
Abstract
While it is well-known that individuals with autism spectrum disorder (ASD) have difficulties processing faces, very little is known about the origins of these deficits. The current study focused on 6- and 11-month-old infants who were at either high-risk (n = 43) or low-risk (n = 31) for developing ASD based on having a sibling already diagnosed with the disorder. Eye-tracking data were collected while the infants viewed color photographs of faces. Similar to previous studies with both typically developing adults and infants, low-risk infants demonstrated a preference for looking at the left side of the face (known as a left visual field bias) that emerged by 11 months of age. In contrast, high-risk infants did not demonstrate a left visual field bias at either age. Comparisons of the amount of attention given to the eye versus mouth regions indicated no differences between the two risk groups.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
There is considerable evidence indicating that individuals with autism spectrum disorder (ASD) have difficulties perceiving and remembering faces. Research studies have shown that children and adults with ASD have difficulty discriminating facial expressions, (e.g., Celani et al. 1999; Rump et al. 2009), categorizing facial gender (e.g., Behrmann et al. 2006; Best et al. 2010), and recognizing faces (e.g., Klin et al. 1999; Lahaie et al. 2006; Newell et al. 2010). The most common explanation for these difficulties is that individuals with ASD, in contrast to typically developing individuals, discriminate faces based more on details and featural information than on spatial or configural information. Indeed, studies with children and adults with ASD indicate that they rely more on the detailed high spatial frequency information contained in faces than do control individuals (Boeschoten et al. 2007; Deruelle et al. 2004).
Even though young infants perceive and recognize faces, it is clear that the level of expertise demonstrated by adults to perceive subtle aspects of a face requires extensive learning, and studies suggest that face processing may not reach full maturity until adolescence or adulthood (Rump et al. 2009; Scherf et al. 2009). Consequently, it has been suggested that there may also be differences in how individuals with ASD learn about faces. More specifically, it has been suggested that people with ASD have problems with top-down learning mechanisms. For example, classic cognitive theories of face processing (e.g., Valentine 1991) suggest that with development, individuals represent the faces they experience in an organized memory space centered on prototypical facial information. These models are used to explain several well-known aspects of face processing including why distinctive faces are remembered better than more typical faces (Best and Strauss 2007; Humphreys 2003; Rhodes et al. 1987), why faces that are typical representatives of a gender are categorized better than faces that are less typical representatives of gender (e.g., O’Toole et al. 1998), and why typical faces are perceived as more attractive than atypical faces (e.g., Rubenstein et al. 1999). Interestingly, studies with children and adults have shown that individuals with ASD have difficulty abstracting prototypic representations of faces, which may significantly impact the way facial knowledge is acquired during development (Gastgeb et al. 2009, 2011).
While it may take until adulthood to acquire full expertise in processing faces (e.g., see review by Mondloch et al. 2002), the research has also clearly shown that the learning process begins during infancy. Within the first year of life, infants are able to abstract prototypical representations of faces (de Haan et al. 2001; Strauss 1979), have better memories for faces from their own cultures than either other cultures or other species (Kelly et al. 2007; Pascalis and Kelly 2009; Liu et al. 2011), are able to categorize faces by gender (Quinn et al. 2002); Newell et al. 2010) and prefer looking at faces that are considered by adults to be more attractive based on typicality (Quinn et al. 2008; Rubenstein et al. 1999).
Thus, in order to understand the origins of the problems that individuals with ASD have with respect to perceiving and remembering faces, it is important to study potential differences in face processing mechanisms in very young children and infants. Studies with children younger than four years of age have indeed shown that young children and toddlers with ASD demonstrate face processing differences when compared to typically developing children (Chawarska et al. 2010; Vlamings et al. 2010; Webb et al. 2006).
Because children younger than 2 years of age cannot be reliably diagnosed with ASD, there has been a growing interest in studying infants who have an older sibling already diagnosed with ASD. These genetically “high-risk” (HR) infants are usually compared to infants considered to be of “low-risk” (LR) for developing ASD based on their having older siblings who do not have ASD. Current estimates suggest that as many as 20% of HR infants will be eventually diagnosed with ASD (Elsabbagh and Johnson 2010; Ozonoff et al. 2011; Tager-Flusberg 2010). While most HR infants do not actually end up being diagnosed with ASD, it is clear that, because of heritability, HR infants may have many traits in common with diagnosed individuals. In fact, it has been shown that HR infants have delays and problems in the development of basic processes such as language and motor skills (for review, see Rogers 2009). Therefore, studying HR infants will help researchers gain an understanding of the ASD endophenotype.
More specific to face processing, research with first-degree family members of individuals who have ASD suggest there may be a genetic basis to face processing deficits. Studies of parents (Dawson et al. 2005; Pellicano 2008) of children who have ASD demonstrate atypical face processes in these individuals and ERP studies specifically with HR infants suggest there may be face processing difficulties by as early as 10–12 months of age (Luyster et al. 2011; McCleery et al. 2009).
Eye-tracking methodologies have also been used to study potential differences in the way in which individuals with ASD process faces and have been extended to studying HR versus LR infants. Since one clinical symptom of ASD is reduced eye contact (American Psychiatric Association 2000), a number of eye-tracking studies have examined the amount of time that older children and adults with ASD look at eyes versus mouths. Several of these studies suggest that individuals with ASD attend less to the eyes and more to the mouth than do typically developing individuals (Corden et al. 2008; Hernandez et al. 2009; Neumann et al. 2006; Norbury et al. 2009; Spezio et al. 2006). However, this finding has not always been replicated (Fletcher-Watson et al. 2009; van der Geest et al. 2001). Similarly, a study of HR infants (Merin et al. 2007) found decreased eye contact in a group of 6-month-old HR infants, although, a follow-up study of these infants suggested that the decreased eye contact may not be clinically predictive of ASD (Young et al. 2009).
While many studies on HR infants and children with ASD have focused on potential atypical differences in fixating on eye versus mouth regions, there are no published developmental studies investigating presence of a left visual field (LVF) bias for faces in this population. Starting with the first chimeric face study (Wolff 1933) in which participants were shown fused faces composed of either two left halves or two right halves of a face, it has been demonstrated that typically developing individuals are biased to pay more attention to facial information in the LVF. Information from the LVF is projected to the right hemisphere (RH), which is known to be associated with face processing abilities, with notable lateralization in the right fusiform gyrus (see review by Haxby et al. 2000). Not surprisingly, given that individuals with ASD have impaired face processing abilities, it has been demonstrated that there is diminished activation of the right face fusiform area (FFA), and subsequently less lateralization of FFA BOLD activation, in individuals with ASD (see review by Curby et al. 2010).
The direct relation between RH specialization for face processing and the LVF bias during face processing was established by De Renzi and colleagues (1994) when they found that individuals with RH damage demonstrated a decline in face recognition abilities did not display any recognition advantage for stimuli presented in the LVF. Yovel et al. (2008) conducted a longitudinal fMRI and eye-tracking study that showed that the extent of an individual’s LVF bias is correlated with the magnitude of the asymmetry in processing faces in the RH versus the LH. They also found the degree of individual hemispheric asymmetry to be a stable magnitude, measured over time.
More recently, studies have employed the use of eye-tracking technology to confirm the presence of an LVF bias. Using a gender discrimination task, Butler et al. (2005) showed that typically developing individuals make more fixations in the LVF than the RVF. In this study, the LVF effect was more reliable when measuring the location of just the first saccade then the total number of fixations to the LVF versus RVF. However, more recent studies have found a LVF bias for the total amount of time individuals spend looking at the LVF in comparison to the RVF (Butler and Harvey 2006; Guo et al. 2009). In fact, Guo et al. (2009) found the increase in LVF looking time to be seen only for upright human faces, with the first saccade to the LVF also present for the viewing of inverted human faces, and upright and inverted monkey faces.
A leftward gaze bias may seem counter-intuitive to the idea of a left visual field superiority for faces, because looking to the left does in fact put more of the face in the right visual field. Despite this, however, the left gaze has been found to be consistent with the LVF bias (Butler et al. 2005; Butler and Harvey 2006), and increased leftward fixations during face processing is correlated with heightened right hemisphere activation (Yovel et al. 2008). A possible explanation for this is that with the development of face expertise and specialization, we come to process faces in right hemisphere. This leads to a tendency to pay more attention to facial information in the LVF, which is mostly being projected to the RH. Essentially, the argument is that RH specialization leads to more interest and exploration of the facial information on the left, which leads to a bias to turn toward and explore that side of a person’s face. Thus, the argument is the LVF bias comes from specialization and the development of expertise in the perception of faces.
This specialization appears to develop early in typically developing children. Eye-tracking studies of typically developing infants suggest that sometime between 6 and 12 months of age, infants develop an LVF bias and spend more time fixating the side of the face to the left (Guo et al. 2009; Liu et al. 2011; Wheeler 2010). While this bias is demonstrated in typically developing infants, a recent study (Dundas et al. 2011) with adults suggests that individuals with ASD do not demonstrate an LVF bias and that this lack of bias may reflect hemispheric differences in the way individuals with ASD process faces. It is unknown, however, whether very young children with ASD or HR infants might also demonstrate a lack of this LVF bias. It is known that first-degree relatives of individuals with ASD also demonstrate face processing difficulties (Dawson et al. 2005; Pellicano 2008). Thus it is possible that, that similar ot adults with ASD, HR infants may not demonstrate an LVF bias, and hence, it might be an endophenotypic maker for ASD. The purpose of the present study is to explore whether HR infants in comparison to LR infants demonstrate differences in the amount of attention they spend to the left versus right half of a face. In line with prior research, the study also examined whether or not there is a difference in fixating on the eye versus mouth region of faces.
Method
Participants
Participants consisted of infant siblings of children with ASD (high-risk infants; HR) and infant siblings of typically developing children (low-risk infants; LR). HR infants were required to have at least one older sibling diagnosed with ASD and LR infants were required to have no older siblings diagnosed with ASD. Two age groups were tested, 6-month-old and 11-month-old infants. The 6-month-old group consisted of 15 HR infants and 14 LR infants. Five HR and 3 LR infants were originally eliminated because of fussiness and an inability to maintain eye-tracking. The 11-month-old group consisted of 28 HR infants and 17 LR infants. One HR and 4 LR infants were eliminated because of fussiness and an inability to maintain eye tracking. Twenty of the 11-month-old infants were also tested at 6 months of age and thus represent a longitudinal sub-sample.
All infants were recruited by the Autism Center for Excellence (ACE) at the University of Pittsburgh. For the HR infants, their older sibling’s ASD diagnosis was confirmed using the Autism Diagnostic Observation Schedule-Generic (ADOS-G, Lord et al. 2000) and the Autism Diagnostic Interview-Revised (ADI-R, Lord et al. 1994). For the LR infants a phone screen was completed with a parent before inclusion in the study to insure that there were no older siblings or first and second degree relatives of the infant diagnosed with ASD. Additionally, both LR and HR infants were excluded if they had a birth weigh less than 2,500 g, or had problems with pregnancy, labor or delivery, traumatic brain injury, prenatal illicit drug or alcohol use, or birth defects. HR and LR infants were evaluated at each age point (i.e., 6 months of age and 11 months of age) using the Mullen Scales of Early Learning (MSEL; Mullen 1995). The MSEL is a standardized measure of language and cognitive functioning that consists of four subscales: visual reception, fine motor, receptive language, and expressive language. Patterned after Rogers (2009), the receptive and expressive language age equivalents were combined into a verbal developmental quotient (DQ). Similarly, the visual reception and fine motor age equivalents were combined into a nonverbal DQ. Table 1 summarizes the participants’ demographic characteristics. For the longitudinal participants, their separate Mullen scores at 6 and 11 months are included. As a group, the HR and LR infants were matched on verbal, nonverbal, and total DQ, with no significant differences were found between the two groups for verbal, nonverbal, or total DQ scores at either age.
Stimuli
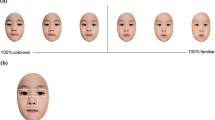
Stimuli were colored photographs of human faces that were approximately 12 × 19 degrees of visual angle. Each infant viewed six different faces. Because prior research on the LVF bias suggests that it is related to the processing of configural information, in order to maximize the infants attention to the internal configural features of the face, rather than show six different individuals, infants were shown a single person (a male) whose internal facial features and spatial distances were manipulated on each of the six trials by using a facial morphing program (see Gastgeb et al. 2011 for more information on stimulus design). The features and spatial distances that were manipulated included nose/mouth distance, nose width, forehead height, and lip thickness. Examples of the stimuli are illustrated in Fig. 1.

Stimulus Examples
Apparatus
Testing occurred in a quiet, dark laboratory room that simulated a small movie theater. Each infant was seated in a high chair in front of a large rear projection movie screen (69 × 91 cm). The infant’s guardian sat in a chair directly behind the infant and was instructed not to talk to or touch the infant during the testing. A stand-alone eye-tracker that required no attachments to the participants was positioned on a table in front of the infants. Stimuli were rear projected onto the screen using Tobii Studio software, and eye movements were recorded by a Tobii X120 stand-alone eye tracker at a sampling rate of 60 Hz, accuracy of 0.5 degrees of visual angle, spatial resolution of 0.2 degrees, and drift of 0.3 degrees. The eye-tracker sat 81 cm in front of the projection screen, and the infants were positioned approximately 162 cm from the screen. A Dell Dimension 9200 displayed experimental stimuli and recorded eye-movement and behavioral accuracy data. Eye-tracking data were processed using Tobii Studio software, Version 2.0.6.
Procedure
After the infants were placed in the high chair, a cartoon was played to attract their attention to the screen and to keep their attention. Once the infants were quiet and oriented, the cartoon was turned off and the eye-tracking calibration began. The calibration stimulus consisted of a drawing of a red rattle that shook and played an interesting sound. A live view of the infants’ eye movements allowed the experimenter to determine when the infants were looking at the rattle. Once the infants oriented to the rattle, a button was pressed that moved the rattle to a different position. Again, once the infants looked at the rattle, the rattle’s position was moved again. In total, calibration required the infants to accurately look at five different calibration positions.
Once an accurate calibration had occurred, infants were shown the six different faces for 5 s each. If any of the infants became fussy after viewing any of the faces, the face presentation was temporarily suspended and the cartoon was turned on until the infant was calm and oriented again to the screen whereupon the presentation of the face stimuli continued. As such, each infant merely viewed six different static faces while eye-tracking was recorded.
Data Reduction
The amount of time that the infants spent looking to the left or right was analyzed by creating regions of interest (ROIs) that included the entire right or left sides of the faces (see Fig. 2). The proportion of time the infant looked to the left side of the face was calculated by taking the amount of time the infant looked at the left averaged across all six face trials divided by the total amount of time the infants looked to both the left and the right, averaged across all six face trials. The amount of time spent looking at the eye or mouth regions was also analyzed. The eye ROI included the highest point of the eyebrow to the top of the orbital bone. The mouth ROI was a region starting half way between the bottom of the nose and the top of the mouth and ending an equal distance below the mouth. Proportion of time to the eye region was calculated by taking the amount of time looked at the eye region averaged across all six face trials over the total amount of time spent looking at both the eye and mouth regions averaged across all six face trials.

Example areas of interest (AOIs)
Results
Left Visual Field (LVF) Analyses
Of primary interest was whether the infants spent more time fixating on the the left side of the face or whether they distributed their attention equally to the two sides of the face; and, whether the amount of attention to the left varied based on either the age of the infants or their risk status. The proportion of time the infants spent looking to the left can be seen in Fig. 3. Because this was a mix of both cross-sectional and longitudinal participants, separate analyses were initially conducted on each age group. Beginning with the 6-month-old infants, a one-way ANOVA which included risk group (HR vs. LR) as a between factor was conducted on the proportion of time infants spent looking to the LVF. As seen in Fig. 3, the HR and LR groups were not different from each other (F(1,27) = .12, p = .74) and the proportion of time that both the HR infants (t(14) = .31, p = ns) and the LR infants (t(13) = .192, p = ns) spent looking to the LVF was not reliably different from change (.5).

Proportion of looking to LVF by risk and age (all infants)
In contrast to the results of the 6-month-olds, for the 11-month- old infants, the one-way ANOVA of the proportion of time infants spent looking at the LVF demonstrated a significant main effect for risk group (F(1,43) = 7.94, p = .007, η 2p = .156). As seen in Fig. 3, the 11-month-old LR infants spent significantly more than half of their face viewing time viewing the left side of the face (t(16) = 2.71, p = .02). In contrast, the HR infants did not look longer at the left than the right (t(27) = −1.06, p = ns).
In order to more directly test whether LR infants develop a LVF bias between 6 and 11 months of age that may not be seen in HR infants, a second set of analyses was conducted on only the infants for whom there was longitudinal data. For these infants, a two-way ANOVA was conducted on the proportion of time spent looking to the left. This ANOVA included risk group (HR vs. LR) as a between factor and age (6 vs. 11 months) as a within factor. While the main effect of risk group was not significant (F(1, 18) = 2.57, p = .126) there was a significant interaction between risk group and age (F(1,18) = 4.31, p = .05, η 2p = .193). As can be seen in Fig. 4, the only group that looked to the left side of the face significantly more than half of the time was the 11-month-old LR infant group (t(9) = 2.82, p = .02).

Proportion of looking to LVF by risk and age (longitudinal data)
Eye Versus Mouth Analyses
These analyses were aimed at examining the proportion of time infants spent fixating on the eye region as opposed to the mouth region. Results for both the 6 and 11-month-old infants are presented in Fig. 5. As with the LVF analyses, separate one-way ANOVAs were conducted on the 6- month and 11- month old infants. The dependent variable of these analyses was the proportion of time infants spent looking at the eyes and the between variable was risk group (HR vs. LR). Neither of these analyses yielded any significant results indicating that for both the 6-month-old infants (F(1,27) = .42, p = .52), and the 11-month-old infants (F(1,43) = .001, p = .65), the HR and LR infants looked at the eye region for a similar proportion of time.

Proportion of looking to eyes by risk and age (all infants)
Because the means suggested that both groups may have shown a decrease in the proportion of time that they spent looking at the eye region from 6 to 11 months of age, a separate ANOVA was again run on just the longitudinal sample. This two-way ANOVA of the proportion of looking to the eye region included age (6 vs. 11 months) as a within factor and risk group (HR vs. LR) as a between factor. This ANOVA yielded no significantly reliable results. Thus, the proportion of time spent looking at the eye region was not different between the two risk groups nor the two age groups and did not change over development.
Overall Looking and Habituation
Finally, analyses were conducted in order to determine whether the above results might have been impacted by overall differences in the amount of time infants spent looking at the faces or by potential habituation effects across the six stimuli. Infants total looking across the first three trials was compared to their total looking across the last three trials in order to determine whether there was any habituation of attention and whether this may have differed by risk group. Specifically, for each age group (6 and 11 months) a 2-way ANOVA was conducted that included risk group (HR vs LR) as a between factor and habituation (First vs Last three trials) as a within factor. The infant looking times are shown in Fig. 6. Results indicated regardless of risk group or age, infants did not decrease their looking or habituate from the first to the last three trials and that looking times did not differ between HR and LR infants.

Amount of time looking at the first vs last three trials (all infants)
Discussion
First, the results of this study clearly indicated that somewhere between 6 and 11 months of age, LR typically developing infants developed an LVF bias and spent more time fixating to the left side of the face. This result was demonstrated with respect to both the cross-sectional and longitudinal analyses. While the sample size of our 6- month-olds is slightly smaller than the 11-month olds, the means of the younger infants are very close to fifty percent or chance, indicating no LVF bias. Importantly, these results are similar to two prior eye-tracking studies with typically developing infants, one published (Guo et al. 2009) and one an unpublished thesis (Wheeler 2010), that have also reported that while infants younger than 6 months of age do not demonstrate a LVF bias, infants older than 9–11 months of age have an LVF bias for faces. Another very recent eye-tracking study (Liu et al. 2011) also found that infants have an LVF bias when viewing faces. However, because the data from infants between 4 and 9 months of age were combined, it is unknown when this effect emerged. Thus, the current study confirms the newly discovered phenomena that infants, similar to adults, have an LVF bias for faces, as defined by attending more to the left side of the face than the right. It also appears that this LVF bias emerges sometime after 6 months of age but before 11 months of age.
In contrast, the HR infants did not demonstrate an LVF bias at either 6 or 11 months of age. It is possible that the HR infants were merely demonstrating delayed development and that the LVF bias will emerge at a later age. However, based on the finding that adults with ASD do not show a LVF bias (Dundas et al. 2011) it is also possible that, as a group, the bias will not emerge in the HR infants and thus will reflect an endophenotypic marker related to the face processing differences seen in first degree relatives of individuals with ASD (Dawson et al. 2005; Pellicano 2008). Since the HR infants in the current study are not yet old enough to be differentially diagnosed with respect to an ASD, it is not known whether a lack of an LVF bias will be predictive of an ASD diagnosis.
Because the discovery of an LVF bias in typically developing infants is so new, it is not yet known why or how it emerges. It has been suggested that during the first year of life, the infants “face space” becomes both attuned and narrowed based on the faces the infant has encountered in his or her environment. Thus, just as speech perception becomes more attuned to the phonemic sounds used in the infant’s native environment, face perception becomes more attuned with respect to aspects of face perception such as gender, typicality, and race (McKone et al. 2009; Slater et al. 2010). While very speculative, the developing LVF bias may reflect this specialization in the sense that the ability to discriminate gender, race or typicality depends upon the developing ability to process subtle configural aspects of the face. As configural facial processing emerges and improves, infants may develop the LVF bias.
It is known that, in adults, the LVF bias is related to RH specialization for face processing (e.g., De Renzi et al. 1994; Yovel et al. 2008). It is also known that an LVF bias is related to the processing of configural facial information. For example, when inverted faces are viewed, configural processing is disrupted, lateralized activity in the RH is reduced (Yovel and Kanwisher 2005; Leehey et al. 1978; Levine et al. 1988) and the bias to the LVF is reduced (Luh 1998) or eliminated (Coolican et al. 2008). Therefore, it is possible that in infants, the emergence of the LVF bias reflects their early developing expertise with faces and ultimately their ability to process configural facial information. The emergence of the LVF bias may also reflect the beginning of RH specialization. As such, a lack of an LVF bias could be an early indicator of face processing difficulties.
Alternatively, it is also possible that early LVF bias for facial information is responsible for the right hemispheric specialization for faces. While some studies demonstrate that young children are showing right lateralized BOLD activation to faces (Cantlon et al. 2010), others suggest that these properties are not emerging until later in childhood and early adolescence (Aylward et al. 2005). One explanation could be that this leftward gaze bias is related to the sub-cortical face process system proposed by Johnson (2005) and its early presence is actually driving the right hemispheric specialization for processing faces. This implies that a disruption in this early processing bias could ultimately lead to face processing deficits.
In contrast to the LVF bias that was seen in only the LR infants, these results also indicated that there were no group differences with respect to the amount of time HR and LR spent attending to the eye or mouth regions of the face. This finding supports recent research indicating there do not seem to be general group differences between HR and LR infants in their distribution of attention to the eye versus the mouth regions (Merin et al. 2007) and that eye/mouth attention is not predictive of an ASD diagnosis (Young et al. 2009).
In summary, this is the first study that has looked at the LVF bias in infants at-risk for ASD. There are only two previously published studies on the LVF bias in typically developing infants making it a very new area of exploration. Yet, the findings of this study suggest that, unlike eye/mouth region differences, the LVF bias clearly distinguishes HR and LR infants. Hence, it may be an important marker for face processing deficits associated with ASD and a marker that might even be predictive of an ASD diagnosis. Further examining the emergence of this bias and how it relates to face processing could help our understanding of this valuable perceptual processing skill and the exact nature of the face processing deficits in seen in ASD.
References
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: American Psychiatric Association.
Aylward, E. H., Park, J. E., Field, K. M., Parson, A. C., Richards, T. L., Cramer, S. C., et al. (2005). Brain activation during face perception: evidence of a developmental change. Journal of Cognition and Neuroscience, 17, 308–319.
Behrmann, M., Avidan, G., Leonard, G. L., Kimchi, R., Luna, B., Humphreys, K., et al. (2006). Configural processing in autism and its relationship to face processing. Neuropsychologia, 44, 110–129.
Best, C. A., Minshew, N. J., & Strauss, M. S. (2010). Gender discrimination of eyes and mouths by individuals with autism. Autism Research, 3, 88–93.
Best, C. A., & Strauss, M. S. (2007, April). A face in the crowd: Recognition memory for distinctive faces in infancy. Paper presented at the biennial meeting of the Society for Research in Child Development, Boston, MA.
Boeschoten, M. A., Kenemans, J. L., van Engeland, H., & Kemner, C. (2007). Abnormal spatial frequency processing in high-functioning children with pervasive developmental disorder (PDD). Clinical Neurophysiology, 118, 2076–2088.
Butler, S., Gilchrist, I. D., Burt, D. M., Perrett, D. I., Jones, E., & Harvey, M. (2005). Are the perceptual biases found in chimeric face processing reflected in eye-movement patterns? Neuropsychologia, 43, 52–59.
Butler, S., & Harvey, M. (2006). Perceptual biases in chimeric face processing: Eye-movement patterns cannot explain it all. Brain Research, 1124, 96–99.
Cantlon, J. F., Pinel, P., Dehaene, S., & Pelphrey, K. A. (2010). Cortical representations of symbols, objects, and faces are pruned back during early childhood. Cerebral Cortex, 21, 191–199.
Celani, G., Battacchi, M. W., & Arcidiacono, L. (1999). The understanding of the emotional meaning of facial expressions in people with autism. Journal of Autism and Developmental Disorders, 29, 57–66.
Chawarska, K., Volkmar, F., & Klin, A. (2010). Limited attentional bias for faces in toddlers with autism spectrum disorders. Archives of General Psychiatry, 67, 178–185.
Coolican, J., Eskes, G. A., McMullen, P. A., & Lecky, E. (2008). Perceptual biases in processing facial identity and emotion. Brain and Cognition, 66, 176–187.
Corden, B., Chilvers, R., & Skuse, D. (2008). Avoidance of emotionally arousing stimuli predicts social–perceptual impairment in Asperger’s syndrome. Neuropsychologia, 46, 137–147.
Curby, K., Willenbockel, V., Tanaka, J., & Schultz, R. (2010). Face processing in autism: Insights from the perceptual expertise framework. In I. Gauthier, M. Tarr, & D. Bub (Eds.), Perceptual expertise: Bridging brain and behavior. New York: Oxford University Press.
Dawson, G., Webb, S. J., Wijsman, E., Schellenberg, G., Estes, A., Munson, J., et al. (2005). Neurocognitive and electrophysiological evidence of altered face processing in parents of children with autism: Implications for a model of abnormal development of social brain circuitry in autism. Development and Psychopathology, 17, 679–697.
de Haan, M., Johnson, M. H., Maurer, D., & Perrett, D. I. (2001). Recognition of individual faces and average face prototypes by 1- and 3- month old infants. Cognitive Development, 16, 659–678.
De Renzi, E., Perani, D., Carlesimo, G. A., Silveri, M. C., & Fazio, F. (1994). Prosopagnosia can be associated with damage confined to the right hemisphere- an MRI and PET study and a review of literature. Neuropsychologia, 32, 893–902.
Deruelle, C., Rondan, C., Gepner, B., & Tardif, C. (2004). Spatial frequency and face processing in children with autism and Asperger syndrome. Journal of Autism and Developmental Disorders, 34, 199–210.
Elsabbagh, M., & Johnson, M. H. (2010). Getting answers from babies about autism. Trends in Cognitive Sciences, 14, 81–87.
Fletcher-Watson, S., Leekam, S. R., Benson, V., Frank, M. C., & Findlay, J. M. (2009). eye-movements reveal attention to social information in autism spectrum disorder. Neuropsychologia, 47, 248–257.
Gastgeb, H. Z., Rump, K. M., Best, C. A., Minshew, N. J., & Strauss, M. S. (2009). Prototype formation in autism: can individuals with autism abstract facial prototypes? Autism Research, 2, 279–284.
Gastgeb, H. Z., Wilkinson, D. A., Minshew, N. J., & Strauss, M. S. (2011). Can individuals with autism abstract prototypes of natural faces? Journal of Autism and Developmental Disorders, 41(12), 1609–1618.
Guo, K., Meints, K., Hall, C., Hall, S., & Mills, D. (2009). Left gaze bias in humans, rhesus monkeys and domestic dogs. Animal Cognition, 12, 409–418.
Haxby, J. V., Hoffman, E. A., & Gobbini, M. I. (2000). The distributed human neural system for face perception. Trends in Cognitive Sciences, 4, 223–233.
Hernandez, N., Metzger, A., Magne, R., Bonnet-Brilhault, F., Roux, S., Barthelemy, C., et al. (2009). Exploration of core features of a human face by healthy and autistic adults analyzed by visual scanning. Neuropsychologia, 47, 1004–1012.
Humphreys, K. (2003). The development of face-space: An exploration. Unpublished doctoral dissertation, University of London, London, England.
Johnson, M. H. (2005). Sub-cortical face processing. Nature Reviews Neuroscience, 6, 766–774.
Kelly, D. J., Quinn, P. C., Slater, A. M., Lee, K., Ge, L., & Pascalis, O. (2007). The other-race effect develops during infancy: Evidence of perceptual narrowing. Psychological Science, 18, 1084–1089.
Klin, A., Sparrow, S. S., de Bildt, A., Cicchetti, D. V., Cohen, D. J., & Volkmar, F. (1999). A normed study of face recognition in autism and related disorders. Journal of Autism and Developmental Disorders, 29, 499–508.
Lahaie, A., Mottron, L., Arguin, M., Berthiaume, C., Jemel, B., & Saumier, D. (2006). Face perception in high-functioning autistic adults: Evidence for superior processing of face parts, not for a configural face-processing deficit. Neuropsychology, 20, 30–41.
Leehey, S. C., Carey, S., Diamond, R., & Cahn, A. (1978). Upright and inverted faces: The right hemisphere knows the difference. Cortex, 14, 411–419.
Levine, S. C., Banich, M. T., & Koch-Weser, M. P. (1988). Face recognition: A general or specific right hemisphere capacity? Brain and Cognition, 8, 303–325.
Liu, S., Quinn, P. C., Wheeler, A., Xiao, N., Ge, L., & Lee, K. (2011). Similarity and difference in the processing of same- and other-race faces as revealed by eye tracking in 4- to 9-month-olds. Journal of Experimental Child Psychology, 108, 180–189.
Lord, C., Risi, S., Lambrecht, L., Cook, E. H., Leventhal, B. L., DiLavore, P. C., et al. (2000). The autism diagnostic observation schedule-generic: A standard measure of social and communication deficits associated with the spectrum of autism. Journal of Autism and Developmental Disorders, 30(3), 205–223.
Lord, C., Rutter, M., & Le Couteur, A. (1994). Autism diagnostic interview-revised: A revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. Journal of Autism and Developmental Disorders, 24, 659–695.
Luh, K. E. (1998). Effect of inversion on perceptual biases for chimeric faces. Brain and Cognition, 37(1), 105–108.
Luyster, R. J., Wagner, J. B., Vogel-Farley, V., Tager-Flusberg, H., & Nelson III, C. A. (2011). Neural correlates of familiar and unfamiliar face processing in infants at risk for autism spectrum disorders. Brain Topography, 24, 220–228.
McCleery, J. P., Akshoomoff, N., Dobkins, K. R., & Carver, L. J. (2009). Atypical face versus object processing and hemispheric asymmetries in 10-month-old infants at risk for autism. Biological Psychiatry, 66, 950–957.
McKone, E., Crookes, K., & Kanwisher, N. (2009). The cognitive and neural development of face recognition in humans. In M. S. Gazzaniga (Ed.), The cognitive neurosciences IV (pp. 467–482). Cambrige, MA: Bradford Books.
Merin, N., Young, G. S., Ozonoff, S., & Rogers, S. J. (2007). Visual fixation patterns during reciprocal social interaction distinguish a subgroup of 6-month-old infants at-risk for autism from comparison infants.
Mondloch, C. J., Le Grand, R., & Maurer, D. (2002). Configural face processing develops more slowly than featural face processing. Perception, 31, 553–566.
Mullen, E. M. (1995). Mullen scales of early learning. Circle Pines, MN: American Guidance Service.
Neumann, D., Spezio, M. L., Piven, J., & Adolphs, R. (2006). Looking you in the mouth: Abnormal gaze in autism resulting from impaired top-down modulation of visual attention. Social Cognitive and Affective Neuroscience, 1, 194–202.
Newell, L. C., Best, C. A., Gastgeb, H., Rump, K. A., & Strauss, M. S. (2010). The development of categorization and facial knowledge: Implications for the study of autism. In L. M. Oakes, C. H. Cashon, M. Casasola, & D. H. Rakison (Eds.), The information-processing infant. New York: Oxford University Press.
Norbury, C. F., Brock, J., Cragg, L., Einav, S., Griffiths, H., & Nation, K. (2009). Eye-movement patterns are associated with communicative competence in autistic spectrum disorders. The Journal of Childhood Psychology and Psychiatry, 50, 834–842.
O’Toole, A. J., Deffenbacher, K. A., Valentine, K., McKee, K., Huff, D., & Abdi, H. (1998). The perception of face gender: The role of stimulus structure in recognition and classification. Memory and Cognition, 26, 146–160.
Ozonoff, S., Young, G. S., Carter, A., Messinger, D., Yirmiya, N., Zwaigenbaum, L.,… Stone, W. L. (2011). Recurrence risk for autism spectrum disorders: A baby siblings research consortium study. Pediatrics. 2010–2825.
Pascalis, O., & Kelly, D. J. (2009). The origins of face processing in humans: Phylogeny and ontogeny. Psychological Science, 4, 200–209.
Pellicano, E. (2008). Autism: Face-processing clues to inheritance. [Comment]. Current Biology, 18, R748–R750.
Quinn, P. C., Kelly, D. J., Lee, K., Pascalis, O., & Slater, A. M. (2008). Preference for attractive faces in human infants extends beyond conspecifics. Developmental Science, 11, 76–83.
Quinn, P. C., Yahr, J., Kuhn, A., Slater, A. M., & Pascalils, O. (2002). Representation of the gender of human faces by infants: A preference for female. Perception, 31, 1109–1121.
Rhodes, G., Brennan, S., & Carey, S. (1987). Identification and ratings of caricatures: Implications for mental representations of faces. Cognitive Psychology, 19, 473–497.
Rogers, S. J. (2009). What are infant siblings teaching us about autism in infancy? Autism Research, 2, 125–137.
Rubenstein, A. J., Kalakanis, L., & Langlois, J. H. (1999). Face perception in high-functioning autistic adults: Evidence for superior processing of face parts, not for a configural face-processing deficit. Neuropsychology, 20, 30–41.
Rump, K. M., Giovannelli, J. L., Minshew, N. J., & Strauss, M. S. (2009). The development of emotion recognition in individuals with autism. Child Development, 80, 1434–1447.
Scherf, K. S., Behrmann, M., Kimchi, R., & Luna, B. (2009). Emergence of global shape processing continues through adolescence. Child Development, 80, 162–177.
Slater, A., Quinn, P. C., Kelly, D. J., Lee, K., Longmore, C. A., McDonald, P. R., et al. (2010). The shaping of the face space in early infancy: Becoming a native face processor. Child development perspectives, 4, 205–211.
Spezio, M. L., Adolphs, R., Hurley, R. S. E., & Piven, J. (2006). Abnormal use of facial information in high-functioning autism. Journal of Autism and Developmental Disorders, 37, 929–939.
Strauss, M. S. (1979). Abstraction of prototypical information by adults and 10-month-old infants. Journal of Experimental Psychology. Human Learning and Memory, 5, 618–632.
Tager-Flusberg, H. (2010). The origins of social impairments in autism spectrum disorder: Studies of infants at risk. Neural Networks, 23, 1072–1076.
Valentine, T. (1991). A unified account of the effects of distinctiveness, inversion, and race in face recognition. The Quarterly Journal of Experimental Psychology, 43, 161–204.
van der Geest, J. N., Kemner, C., Verbaten, M. N., & van Engeland, H. (2001). Eye movements, visual attention, and autism: A saccadic reaction time study using the gap and overlap paradigm. Biological Psychiatry, 50, 614–619.
Vlamings, P. H., Jonkman, L. M., van Daalen, E., van der Gaag, R. J., & Kemner, C. (2010). Basic abnormalities in visual processing affect face processing at an early age in autism spectrum disorder. Biological Psychiatry, 68, 1107–1113.
Webb, S. J., Dawson, G., Bernier, R., & Panagiotides, H. (2006). ERP evidence of atypical face processing in young children with autism. Journal of Autism and Developmental Disorders, 36, 881–890.
Wheeler, A. (2010). The emergence of a left visual field bias in infants’ processing of dynamic faces. Master of Arts: University of Toronto, Toronto.
Wolff, W. (1933). The experimental study of forms of expression. Character & Personality, 2, 168–176.
Dundas, E. M., Best, C. A., Minshew, N. J., & Strauss, M. S. (2011). A lack of left visual field bias when individuals with autism process faces. Journal of Autism and Developmental Disorders. doi:10.1007/s10803-011-1354-2
Young, G. S., Merin, N., Rogers, S. J., & Ozonoff, S. (2009). Gaze behavior and affect at 6 months: Predicting clinical outcomes and language development in typically developing infants and infants at risk for autism. Developmental Science, 12, 798–814.
Yovel, G., & Kanwisher, N. (2005). The neural basis of the behavioral face-inversion effect. Current Biology, 15, 2256–2262.
Yovel, G., Tambini, A., & Bradman, T. (2008). The asymmetry of the fusiform face area is a stable individual characteristic that underlies the left-visual-field superiority for faces. Neuropsychologia, 46, 3061–3068.
Acknowledgments
This research was supported by a grant from the National Institutes of Health. The authors would like to thank Kao-Wei Chua and Sara Green for their help with testing and data handling.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dundas, E., Gastgeb, H. & Strauss, M.S. Left Visual Field Biases when Infants Process Faces: A Comparison of Infants at High- and Low-Risk for Autism Spectrum Disorder. J Autism Dev Disord 42, 2659–2668 (2012). https://doi.org/10.1007/s10803-012-1523-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10803-012-1523-y