
Abstract
Genetic variations in a disintegrin and metalloprotease 12 (ADAM12) gene may contribute to develop Osteoarthritis (OA) that is characterized by cartilage matrix degradation and osteophytes formation. Therefore, the aim of present study was to analyze the association between the ADAM12 gene variants and knee OA predisposition. Tetra‐primers ARMS‐PCR was employed, to genotype the ADAM12 gene polymorphisms (rs1044122 and rs1871054) in 400 knee OA patients and equal number of age-matched controls. The association between ADAM12 gene variants and OA susceptibility was estimated using the Chi-square, logistic regression, haplotypes and linkage analyses. A significant association of rs1044122 (genotype: χ2 = 18.94; P < 0.001, allele: χ2 = 19.10; P < 0.001) and rs1871054 (genotype: χ2 = 10.04; P = 0.007, allele: χ2 = 10.57; P = 0.001) was observed with increased OA susceptibility. The variant genotype of rs1044122 increased OA risk more than twice [odds ratio (OR) 2.20; P = 0.001] and the risk was higher in females (OR 2.43; P = 0.001). The variant genotype of rs1871054 was perceived to almost double the risk in females (OR 1.97; P = 0.003). Moreover, a significant association of rs1044122 and rs1871054 under the additive genetic model (P < 0.001 and P = 0.002, respectively) was observed. The targeted ADAM12 gene polymorphisms, showed significant association with knee OA susceptibility. Females harboring the polymorphisms might be at risk. Besides, the haplotype CC of rs1044122 and rs1871054 in the ADAM12 gene may double knee OA risk. These findings may help in determining the etiology of OA and recognizing the people at risk of developing knee OA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Osteoarthritis (OA) is a prevalent degenerative joint disorder and the leading source of years lived with disabilities (YLDs) across the globe (Vos et al. 2015). In 2017 OA prevalence and incidence were estimated to be 303.1 million and 14.9 million respectively, while YLDs was accounted to be 9.6 million (Safiri et al. 2020). The prevalence of OA had been increased substantially over the past 20 years and would likely to be increased further (Holt et al. 2011; Turkiewicz et al. 2015). Moreover, OA occurrence also increased among younger people ≥ 15 years of age (Yu et al. 2015). Knee OA is the most common disorder with a gradual progression leading to disability. However, about 3.4% of the patients develop the accelerated OA in 4 years (Driban et al. 2014, 2020). The joint disorder occurs by the articular cartilage degradation as a consequence of bone-on-bone friction in the joint area that causes pain and stiffness with movement limitations. Various risk factors including age, female sex, excessive joint use, and obesity, contribute to OA development, and approximately 30% of OA risk is genetically determined (Valdes et al. 2010). Various Genome-Wide Association Studies (GWAS) have recognized that some single nucleotide polymorphisms (SNPs) showed an association with the reduced thickness of articular cartilage in the knee and hip OA patients (Casalone et al. 2018; Styrkarsdottir et al. 2017).
A disintegrin and metalloprotease 12 (ADAM12) gene is a member of the ADAM family and one of the candidate genes associated with OA susceptibility (Wu et al. 2017). The ADAM family comprises more than 30 zinc-dependent proteases that are accountable for proteolytic activities, adhesion and intracellular signaling (Giebeler and Zigrino 2016). Similarly, the ADAM12 gene is responsible for the development of bones, proliferation of chondrocytes, and differentiation of osteoclasts with a very critical role concerning both the normal physiology and OA pathology (Okada et al. 2008). Therefore, the genetic investigations of the ADAM12 were carried out in various OA-centered studies encompassing diverse ethnic groups and populations (Hao et al. 2017; Poonpet et al. 2016).
Since the chondrocytes maintain the equilibrium between the synthesis and degradation of cartilage extracellular matrix (ECM), the polymorphisms in ADAM12 gene in OA may enhance cartilage degradation process by disturbing the balance (Okada et al. 2008; Roy et al. 2004). In addition, the ADAM12 gene may contribute to the arthritis predisposition through osteophytosis that is related to bone remodeling and neochondrogenesis (Kerna et al. 2013). Osteophytes act as an indicator of the remodeling processes and reflect OA progression in affected joints. The rs1044122 represents synonymous polymorphism in the ADAM12 gene, which showed a significant association with osteophytosis, predominantly in female cases of OA (Kerna et al. 2013). Besides, the intronic variant rs1871054 may elevate the ADAM12 gene translation in bones and joints with progressive cartilage ECM degeneration (Lv et al. 2017). Though various studies have evaluated the relationship between these SNPs of the ADAM12 gene and the proneness to knee OA in multiple ethnic groups, the obtained results are varying among the studied populations. For instance, the rs1044122 has not shown any association with OA susceptibility in various studies (Jung et al. 2019; Lou et al. 2014; Valdes et al. 2006; Wang et al. 2015; Yang et al. 2017). Similarly, the association of rs1871054 was not observed in the Caucasian population (Valdes et al. 2006). Besides, a meta-analysis confirmed the substantial contribution of rs1871054 to enhance knee OA exposure in the Chinese population (Lv et al. 2017). In addition, a meta- analysis based on 5048 OA cases and 6848 controls suggested that the rs1044122 and rs1871054 might have a strong association with the vulnerability to OA (Hu et al. 2017). Hence, ADAM12 gene polymorphisms might be involved in developing OA through the excessive degeneration of articular cartilage and osteophytes development. The association analyses of the ADAM12 gene polymorphisms with OA predisposition may provide an insight into OA research. Therefore, the study more precisely depicts the role of rs1044122 and rs1871054 in the ADAM12 gene for conferring knee OA predisposition in the local population.
Methods
The Studied Participants
The study enrolled 400 physicians-diagnosed patients with radiographic knee OA based on medical history, physical examination, and radiographic evaluation. The patients were aged over 30 years and visited the department of orthopedics, trauma, and reconstructive surgery, Jinnah Postgraduate Medical Center (JPMC), Karachi, Pakistan, from January 2016 to February 2019. The standards set by the American College of Rheumatology (ACR) comprise narrow joint space, osteophytes or bone spurs with OA symptoms including joint stiffness with pain, crepitus, tenderness and joint deformation (Ashford and Williard 2014). In the present investigation, the inclusion criteria used for primary OA were wide-ranged that included the associated signs, symptoms and Kellgren–Lawrence (K–L) system-based radiographic features of OA. Moreover, the patients who had a total knee joint replacement surgeries with K–L grade > 2 have also participated in the study, excluding the patients with fractures, chronic infections, and autoimmune disorders such as rheumatoid arthritis, polyarthritis and dysplasia. Each patient indicated the pain and symptom through a 10 cm visual analogue scale (VAS) and Western Ontario and McMaster Universities arthritis index (WOMAC). Age-matched 400 healthy individuals also have participated in the study as controls who never had the signs or symptoms of bone and joint disorders based on their clinical record and a detailed investigation by physiatrists.
Ethical review boards of The Karachi Institute of Biotechnology and Genetic Engineering (KIBGE) and JPMC have approved the research. The written informed consent from each participant followed a five ml venous blood sampling in the acid citrate dextrose (ACD) vacutainers. The processes involving human subjects followed the ethical principles of human research and the Helsinki declaration of 1975, as reviewed in 2000.
Genotyping
Genomic DNA in the study was extracted from the samples by the standard phenol- chloroform technique (Sambrook et al. 1989). Construction of specific primers by Primer1 tool (http://primer1.soton.ac.uk/primer1.html) followed the rs1044122 and rs1871054 genotyping in each sample using tetra-primers Amplification Refractory Mutation System- Polymerase Chain Reaction (ARMS-PCR) (Collins and Ke 2012). The PCR primers and their relative amplicons’ sizes have been shown in Fig. 1A and B. The total volume of each PCR was 25 μl containing 250 ng DNA. For rs1044122, 016 µM forward inner (FI) primer (5′- TCCTCCCCTCCACCGGTCT-3′), 0.3 µM reverse inner (RI) primer (5′-ACGCTAGGTGCACGTTGG-3′), 0.24 µM forward outer (FO) primer (5′-CTTCTATTCCAGATTTGGTGGGGT-3′), 0.08 µM reverse outer (RO) primer (5′- CCAGGCACCAAACTAACTGCTTT-3′) along with 200 μM dNTPs, 2.0 mM MgCl2, 1X (NH4)2SO4 buffer and one unit of Taq polymerase (MOLEQULEON, Auckland, New Zealand) were used. DNA was melted for 5 min at 95 °C following 35 rounds of DNA melting for 45 s at 94 °C, primers annealing at 56 °C for 45 s, polymerization at 72 °C for 30 s and extension of the polymerization for 5 min at 72 °C.

A ADAM12 with rs1044122 showing the primers positions for T-ARMS-PCR with the amplicons’ sizes. B ADAM12 with rs1871054 showing the primers positions for T-ARMS-PCR with the amplicons’ sizes
For rs1871054, 0.16 µM FI (5′-CAGAGTAGCACAGGCCCCC-3′) primer, 0.3 µM RI (5′-ATTCCTTCCCAAGAAGCACGA-3′) primer, 0.1 µM FO (5′-CAGAGACACCCTAGGGCCAAC-3′) primer and 0.1 µM RO (5′- CAATTTCGGGATGAATCATGACA-3′) primer along with 200 μM dNTPs, 1.7 mM MgCl2, 0.85X (NH4)2SO4 buffer and one unit of Taq polymerase (MOLEQULEON, Auckland, New Zealand) were used. DNA was melted for 5 min at 95 °C before undergoing 35 rounds of melting for 30 s at 94 °C, primer annealing for 30 s at 58 °C, polymerization at 72 °C for 30 s, and elongation of the polymerization for 5 min at 72 °C. The amplicons were identified through 2.5% agarose gel electrophoresis with ethidium bromide stain (10 mg/ml), and a 100 base pairs (bp) DNA ladder, under UV exposure of the gel documentation system (Gel Doc 2000, BioRad, California, USA). To validate the PCR results, 20 (5%) samples from the patients, and an equal number of the samples from controls, were randomly selected and sequenced. For sequencing, the DNA samples were subjected to amplification by the FO and RO primers of rs1044122 and rs1871054. The amplicons were filtered through the AccuPrep PCR purification kit, Bioneer (Korea), and sequenced from Bioneer (Korea) using ABI 3130 genetic analyzer (Applied Biosystems, USA) with Big Dye™ terminator cyclic sequencing. Molecular evolutionary genetics analysis (MEGA) v6.0 was used to investigate the DNA sequences (Tamura et al. 2013).
Statistical Analyses
In addition to the descriptive statistics of the study variables, Pearson’s chi-square test was performed to analyze the categorical variables and to check the association of clinicopathological characteristics in OA patients with the variant genotypes, employing SPSS Statistics v20 (IBM Corp., Armonk, NY, USA). Baseline quantitative statistics are indicated as the mean ± standard error of the mean (SEM). Chi-square goodness of fit test was applied to check the Hardy–Weinberg equilibrium (HWE). Univariate logistic regression analyses were employed to assess the strength of the relationship between ADAM12 gene polymorphisms and OA susceptibility by estimating the odds ratio (OR) with 95% confidence interval (CI) under various models of inheritance. For adjusted OR, multivariate logistic regression analyses were used after the adjustment of confounding variables comprising sex, age and body mass index (BMI) as covariates. For sex-based association analyses, the data were stratified based on gender. The correlation between the risk and number of the variant alleles was checked by the Cochran-Armitage (CA) trend test under the additive model of inheritance. Linkage disequilibrium (LD) between the rs1044122 and rs1871054 in the ADAM12 gene was predicted among patients of the OA and control group using the HaploView ver.4.2 software (https://www.broadinstitute.org/haploview/haploview) (Barret et al. 2005). The PLINK ver.1.07 software (http://zzz.bwh.harvard.edu/plink/gplink.shtml) was employed to evaluate the haplotypes associations with OA predisposition through the estimation of ORs and 95% CI (Purcell et al. 2007). P < 0.05 reflected statistically significant outcomes.
Results
Participants Characteristics
A total of 800 participants (aged 31 to 70 years) were included in the study, comprising 400 knee OA patients and the same number of age-matched controls. The mean age of all participants was 49.79 ± 0.36 years, with no significant difference between the patients and controls (50.45 ± 0.49 versus 49.13 ± 0.53, respectively; P = 0.07). The case group comprised 312 (78%) females and 88 (22%) males while the control group comprised 300 (75%) females and 100 (25%) males and the difference was also statistically insignificant (χ2 = 1.00; P = 0.31). However, the mean BMI of patients (38.10 ± 0.45) was significantly higher than controls (26.10 ± 0.25; P < 0.001). The association of rs1044122 and rs1871054 genotypes with the clinicopathological features of knee OA, was investigated. None of the study variables showed a positive association with the genotypes of rs1044122 (Table 1) and rs1871054 (Table 2). The mean VAS score of patients was 6.31 ± 0.06, and the WOMAC arthritis index was 55.2 ± 0.75.
Tetra‐primers ARMS‐PCR and Sequencing
ADAM12 gene polymorphisms (rs1044122 and rs1871054) were genotyped in each DNA sample using the optimized tetra‐primers ARMS‐PCR protocol that revealed the wild- type TT, heterozygous TC, and the alternative CC genotypes for rs1044122 and rs1871054. An amplicon of 584 and 576 bp indicated the amplification through the outer primers of rs1044122 and rs1871054, respectively. In the case of rs1044122, the amplification by FI and RO primers generated a 259 bp amplicon representing the wild-type TT genotype. Amplification by RI and FO primers generated a 361 bp amplicon representing the variant CC genotype. However, in the case of heterozygous TC genotype, three fragments of 584 bp, 259 bp and 361 bp were observed. For rs1871054, amplification by RI and FO primers generated a 359 bp amplicon representing the wild-type TT genotype. Amplification by FI and RO primers generated a 257 bp amplicon representing the variant CC genotype. However, in the case of heterozygous TC genotype, three fragments of 576 bp, 359 bp, and 257 bp were observed. Figure 2 shows the outcomes of tetra-primers ARMS-PCR for rs1044122 and rs1871054. The PCR results were cross-validated by re-genotyping the polymorphisms in 40 (5%) samples from the study population after the random selection the results were identical both times. Additionally, the PCR findings were completely concordant with the results of sequencing. The representative electropherograms of sequences are shown in Fig. 3 (rs1044122) and Fig. 4 (rs1871054).

Genotyping of rs1044122 and rs1871054 in ADAM12 using tetra-primers ARMS-PCR. A A 259 bp PCR product in lanes including 1, 3, 5, 6, 8, 10, 12, and 13, represents the TT genotype of rs1044122. A 361 bp amplicon in lanes, including 4, 7, 11, and 14, shows the CC genotype. Amplification of both 259 and 361 bp in lanes, including 2, and 9 indicate the TC genotypes for rs1044122. B A 359 bp PCR product in lanes, including 1, 3, 7, 9, and10, represents the TT genotype of rs1871054. A 257 bp amplicon in lanes, including 2, 5, 6, and 11, shows the CC genotypes. Amplification of both 359 and 257 bp in lanes, including 4, and 8, indicate the TC genotypes for rs1871054. Lane M in A and B shows a 100 bp ladder. The 584 and 576 bp products in A, and B, respectively, are the internal control for the PCR

The electropherograms of sequences for rs1044122 in the ADAM12 gene. A Two different peaks within a trace show rs1044122. B A single red-colored peak shows the wild-type T allele. C A single blue-colored peak shows the variant C allele (Color figure online)

The electropherograms of sequences for rs1871054 in the ADAM12 gene. A Two different peaks within a trace show the rs1871054. B A single red-colored peak shows the wild-type T allele. C A single blue-colored peak shows the variant C allele (Color figure online)
ADAM12 Gene Polymorphisms Association with Osteoarthritis Susceptibility
The Pearson chi-square test with 2 degrees of freedom revealed a significant association of rs1044122 (χ2 = 18.94; P < 0.001) and rs1871054 (χ2 = 10.04; P = 0.007) genotypes with knee OA exposure. The distribution of rs1044122 and rs1871054 followed HWE in each of the study groups (Table 3). Assuming the minor allele of rs1044122 and rs1871054 as a risk allele, multiple inheritance models were employed in the study to investigate the association of the ADAM12 genetic alterations with knee OA exposure. The variant alleles of rs1044122 and rs1871054 showed a statistically significant association with disease susceptibility in the patients suffering from knee OA (OR 1.60, χ2 = 19.10; P < 0.001 and OR 1.38, χ2 = 10.57; P = 0.001, respectively). The variant genotype of rs1044122 was found to increase the risk more than twice (CC versus TT: OR 2.20, χ2 = 11.08; P = 0.001), as shown in Table 4. In addition, the genetic variant rs1044122 was perceived to have a significant association with increased knee OA predisposition under the co-dominant (TC versus TT: OR 1.74, χ2 = 13.36; P < 0.001), dominant (TC + CC versus TT: OR 1.83, χ2 = 18.01; P < 0.001), recessive (CC versus TT + TC: OR 1.71, χ2 = 5.57; P = 0.01), over-dominant(TC versus TT + TC: OR 1.50, χ2 = 7.91; P = 0.005), and additive (2CC + TC versus 2TT + TC: OR 1.56; P < 0.001) models. The risk of OA was also observed to be conferred by rs1044122 after the adjustment for sex, age, and BMI under the dominant (TC + CC versus TT: OR 1.53; P = 0.03), and additive (2CC + TC versus 2TT + TC: OR 1.38; P = 0.02) inheritance models.
In females the minor allele of rs1044122 showed a significant association with OA under each model of inheritance and the variant genotype of rs1044122 was found to confer comparatively higher disease risk (CC versus TT: OR 2.43, χ2 = 11.07; P = 0.001), shown in Table 5. The knee OA risk was also observed under the co-dominant (TC versus TT: OR 1.7; P = 0.03), dominant (TC + CC versus TT: OR 1.80; P = 0.01), additive (2CC + TC versus 2TT + TC: OR 1.53; P = 0.01), and allelic (C versus T: OR 1.58; P = 0.008) models of rs1044122 in females after the adjustment for sex, age, and BMI.
The variant genotype of rs1871054 was observed to increase the risk approximately twice (CC versus TT: OR 1.84, χ2 = 9.79; P = 0.002), as shown in Table 4. The minor allele of rs1871054 showed a significant association with knee OA risk under the co- dominant (TC versus TT: OR 1.42, χ2 = 4.42; P = 0.03), dominant (TC + CC versus TT: OR 1.56, χ2 = 7.95; P = 0.005), recessive (CC versus TT + TC: OR 1.47, χ2 = 5.62; P = 0.01), and additive (2CC + TC versus 2TT + TC: OR 1.36; P = 0.002) models of inheritance. The genetic variant rs1871054 was perceived to be associated with knee OA risk in females under the co-dominant (TC versus TT: OR 1.47, χ2 = 3.95; P = 0.04), dominant (TC + CC versus TT: OR 1.62, χ2 = 7.04; P = 0.008), recessive (CC versus TT + TC: OR 1.53, χ2 = 5.14; P = 0.02), additive (2CC + TC versus 2TT + TC: OR 1.40; P = 0.003), and allelic (C versus T: OR 1.41, χ2 = 0.93; P = 0.002) models as shown in Table 6. The variant genotype of rs1871054 was found to confer relatively higher disease risk in females (CC versus TT: OR 1.97, χ2 = 8.91; P = 0.003).
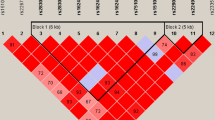
A weak linkage disequilibrium (LD) between rs1044122 and rs1871054 in the ADAM12 gene was observed (D′ = 0.56; r2 = 0.15) in the present study. Moreover, haplotype CC of the ADAM12 gene polymorphisms (rs1044122|rs1871054) showed the most significant association with increased susceptibility to knee OA (CC versus TT: OR 1.79; P < 0.001), as shown in Table 7.
Discussion
One of the main findings of the study includes the development of an efficient and economic tetra‐primers ARMS‐PCR protocol to genotype rs1044122 and rs1871054 in the ADAM12 gene. The research might be carried out for the first time to examine the relationship between the ADAM12 gene variants and knee OA vulnerability in the local population of Pakistan.
Knee OA is an extremely complicated joint disorder, contributed by a combination of multiple risk elements, including environmental factors, genetics, aging, and obesity (Khan et al. 2020; Sandell 2012). In humans, the ADAM12 gene, the candidate for knee OA susceptibility, is located at chromosome 10q26.3 and codes for ADAM12 protein that has structural and functional similarities with ADAMs (Gilpin et al. 1998). There are two forms of ADAM12 protein. ADAM12-S is the small secreted form, and ADAM12 -L is the long membrane-attached form. ADAM12-S peptide contains a protease, metalloprotease, disintegrin, and a cysteine-rich domain. In the long-form of ADAM12 protein, a cytoplasmic and transmembrane domain are also linked (Gilpin et al. 1998). Zymogen, an inactive form of ADAM12 protein, has a prodomain preserving the metalloprotease activities in the dormant state, possibly via a cysteine switch (Loechel et al. 1998). The prodomain is chemically cleaved into an active ADAM12 protein revealing the proteolytic activities in the metalloprotease domain (Loechel et al. 1998; Springman et al. 1990).The activated ADAM12 protein plays an essential role to cleave insulin-like growth factor binding protein 5 (IGFBP-5) inside the cartilage ECM to discharge the IGF-1 from the IGFBP-5 complex (Okada et al. 2008). The proteolytic activities of ADAM12 protein are highly susceptible to genetic variations. As a result, the lack of IGF-1, which is one of the growth factors for chondrocytes proliferation, may predispose the joint to its articular cartilage degeneration process and OA development (Poonpet et al. 2016).
The ECM of cartilage is well-maintained through the proliferation of chondrocytes. Under normal physiological conditions, chondrocytes uphold the balance between the development and deterioration of cartilage ECM, ensuring the articular cartilage maintenance. In the case of ADAM12 genetic alterations, the equilibrium shifts towards the excessive degradation of cartilage through the overexpression of ADAM12 gene- encoded matrix-metalloproteinase, which leads to cartilage loss and OA (Okada et al. 2008). The probable approaches of such genetic variations to overexpress the ADAM12 gene include the uncontrolled transcription process, translation of relative isoforms, or stabilization of the mRNAs (Pastinen et al. 2006). Although the genetic variants, including synonymous and intronic polymorphisms of the ADAM12 gene, do not change the protein composition, still the gene expression might be transformed through altering the mRNA level that may change the time intervals of the overall translational process. Additionally, genetic variations in the ADAM12 may change the translation rate or the protein maturation mechanism (Bartoszewski et al. 2010; Kimchi-Sarfaty et al. 2007). In this way, the genetic polymorphisms may lead to the enhanced expression of the ADAM12 gene, which explains the increased mRNA level detected in the synovial tissues of OA patients (Kerna et al. 2013).
The synonymous polymorphism rs1044122 (c.2475T > C, p. Ala825Ala) at 21st exon of the ADAM12 gene represents the variation of Ala → Ala at 825th aminoacid residue in a single peptide of ADAM12. The polymorphism was found to be mainly associated with osteophytes development, predominantly in females (Kerna et al. 2013). In the recent analyses, rs1044122 has shown a statistically significant association with knee OA, similar to the previous studies (Hu et al. 2017; Kerna et al. 2013). The variant genotype of rs1044122 has been observed to confer the risk more than twice in the current study, contrary to the Asian and Caucasian populations in which the genetic predisposition was not found (Yang et al. 2017). Similarly, the risk was not observed in the Chinese population (Lou et al. 2014; Wang et al. 2015). In the present study, rs1044122 conferred higher disease risk in females as compared to males, similar to the Estonian population, revealing twice the disease risk conferred by the altered genotype of rs1044122 in females (Kerna et al. 2013). The knee OA risk was also increased under the dominant genetic model of rs1044122 after sex, age, and BMI adjustment, contrary to the Asians and Chinese populations (Lou et al. 2014; Wang et al. 2015; Yang et al. 2017). The statistically significant knee OA association of rs1044122 under the dominant inheritance model of the current research reveals that a single copy of the altered allele may increase knee OA exposure and both the heterozygous as well as homozygous variant genotypes of rs1044122 may confer the disease risk (Bush and Moore 2012; Clarke et al. 2011).
The rs1871054 (c.1154 + 145T > C), at the 11th intron of the ADAM12 gene, may enhance the gene expression in synovial joint leading to inflammation (Lv et al. 2017). A significant association of rs1871054 was reported in the Asians but not in the Caucasian population (Lv et al. 2017). The rs1871054 showed a positive association with advanced OA and osteophytes development, particularly in tibiofibular joints of males with knee OA, suggesting the relationship to be sex-based and specific to the affected joint sites (Kerna et al. 2013). Besides, the rs1871054 showed an insignificant association with OA in the Estonian and Caucasian populations (Valdes et al. 2006; Kerna et al. 2009). In the present study, rs1871054 has been found to elevate the disease risk, in concordance with the Asian and Chinese populations (Lou et al. 2014; Wang et al. 2015; Yang et al. 2017). The variant genotype of rs1871054 has elevated the risk about two times in females, while the variant allele of rs1871054 increased the risk about one and a half times in the present study, as reported in the Chinese population (Lou et al. 2014). An association under the dominant model of rs1871054 in females of the current investigation reveals the higher disease predisposition with mere a single copy of the altered allele (Bush and Moore 2012; Clarke et al 2011). As the genotypic distributions of rs1044122 and rs1871054 in both the cases and control groups have been in HWE, the risk conferred by the genetic alterations in the present analyses might be multiplicative (Clarke et al 2011). Moreover, a significant association of rs1044122 and rs1871054 under the additive model of recent investigation reveals the constant knee OA risk increment for each copy of their variant allele (Bush and Moore 2012).
The analyses of the relationship between clinicopathological characteristics and the ADAM12 gene polymorphisms in knee OA patients have revealed insignificant associations in the present research. These findings disclose that the study variables may act as independent risk elements for disease development without any mutual effect. A strong LD between rs1044122 and rs1871054 in the ADAM12 gene was reported earlier (Lou et al. 2014).
However, in the current research, a weak LD between rs1871054 and rs1044122 has been identified, in concordance with the previous study (Kerna et al. 2013). These outcomes reveal that rs1044122 and rs1871054 in the ADAM12 gene may belong to different haploblocks, and their genetic risk assessments need separate evaluations. However, further investigation is still required to validate the findings of the present study and to clarify whether the variants of the ADAM12 gene predispose the joint to the processes of cartilage degeneration and OA development.
Conclusions
The rs1044122 and rs1871054 in the ADAM12 gene showed a statistically significant association with knee OA susceptibility in the studied population of Pakistan. Females harboring the rs1044122 and rs1871054 might be at risk of OA development. Besides, the haplotype CC of rs1044122 and rs1871054 in the ADAM12 gene may double the knee OA risk. The study findings might be useful for determining the etiology of OA and recognizing the people at risk of developing knee OA. The study outcomes may help in the development of knee OA biomarkers for reviewing the genetic exposure to the OA and manufacturing the personalized medications in the future. Hence, the study might be advantageous for developing better diagnostic and therapeutic interventions of knee OA.
Data Availability
The datasets analyzed during this study may be provided on reasonable request from the corresponding author.
References
Ashford S, Williard J (2014) Osteoarthritis: a review. Nurse Pract 39:1–8. https://doi.org/10.1097/01.NPR.0000445886.71205.c4
Barrett JC, Fry B, Maller J, Daly MJ (2005) Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics 21:263–265. https://doi.org/10.1093/bioinformatics/bth457
Bartoszewski RA, Jablonsky M, Bartoszewska S, Stevenson L, Dai Q, Kappes J, Collawn JF, Bebok Z (2010) A synonymous single nucleotide polymorphism in DeltaF508 CFTR alters the secondary structure of the mRNA and the expression of the mutant protein. J Biol Chem 285:28741–28748. https://doi.org/10.1074/jbc.M110.154575
Bush WS, Moore JH (2012) Chapter 11: Genome-wide association studies. PLoS Comput Biol 8:e1002822. https://doi.org/10.1371/journal.pcbi.1002822
Casalone E, Tachmazidou I, Zengini E et al (2018) A novel variant in GLIS3 is associated with osteoarthritis. Ann Rhem Dis 77:620–623. https://doi.org/10.1136/annrheumdis-2017-211848
Clarke GM, Anderson CA, Pettersson FH, Cardon LR, Morris AP, Zondervan KT (2011) Basic statistical analysis in genetic case-control studies. Nat Protoc 6:121–133. https://doi.org/10.1038/nprot.2010.182
Collins A, Ke X (2012) Primer1: primer design web service for tetra-primer ARMS-PCR. Open Bioinform J 6:55–58. https://doi.org/10.2174/1875036201206010055
Driban JB, Eaton CB, Lo GH, Ward RJ, Lu B, McAlindon TE (2014) Association of knee injuries with accelerated knee osteoarthritis progression: data from the osteoarthritis initiative. Arthritis Care Res 66:1673–1679. https://doi.org/10.1002/acr.22359
Driban JB, Bannuru RR, Eaton CB, Spector TD, Hart DJ, McAlindon TE, Lu B, Lo GH, Arden NK (2020) The incidence and characteristics of accelerated knee osteoarthritis among women: the Chingford cohort. BMC Musculoskelet Disord 21:60. https://doi.org/10.1186/s12891-020-3073-3
Giebeler N, Zigrino P (2016) A disintegrin and metalloprotease (ADAM): historical overview of their functions. Toxins 8:122. https://doi.org/10.3390/toxins8040122
Gilpin BJ, Loechel F, Mattei MG, Engvall E, Albrechtsen R, Wewer UM (1998) A novel, secreted form of human ADAM 12 (meltrin alpha) provokes myogenesis in vivo. J Biol Chem 273:157–166. https://doi.org/10.1074/jbc.273.1.157
Hao Z, Li X, Dai J, Zhao B, Jiang Q (2017) Genetic effects of rs3740199 polymorphism in ADAM12 gene on knee osteoarthritis: a meta-analysis. J Orthop Surg Res 12:94. https://doi.org/10.1186/s13018-017-0594-z
Holt HL, Katz JN, Reichmann WM, Gerlovin H, Wright EA, Hunter DJ, Jordan JM, Kessler CL, Losina E (2011) Forecasting the burden of advanced knee osteoarthritis over a 10-year period in a cohort of 60–64 year-old US adults. Osteoarthr Cartil 19:44–50. https://doi.org/10.1016/j.joca.2010.10.009
Hu X, Sun G, Wang W (2017) Association of ADAM 12 polymorphisms with the risk of knee osteoarthritis: meta-analysis of 5048 cases and 6848 controls. Rheumatol Int 37:1659–1666. https://doi.org/10.1007/s00296-017-3778-2
Jung JH, Song GG, Kim JH, Choi SJ (2019) Association of single nucleotide polymorphisms in a disintegrin and metalloproteinase 12 gene with susceptibility to knee osteoarthritis: a meta-analysis. Arch Rheumatol 34:62–70. https://doi.org/10.5606/ArchRheumatol.2019.6726
Kerna I, Kisand K, Tamm AE, Lintrop M, Veske K, Tamm AO (2009) Missense single nucleotide polymorphism of the ADAM12 gene is associated with radiographic knee osteoarthritis in middle-aged Estonian cohort. Osteoarthr Cartil 17:1093–1098. https://doi.org/10.1016/j.joca.2009.02.006
Kerna I, Kisand K, Tamm AE, Kumm J, Tamm AO (2013) Two single-nucleotide polymorphisms in ADAM12 gene are associated with early and late radiographic knee osteoarthritis in Estonian population. Arthritis 2013:878126. https://doi.org/10.1155/2013/878126
Khan B, Khan OY, Zehra S, Azhar A, Fatima S (2020) Association between obesity and risk of knee osteoarthritis. Pak J Pharm Sci 33:295–298
Kimchi-Sarfaty C, Oh JM, Kim IW, Sauna ZE, Calcagno AM, Ambudkar SV, Gottesman MM (2007) A “silent” polymorphism in the MDR1 gene changes substrate specificity. Science 315:525–528. https://doi.org/10.1126/science.1135308
Loechel F, Gilpin BJ, Engvall E, Albrechtsen R, Wewer UM (1998) Human ADAM12(meltrin alpha) is an active metalloprotease. J Biol Chem 273:16993–16997. https://doi.org/10.1074/jbc.273.27.16993
Lou S, Zhao Z, Qian J, Zhao K, Wang R (2014) Association of single nucleotide polymorphisms in ADAM12 gene with susceptibility to knee osteoarthritis: a case- control study in a Chinese Han population. Int J Clin Exp Pathol 7:5154–5159
Lv ZT, Liang S, Huang XJ, Cheng P, Zhu WT, Chen AM (2017) Association between ADAM12 single-nucleotide polymorphisms and knee osteoarthritis: a meta-analysis. BioMed Res Int 2017:5398181. https://doi.org/10.1155/2017/5398181
Okada A, Mochizuki S, Yatabe T et al (2008) ADAM-12 (meltrin alpha) is involved in chondrocyte proliferation via cleavage of insulin-like growth factor binding protein 5 in osteoarthritic cartilage. Arthritis Rheum 58:778–789. https://doi.org/10.1002/art.23262
Pastinen T, Ge B, Hudson TJ (2006) Influence of human genome polymorphism on gene expression. Hum Mol Genet 15:9–16. https://doi.org/10.1093/hmg/ddl044
Poonpet T, Tammachote R, Tammachote N, Kanitnate S, Honsawek S (2016) Association between ADAM12 polymorphism and knee osteoarthritis in Thai population. Knee 23:357–361. https://doi.org/10.1016/j.knee.2016.01.007
Purcell S, Neale B, Todd-Brown K, Thomas L, Ferreira MA et al (2007) PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet 81:559–575. https://doi.org/10.1086/519795
Roy R, Wewer UM, Zurakowski D, Pories SE, Moses MA (2004) ADAM 12 cleaves extracellular matrix proteins and correlates with cancer status and stage. J Biol Chem 279:51323–51330. https://doi.org/10.1074/jbc.M409565200
Safiri S, Kolahi A, Smith E et al (2020) Global, regional and national burden of osteoarthritis 1990–2017: a systematic analysis of the global burden of disease study 2017. Ann Rheum Dis 79:819–828. https://doi.org/10.1136/annrheumdis-2019-216515
Sambrook J, Fritsch EF, Maniatis T (1989) Molecular cloning, 2nd edn. Cold Spring Harbor Laboratory Press, New York
Sandell LJ (2012) Etiology of osteoarthritis: genetics and synovial joint development. Nat Rev Rheumatol 8:77–89. https://doi.org/10.1038/nrrheum.2011.199
Springman EB, Angleton EL, Birkedal-Hansen H, Van Wart HE (1990) Multiple modes of activation of latent human fibroblast collagenase: evidence for the role of a Cys73 active-site zinc complex in latency and a" cysteine switch" mechanism for activation. Proc Natl Acad Sci USA 87:364–368. https://doi.org/10.1073/pnas.87.1.364
Styrkarsdottir U, Helgason H, Sigurdsson A et al (2017) Whole-genome sequencing identifies rare genotypes in COMP and CHAD associated with high risk of hip osteoarthritis. Nat Genet 49:801–805. https://doi.org/10.1038/ng.3816
Tamura K, Stecher G, Peterson D, Filipski A, Kumar S (2013) MEGA6: molecular evolutionary genetics analysis version 6.0. Mol Biol Evol 30:2725–2729. https://doi.org/10.1093/molbev/mst197
Turkiewicz A, Gerhardsson de Verdier M, Engstrom G, Nilsson PM, Mellstrom C, Stefan Lohmander L, Englund M (2015) Prevalence of knee pain and knee OA in southern Sweden and the proportion that seeks medical care. Rheumatology 54:827–835. https://doi.org/10.1093/rheumatology/keu409
Valdes AM, Van OM, Hart DJ, Surdulescu GL, Loughlin J, Doherty M, Spector TD (2006) Reproducible genetic associations between candidate genes and clinical knee osteoarthritis in men and women. Arthritis Rheum 54:533–539. https://doi.org/10.1002/art.21621
Valdes AM, McWilliams D, Arden NK, Doherty SA, Wheeler M, Muir KR, Zhang W, Cooper C, Maciewicz RA, Doherty M (2010) Involvement of different risk factors in clinically severe large joint osteoarthritis according to the presence of hand interphalangeal nodes. Arthritis Rheum 62:2688–2695. https://doi.org/10.1002/art.27574
Vos T, Barber RM, Bell B et al (2015) Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the global burden of disease study 2013. Lancet 386:743–800. https://doi.org/10.1016/S0140-6736(15)60692-4
Wang L, Guo L, Tian F, Hao R, Yang T (2015) Analysis of single nucleotide polymorphisms within ADAM12 and risk of knee osteoarthritis in a Chinese Han population. BioMed Res Int 2015:518643. https://doi.org/10.1155/2015/518643
Wu Z, Xu XW, Zhang XW (2017) The association of ADAM12 polymorphism with osteoarthritis susceptibility: a meta-analysis. Ther Clin Risk Manage 13:821–830. https://doi.org/10.2147/TCRM.S134581
Yang Y, Wang D, Zhou K, Xie T, Zhou Z, Pei F, Yu H (2017) Association between ADAM12 gene polymorphisms and osteoarthritis risk: a meta-analysis of 10,775 participants. Int J Clin Exp Med 10:8421–8428
Yu D, Peat G, Bedson J, Jordan KP (2015) Annual consultation incidence of osteoarthritis estimated from population-based health care data in England. Rheumatology 54:2051–2160. https://doi.org/10.1093/rheumatology/kev231
Acknowledgements
The authors acknowledge Dr. Muhammad Saeed Minhas, Orthopedic Surgeon in the JPMC, for collaboration and support.
Funding
Not applicable.
Author information
Authors and Affiliations
Contributions
SF, BK: Conception and design of work. SF, BK, OYK: Data analyses and interpretation. BK, MA: Drafting of the manuscript. SF, SZ, OYK: Revision of the manuscript. AA, OYK, SF: Final approval of the manuscript to be published.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Consent for Publication
Not applicable.
Ethical Approval
All procedures performed in the study involving human participants were under the ethical standards of the Helsinki declaration (1964 and its later amendments). The institutional ethics committee of Jinnah Postgraduate Medical Centre (JPMC), Karachi and the Karachi Institute of Biotechnology and Genetic Engineering (KIBGE), Pakistan, has approved the study. All the samples have been collected with written informed consent.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Fatima, S., Khan, B., Khan, O.Y. et al. Tetra-primers ARMS-PCR Based Association Analyses of Synonymous and Intronic Variants in the ADAM12 Gene with Susceptibility to Knee Osteoarthritis: A Case-Control Study. Biochem Genet 60, 1695–1715 (2022). https://doi.org/10.1007/s10528-022-10189-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10528-022-10189-5