
Abstract
We estimated the proportion of drug users at treatment centres in Italy who had undergone HIV testing and the correlates of testing. Of the 1,917 drug injectors, 37.4% had been tested in the current year; of the 665 non-injectors, 28% had been tested. Among injectors, testing was associated with: being older than 35, foreign nationality, residing in central Italy, drug use for over 2 years, and having undergone both pharmacological and psychological treatment. Among non-injectors, an association was found for foreign nationality and not having been treated at other facilities. The results stress the need to facilitate access to testing.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The most recent guidelines on HIV testing reaffirm the need to increase screening among persons at high risk of infection, including injecting drug users, among whom testing should be performed at least once a year [1, 2]. The reasons for not undergoing HIV testing are reported to be related to the drug users themselves, the available facilities, or both. In particular, drug users may not be aware of having engaged in at-risk behaviour, or it may be difficult for them to access healthcare facilities. Furthermore, there can be a lack of appropriate facilities, or the facilities may have insufficient budgets. In Italy, the prevalence of HIV infection among drug users (both injectors and non-injectors) being treated at public drug-treatment centres (known as “SerTs”) has been decreasing unexplainably, though the proportion of drug users tested has also decreased [3]. In particular, in 2007, 38.0% of the drug users attending SerTs had never been tested or had been tested in the past yet not in the current year, whereas this proportion was much higher in the past (e.g., in 2001, it was 50%) [3]. However, no information is available on why so few drug users are undergoing HIV testing or on the characteristics of those failing to be tested, information that is crucial in controlling the spread of infection.
The objective of the present study was to determine the proportion of drug users (both injectors and non-injectors) being treated at SerTs who undergo HIV testing and to identify the correlates of testing.
Methods
In 2005 and 2007, we conducted a cross-sectional study on a sample of SerTs. In Italy there are 550 public drug-treatment centres, located in all 20 of the country’s regions. The centres offer free medical care and psychological assistance on an outpatient basis to persons who use drugs, whether injectors or not. Drug-users seek assistance at these centres on their own initiative. For each of year, 50 of the 550 existing SerTs were randomly selected with probability proportional to size sampling (number of drug users attending SerTs annually), and for each SerT, 30 drug users were selected by simple random sampling from each year’s list of attendees. Drug users who were selected in 2005 were excluded from the analysis performed in 2007.
After having provided written informed consent, these individuals underwent a structured interview using a specifically designed anonymous questionnaire, administered by trained SerT personnel. The questionnaire included socio-demographic data and information on: HIV testing; reasons for not having been tested; drug use (type, administration, and year started); sexual behaviour; number of years of SerT attendance; and type of treatment. The serological data were taken from the individuals’ clinical charts. All of the temporal variables were taken “at the time of the interview”. No incentives for participation (financial or otherwise) were provided.
Data analyses were performed separately for injectors and non-injectors. The proportion of persons tested in 2005 and 2007 was calculated, and the characteristics of the individuals who had undergone testing were compared to those who had not (never tested and those tested with a negative result in the years prior to the interview); differences were calculated with the chi-square test, given that all of the variables were, or transformed into, categorical variables.
For the analysis of the reasons for not undergoing testing (for which multiple answers were allowed), the percentage was calculated for each reason out of the total number of drug users. To identify correlates of testing, a multivariate logistic regression model was used, with testing (Yes/No) as the dependent variable. The multivariate model included all variables with a P-value lower than 0.15 in the univariate analysis, in addition to age, gender, and HIV serostatus. The goodness-of-fit was evaluated with the Hosmer and Lemeshow [4] test. The statistical analyses were performed with SPSS (version 17.0).
Results
Of the 100 SerTs selected, 87 participated (45 in 2005 and 42 in 2007). The SerTs that refused to participate declared that they did not have personnel available to collaborate on this study. However, they were not significantly different from the participating SerTs in terms of geographic location (P-value > 0.05, chi-square test) or the mean number of patients (P-value > 0.05, Student’s t-test). A total of 2,610 drug users were selected (1,350 in 2005 and 1,260 in 2007); 28 (1.1%) refused to participate, all of whom reported that they did not have the time. Thus, 2,582 drug users were included in the analysis; 1,917 (74.2%) were injectors and 83.4% were males. The median age was 33 years for females [interquartile range (IQR): 17–64] and 35 years for males (IQR: 18–66); the most represented age-group was that including persons aged 35–44 years.
The types of drugs used (at least once in lifetime) were: heroin (92.5% of participants), cocaine (65.6%), and amphetamines or ecstasy (29.9%). The median duration of drug use was: 18 years for cannabis, 16 years for heroin, 13 years for amphetamines, and 12 years for cocaine (data not shown in table). Of the 2,388 persons using heroin when first visiting the SerT, 69.0% engaged in daily use and 79.4% were injectors; of the 1,694 cocaine users, 19.7% were daily users and 75.2% injected. The use of more than one type of drug was very common: 83.5% of the drug users used two or more substances simultaneously. Only 16.7% of the participants used one type of drug only, 82% of whom were heroin users.
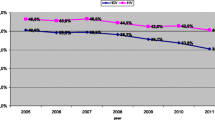
A total of 902 (34.9%) participants had been tested for HIV in the year of the interview, whereas 1,680 (65.1%) had not [i.e., both those never tested (n = 273, 16.2%) and those with a negative result in the past but who had not repeated the test in the year of the interview (n = 1,407, 83.8%)]. In 2005, 586 (43.3%) participants (both injectors and non-injectors) were tested, and in 2007, 316 (25.0%) were tested. Of the 1,917 injectors, 37.4% were tested in the year of the interview; of the 665 non-injectors, 28.0% were tested in that year.
Among the injectors, the reasons for not undergoing testing were: did not have the time or felt that it was not important (42.0%), did not engage in syringe exchange (24.6%), did not engage in at-risk sexual behaviour (21.7%), and difficulties with venous access (8%). For the remaining participants, the reason was related to how the specific SerT was organised: 13.3% reported that the SerT did not have the resources to take blood samples, and 11.5% reported that the hours in which the laboratory took blood samples did not coincide with their work hours.
The variables that were significantly associated with HIV testing in the univariate analysis are shown in Table 1 (injectors) and Table 2 (non-injectors).
According to the multivariate analysis, among injectors (Table 1), testing was significantly associated with: age greater than 35 years, foreign nationality, residing in certain regions in central Italy, having engaged in drug use for more than 2 years, having undergone both pharmacological and psychological treatment at the SerT, and inclusion in the study in 2005. Among non-injectors (Table 2), an association was found for foreign nationality, not having received any type of treatment at other facilities, and inclusion in the study in 2005.
Discussion
Failure to undergo testing can have serious consequences in preventing infection and on the health of already infected persons, due to the lack of early treatment and care. According to studies performed in other countries [5, 6], drug users can constitute a “bridge population” and transmit the virus to other groups, for example, heterosexuals. In Italy, according to the National AIDS Registry, 21.2% of the heterosexuals diagnosed since the beginning of the AIDS epidemic had acquired infection from a drug-using partner.
In our study, 34.9% of the participants (more than one-third of injectors and more than one-fourth of non-injectors) had been tested in the year of the interview. This is lower than the percentage reported by the Ministry of Health and is in part due to the extremely low proportion of persons tested in 2007. Our results are also consistent with the trend of decrease in the proportion of drug users who undergo HIV testing. As reported in other studies [7], HIV testing among injectors was significantly associated with being older than 35 years of age, which may reflect a greater probability of undergoing testing or an increased perception of risk with age. Moreover, non-national injectors were three times more likely than Italian injectors to have been tested. A plausible explanation for this finding could be an increased awareness of health status resulting from recent increases in new diagnoses of both HIV infection and AIDS among non-nationals [8], though there were too few non-nationals to draw any concrete conclusions.
Of particular interest is the finding that the proportion of drug users who had undergone testing differed by region. In some regions (generally in the north), the SerTs seem to be more efficient and perform testing for most of the attending injectors, which could be explained by the higher diffusion of infection in some regions compared to others [8, 9]. The finding that, among injectors, testing was associated with more than 2 years of drug use could reflect a greater perception on the part of both the drug user and the SerT of the risk of infection with the increasing number of years of drug use.
Drug users undergoing both pharmacological and psychological treatment were twice as likely to have undergone testing compared to those undergoing only one of the two types of treatment. This is probably related to the fact that these individuals are involved in a more complete treatment program, which involves them physically, psychologically and socially, and that they are more willing than persons undergoing methadone treatment alone to accept proposals made by the SerT personnel. Other studies have found that very low proportions of drug users not undergoing treatment are tested for HIV [10].
Finally, the drug users who were included in the study in 2005 were twice as likely to have undergone testing than those included in 2007. In fact, in 2007 only one-fourth of the drug users had undergone testing. Although this finding may confirm the trend of decrease in the proportion of drug users undergoing testing reported by the Ministry of Health [3], other factors that are not easily identifiable may also play a role, such as a lack of resources.
Among non-injectors, testing was significantly associated with foreign nationality, not having undergone treatment in other facilities, and having been included in the 2005 analysis. Factors related to sexual behaviour, such as a high number of sexual partners or a low age at first sexual experience did not constitute a determinant for testing. Nonetheless, according to other studies, the risk of sexual transmission of HIV among non-injectors is much higher than that among the general population, and sexual transmission among these individuals is becoming increasingly more common [11], not to mention the finding that the use of non-injecting drugs is also on the rise [3, 12].
Some limitations of this study should be mentioned. First of all, the fact that this was a cross-sectional study did not allow us to evaluate causality between the variables studied and failure to undergo testing but only to describe general correlations. Furthermore, the study population only consisted of persons seen at SerTs, who are not necessarily representative of the entire drug-using population in Italy, and no information is available on testing or HIV seroprevalence among drug users not being seen at SerTs. Regarding the information on drug use and sexual behaviour, we also cannot exclude either recall bias or, given that an interview was performed, response bias.
To conclude, the results of our study stress the need to promote testing among drug users, including non-injectors. Screening should be offered not only during the welcoming phase in SerTs but also on a regular basis during the entire duration of treatment, especially in geographic areas with a higher prevalence of HIV infection, and persons who test negative should be provided with information for avoiding contagion. SerT personnel should be made aware of the necessity of routine testing among injecting drug users. Furthermore, there is an apparent need to simplify access to testing, which could be achieved by arranging for blood samples to be drawn at the SerTs themselves (or creating mobile testing units). Efforts should also focus on young persons, on other persons who do not have a long history of drug use, and on non-Italians. Finally, through counseling, it may be possible to remove the obstacles that may lead a drug user to refuse testing.
References
Centers for Disease Control and Prevention (CDC). Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health care settings. MMWR. 2006;55(RR14):1–17.
UNAIDS/WHO. Guidance on provider-initiated HIV testing and counseling in health facilities. WHO. 2007;1–57.
Ministero del Lavoro, della Salute e delle Politiche Sociali—Sistema Informativo Sanitario—Dipartimento per la Prevenzione. Rilevazione attività nel settore delle tossicodipendenze-Anno 2007. 2008.
Hosmer DW, Lemeshow S. Applied logistic regression. London: Wiley; 1989.
Kane S. HIV, heroin and heterosexual relations. Soc Sci Med. 1991;32(9):1037–50.
Marvanykovi F, Melles K, Racz J. Sex and drugs: Relationships of risk perception and behavioural patterns among i.v. drug users. Psychiatr Hung. 2006;21(3):241–55.
McGarrigle CA, Mercer CH, Fenton KA, Copas AC, Wellings K, Erens B, et al. Investigating the relationship between HIV testing and risk behaviour in Britain: National Survey of Sexual Attitudes and Lifestyles 2000. AIDS. 2005;19:77–84.
Centro Operativo AIDS. Aggiornamento delle nuove diagnosi di infezione da HIV e dei casi di AIDS notificati in Italia al 31 dicembre 2008. Notiziario. 2009;22(3). Available at: http://www.iss.it/binary/publ/cont/onlinecoa1.pdf. Accessed 14 July 2009.
Rezza G, Salmaso S, Abeni D, Brancato G, Anemona A, Rovetta C, et al. HIV prevalence and frequency of risk behaviour in injecting drug users entering treatment and out of treatment a cross-sectional study in five Italian cities. J Drug Issues. 1994;24:527–35.
Donoghoe MC, Rhodes TJ, Hunter GM, Stimson GV. HIV testing and unreported HIV positivity among injecting drug users in London. AIDS. 1993;7:1105–11.
Miguez-Burbano MJ, Pineda-Medina L, Lecusay R, Page JB, Castillo G, Burbano X, et al. Continued high risk behaviors in HIV infected drug abusers. J Addict Dis. 2002;21(4):67–80.
Strathdee SA, Sherman SG. The role of sexual transmission of HIV infection among injection and non injection drug users. J Urban Health. 2003;80(3):7–14.
Acknowledgments
The authors wish to thank Roberta Urciuoli for secretarial and technical assistance, Mark Kanieff for revising the manuscript, and all of the participating SerTs. The study was approved and funded by the VI Programma Nazionale di Ricerca sull’AIDS, 2006.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
See Appendix for SERT Study Group.
Appendix
Appendix
SerT Study Group: Aliberti C, Porto S. Epidio (AP); Ardissone G, Sanremo Bussana (IM); Astegiano G, Genova; Audino G, Catanzaro; Baccaglini E, Gomma M, Verona; Baccari M, Foligno (PG); Balestra R, Masala F, Trieste; Barbato A, Capua; Beccerica E, Macerata; Belsanti S, Tarquinia (VT); Burroni P, Torino; Capogrosso I, Manduria (TA); Cioffari P, Como; Civitelli P, Thiene (VI); Coccia C, Conegliano (TV); Consoli M, Borgo San Dalmazzo (CN); Conterno I, Savigliano (CN); Conticchio Panza MF, Bari; Cuccuini M, Terni; Curcio F, Napoli; Cutrì R, Firenze; D’Ambra MF, Napoli; D’Egidio P, Pescara; Dadone P, Carmagnola (TO); Dal Lago P, Durano B, Camposampiero (PD); Del Vecchio F, Napoli; Dell’Aera S, Enna; Di Carlo M, Avezzano; Donadoni P, Bergamo; Farina P, Nettuno (RM); Favignano L, Avellino; Franco M, Roma; Gioè P, Palermo; Grenci G, Firenze; Leonetti A, Mondovì (CN); Lopez A, Altamura (BA); Lupi AM, Casella P, Roma; Macrì F, Napoli; Mantovani G, Vicenza; Orazi L, Pierantozzi M, Roma; Pennini G, Trezzo sull’Adda (MI); Pieri MC, Bologna; Pini D, Rivoli (TO); Pioli E, Lucca; Pirastu R, Iglesias; Poli C, Brindisi; Pontrelli MP, Bari; Possidente F, Gorgonzola (MI); Profeta V, Teramo; Pulvirenti L, Caltagirone (CT); Quagli S, Giaveno (TO); Quaresima S, Crema (CR); Raimondi G, Nocera Inferiore (SA); Richini M, Darfo (BS); Santini V, San Severo (FG); Scichilone L, S. Cataldo (CL); Soia M, Pavia; Sparaco A, Trapani; Tomassetti S, Roma.
Rights and permissions
About this article
Cite this article
Camoni, L., Federico, B., Capelli, G. et al. Few Italian Drug Users Undergo HIV Testing. AIDS Behav 15, 711–717 (2011). https://doi.org/10.1007/s10461-009-9616-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-009-9616-0