not (0) in the last year. A total score varying from 0 to 18 was calculated at each collection time, and a mean score was derived across the three time points. Paternal depressive symptoms were assessed at 2-,8- and 21-months after the childbirth using the Edinburgh Postnatal Depression Scale (EPDS). We created a latent score of paternal depressive symptoms over early childhood using a confirmatory factor analysis (RMSEA = 0.01, CFI = 1.00, SRMR = 0.015). Child behavioral dysregulation problems were assessed by parents when the child was four years old (before the mediator) with the four subscales of the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 1997) (i.e., emotional symptoms, conduct problems, hyperactivity/inattention, relationship problems) which were later combined into a mean score. Child cognitive abilities were assessed during a half-day clinic when the child was eight years old using the Wechsler Intelligence Scale for Children (Wechsler et al., 1992). A short form of the measure was employed to reduce the likelihood that the children would become fatigued. The WISC-III UK comprises five verbal subtests and five performance subtests. Scores were age-normed in accordance with standard procedures. A child general cognitive abilities score was created by Barker and colleagues (2018) by extracting the common variance from the verbal and performance tests in a latent factor (Barker et al. 2018). Finally, children’s own bullying behaviors (overt and relational) were assessed using the Bullying and Friendship Interview Schedule (Wolke et al., 2001), where children answered the frequency in which they engage in nine bullying perpetration behaviors. Table 1 presents the socio-demographic characteristics of the study sample and by childcare trajectories.
Socio-demographic characteristics included in the population representativeness and social selection into childcare propensity scores
Children’s characteristics included child birth order and child sex. Parent’s characteristics included mother age, if the mother had a subsequent pregnancy in the 4-year post-delivery of the targeted study child, presence or absence of the father in the household at child 8 months of age, maternal mental health history (lifetime presence or absence of a clinical diagnostic of externalized or internalized mental health issues), maternal depressive symptoms and maternal employment status at child 8-month of age for which mothers answered either “no (n = 6165)” or “yes, inside the home (n = 479); outside the home (N = 4330); outside and inside the home (n = 114)”. The score obtained at Family Adversity Index (Bowen et al., 2005) was also included in the population representativeness and social selection propensity scores.
Maternal and paternal education were divided into two categories (i.e., obtained a high school diploma or less—O-Levels in the UK—and attended subsequent professional or academic training). Mothers and fathers also reported their social class using the Standard Occupational Classification (Register General’s Classification, 1990). This scale goes from 1 (director position) to 5 (manual occupation), but we regrouped levels 3 to 5 into one (i.e., technical, manual and non-manual occupation) to avoid low frequency cells. Finally, mothers’ neighborhood quality was assessed during her pregnancy using the Neighborhood Quality Index (12 items); a cumulative index where a higher score indicates a higher quality neighborhood (Taylor et al., 2013).
Statistical Analyses
Accounting for population representativeness and social selection into childcare
First, because our sample was considerably reduced compared to the original ALSPAC sample, we computed population representativeness weight using inverse probability weighting (Austin & Stuart, 2015). We identified, using bivariate analyses (i.e., χ2 testing, and 1-way analysis of variance using 2-tailed tests with a p value < 0.10; see Table S2 in Supplementary Material), the sociodemographic characteristics that were associated with being included or not in our analytical sample, as based on the availability of the main study variables (i.e., maternal depression, childcare attendance, victimization experiences and child depressive scores). Then, we performed a binomial logistic regression where the set of socio-demographic characteristics previously identified predicted being included or not in our analytical sample. Missing data on variables were managed using multiple imputations by chained equations using the Amelia package in R (Honaker et al., 2011). Covariance balance between children included and excluded from our analytical sample was assessed using standardized mean differences, before and after propensity score weighting (PSW). The population representativeness weight was applied in the mediational model (i.e., objective 1).
Then, to further investigate the potential moderating role of childcare attendance on child development, we computed a second weight to account for social selection bias in childcare attendance. Indeed, the parental decision to enroll a child in childcare services is not random as socio-demographic and family characteristics are associated with this decision and with the intensity of weekly childcare attendance (Dearing & Zachrisson, 2017). We identified these characteristics with bivariate analyses (p value < 0.10) among all children in the ALSPAC study, with data collected at least once between birth and age three years for more robustness of the pattern of findings. Using a multinomial regression, we computed a second inverse probability weight with the socio-demographic characteristics previously identified. Covariance balance between trajectories was assessed using standardized mean differences before and after PSW (Austin & Stuart, 2015). Finally, to simultaneously control for population representativeness and social selection bias in childcare attendance in our moderated mediated model, we multiplied the two weights previously calculated and applied their product for maximum robustness (Ridgeway et al., 2015). The population representativeness weight and the weight for social selection into childcare were calculated on the fully imputed sample to avoid case deletion due to missing data on identified variables to predict population representativeness. All subsequent analyses were performed on our final analytical sample with complete data on the main study variables (n = 5526). All analyses were performed with R version 3.6.1 (R Core Team, 2020).
Does peer victimization mediate the association between mothers’ and children’s depressive symptoms?
Using the lavaan package in R (Rosseel, 2012), we estimated mediational models with robust standard errors to investigate whether the association between maternal depressive symptoms in early childhood and child depressive symptoms in late childhood was mediated by child’s peer victimization experiences. We adjusted for child sex, family adversity and paternal depressive symptoms in early childhood, children’s behavioral dysregulation in early childhood, children’s cognitive ability and bullying behaviors in middle childhood as well as peer victimization at 10 years of age. The population representativeness score was applied to this model. We report standardized regression coefficients throughout the results section.
Does childcare attendance moderate the association between maternal depressive symptoms and (a) peer victimization experiences and (b) depressive symptoms in late childhood?
We tested the moderating role of childcare attendance on the direct associations between maternal depressive symptoms in early childhood and a) peer victimization experiences in middle childhood and b) child’s depressive symptoms in late childhood using linear regressions. If a significant moderating effect between exposure to maternal depression and childcare attendance trajectories was detected, we stratified the analysis by childcare attendance trajectories to probe the interaction effect. The regressions were adjusted with the same set of covariates as previously described and we applied the weights for populational representativeness and social selection into childcare services.
Does childcare attendance moderate the mediated association between mothers’ and children’s depressive symptoms via peer victimization experiences?
Finally, we examined whether childcare attendance moderated the indirect association between maternal depressive symptoms in early childhood and children’s depressive symptoms through peer victimization. We used a multigroup approach where each direct and indirect path were simultaneously estimated for each of the three groups (i.e., 0 = low childcare, 1 = part-time and 2 = full-time childcare attendance). We adjusted the regressions with the same set of covariates as in our previous models. We then compared the fit of the model in which the direct and indirect effects were estimated for each childcare attendance group with the fit of the model with path constraints (i.e., where direct and indirect effects are assumed to be equal between childcare groups) using the Satorra-Bentler test for nested models.
Results
As shown in Table 2, maternal depressive symptoms two months after giving birth were positively correlated with children’s peer victimization experiences, children’s depressive symptoms, exposure to family adversity, paternal depressive symptoms, children’s emotional dysregulation problems and negatively correlated with children’s cognitive abilities. Peer victimization was negatively correlated with children’s cognitive abilities and positively correlated with children’s and mothers’ depressive symptoms and the following covariates: exposure to family adversity, children’s behavioral dysregulation problems, bullying perpetration at age eight and ten, and to peer victimization at age ten. Finally, child depressive symptoms were positively correlated with each covariate included in the main analysis except for a negative correlation with cognitive abilities.
Balance of Socio-Demographic Characteristics Obtained with Propensity Score Weighting
Significant differences in children’s, parents’ and family characteristics were observed among children in our analytical sample and the original ALSPAC sample (see Table S1 in Supplementary Material). We also found differences in socio-demographic characteristics between children following different trajectories of childcare intensity (see Table S2). These characteristics were thus included in the computation of the two PSW scores, one for populational representativeness and one for social selection into childcare services. As shown, in the standardized mean difference plots in supplementary material (see Fig. S1 for population representativeness and S2 for social selection into childcare), PSW significantly reduced standardized mean differences for every socio-demographic characteristic between children in our analytical sample and the original ALSPAC sample, and between children following distinct childcare trajectories, thus increasing their comparability. Of note, the most important characteristics distinguishing children in our analytical sample and the original ALSPAC study were maternal age and education level whereas the most distinguishing factor for attending childcare (part- or full-time) was maternal employment at eight months post-partum.
Does Peer Victimization Mediate the Association Between Mother’s and Child’s Depressive Symptoms?
We fitted a mediational model where maternal depressive symptoms during early childhood were associated with children’s peer victimization in middle childhood (B = 0.04, p < 0.001, R2 = 0.18), and children’s depressive symptoms in late childhood (B = 0.04, p = 0.021, R2 = 0.20). Peer victimization experiences were also associated with children’s depressive symptoms (B = 0.07, p < 0.001). When investigating the mediational effect of peer victimization, we found a significant indirect effect (B = 0.01, p = 0.027; see Fig. 2 and Table 3). The total effect between maternal and child depressive symptoms remained significant after accounting for the indirect effect of peer victimization (B = 0.04, p = 0.013). Additionally, we tested whether the mediated associations varied according to child sex and did not find a significant moderation (Chi-square difference = 3.95, df = 3, p = 0.273).

Mediational pathways from mothers to children’s depressive symptoms via peer victimization. The full black lines represent the associations between study variables. The dashed black line represents the mediation total effect. The dashed gray lined represents the indirect effect between mothers’ and children’s depressive symptoms via peer victimization experiences (i.e., indirect effect). The mediational model is weighted with the populational representativeness score and adjusted with the set of covariates for the main analysis: children’s sex, family adversity in early childhood, children’s behavioral dysregulation in early childhood, and children’s cognitive abilities, bullying behaviors in middle childhood and peer victimization reported at 10 years old.
Does childcare attendance moderate the association between maternal depressive symptoms and (a) peer victimization experiences and (b) depressive symptoms in late childhood?
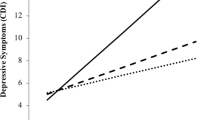
We did not find a significant interaction between childcare attendance and maternal depressive symptoms in early childhood when predicting peer victimization at eight years old (B maternal depression × childcare part-time = −0.01, p = 0.739; B maternal depression × childcare full-time = −0.01, p = 0.771). However, we found that part-time childcare attendance attenuated the relation between maternal depression in early childhood and children’s depressive symptoms in late childhood (B maternal depression × childcare part-time = −0.08, p = 0.008). We did not find this association for full-time childcare attendance (B maternal depression × childcare full-time = −0.05, p = 0.197). Using stratified analyses, we found that the associations between mothers and children’s depressive symptoms were no longer significant for children attending part-time (B = −0.10, p = 0.072, R2 = 0.23), whereas this association remained for children who attended low childcare (B = 0.06, p = 0.002, R2 = 0.20). The association between maternal depression and children’s depressive symptoms was not significant for children in full-time childcare (B = 0.01, p = 0.870, R2 = 0.23). All standardized regression coefficients are presented in Supplementary Table S5.
Does Childcare Attendance Moderate the Mediated Association Between Mother and Child Depressive Symptomatology via Peer Victimization Experiences?
We did not find a significant moderating effect of childcare attendance on the association between maternal and child depressive symptoms via peer victimization experiences. More specifically, the strength of the indirect effects was not significantly different between childcare trajectories (low childcare, part-time childcare and full-time childcare; all ps > 0.800; see Table S4 in Supplementary Material).
Discussion
Using data from a population-based longitudinal study of children followed up prospectively from pregnancy to 10 years, we found that children growing up with mothers who reported higher levels of maternal depressive symptoms during their offspring’s early childhood had higher levels of depressive symptoms in late childhood, and that this association was partially explained by peer victimization experiences. While the mediational pathway was not moderated by childcare attendance, we found a significant interaction between part-time childcare attendance and maternal depression where part-time attendance was a protective factor of the intergenerational transmission of depressive symptoms from mothers to children. We found an interaction similar in direction and strength between full-time childcare attendance and maternal depression; however, this interaction did not reach statistical significance, potentially due to the limited sample size of children in the full-time childcare trajectories. In addition, when investigating the main effect between exposure to maternal depression and child depression according to childcare trajectories (i.e., stratified analysis), we found no association between maternal depression and child depression for children who attended part- and full-time childcare—suggesting a cancellation of risk—whereas there was a significant association between mothers’ and children’s depression symptoms for children who did not attend group-based childcare. Our results are concordant with the Integrative Model for the Transmission of Risk (Goodman & Gotlib, 1999) which posits deficits in affective, social, and cognitive skills among children exposed to maternal depression, increasing their vulnerabilities to psychopathologies. Yet, our results also suggest that environmental factors such as childcare attendance may buffer—or even cancel—this developmental cascade.
Peer Victimization as a Mediating Factor Between Mother and Child Depressive Symptoms
The role of peer victimization experiences has previously been suggested to explain the association between post-natal maternal depression and children’s depressive symptoms (Côté et al., 2018). In our study, we were able to replicate this finding using a shorter timeline between peer victimization and the onset of depressive symptoms. Admittedly, children exposed to high levels of maternal depressive symptoms may experience additional challenges within and outside their home environment (e.g., low level of maternal sensitivity and warm parenting, neighborhood violence (Bernard et al., 2018; Saitadze, 2022)). These experiences may jeopardize the development of their socio-emotional skills in parallel or jointly with peer victimization (e.g., emotion recognition). Children’s difficulty to recognize their own emotions has previously been associated with higher levels of relational peer victimization and internalized symptomatology among girls (Hamilton et al., 2016).
From a developmental perspective, future studies should also examine the dynamic and potentially reciprocal patterns of associations between peer victimization and mental health symptomatology. Chen et al. (2020) recently found in a cross-sectional study that adolescents’ depressive symptoms partially explained the association between maternal depression and adolescents’ peer victimization experiences. As children enter the teenage years, their depressive symptomatology may partly underlie the association between mothers’ depression and adolescents’ peer victimization. Previously, Boivin et al. (2010) suggested a dynamic relationship between children internalized and externalized symptomatology and peer victimization experiences. During childhood, children who are aggressive and disruptive are generally negatively perceived by peers and are more likely to be excluded from peer-directed play (Bierman et al., 2015) and peer victimized, whereas children who display internalized symptoms are not more frequently victimized by their peers (Bierman et al., 2015). However, as children grow older, internalizing behaviors such as anxiety and social withdrawal become more salient and more negatively perceived by peers who may target children with internalized behaviors more frequently (Boivin et al., 2010). This potential shift across developmental periods between mental health symptomatology and peer victimization experiences deserves further attention.
Protective Role of Childcare Attendance for Children Exposed to Maternal Depressive Symptoms
In concordance with previous studies, we found some evidence that childcare attendance could be a protective factor for children exposed to higher levels of maternal depressive symptoms regarding children’s later internalized symptoms (Charrois et al., 2020; Giles et al., 2011; Herba et al., 2013; Lee et al., 2006; Paquin et al., 2020). Similar to Lee et al. (2006) and Giles et al. (2011), we found that part-time childcare attendance was a protective exposure for children exposed to maternal depression. Comparatively to Giles et al. (2011), we did not find that full-time childcare interacted with maternal depression. This result is surprising given the sample size (N = 255 children) of the full-time childcare group which would allow for the detection of small effect sizes. Future studies should examine whether the quality of childcare could be confounding factor for children who spend extended periods in childcare settings. Additionally, these studies should explore complementary processes that could potentially contribute to higher levels of depressive symptomatology among children in full-time childcare, such as the quality of childcare.
For children exposed to maternal depression, the time away from home and exposure to the peer group as well as caring adults might counteract (or buffer) the effect of mother’s depressive symptoms on children’s social development and well-being, further protecting them from the onset of internalized symptoms. However, this protective role did not come into effect through a diminution in peer victimization experiences. Future studies should attempt to identify how childcare attendance modifies the association between mothers and children’s depressive symptoms, that is, the mechanisms underlying this association. For example, Herba et al. (2013) found that children exposed to maternal depression who also attended childcare services had lower levels of social withdrawal than those who remain under maternal care. Notably, social withdrawal during early childhood was indirectly associated with adolescent depressive symptoms in young adulthood through adolescents’ interpersonal impairments (i.e., quality of peer interactions and friendship) (Katz et al., 2011). Of note, Herba et al. (2013) examined the moderating effect of the age of the child at childcare entry as well as the type of childcare attended. Finally, it is also possible that the association between maternal depression and peer victimization experiences could be mediated by other factors such as parenting practices. A deeper examination of the first segment of the mediation model can inform the development of preventive interventions in early childhood.
Lastly, another potential mechanism at play is the improvement of maternal mental health during early childhood while her child attends childcare services. More specifically, during the time the child attends childcare, mothers may have more time to focus on their mental and physical health or prevent further increases in parental stress. This limited time apart may help children and mothers to preserve warmer and more sensitive interactions, a known mediating factor between maternal depression and positive child development (Elgar et al., 2007). To better understand these reciprocal associations between childcare attendance and mothers’ mental health and parenting practices, future studies are necessary and should rely on statistical models aiming to disentangle between and within-person effects.
Strengths and Limitations
The strengths of this study include its large sample, the long-term follow-up, the repeated measures of maternal and paternal depressive symptoms during early childhood, and the range of socio-demographic and child characteristics that were included in the two propensity scores derived to account for social selection into childcare services and population representativeness. The population representativeness score adjusts for differential attrition which contributes to increase the generalizability of the results to the original population whereas the propensity score for social selection into childcare allows to isolate the effect of childcare attendance on the outcome investigated by increasing the comparability of children following different childcare trajectories beyond their potential confounders.
There are, however, a few limitations that may have constrained the study findings. First, we did not have a measure of maternal depression when the child was 10 years old, and thus could not control for the co-occurring influence of maternal depression in the targeted associations. Though, in a previous study, Charrois et al. (2020) investigated the association between maternal depression in early childhood and internalized symptoms in early adolescence and found that the association remained significant even after controlling for concurrent maternal depression. This result suggests that adding this control variable might not have greatly changed the magnitude and direction of our results. Second, we did not control for children’s internalized symptoms and peer victimization experiences during early childhood, but we adjusted for children’s behavioral dysregulation problems in early childhood using the total difficulty score of the SDQ (Goodman, 1997), which may have captured such individual differences. Third, we did not have the information to consider sibling bullying which could also occurs among children exposed to maternal depression and increase their risk of developing depressive symptoms. Unfortunately, sibling bullying was collected in the ALSPAC study after child’s depressive symptoms. Finally, we did not have a measure of childcare quality which prevented us to examine how this indicator may further modify the associations uncovered in the present study. Disentangling the effect of childcare quality versus quantity has important clinical and political implications (Belsky, 2006).
Implications
Childcare attendance did not modify the association between exposure to maternal depression in early childhood and peer victimization in middle childhood, yet part-time childcare attendance modified the direct association between mothers and children’s depression. Universal childcare access with flexible attendance policies (i.e., allowing part-time care) could be a promising public health initiative as it would allow reaching mothers who are going back to work gradually and who have more limited income to register their children in group-based childcare. This childcare policy could increase the social support system of mothers struggling with depression through new relationships with parents, childcare providers, and peers (Johnson & Padilla, 2019; McCartney et al., 2007). Finally, as peer victimization partly explained the association between depressive symptomatology in mothers and children, pediatricians, as well as other health and education stakeholders who are in close contact with mothers and children, may want to monitor children’s peer victimization experiences, especially in the context of prior exposure to maternal depression. Psychological support to rapidly reduce peer victimization may represents a promising strategy to prevent the onset, persistence, or aggravation of children’s depressive symptoms.
References
Angold, A., Costello, E. J., Messer, S. C., Pickles, A., Winder, F., & Silver, D. (1995). Development of a short questionnaire for use in epidemiological studies of depression in children and adolescents. International Journal of Methods in Psychiatric Research, 5, 237–249.
Apter-Levi, Y., Pratt, M., Vakart, A., Feldman, M., Zagoory-Sharon, O., & Feldman, R. (2016). Maternal depression across the first years of life compromises child psychosocial adjustment; relations to child HPA-axis functioning. Psychoneuroendocrinology, 64, 47–56. https://doi.org/10.1016/j.psyneuen.2015.11.006.
Austin, P. C., & Stuart, E. A. (2015). Moving towards best practice when using inverse probability of treatment weighting (IPTW) using the propensity score to estimate causal treatment effects in observational studies. Statistics in Medicine, 34(28), 3661–3679.
Azeredo, C. M., Santos, I. S., Barros, A. J. D., Barros, F. C., & Matijasevich, A. (2017). Maternal depression and bullying victimization among adolescents: Results from the 2004 Pelotas cohort study. Depression and Anxiety, 34(10), 897–907. https://doi.org/10.1002/da.22662.
Barker, E. D., Cecil, C.A.M., Walton, E., Houtepen, L.C., O'Connor, T.G., Danese, A., & Roberts, S. (2018). Inflammation-related epigenetic risk and child and adolescent mental health: A prospective study from pregnancy to middle adolescence. Development and Psychopathology, 30, 1145–1156.
Belsky, J. (2006). Early child care and early child development: Major findings of the NICHD study of early child care. European Journal of Developmental Psychology, 3(1), 95–110. https://doi.org/10.1080/17405620600557755.
Bernard, K., Nissim, G., Vaccaro, S., Harris, J. L., & Lindhiem, O. (2018). Association between maternal depression and maternal sensitivity from birth to 12 months: A meta-analysis. Attachment & Human Development, 20(6), 578–599. https://doi.org/10.1080/14616734.2018.1430839.
Berry, D., Blair, C., Willoughby, M., Garrett-Peters, P., Vernon-Feagans, L., & Mills-Koonce, W. R. (2016). Household chaos and children’s cognitive and socio-emotional development in early childhood: Does childcare play a buffering role? Early Childhood Research Quarterly, 34, 115–127. https://doi.org/10.1016/j.ecresq.2015.09.003.
Bierman, K. L., Kalvin, C. B., & Heinrichs, B. S. (2015). Early childhood precursors and adolescent sequelae of grade school peer rejection and victimization. Journal of Clinical Child & Adolescent Psychology, 44(3), 367–379. https://doi.org/10.1080/15374416.2013.873983.
Boivin, M., Petitclerc, A., Feng, B., & Barker, E. D. (2010). The developmental trajectories of peer victimization in middle to late childhood and the changing nature of their behavioral correlates. Merrill-Palmer Quarterly, 56(3), 231–260.
Bowen, E., Heron, J., Waylen, A., & Wolke, D. (2005). Domestic violence risk during and after pregnancy: Findings from a British longitudinal study. BJOG: An International Journal of Obstetrics & Gynaecology, 112(8), 1083–1089. https://doi.org/10.1111/j.1471-0528.2005.00653.x.
Boyd, A., Golding, J., Macleod, J., Lawlor, D. A., Fraser, A., Henderson, J., Molloy, L., Ness, A., Ring, S., & Davey Smith, G. (2013). Cohort profile: The ‘Children of the 90s’—the index offspring of the Avon Longitudinal Study of Parents and Children. International Journal of Epidemiology, 42(1), 111–127. https://doi.org/10.1093/ije/dys064.
Charrois, J., Côté, S. M., Japel, C., Séguin, J. R., Paquin, S., Tremblay, R. E., & Herba, C. M. (2017). Child-care quality moderates the association between maternal depression and children’s behavioural outcome. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 58(11), 1210–1218. https://doi.org/10.1111/jcpp.12764.
Charrois, J., Côté, S. M., Paquin, S., Séguin, J. R., Japel, C., Vitaro, F., Kim-Cohen, J., Tremblay, R. E., & Herba, C. M. (2020). Maternal depression in early childhood and child emotional and behavioral outcomes at school age: Examining the roles of preschool childcare quality and current maternal depression symptomatology. European Child & Adolescent Psychiatry, 29(5), 637–648. https://doi.org/10.1007/s00787-019-01385-7.
Chen, J.-K., Wu, C., Chang, C.-W., & Wei, H.-S. (2020). Indirect effect of parental depression on school victimization through adolescent depression. Journal of Affective Disorders, 263, 396–404. https://doi.org/10.1016/j.jad.2019.11.126.
Cicchetti, D., & Toth, S. L. (1998). The development of depression in children and adolescents. American Psychologist, 53(2), 221–241. https://doi.org/10.1037/0003-066X.53.2.221.
Côté, S. M., Ahun, M. N., Herba, C. M., Brendgen, M., Geoffroy, M.-C., Orri, M., Liu, X., Vitaro, F., Melchior, M., Boivin, M. & & Tremblay, R. E. (2018). Why is maternal depression related to adolescent internalizing problems? A 15-year population-based study. Journal of the American Academy of Child & Adolescent Psychiatry, 57(12), 916–924. https://doi.org/10.1016/j.jaac.2018.04.024.
Cox, J. L., Holden, J. M., & Sagovsky, R. (1987). Detection of postnatal depression: Development of the 10-item Edinburgh Postnatal Depression Scale. The British Journal of Psychiatry, 150(6), 782–786. https://doi.org/10.1192/bjp.150.6.782.
Dearing, E., & Zachrisson, H. D. (2017). Concern over internal, external, and incidence validity in studies of child-care quantity and externalizing behavior problems. Child Development Perspectives, 11(2), 133–138. https://doi.org/10.1111/cdep.12224.
Elgar, F. J., Mills, R. S. L., McGrath, P. J., Waschbusch, D. A., & Brownridge, D. A. (2007). Maternal and paternal depressive symptoms and child maladjustment: The mediating role of parental behavior. Journal of Abnormal Child Psychology, 35(6), 943–955. https://doi.org/10.1007/s10802-007-9145-0.
Fraser, A., Macdonald-Wallis, C., Tilling, K., Boyd, A., Golding, J., Davey Smith, G., Henderson, J., Macleod, J., Molloy, L., Ness, A., Ring, S., Nelson, S. M., & Lawlor, D. A. (2013). Cohort profile: The Avon Longitudinal Study of parents and children: ALSPAC mothers cohort. International Journal of Epidemiology, 42(1), 97–110. https://doi.org/10.1093/ije/dys066.
Giles, L. C., Davies, M. J., Whitrow, M. J., Warin, M. J., & Moore, V. (2011). Maternal depressive symptoms and child care during toddlerhood relate to child behavior at age 5 years. Pediatrics, 128(1), e78–e84. https://doi.org/10.1542/peds.2010-3119.
Goelman, H., Zdaniuk, B., Boyce, W. T., Armstrong, J. M., & Essex, M. J. (2014). Maternal mental health, child care quality, and children’s behavior. Journal of Applied Developmental Psychology, 35(4), 347–356. https://doi.org/10.1016/j.appdev.2014.05.003.
Goodman, R. (1997). The strengths and difficulties questionnaire: A research note. Journal of Child Psychology and Psychiatry, 38(5), 581–586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x.
Goodman, S. H. (2007). Depression in mothers. Annual Review of Clinical Psychology, 3(1), 107–135. https://doi.org/10.1146/annurev.clinpsy.3.022806.091401.
Goodman, S. H., & Gotlib, I. H. (1999). Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychological Review, 106(3), 458–490. https://doi.org/10.1037/0033-295X.106.3.458.
Goodman, S. H., Rouse, M. H., Connell, A. M., Broth, M. R., Hall, C. M., & Heyward, D. (2011). Maternal depression and child psychopathology: A meta-analytic review. Clinical Child and Family Psychology Review, 14(1), 1–27. https://doi.org/10.1007/s10567-010-0080-1.
Gray, A. (2005). The changing availability of grandparents as carers and its implications for childcare policy in the UK. Journal of Social Policy, 34(4), 557–577. https://doi.org/10.1017/S0047279405009153.
Gregg, P., Washbrook, E., Propper, C., & Burgess, S. (2005). The effects of a mother’s return to work decision on child development in the UK. The Economic Journal, 115(501), F48–F80. https://doi.org/10.1111/j.0013-0133.2005.00972.x.
Hamilton, J. L., Kleiman, E. M., Rubenstein, L. M., Stange, J. P., Flynn, M., Abramson, L. Y., & Alloy, L. B. (2016). Deficits in emotional clarity and vulnerability to peer victimization and internalizing symptoms among early adolescents. Journal of Youth and Adolescence, 45(1), 183–194. https://doi.org/10.1007/s10964-015-0260-x.
Herba, C. M., Tremblay, R. E., Boivin, M., Liu, X., Mongeau, C., Séguin, J. R., & Côté, S. M. (2013). Maternal depressive symptoms and children’s emotional problems: Can early child care help children of depressed mothers? JAMA Psychiatry, 70(8), 830–838. https://doi.org/10.1001/jamapsychiatry.2013.1361.
Honaker, J., King, G., & Blackwell, M. (2011). Amelia: A program for missing data. Journal of Statistical Software, 45(7). https://doi.org/10.18637/jss.v045.i07.
Jaffee, S. R., Sligo, J. L., McAnally, H. M., Bolton, A. E., Baxter, J. M., & Hancox, R. J. (2021). Early-onset and recurrent depression in parents increases risk of intergenerational transmission to adolescent offspring. Journal of Child Psychology and Psychiatry, 62(8), 979–988. https://doi.org/10.1111/jcpp.13356.
Johnson, A. D., & Padilla, C. M. (2019). Childcare instability and maternal depressive symptoms: Exploring new avenues for supporting maternal mental health. Academic Pediatrics, 19(1), 18–26. https://doi.org/10.1016/j.acap.2018.05.006.
Jung, T., & Wickrama, K.A.S. (2008). An introduction to latent class growth analysis and growth mixture modeling. Social and Personality Psychology Compass, 2, 302–317.
Katz, S. J., Conway, C. C., Hammen, C. L., Brennan, P. A., & Najman, J. M. (2011). Childhood social withdrawal, interpersonal impairment, and young adult depression: A mediational model. Journal of Abnormal Child Psychology, 39(8), 1227 https://doi.org/10.1007/s10802-011-9537-z.
Larose, M. P., Côté, S. M., Ouellet-Morin, I., Maughan, B., & Barker, E. D. (2021). Promoting better functioning among children exposed to high levels of family adversity: The protective role of childcare attendance. Journal of Child Psychology and Psychiatry, 62(6), 762–770.
Lee, L.-C., Halpern, C. T., Hertz-Picciotto, I., Martin, S. L., & Suchindran, C. M. (2006). Child care and social support modify the association between maternal depressive symptoms and early childhood behaviour problems: A US national study. Journal of Epidemiology & Community Health, 60(4), 305–310. https://doi.org/10.1136/jech.2005.040956.
McCartney, K., Dearing, E., Taylor, B. A., & Bub, K. L. (2007). Quality child care supports the achievement of low-income children: Direct and indirect pathways through caregiving and the home environment. Journal of Applied Developmental Psychology, 28(5–6), 411–426. https://doi.org/10.1016/j.appdev.2007.06.010.
McLachlan, G. J., & Peel, D. (2004). Finite mixture models. John Wiley & Sons.
Olweus, D. (1993). Bullying at school: What we know and what we can do. Blackwell Publishing.
Oncioiu, S. I., Orri, M., Boivin, M., Geoffroy, M.-C., Arseneault, L., Brendgen, M., Vitaro, F., Navarro, M. C., Galéra, C., Tremblay, R. E., & Côté, S. M. (2020). Early childhood factors associated with peer victimization trajectories from 6 to 17 years of age. Pediatrics, 145(5), e20192654. https://doi.org/10.1542/peds.2019-2654.
Orri, M., Tremblay, R. E., Japel, C., Boivin, M., Vitaro, F., Losier, T., Brendgen, M. R., Falissard, B., Melchior, M., & Côté, S. M. (2019). Early childhood child care and disruptive behavior problems during adolescence: A 17-year population-based propensity score study. Journal of Child Psychology and Psychiatry, 60(11), 1174–1182. https://doi.org/10.1111/jcpp.13065.
Paquin, C., Castellanos-Ryan, N., Vitaro, F., Côté, S. M., Tremblay, R. E., Séguin, J. R., Boivin, M., & Herba, C. M. (2020). Maternal depression symptoms, child behavior problems, and their transactional relations: Probing the role of formal childcare. Development and Psychopathology, 32(3), 831–844. https://doi.org/10.1017/S0954579419000956.
Pearson, R. M., Evans, J., Kounali, D., Lewis, G., Heron, J., Ramchandani, P. G., O’Connor, T. G., & Stein, A. (2013). Maternal depression during pregnancy and the postnatal period: Risks and possible mechanisms for offspring depression at age 18 years. JAMA Psychiatry, 70(12), 1312–1319. https://doi.org/10.1001/jamapsychiatry.2013.2163.
Perren, S., Stadelmann, S., & von Klitzing, K. (2009). Child and family characteristics as risk factors for peer victimization in kindergarten. Schweizerische Zeitschrift Für Bildungswissenschaften, 31(1), 13–32.
R Core Team. (2020). R: A language and environment for statistical computing. [Computer software]. R Foundation for Statistical Computing. https://www.R-project.org/.
Register General’s Classification. (1990). Standard occupation classification.
Ridgeway, G., Kovalchik, S. A., Griffin, B. A., & Kabeto, M. U. (2015). Propensity score analysis with survey weighted data. Journal of Causal Inference, 3(2), 237–249. https://doi.org/10.1515/jci-2014-0039.
Rosseel, Y. (2012). lavaan: An R package for structural equation modeling. Journal of Statistical Software, 48(2), 1–36.
Saitadze, I. (2022). The effects of neighborhood factors, maternal depression and parental emotional support on social—behavioral outcomes of children involved in the child welfare system. Journal of Public Child Welfare, 16(2), 249–271. https://doi.org/10.1080/15548732.2021.1874593.
Schindler, P. J., Moely, B. E., & Frank, A. L. (1987). Time in day care and social participation of young children. Developmental Psychology, 23(2), 255–261. https://doi.org/10.1037/0012-1649.23.2.255.
Taylor, C. M., Golding, J., Hibbeln, J., & Emond, A. M. (2013). Environmental factors predicting blood lead levels in pregnant women in the UK: the ALSPAC study. PLoS ONE, 8(9), e72371. https://doi.org/10.1371/journal.pone.0072371.
Tsypes, A., & Gibb, B. E. (2015). Peer victimization mediates the impact of maternal depression on risk for suicidal ideation in girls but not boys: A prospective study. Journal of Abnormal Child Psychology, 43(8), 1439–1445. https://doi.org/10.1007/s10802-015-0025-8.
Verboom, C. E., Sijtsema, J. J., Verhulst, F. C., Penninx, B. W. J. H., & Ormel, J. (2014). Longitudinal associations between depressive problems, academic performance, and social functioning in adolescent boys and girls. Developmental Psychology, 50(1), 247–257. https://doi.org/10.1037/a0032547.
Wechsler, D., Golombok, S., & Rust, J. (1992). WISC-III UK Wechsler intelligence scale for children: UK manual. The Psychological Corporation.
West, A., & Noden, P. (2016). Public funding of early years education in England: An historical perspective. London School of Economics.
Wolke, D., Woods, S., Bloomfield, L., & Karstadt, L. (2001). Bullying involvement in primary school and common health problems. Archives of Disease in Childhood, 85(3), 197–201. https://doi.org/10.1136/adc.85.3.197.
Zachrisson, H. D., & Dearing, E. (2015). Family income dynamics, early childhood education and care, and early child behavior problems in Norway. Child Development, 86(2), 425–440. https://doi.org/10.1111/cdev.12306.
Zwierzynska, K., Wolke, D., & Lereya, T. S. (2013). Peer victimization in childhood and internalizing problems in adolescence: A prospective longitudinal study. Journal of Abnormal Child Psychology, 41(2), 309–323. https://doi.org/10.1007/s10802-012-9678-8.
Acknowledgements
We are extremely grateful to all the families who took part in this study, the midwives for their help in recruiting them, and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses.
Funding
The UK Medical Research Council and Wellcome (Grant ref: 217065/Z/19/Z) and the University of Bristol provide core support for ALSPAC. M-PL is supported by a postdoctoral fellowship from the Fonds de Recherche en Santé du Québec. IO-M is a Canada Research Chair in the Developmental Origins of Vulnerability and Resilience. The funding sources had no involvement in the interpretation of data, writing of the report, and the decision to submit the article for publication. This publication is the work of the authors and Author will serve as guarantors for the contents of this paper. Open Access funding provided by University of Turku (including Turku University Central Hospital).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no competing interests.
Ethical Approval
The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Ethical approval for the study was obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees.
Informed Consent
Informed consent was obtained from all participants included in the study. Informed consent to use the data collected via questionnaires and clinics was obtained from participants following the recommendations of the ALSPAC Ethics and Law Committee at the time.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Larose, MP., Barker, E.D., Ouellet-Morin, I. et al. Does Childcare Attendance Moderate the Associations Between Mother-Child Depressive Symptoms and Children’s Peer Victimization Experiences?. J Child Fam Stud (2024). https://doi.org/10.1007/s10826-024-02885-0
Accepted:
Published:
DOI: https://doi.org/10.1007/s10826-024-02885-0