
Abstract
Fractional flow reserve (FFR) is an index for identifying functionally significant stenotic lesions. A FFR value of ≤0.75 is considered clinically significant and indicative of physiological ischemia. Focal lesions with 30–80 % stenosis by angiography with lesion lengths of less than 20 mm were selected from left anterior descending arteries of 74 patients. The analysis for the total lesion was processed first, and then each lesion was divided into three segments to assess the each segment. Data on plaque geometry and composition of two FFR groups, FFR ≤ 0.75 and FFR > 0.75, were compared by total and segmental analysis. Lesions with FFR ≤ 0.75 had more fibrofatty tissue (13.5 ± 7.4 vs. 10.2 ± 6.5 %, p = 0.05) and less dense calcium (7.2 ± 5.3 vs. 11.9 ± 7.5 %, p = 0.01) compared to lesions with FFR > 0.75. The content of necrotic core in mid segments was higher compared to proximal and distal segments (22.9 ± 10.6, 20.2 ± 10.9, 17.1 ± 11.2 %, respectively, p = 0.032) in lesions with FFR > 0.75 but the difference was less obvious in lesions with FFR ≤ 0.75 (17.9 ± 9.9, 18.7 ± 9.9, 15.8 ± 9.0 %, respectively, p = 0.533). Coronary lesions with FFR > 0.75 have larger content of dense calcium and slightly less fibrofatty tissue compared to lesions with FFR ≤ 0.75. While segmental plaque compositions for each segment show noticeable variations in lesions with FFR > 0.75 such as high concentrations of necrotic core in mid segment, these differences in each segment become obscure in FFR ≤ 0.75 and are evenly distributed across the lesion.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
While the physiological significance of coronary artery stenosis can be assessed using fractional flow reserve (FFR), coronary plaques at high risk of rupture and clinical events can be identified by virtual histology intravascular ultrasound (VH-IVUS) as plaques with high amounts of necrotic core abutting the lumen. The FIRST trial was performed to assess the correlation between FFR, IVUS and VH-IVUS for intermediate coronary lesions, and showed that anatomic measurements using IVUS such as the minimum lumen area (MLA) correlates well with FFR, however plaque morphological characteristics did not [1]. Plaque ruptures occur not only in patients with acute coronary syndrome (ACS) but also in non-ACS cases and in asymptomatic patients, and this implies that not all plaque ruptures result in acute events [2]. Therefore, assessment of plaque composition at non-MLA sites is just as important as MLA sites. Brugaletta et al. [3] studied the geometry and composition of lesions with FFR ≤ 0.80 and found that they did not differ in composition to lesions with FFR > 0.80, despite the FFR ≤ 0.80 lesions having larger plaque size. Thus, the correlation between FFR and plaque composition still remains uncertain and a different approach is required to clarify this relationship by focusing on segmentalized lesion as well as the whole atherosclerotic lesion. Therefore, the objectives of this study were to compare geometry and composition findings with FFR and to assess its relationship by investigating plaque morphology and composition through both total and segmental analyses of coronary artery lesions.
Methods
Patient population
Between June 2011 and August 2014, 74 moderate coronary lesions from 74 patients were assessed with quantitative coronary angiography (QCA), IVUS, VH-IVUS and FFR for functional, morphological and compositional lesion characteristics. All patients presenting with angina excluding ST-segment elevation myocardial infarction (STEMI) were examined. The visual assessment of diameter stenosis (DS) from the angiograms was conducted for the classification. Both culprit and non-culprit lesions were examined and only left anterior descending (LAD) lesions with a DS less than 80 % were included in the study. Focal lesions not exceeding a lesion length of 20 mm from LAD artery were selected for inclusion. Exclusion criteria was a left ventricular ejection fraction <30 %, acute myocardial infarction, left main disease, chronic total occluded lesions, heavily calcified or thrombotic lesions, life expectancy <1 year and known chronic kidney disease (creatinine > 2 mg/dL). This study was carried out according to the Declaration of Helsinki guidelines and was approved by the Institutional Review Board ethics committee at Ulsan University Hospital. All enrolled patients provided written informed consent.
QCA analysis
Two-dimensional QCA was performed using dedicated software packages (CASS 5.9; Pie Medical Imaging, Maastricht, Netherlands). The reference vessel diameter (RVD), minimum lumen diameter (MLD), DS and lesion length (LL) were measured by an experienced, independent investigator who was blinded to the FFR, VH-IVUS and clinical data.
IVUS and VH-IVUS
IVUS images were recorded using a 2.9F Eagle Eye catheter (Volcano Corp., Rancho Cordova, California) and incorporated a 20-MHz phased-array transducer. The catheter was pulled back with an automated pullback system at 0.5 mm/s. All measurements were performed after the administration of 200 µg intracoronary nitroglycerin. Geometric quantitative IVUS analyses were performed according to criteria from the IVUS clinical expert consensus document [4]. VH-IVUS images were analyzed using pcVH 2.2 software (Volcano Therapeutics, Rancho Cordova, California, USA) by another independent investigator who was blinded to the clinical characteristics of the participants. Volumetric VH-IVUS data of the geometric and compositional data were automatically generated for the analyzed segment based on the application of the trapezium method to the cross-sectional area [5]. Four tissue components—fibrous tissue (FT), fibrofatty tissue (FF), necrotic core (NC) and dense calcium (DC) were identified from VH-IVUS and both mean area and the relative volume of each component were calculated. Lesions were classified into pathological intimal thickening (PIT; intimal thickening ≥600 µm for >20 % of the circumference with >15 % FF and no confluent NC or DC), fibrotic plaque (FI; consisting of FT without confluent NC or DC), fibrocalcific plaque (FC; DC > 10 % without confluent NC), fibroatheroma (FA; NC > 10 % with a layer of fibrous tissue), calcified fibroatheroma (CaFA; FA with DC > 10 %), thin-cap fibroatheroma (TCFA; NC > 10 % in direct contact with the lumen), or calcified thin-cap fibroatheroma (CaTCFA; TCFA with DC > 10 %) [6] by two experienced, independent investigators.
FFR measurement
The FFR measurements were done according to current guidelines [7]. After the administration of nitroglycerin, a 0.014 inch pressure monitoring guidewire (PressureWire Certus, St. Jude Medical, Uppsala, Sweden) through a 6F or 7F guiding catheter was advanced past the lesion far distally. Maximal hyperemia was induced by administering intravenous adenosine (140 µg/kg/min) or intracoronary nicorandil (2 mg) [8]. The FFR was calculated by dividing the mean distal coronary pressure by the mean aortic pressure during hyperemia. Normally, FFR measurements are obtained just distal (2–3 cm) to the lesion but in this study, the FFR was measured far distal to the lesion for the detection of a true ischemic lesion. It has been shown that the median gradient between proximal measurement and distal measurement is 0.06 [9]. The cutoff value of FFR used for the current analysis was 0.75.
Segment selection
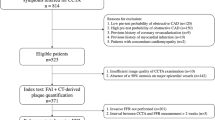
Each lesion was divided into three segments as shown in Fig. 1. The black dotted lines correspond to PB of 40 % and the red dotted lines LA index of 0.3. The length of each segment can vary based on the lesion characteristics such as the location of the most stenotic part. The lumen area (LA) index is calculated by dividing the lesion LA with reference LA and the reference LA is a mean value of the proximal LA and distal LA. A LA index of 0.3 was a criterion to identify the mid segment. Lesions were selected when the plaque burden (PB) was above 40 %. The cross-sectional areas of both ends of mid segment represent the same LA index.

Definition of each segment a for a typical lesion and for the lesions when the most stenotic part is b in the more proximal portion or c in the more distal portion. P proximal segment, M mid segment, D distal segment, LA lumen area, PB plaque burden
Statistical analysis
All statistical analyses were performed using SPSS version 21.0 (SPSS Inc, Chicago, IL, USA). Continuous variables are presented as mean ± SD and categorical variables as frequency and percentage. Analysis of discrete variables was performed using Chi square or Fisher’s exact test. The normal distribution of continuous variables was explored by Shapiro–Wilk test and comparison between groups was done by non-parametric tests such as Man–Whitney U and Kruskal–Wallis H test. The relationship and variability between the variables were analyzed by Pearson correlation analysis and receiver operating characteristic (ROC) was used to determine the predictive parameter. A p value of <0.05 was considered statistically significant.
Results
Patient demographics and lesion characteristics
Seventy-four consecutive patients were enrolled in this study. Table 1 shows their clinical characteristics and FFR values. The mean age of participants was 57.8 ± 9.5 years old and 73 % (54 of 74) were male. All lesions were located in LAD and 44.6 % (33 of 74) underwent percutaneous coronary intervention (PCI). For patients with unstable angina (47.3 %, 35 of 74) and NSTEMI (5.4 %, 4 of 74), the cardiac enzymes were examined and elective PCI was performed accordingly. Among lesions with a FFR ≤ 0.75, 75 % (15 of 20) were treated with DES and 15 % (3 of 20) were treated with DEB, while 10 % (2 of 20) had a FFR value of 0.74, receiving no PCI. 72.2 % (39 of 54) of lesions with a FFR of >0.75 did not receive PCI however the remaining 27.8 % (15 of 54) received PCI for the following reasons; the lesion MLA by IVUS was <4 mm2 in nine patients and the FFR was less than 0.80 in eight patients. Mean FFR was 0.66 ± 0.06 in the FFR ≤ 0.75 group and 0.84 ± 0.06 in the FFR > 0.75 group.
QCA and IVUS findings
The QCA results and IVUS geometric parameters are listed in Table 2. Smaller MLD (1.13 ± 0.33 vs. 1.49 ± 0.38 mm, p < 0.001) and higher DS (56.0 ± 13.5 vs. 47.1 ± 12.3 %, p = 0.021) from QCA, and smaller MLA (2.99 ± 0.51 vs. 3.93 ± 0.81 mm2, p < 0.001) from IVUS were found in lesions with FFR ≤ 0.75. PB calculated from each slice of IVUS images was higher at the lesions with FFR ≤ 0.75 compared to lesions with FFR > 0.75 (66.3 ± 9.2 vs. 61.2 ± 8.4, p = 0.028). For PA, VA and LA, the pcVH software program provided the volumetric data of the lesion and we divided each volume with the corresponding lesion length to obtain the mean area of each value. We first analyzed the whole lesion and then the subdivided segments by LA index were processed separately in the same manner.
To determine the relationship between FFR and MLA, a ROC curve analysis was performed along with a scatterplot as shown in Fig. 2. The best cutoff value of MLA to predict a FFR ≤ 0.75 was 3.21 mm2 (AUC = 0.843). The diagnostic performance of the MLA cutoff value of 3.21 mm2 to identify hemodynamically significant stenosis (FFR ≤ 0.75) revealed that the accuracy, sensitivity, specificity, positive predictive value, and negative predictive value were 75.7, 80.0, 74.1, 53.3, 90.9 %, respectively. FFR moderately correlated with MLA (r = 0.517, p < 0.001) and showed negative correlation with DS (r = −0.405, p < 0.001) and PB (r = −0.270, p = 0.020).

a ROC analysis and b scatterplot of MLA and FFR. FFR fractional flow reserve, MLA minimum lumen area, ROC receiver operating characteristics
VH-IVUS findings
Table 3 shows the plaque composition and phenotypes from VH-IVUS analyses. The results showed slightly more FF (13.5 ± 7.4 vs. 10.2 ± 6.5 %, p = 0.05) and less DC (7.2 ± 5.3 % vs. 11.9 ± 7.5 %, p = 0.01) in lesions with FFR ≤ 0.75. Plaques were classified as one of the seven phenotypes; 1 PIT, 1 FI, 2 FC, 17 FA, 19 CaFA, 3 TCFA and 31 CaTCFA. In lesions with FFR ≤ 0.75, FA and CaTCFA were major phenotypes and they were 35 % (7 of 20) each. In lesions with FFR > 0.75, CaTCFA had the highest population (44.4 %, 24 of 54) followed by CaFA (27.8 %, 15 of 54). A ROC analysis was also performed for TCFA or CaTCFA and no TCFA or CaTCFA to identify the relationship between MLA and. FFR, and the AUC values were 0.834 and 0.845, respectively.
Segmental analysis
To evaluate the segmental plaque morphology and composition, the three segments in each lesion (proximal, mid and distal) were studied individually for each FFR group. Table 4 shows the segmental characteristics for each FFR group. The length of each segment depends on the plaque morphology as shown in Fig. 1 which was defined by PB and LA index. For the plaque classification, each segment was considered separately and we evaluated the types only with the information on that segment. The IVUS lesion length of the mid-segment was longer than proximal and distal segments in both groups. In the FFR ≤ 0.75 group, the mean PB, LA and MLA of mid-segments were 63.0 ± 7.1 %, 4.96 ± 1.94 and 2.99 ± 0.51 mm2, respectively, and were significantly different compared to the proximal and distal segments. In the FFR > 0.75 group, similar anatomic characteristics were seen in each segment for PB, LA and MLA. NC percent were higher in mid-segments compared to proximal and distal segments (22.9 ± 10.6, 20.2 ± 10.9 and 17.1 ± 11.2 %, respectively, p = 0.032).
Plaque classifications for each FFR group are shown in Table 5. In the FFR ≤ 0.75 group, the majority of plaque was FA; 50 % (10 of 20) in proximal, 40 % (8 of 20) in mid and 50 % (10 of 20) in distal segments respectively. TCFA or CaTCFA was not seen in distal segments in lesions with FFR ≤ 0.75. In the FFR > 0.75 group, more CaTCFA were seen; 38.9 % (21 of 54) in mid, 27.8 % (15 of 54) in proximal and 11.1 % (6 of 54) in distal segments, respectively.
Discussion
The major findings of this analysis include: (1) anatomic parameters such as DS, MLA and PB showed correlation with FFR, (2) coronary lesions with FFR more than 0.75 have larger content of DC and less FF tissue compared to lesions with FFR ≤ 0.75, (3) in the segmental analysis, more NC were found in mid segments of lesions with FFR > 0.75, and (4) NC-rich plaques such as TCFA or CaTCFA were identified more in lesions with FFR > 0.75.
Since plaque characteristics are best described by the plaques in mid segment, segmental analysis was also performed to obtain better insight. Overall plaque morphology of two FFR groups using IVUS showed no significant differences except for MLA, however, segmental analysis showed the dominant findings seen in the mid segments. As seen in previous studies, the best cutoff value of MLA ranges from 3.0 to 4.0 mm2 [1, 10, 11], and the present study showed that a MLA of 3.21 mm2 can be used as an index of identifying lesions with a FFR of ≤0.75. The optimal cutoff for an MLA is vessel dependent and our study focused on LAD lesions only with an average RVD of 2.78 mm. PB showed moderate correlation with FFR (r = −0.270, p = 0.020) and its higher concentration in mid segment was observed on the segmental analysis.
In a previous study, plaques from lesions with FFR ≤ 0.80 exhibited higher FF tissue content (p = 0.02) than those lesions with FFR > 0.80 and in addition, the relative content of NC was slightly higher (p = 0.08) in lesions with FFR > 0.80 [3]. Similarly, our analysis revealed that plaques from lesions with FFR ≤ 0.75 showed higher FF (p = 0.05), lower NC (p = 0.21), and lower DC (p = 0.01) compared to FFR > 0.75. These results suggest a possible explanation of major adverse cardiac events (MACE) in patients with angiographically intermediate lesions when these lesions are left untreated as no functionally significant ischemia was found.
On segmental analysis, NC concentration in mid segments was higher (p = 0.032) than other segments in FFR > 0.75 group. High concentration of NC in mid segments in the FFR > 0.75 group could be considered a marker of plaque vulnerability. The results also indicate that each plaque composition tends to distribute evenly along the lesion when FFR becomes low. The association of NC concentration and cardiac events has received a lot of attention in VH-IVUS research. Atherosclerotic plaques related to ACS often occur with mild stenosis and lesions associated with this recurrent event were TCFA or were characterized by a large PB, small LA or some combination of these characteristics. The PROSPECT trial showed 11.6 % of patients experienced major adverse cardiovascular events in 3-years follow-up at the site of nonculprit lesions [12].
On phenotype comparison, TCFA and CaTCFA were found more in the FFR > 0.75 group compared to the FFR ≤ 0.75 group and these NC-rich plaques may cause plaque rupture. The segmental analysis also revealed that TCFA or CaTCFA were present in all three segments in the FFR > 0.75 group but they were absent in distal segments with less seen in proximal and mid segments in the FFR ≤ 0.75 group, showing the higher possibility of plaque rupture with a higher FFR. More plaque rupture prone characteristics for lesions with FFR > 0.75 compared to lesions with FFR ≤ 0.75 support the previous findings of the PROSPECT trial and indicates the sinister role of TCFA in lesions with FFR > 0.75. Lesions without CaTCFA or TCFA had better correlation with FFR compared to lesions with CaTCFA or TCFA. Long term clinical follow-up is required to ascertain the findings from the present study.
Limitations
This is a registry study and included a small number of patients. The purpose of this study was to compare two FFR groups for plaque characteristics and did not include clinical outcomes. Hence, further clinical studies are required to evaluate the clinical outcomes and correlation between FFR and VH-IVUS. Another limitation of VH-IVUS for the assessment of plaque composition is that VH-IVUS might overestimate NC content in the presence of high attenuation objects such as dense calcifications [13, 14]. However, VH-derived TCFA is a qualitative index defined by confluent NC in direct contact with the lumen, the overestimation of NC may not affect the identification of TCFA.
Conclusions
Coronary lesions with FFR > 0.75 have larger content of dense calcium and less fibrofatty tissue compared to lesions with FFR ≤ 0.75. While segmental plaque compositions for each segment show noticeable variations in lesions with FFR > 0.75 such as high concentrations of necrotic core in mid segment, these differences in each segment become obscure in FFR ≤ 0.75 and are evenly distributed across the lesion.
Abbreviations
- ACS:
-
Acute coronary syndrome
- CaFA:
-
Calcified fibroatheroma
- CaTCFA:
-
Calcified thin-cap fibroatheroma
- DC:
-
Dense calcium
- DS:
-
Diameter stenosis
- FA:
-
Fibroatheroma
- FF:
-
Fibrofatty tissue
- FFR:
-
Fractional flow reserve
- FC:
-
Fibrocalcific plaque
- FI:
-
Fibrotic plaque
- FT:
-
Fibrous tissue
- LA:
-
Lumen area
- LAD:
-
Left anterior descending
- LL:
-
Lesion length
- MACE:
-
Major adverse cardiac events
- MLA:
-
Minimum lumen area
- MLD:
-
Minimum lumen diameter
- NC:
-
Necrotic core
- PCI:
-
Percutaneous coronary intervention
- PIT:
-
Pathological intimal thicknening
- QCA:
-
Quantitative coronary angiography
- ROC:
-
Receiver operating characteristic
- RVD:
-
Reference vessel diameter
- TCFA:
-
Thin-cap fibroatheroma
- VH-IVUS:
-
Virtual histology intravascular ultrasound
References
Waksman R, Legutko J, Singh J et al (2013) FIRST: Fractional Flow Reserve and Intravascular Ultrasound Relationship Study. J Am Coll Cardiol 61:917–923. doi:10.1016/j.jacc.2012.12.012
Maehara A, Mintz GS, Bui AB et al (2002) Morphologic and angiographic features of coronary plaque rupture detected by intravascular ultrasound. J Am Coll Cardiol 40:904–910
Brugaletta S, Garcia-Garcia HM, Shen ZJ et al (2012) Morphology of coronary artery lesions assessed by virtual histology intravascular ultrasound tissue characterization and fractional flow reserve. Int J Cardiovasc Imaging 28:221–228. doi:10.1007/s10554-011-9816-3
Mintz GS, Nissen SE, Anderson WD et al (2001) American College of Cardiology clinical expert consensus document on standards for acquisition, measurement and reporting of intravascular ultrasound studies (ivus): A report of the american college of cardiology task force on clinical expert consensus documents developed in collaboration with the european society of cardiology endorsed by the society of cardiac angiography and interventions. J Am Coll Cardiol 37:1478–1492. doi:10.1016/S0735-1097(01)01175-5
Huisman J, Egede R, Rdzanek A et al (2010) Between-centre reproducibility of volumetric intravascular ultrasound radiofrequency-based analyses in mild-to-moderate coronary atherosclerosis: an international multicentre study. EuroIntervention 5:925–931
Garcia-Garcia HM, Mintz GS, Lerman A et al (2009) Tissue characterisation using intravascular radiofrequency data analysis: recommendations for acquisition, analysis, interpretation and reporting. EuroIntervention 5:177–189
Pijls NH, De Bruyne B, Peels K et al (1996) Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. The New England journal of medicine 334:1703–1708. doi:10.1056/nejm199606273342604
Jang HJ, Koo BK, Lee HS et al (2013) Safety and efficacy of a novel hyperaemic agent, intracoronary nicorandil, for invasive physiological assessments in the cardiac catheterization laboratory. Eur Heart J 34:2055–2062. doi:10.1093/eurheartj/eht040
Rodes-Cabau J, Gutierrez M, Courtis J et al (2011) Importance of diffuse atherosclerosis in the functional evaluation of coronary stenosis in the proximal-mid segment of a coronary artery by myocardial fractional flow reserve measurements. Am J Cardiol 108:483–490. doi:10.1016/j.amjcard.2011.03.073
Abizaid AS, Mintz GS, Mehran R et al (1999) Long-term follow-up after percutaneous transluminal coronary angioplasty was not performed based on intravascular ultrasound findings: importance of lumen dimensions. Circulation 100:256–261
Koo BK, Yang HM, Doh JH et al (2011) Optimal intravascular ultrasound criteria and their accuracy for defining the functional significance of intermediate coronary stenoses of different locations. JACC Cardiovascular interventions 4:803–811. doi:10.1016/j.jcin.2011.03.013
Stone GW, Maehara A, Lansky AJ et al (2011) A prospective natural-history study of coronary atherosclerosis. The New England journal of medicine 364:226–235. doi:10.1056/NEJMoa1002358
Pu J, Mintz GS, Brilakis ES et al (2012) In vivo characterization of coronary plaques: novel findings from comparing greyscale and virtual histology intravascular ultrasound and near-infrared spectroscopy. Eur Heart J 33:372–383. doi:10.1093/eurheartj/ehr387
Sales FJ, Falcao BA, Falcao JL et al (2010) Evaluation of plaque composition by intravascular ultrasound “virtual histology”: the impact of dense calcium on the measurement of necrotic tissue. EuroIntervention 6:394–399. doi:10.4244/eijv6i3a65
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
None.
Rights and permissions
About this article

Cite this article
Chung, JH., Ann, S.H., Singh, G.B. et al. Segmental assessments of coronary plaque morphology and composition by virtual histology intravascular ultrasound and fractional flow reserve. Int J Cardiovasc Imaging 32, 373–380 (2016). https://doi.org/10.1007/s10554-015-0794-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10554-015-0794-8