
Abstract
A longitudinal study of 300 HIV-positive gay, bisexual or non-gay-identified men-who-have-sex-with-men was undertaken to consider patterns relating to HIV medication adherence. The purpose of our analyses was to consider the rate of adherence in relation to both age and executive functioning as assessed by the Trail Making Test A and B. Executive functioning was assessed at baseline and month 10. Our analytic sample consisted of 213 men who remained on the same protease inhibitor throughout the assessment timeframe. Adherence rates were relatively high with more than 50% of the sample maintaining a 95%+ adherence rate at both baseline and month 10. Analyses at baseline indicated executive functioning and age were related to rate of adherence. Analyses at month 10 indicated no significant relations. Findings support previous research and suggest that the status of executive functioning as well as age be given consideration when working with HIV-positive individuals.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The advent of antiretroviral therapy (ART formerly known as HAART) has been a major stepping-stone in treatment of HIV disease. The widespread use of the ART has led to improved clinical outcomes, including reduced mortality rates (Palella et al., 1998). However, ART is not without its limitations. Studies have suggested those using ART must sustain a 90–95% adherence rate in order to suppress the virus (Paterson et al., 2000). A failure to maintain a strict adherence to the regimen can cause a rise in the level of detectable virus in the blood as well as the development of drug resistant strains (Wainberg & Friedland, 1998). Due to the complexity of the ART regimen, with patients sometimes taking numerous pills a day at varying times, it has been said that “combination therapy for HIV illness is perhaps the most rigorous, demanding and unforgiving of any outpatient oral therapy ever introduced” (Rabkin & Chesney, 1999).
Much of recent research surrounding ART has focused on factors that preclude individuals from remaining highly adherent. The ability to maintain a strict rate of adherence has been shown to be susceptible to a number of external factors. Substance use and abuse has been consistently linked to both a reduced adherence to ART (Power et al., 2003) as well as to a decline in cognitive functions that could contribute to a decrease in adherence rates (Bondi, Drake, & Grant, 1998). Poor adherence patterns have been noted among injection drug users (Shannon et al., 2005). In addition, a number of psychosocial factors have been shown to affect adherence rates. Depression (Kalichman, Difonzo, Austin, Luke, & Rompa, 2002), anxiety (Bybee & Zigler, 1991), guilt (Treisman, Angelino, & Hutton, 2001), self-efficacy and avoidant coping strategies (Halkitis, Kutnick, & Slater, 2005) have all been shown to negatively impact adherence to ART.
In addition to the aforementioned factors, the role of cognitive impairment in relation to medication adherence is one that continues to be of paramount importance. Cognitive impairment is often associated with HIV infection, and can range in severity from a subtle neuropsychological impairment without evidence of disease to HIV-1-associated dementia (Baldewicz et al., 2004). While research attempting to understand the relation between disease progression and its impact on cognitive functioning remains inconclusive, the advent and widespread use of HAART has had a significant impact on the relation between cognitive impairment and HIV infection.
Since the advent of ART, the prevalence of HIV-related cognitive impairment has been shown to have decreased (Ferrando et al., 1998). These medication regimens have been shown to provide superior neuroprotective benefits in domains such as attention, concentration, learning, memory and psychomotor speed when compared with less potent antiretroviral regimens (Ferrando et al., 1998; Ferrando, Rabkin, van Gorp, Lin, & McElhiney, 2003). However, although ART has reduced the overall incidence of HIV dementia, HIV-associated cognitive impairments continue to be a major clinical problem (Goodkin et al., 2001) and recent studies have indicated that patients continue to exhibit neurocogntive impairment even after extended periods on ART (Starace et al., 2002; Tozzi et al., 2001). In one recent study, HIV-associated neurocognitive impairments were found to be present in nearly one-third of those patients on ART (Tozzi et al., 2004).
HIV infection has also been shown to lead to significant cognitive dysfunction in areas such as information possessing, memory, attention, and executive function (Bornstein et al., 1992; Heaton et al., 1995; Miller et al., 1990). Other areas of neuropsychological dysfunction have been implicated in HIV infection as well. A meta-analysis from 41 studies examining neuropsychological functioning in HIV infection indicated the domains of cognitive functioning which showed the greatest deficits were motor functioning, executive functioning and information processing speed (Reger, Welsh, Razani, Martin, & Boone, 2002). These neuropsychological deficits have been identified in the past as affecting an infected person’s ability to work (Albert et al., 1995), their activities of daily living (Albert et al., 1994) and their ability to manage medication regiments (Heaton et al., 2004).
Cognitive functioning in relation to ART adherence is a topic that recently has been explored in greater depth. Several studies have found significant relations between a global cognitive dysfunction and a sub-optimal rate of adherence to the ART regimen. Research indicates that specific cognitive domains such as executive functioning and memory may have a direct impact on adherence rates. For example, Hinkin et al. (2002) explored the extent to which neuropsychological dysfunction was a predictor of poor adherence. The study examined 137 HIV infected individuals who were on the ART regimen. Participants were given a comprehensive battery of neuropsychological tests and were followed over a 4-week period to measure their adherence using the Aardex® Medication Event Management System (MEMS) Track Caps, also known as Electronic Drug Monitoring (EDM). Results indicated that those participants with cognitive dysfunction were significantly more likely to have poor rates of adherence. Results also indicated that executive dysfunction and memory impairment were the two domains of cognition most strongly correlated with a lack of adherence to medication.
Deficits in cognitive flexibility and executive function, as measured by the Trail Making B Test and Kaufman Adult Intelligence Test (KAIT), were found to be associated with sub-optimal adherence to HAART over a 4-week period in HIV-infected participants (Avants, Margolin, Warburton, Hawkins, & Shi, 2001). Also, Wagner (2002) examined adherence and cognition based on a battery of neuropsychological tests in relation to three different types of adherence measures: EDM, medication diaries, or control with no surveillance. Results of the study indicated that cognitive functioning was the factor most strongly correlated with low-adherence across all three groups. In a follow-up study, Hinkin et al. (2004) investigated both neuropsychological dysfunctions in relation to ART adherence as well as advancing age. The data indicated that both age and global neuropsychological performance were significantly associated with medication adherence. More specifically, neuropsychologically compromised participants were more than two times more likely to be poor adherers. Once again, executive functioning was one of the cognitive domains most strongly associated with poor adherence. In addition, older participants, age 50 and above, had a much higher rate of adherence as a group. However, older participants who showed poor adherence were significantly more likely to exhibit a cognitive dysfunction, suggesting an interactive effect of age and cognitive functioning on adherence to HIV medications.
As noted earlier, the relation between cognitive functioning and HIV treatment adherence is only beginning to be explored. We feel this topic is currently and will continue to be of substantial relevance to the further understanding and treatment of HIV and we seek to add to the current body of knowledge. The dissemination of such knowledge could be used to enhance the currently implemented intervention strategies or inform the development of new programs for enhancing adherence such as teaching useful adherence techniques and incorporating routine neuropsychological screening into visits with primary care providers. These data also have important clinical implications for practitioners working with HIV-positive individuals, particularly in light of the aging HIV-positive population in the United States. Finally, this work provides a foundation for more elaborate studies that combine an understanding of HIV medication adherence with cognitive functioning and behavior. Thus, the goal of the analysis put forth in this paper is to examine HIV medication adherence as it relates to both age and executive functioning. Our data were drawn from a longitudinal, quantitative study of HIV medication adherence among 300 gay, bisexual, and non-gay-identified men-who-have-sex-with-men (MSM).
Methods
Design
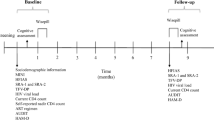
The data for our analysis were drawn from a longitudinal study of HIV medication adherence locally known as Project Pills (Protease Inhibitor Longitudinal Life Study), wherein a sample of 300 HIV-positive gay, bisexual, and non-gay-identified MSM in the New York City metropolitan area were sampled. Although participants underwent eight assessments spanning 1 year (baseline, baseline +2 weeks, 2, 4, 6, 8, 10, and 12 months), the data described here will only pertain to the assessments undertaken at the baseline +2 weeks and month ten time points where medication adherence and cognition were assessed simultaneously.
Participants and Procedures
A targeted recruitment strategy was used in all active recruitment of participants, which was done at both AIDS service organizations and in mainstream gay venues such as bars, cafes, dance clubs, sex clubs, and on streets in predominantly gay neighborhoods. These efforts were supplemented by passive recruitment which included leaving printed materials in stores, AIDS service agencies, gay-themed venues and by posting advertisements in gay and mainstream publications. Although random sampling for this study was implausible, a targeted sampling strategy (Watters & Biernacki, 1989) was used to ensure that while not random, the sample was diverse. Also, by directing attention at venues that serve the needs of HIV-positive gay and bisexual men of color, a considerable effort was made to ensure recruitment of men of diverse ethnicity.
Potential participants were screened for eligibility over the telephone. Inclusion criteria included: (1) being biologically male, (2) the ability to read and communicate in English; (3) identifying oneself as HIV-positive; (4) reporting as having had sex with another man in the previous year; (5) being 18 years of age or above, (6), and being on a ART regimen that included at least one protease inhibitor which was prescribed at the time of the study (2000-2004): Saquinavir (Fortovase), Ritonavir (Norvir), Indinavir (Crixivan), Nelfinavir (Viracept), Amprenavir (Agenerase), and Lopinavir (Kaletra). Individuals who met eligibility criteria and who were still interested in participating after having been screened were then scheduled for a baseline interview that consisted of two sessions.
At the first of the two baseline appointments, the specifics of the study were conveyed to participants, consent was obtained, and the use of the EDM system was explained. Demographic and psychosocial characteristics were obtained via quantitative measures using the Audio-CASI administered quantitative survey (Turner et al., 1998). At the conclusion of the first baseline session, the second appointment, this one a baseline follow-up, was scheduled for 2 weeks later. At the baseline follow-up session, the proper functioning of the EDM was assessed, and the data it recorded was given to participants to verify for accuracy. The Trail Making Test (TMT) (Wagner, 2002) was also administered at the baseline meeting to assess executive/frontal functioning. Participants then returned for assessments at 2, 4, 6, 10, and 12-month intervals. At each time point EDM information was assessed and the data recorded was given to participants to document their adherence-related behaviors. At the 10-month time point the TMT was repeated to assess executive/frontal functioning. Each appointment took ∼90–120 min to complete and participants were provided a monetary incentive of $20.
Measures
The data reported are based on EDM and executive functioning data obtained at both baseline and month 10. Demographic and health characteristics were drawn from baseline surveys.
Socio-demographic Characteristics
We assessed self-reported year of birth, race/ethnicity, sexual orientation, relationship status, employment status, annual income, and health care coverage. Additionally, participants were asked to specify the year in which they had first tested positive for HIV antibodies and whether they had been diagnosed with AIDS, and if so, in what year the AIDS diagnosis had been made.
HIV Medication Regimen
At each time point participants self-reported their HIV medication regimen using a chart of medications to identify those in their ART regimen. With the consent of participants, regimens were confirmed with the participants’ healthcare providers.
Adherence
Adherence to the protease inhibitor included in each participant’s medication regimen was measured at baseline, as well as each 2-month time interval by using EDM. The EDM monitored adherence by means of a computer chip embedded into a standard sized medication bottle cap, the system records the dates and times at which the medication bottle is opened and records these as events (Kruse, Rampmaier, Ullrich, & Webber, 1994; Matsuyama, Mason, & Jue, 1993; Waterhouse, Calzone, Mele, & Brenner, 1993). This information was then downloaded as a data file and used along with dosing information for the specific protease inhibitor to determine percentage of adherence to that medication. Additionally, participants along with a research assistant reviewed the data to specify which doses were correctly identified as having been taken or missed by the EDM. Baseline treatment and dosing regimens were confirmed with the participant’s healthcare providers to insure accuracy. Incorrect data was revised to reflect either the time at which a specific medication had been taken but had not been recorded or to reflect the reason for missing a dose. As previous research has found, deriving adherence percentages from EDM data without such consideration may not be an accurate account of adherence percentages, and adherence rates to HIV medications may even be underestimated (Hill, Kendall, & Fernandez, 2003; Hugen et al., 2002; Wagner & Rabkin, 2000). This corrected data was used to obtain adherence percentages for the specific protease inhibitor being monitored for each participant. In addition, a self-reported measure on adherence was administered via the Audio-CASI system to ensure the validity of the adherence measurements. The measure asked participants to indicate doses missed in the assessment period. More specifically, the self-report items asked participants to indicate the number of doses missed in the previous 2 weeks (baseline) and in the previous 2 months (months 2, 4, 6, 8 10, and 12). Data for the ensuing analyses were based on measures obtained at baseline (a 2 week period of assessment) and at Month 10 (a 2-month period of assessment).
Executive Functioning
Executive functioning was assessed using the TMT. The TMT was originally developed as part of the Army Individual Test Battery (1944) and is currently part of the Halstead-Reitan Testing Battery (Wagner, 2002). It is one of the most commonly used neuropsychological tests because of its high sensitivity to the presence of cognitive impairment (Lezak, 1995). The test has two parts, A and B. Performance is assessed by the time taken to complete each trial correctly (Reitan & Wolfson, 1993). Part A requires competency in areas such as visual scanning, numeric sequencing, and visual motor speed (Gass & Daniel, 1990). Part B is reputed to be more challenging then Part A (Kortte, Horner, & Windham, 2002), as Part B incorporates the characteristics of Part A and also requires the participant be able to switch focus between cognitive sets and deal with more then one stimulus at a time (Avants et al., 2001). It has been suggested that Part B performance is indicative of executive function, and that difficulty with the task might be reflective of impaired executive control or the ability to flexibly shift the course of an ongoing activity (Arbuthnott & Frank, 2000). The Trails Test Part B in particular has been shown to indicate a participant’s inability to execute or modify a plan and is a useful tool in identifying frontal lobe dysfunction (Gaudino, Geisler, & Squires, 1995).
Results
Sample Characteristics
Of the 300 participants in our sample, all were HIV-positive biological males. The average age of the participants was 42 (SD = 7.72) and ranged from 20 to 70. With regards to HIV-positive serostatus, the data indicated participants in our sample had been diagnosed for 9.51 years on average (SD = 4.34), ranging between the years 1984 and 2001. Of these men, 65% (n = 195) reported having an AIDS diagnosis. Those 195 participants who reported having an AIDS diagnosis have been living with the syndrome for 6.26 years on average (SD = 3.69). The earliest diagnosis reported was 1984 and the latest was 2001. Characteristics concerning ethnicity, sexual orientation, relationship status, employment status, income, and healthcare coverage, can be found in Table 1.
Of the 300 participants who completed the initial study, a subset of 213 participants met the criteria for these analyses. Because stopping or switching regimens has been linked to adverse health effects (d’Arminio Monforte et al., 2000), only participants who continued taking the same protease inhibitor throughout the duration of the study were included to potentially avoid impacting neuropsychological function (Parsons, Braaten, Hall, & Robertson, 2006). Thus, limiting the analytic sample to these 213 helped to control for this potential confound. Characteristics of the sub-sample were not significantly different with those of the overall sample. The average was 42 years of age (SD = 7.56) and ranged from 26 to 66. The sub-sample also closely matched the overall sample in terms of ethnicity, healthcare coverage, relationship status, employment status, and annual income, and sexual orientation. These frequencies are shown in Table 1. With regard to HIV disease, data from the analytic sample indicated that participants had been diagnosed as seropositive for 9.58 years on average (SD = 4.30) as compared to 9.51 years on average (SD = 4.34) of the overall sample.
Treatment and Adherence Characteristics
In terms of HIV antiretroviral medication use, participants in this analysis were taking a protease inhibitor on average of 3.26 years (SD = 1.55) and as of their baseline interview had been taking their current protease inhibitor (PI) for an average of 1.67 years (SD = 1.73). Viracept was the most frequently taken PI with 28% (n = 60) of participants using this medication. This was followed by Crixivan (n = 37) and Kaletra (n = 36), with ∼17% of the sample. The remainders were as follows: Norvir (14%, n = 30), Fortovase (11%, n = 24) and Agenerase (10%, n = 22). It should be noted that no discrepancies were found with regard to actual medications being taken as reported by participant and health care provider.
With regard to adherence, adjusted EDM data as well as data collected by the self-report by means of Audio-CASI, were used to place participants into four categories as such: 95% or greater, 90–94, 80–89, and <80%. This four-group method of classification was used in other studies to classify HIV medication adherence (Carrieri et al., 2001; Hill et al., 2003; Mannheimer, Friedland, Matts, Child, & Chesney, 2002). As noted in previous analyses (Halkitis et al., 2005), the methods yield significantly equivalent results. Thus, in the ensuing analyses we utilize only the adjusted EDM data to examine the relations of interest.
Adherence as measured by the adjusted EDM data at the baseline interview placed the majority of participants, over 65% (n = 139) in the 95% or greater category in terms of medication adherence. Adherence as measured at month 10 put over 50% (n = 109) in the 95% or greater category. Adherence rates by category for baseline and month 10 are shown in Table 2.
Because previous literature recommends that executive functioning be examined in terms of two adherence groups 95%+ and <95% (Hinkin et al., 2004), we re-grouped adherence rate as per the two levels and utilized this variable for adherence in our analyses. Re-grouping adherence in this manner resulted in the following rates: 69.2% (n = 139) had 95%+ adherence at baseline and 56.8% (n = 109) of the participants had 95%+ adherence at month 10.
Executive Functioning
Participants took an average of 33.67 (SD = 14.34) seconds to complete trails Part A at the baseline interview, with a range between 12 and 97 s. Completion of trails in Part B at the baseline interview took participants 86.34 (SD = 57.53) s, with a range between 25 and 503 s. At month 10, participants took an average of 32.15 (SD = 14.38) s to complete trails Part A, with a range between 14 and 117 s. The trails of Part B took participants an average of 78.77 (SD = 39.91) s to complete at the month 10 interviews, with a range between 21 and 240 s.
Relations between Adherence, Executive Functioning and Age
We examined the relations between the adherence and executive function while also considering age, since previous research indicated that people with HIV whose age is 50 years or greater are significantly more likely to show neuropsychological deficits, specifically on measures of executive functioning (Hinkin et al., 2004).
A comparison of means using independent samples t-tests determined the relations between age and executive functioning as well as adherence and executive functioning. Given these multiple comparison, we used a Bonferroni correction and set the significant value at p = 0.025). The results indicated no relation between age level (<50, 50+) and performance in executive functioning both at baseline and month 10. We then conducted independent samples t-test to consider rates of test completion on Trails A and B, based on our adherence groupings. The results are shown in Table 3 and indicate that at baseline there was a significant difference between those who were categorized as optimal adherers (95%+) and those with sub-optimal rates of adherence (<95%) on the TMT B [t (197) = 2.85, p < 0.01], with those with sub-optimal adherence taking a significantly greater amount of time to complete the test.
We also compared rate of adherence based on our age groupings. A Chi-Square test of independence indicated that participants in the 50+ age group had a significantly better rate of adherence overall at baseline than those in the younger group [χ 2 (1) = 7.14, p < 0.01]. However, the difference in adherence rate between groups did not remain significant at month 10. Complete adherence rates based on our age groupings can be found in Table 4.
Discussion
Using objective measures of neuropsychological function (TMT Part A and Part B) and rate of medication adherence (EDM), these analyses sought to examine the relation between executive functioning, medication adherence, and age in HIV-positive gay, bisexual, and non-gay-identified MSM. Since data on adherence and cognitive executive functioning was gathered simultaneously at two distinct time points (baseline and 10 months) it is important to consider the significant findings from both.
At baseline, age explained adherence to HIV treatment. HIV-positive men who were categorized as 50 or older were significantly more likely to have an adherence rate of 95% or greater then their younger counterparts. This finding closely matches the findings of Hinkin et al. (2002, 2004). However, unlike previous investigations, our analysis of the data collected at month 10 indicated no significant differences between age cohorts.
Data from our baseline analyses indicated a significant difference between those who were categorized as optimal adherers (95%+) and those with sub-optimal rates of adherence (<95%) on the TMT B, with those with sub-optimal adherence taking a significantly greater amount of time to complete the test. These findings replicate those previously found (Avants et al., 2001; Hinkin et al., 2002, 2004; Kimmerling, Wagner, & Ghosh-Dastidar, 2003) in which results all indicated a significant relation between executive/frontal systems dysfunction as specifically measured by Trails B and a sub-optimal rate of adherence. While not significant, baseline data indicated a strong relation between those who were categorized as optimal adherers (95%+) and those with sub-optimal rates of adherence (<95%) on the TMT A. This data supports findings by Wagner (2002) who also found a significant relation between cognitive impairment as assessed by Trails A and sub-optimal medication adherence as measured by EDM. Once again, data from the month 10 time point showed no significant relation between level of adherence and performance on TMT A or B. It should be noted that Tombaugh (2004) has shown a comprehensive set of norms for this battery and moreover how scores vary along levels of age and education. Thus, given the diversity of our sample along these dimensions we cannot make a direct comparison of our participant’s scores to a “norm” group.
The importance of properly functioning executive systems is vital to all people, however, within the HIV-positive MSM population the utilization of properly functioning EF are further highlighted. The social realities of this group, such as maintaining optimal adherence to medication, preventing the transmission of HIV and other STDs, coupled with the environmental realities of an increased propensity toward substance use and risky sexual behavior make the reliance on EF-related domains all the more essential. As planning, judgment, impulse control and decision-making are related to executive functioning, a dearth in any of these areas has potentially life threatening consequences for HIV-positive men. If research continues to suggest executive functioning and optimal medication adherence are highly related, then it will be important for clinicians to begin to look and test for deficits in EF as well as explain the intricate relationship between cognitive functioning and a person’s ability to effectively suppress HIV.
This study had a number of limitations that may have contributed to the deterioration of the significant relations between performance on the TMT A and B and rate of adherence between baseline and month 10. Certain confounds may have affected the relations between overall age and adherence from baseline to month 10. First, the data were gathered retrospectively and a full neuropsychological testing battery never was given to assess participant’s global cognitive abilities before adherence data was collected. The literature suggests that depressive symptoms (Kalichman et al., 2002) are more prevalent in sub-optimal adherers and may actually be the underlying catalyst behind poor performance on tests of cognitive function when measured objectively (Ammassari et al., 2003, 2004). Our analysis did not take into account any objective measures used to assess depressive symptoms of participants. In addition, while a relation between drug use and sub-optimal adherence to medication has been established (Halkitis et al., 2005), it is not known whether lack of adherence stems from impaired cognitive functioning due to substance use (Rosselli & Ardila, 1996), the type of lifestyle led by someone using illicit substances (Hinkin et al., 2004), or some combination of both. Future analyses of the data should account for these behaviors.
It is also important to recognize the possible practice effects on the TMT (administered at two time points within 1 year) as well as the implications of simply partaking in a study measuring adherence over time, which may have had intervention-like qualities. The self-selected nature of the sample (despite our active recruitment strategy), could also be seen as a possible limitation as it is possible that the sample of men who responded may have been more concerned with adherence then that of the general population.
We also recognize that participants included in our analysis had been taking a protease inhibitor on average of close to 3 years. Because we did not control for how long participants had been taking a PI before entering into this study, it is possible that those participants who were on medication for a longer period of time before enrolling may have benefited from possible neuroprotective effects of medication, potentially effecting performance on measures of executive functioning (Ferrando et al., 1998). However, research has also suggested that elevation of viral load specifically in the cerebrospinal fluid and brain (CNS) is associated with HIV-neurocognitive disorders (Di Stefano et al., 1998; Ellis et al., 1997; McArthur et al., 1997). With the exception of Indinavir, protease inhibitors have been shown to have poor blood-brain barrier penetration, raising concern that HAART regimens similar to those used by subjects in this analysis do not grant any substantial benefit to CNS disease or neurocognitive performance (Ferrando et al., 2003).
Finally, we also would like to point out that differences in adherence rates from baseline to month 10 might be attributed to an overall trend which suggests that longitudinally, particularly when measuring for time periods greater then 1 month, adherence to medication often declines, particularly in those participants who have higher initial levels of adherence (Gross, Bilker, Friedman, & Strom, 2001; Liu et al., 2001; Mannheimer et al., 2002).
Limitations not withstanding, these analyses demonstrate significant relations between executive/frontal function and rate of adherence to HIV medication. The data shows a significant relation between age and level of adherence. While the significance of these relations only pertains to data collected at the baseline (2 weeks) time point, studies which parallel our results have been roughly equivalent in duration (2–4 weeks). Why the significance of these relations deteriorates over the course of 10 months is an unknown. To our knowledge there have been no previous studies, which have simultaneously tracked medication adherence and executive functioning, for an equivalent amount of time, although the work of Cohen et al. (2001) establishes a positive relation between executive function and HAART administration. However this study does not consider the role of optimal medication adherence in these relations.
As has been noted throughout the adherence literature (see Sankar, Golin, Simoni, Luborsky, & Pearson, 2006 for review), there is no definitive standard for assessing adherence to ART/HARRT. We recognize that by modifying the EDM data with feedback from the participant we are taking a seemingly objective measure and introducing it with subjectivity. However, we believe the adjusted EDM data are a more accurate measurement of the actual adherence rates of the participants, who needed to adjust their use of the EDM to address the realities of their daily lives.
Our data, like much of the previous literature, has shown a significant relation between optimal adherence and the use of specific cognitive domains such as executive functioning. However, the inconsistency in our long-term data coupled with the lack of studies which monitor adherence in relation to executive functioning over longer periods of time will not allow us to accurately predict if cognitive dysfunction causes poor adherence or if poor adherence results in problematic clinical outcomes including cognitive dysfunction, which Hinkin et al. (2004), referred to as the “Bi-Directional relationship.” However, building on the findings of Cohen et al. (2001), it is likely that those on HARRT who demonstrate improvement in immune and executive functioning are also adhering at an optimal rate. With HIV rates continuing to remain stable within MSM population and over 60,000 HIV infected individuals currently older than 50 years of age and rising (Valcour & Paul, 2006), there is clearly a need to expand further research into this area.
References
Albert, S. M., Todak, G., Elkin, E., Marder, K., Dooneief, G., & Stern Y. (1994). Time allocation and disability in HIV infection: A correlational study. Journal of Occupational Science, 1, 21–30.
Albert, S. M., Marder, K., Dooneief, G., Bell, K., Sano, M., & Todak, G. et al. (1995). Neuropsychologic impairment in early HIV infection. A risk factor for work disability. Archives of Neurology, 52(5), 525–530.
Ammassari, A., Antinori, A., Aloisi, M. S., Trotta, M. P., Murri, R., & Bartoli, L. et al. (2004). Depressive symptoms, neurocognitive impairment, and adherence to highly active antiretroviral therapy among HIV-infected persons. Psychosomatics, 45(5), 394–402.
Ammassari, A. A., Starace, F., Aloisi, M. S., Trotta, M. P., Murri, R., & D’Arminio Monforte, A. et al. (2003). Medication adherence among HIV+ adults: Effects of cognitive dysfunction and regimen complexity. Neurology, 61(5), 723–4; author reply 724.
Arbuthnott, K., & Frank, J. (2000). Trail making test, part B as a measure of executive control: Validation using a set-switching paradigm. Journal of Clinical and Experimental Neuropsychology: Official Journal of the International Neuropsychological Society, 22(4), 518–528.
Army Individual Test Battery (1944). Manuel of directions and scoring. Washington, DC: War Department, Adjutant General’s Office.
Avants, S. K., Margolin, A., Warburton, L. A., Hawkins, K. A., & Shi, J. (2001). Predictors of nonadherence to HIV-related medication regimens during methadone stabilization. The American Journal on Addictions/American Academy of Psychiatrists in Alcoholism and Addictions, 10(1), 69–78.
Baldewicz, T. T., Leserman, J., Silva, S. G., Petitto, J. M., Golden, R. N., & Perkins, D. O. et al. (2004). Changes in neuropsychological functioning with progression of HIV-1 infection: Results of an 8-year longitudinal investigation. AIDS and Behavior, 8(3), 345–355.
Bondi, M. W., Drake, A. I., & Grant, I. (1998). Verbal learning and memory in alcohol abusers and polysubstance abusers with concurrent alcohol abuse. Journal of the International Neuropsychological Society: JINS, 4(4), 319–328.
Bornstein, R. A., Nasrallah, H. A., Para, M. F., Whitacre, C. C., Rosenberger, P., & Fass, R. J. et al. (1992). Neuropsychological performance in asymptomatic HIV infection. The Journal of Neuropsychiatry and Clinical Neurosciences, 4(4), 386–394.
Bybee, J. A., & Zigler, E. (1991). Self-image and guilt: A further test of the cognitive-developmental formulation. Journal of Personality, 59(4), 733–745.
Carrieri, P., Cailleton, V., Le Moing, V., Spire, B., Dellamonica, P., & Bouvet, E. et al. (2001). The dynamic of adherence to highly active antiretroviral therapy: Results from the french national APROCO cohort. Journal of Acquired Immune Deficiency Syndromes (1999), 28(3), 232–239.
Cohen, R. A., Boland, R., Paul, R., Tashima, K. T., Schoenbaum, E. E., & Celentano, D. D. et al. (2001). Neurocognitive performance enhanced by highly active antiretroviral therapy in HIV-infected women. AIDS (London, England), 15(3), 341–345.
d’Arminio Monforte, A., Lepri, A. C., Rezza, G., Pezzotti, P., Antinori, A., & Phillips, A. N. et al. (2000). Insights into the reasons for discontinuation of the first highly active antiretroviral therapy (HAART) regimen in a cohort of antiretroviral naive patients. I.CO.N.A. study group. Italian cohort of antiretroviral-naive patients. AIDS (London, England), 14(5), 499–507.
Di Stefano, M., Monno, L., Fiore, J. R., Buccoliero, G., Appice, A., & Perulli, L. M. et al. (1998). Neurological disorders during HIV-1 infection correlate with viral load in cerebrospinal fluid but not with virus phenotype. AIDS (London, England), 12(7), 737–743.
Ellis, R. J., Hsia, K., Spector, S. A., Nelson, J. A., Heaton, R. K., & Wallace, M. R. et al. (1997). Cerebrospinal fluid human immunodeficiency virus type 1 RNA levels are elevated in neurocognitively impaired individuals with acquired immunodeficiency syndrome. HIV neurobehavioral research center group. Annals of Neurology, 42(5), 679–688.
Ferrando, S., van Gorp, W., McElhiney, M., Goggin, K., Sewell, M., & Rabkin, J. (1998). Highly active antiretroviral treatment in HIV infection: Benefits for neuropsychological function. AIDS (London, England), 12(8), F65–F70.
Ferrando, S. J., Rabkin, J. G., van Gorp, W., Lin, S. H., & McElhiney, M. (2003). Longitudinal improvement in psychomotor processing speed is associated with potent combination antiretroviral therapy in HIV-1 infection. The Journal of Neuropsychiatry and Clinical Neurosciences, 15(2), 208–214.
Gass, C. S., & Daniel, S. K. (1990). Emotional impact on trail making test performance. Psychological Reports, 67(2), 435–438.
Gaudino, E. A., Geisler, M. W., & Squires, N. K. (1995). Construct validity in the trail making test: What makes part B harder? Journal of Clinical and Experimental Neuropsychology: Official Journal of the International Neuropsychological Society, 17(4), 529–535.
Goodkin, K., Wilkie, F. L., Concha, M., Hinkin, C. H., Symes, S., & Baldewicz, T. T. et al. (2001). Aging and neuro-AIDS conditions and the changing spectrum of HIV-1-associated morbidity and mortality. Journal of Clinical Epidemiology, 54(Suppl. 1), S35–S43.
Gross, R., Bilker, W. B., Friedman, H. M., & Strom, B. L. (2001). Effect of adherence to newly initiated antiretroviral therapy on plasma viral load. AIDS (London, England), 15(16), 2109–2117.
Halkitis, P. N., Kutnick, A. H., & Slater, S. (2005). The social realities of adherence to protease inhibitor regimens: Substance use, health care and psychological states. Journal of Health Psychology, 10(4), 545–558.
Heaton, R. K., Grant, I., Butters, N., White, D. A., Kirson, D., & Atkinson, J. H. et al. (1995). The HNRC 500–Neuropsychology of HIV infection at different disease stages. HIV neurobehavioral research center. Journal of the International Neuropsychological Society: JINS, 1(3), 231–251.
Heaton, R. K., Marcotte, T. D., Mindt, M. R., Sadek, J., Moore, D. J., & Bentley, H. et al. (2004). The impact of HIV-associated neuropsychological impairment on everyday functioning. Journal of the International Neuropsychological Society: JINS, 10(3), 317–331.
Hill, Z., Kendall, C., & Fernandez, M. (2003). Patterns of adherence to antiretrovirals: Why adherence has no simple measure. AIDS Patient Care and STDs, 17(10), 519–525.
Hinkin, C. H., Castellon, S. A., Durvasula, R. S., Hardy, D. J., Lam, M. N., & Mason, K. I. et al. (2002). Medication adherence among HIV+ adults: Effects of cognitive dysfunction and regimen complexity. Neurology, 59(12), 1944–1950.
Hinkin, C. H., Hardy, D. J., Mason, K. I., Castellon, S. A., Durvasula, R. S., & Lam, M. N. et al. (2004). Medication adherence in HIV-infected adults: Effect of patient age, cognitive status, and substance abuse. AIDS (London, England), 18(Suppl. 1), S19–S25.
Hugen, P. W., Langebeek, N., Burger, D. M., Zomer, B., van Leusen, R., & Schuurman, R. et al. (2002). Assessment of adherence to HIV protease inhibitors: Comparison and combination of various methods, including MEMS (electronic monitoring), patient and nurse report, and therapeutic drug monitoring. Journal of Acquired Immune Deficiency Syndromes (1999), 30(3), 324–334.
Kalichman, S. C., Difonzo, K., Austin, J., Luke, W., & Rompa, D. (2002). Prospective study of emotional reactions to changes in HIV viral load. AIDS Patient Care and STDs, 16(3), 113–120.
Kimmerling, M., Wagner, G., & Ghosh-Dastidar, B. (2003). Factors associated with accurate self-reported adherence to HIV antiretrovirals. International Journal of STD and AIDS, 14(4), 281–284.
Kortte, K. B., Horner, M. D., & Windham, W. K. (2002). The trail making test, part B: Cognitive flexibility or ability to maintain set? Applied Neuropsychology, 9(2), 106–109.
Kruse, W., Rampmaier, J., Ullrich, G., & Weber, E. (1994). Patterns of drug compliance with medication to be taken once and twice daily assessed by continuous electronic monitoring in primary care. International Journal of Clinical Pharmacology Therapy, 32, 453–457.
Lezak, M. D. (1995). Neuropsychological assessment (3rd ed.). New York: Oxford University Press.
Liu, H., Golin, C. E., Miller, L. G., Hays, R. D., Beck, C. K., & Sanandaji, S. et al. (2001). A comparison study of multiple measures of adherence to HIV protease inhibitors. Annals of Internal Medicine, 134(10), 968–977.
Mannheimer, S., Friedland, G., Matts, J., Child, C., & Chesney, M. (2002). The consistency of adherence to antiretroviral therapy predicts biologic outcomes for human immunodeficiency virus-infected persons in clinical trials. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America, 34(8), 1115–1121.
Matsuyama, J. R., Mason, B. J., & Jue, S. G. (1993). Pharmacists’ interventions using an electronic medication-event monitoring device’s adherence data versus pill counts. The Annals of Pharmacotherapy, 27(7–8), 851–855.
McArthur, J. C., McClernon, D. R., Cronin, M. F., Nance-Sproson, T. E., Saah, A. J., & St Clair, M. et al. (1997). Relationship between human immunodeficiency virus-associated dementia and viral load in cerebrospinal fluid and brain. Annals of Neurology, 42(5), 689–698.
Miller, E. N., Selnes, O. A., McArthur, J. C., Satz, P., Becker, J. T., & Cohen, B. A. et al. (1990). Neuropsychological performance in HIV-1-infected homosexual men: The multicenter AIDS cohort study (MACS). Neurology, 40(2), 197–203.
Palella, F. J. Jr., Delaney, K. M., Moorman, A. C., Loveless, M. O., Fuhrer, J., & Satten, G. A. et al. (1998). Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV outpatient study investigators. The New England Journal of Medicine, 338(13), 853–860.
Parsons, T. D., Braaten, A. J., Hall, C. D., & Robertson, K. R. (2006). Better quality of life with neuropsychological improvement on HAART. Health and Quality of Life Outcomes [Electronic Resource], 4, 11.
Paterson, D. L., Swindells, S., Mohr, J., Brester, M., Vergis, E. N., & Squier, C. et al. (2000). Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Annals of Internal Medicine, 133(1), 21–30.
Power, R., Koopman, C., Volk, J., Israelski, D. M., Stone, L., & Chesney, M. A. et al. (2003). Social support, substance use, and denial in relationship to antiretroviral treatment adherence among HIV-infected persons. AIDS Patient Care and STDs, 17(5), 245–252.
Rabkin, J. G., & Chesney, M. (1999). Treatment adherence to HIV medications: The Achilles heel of new therapeutics. In D. Ostrow, S. Kalichman (Eds.), New HIV therapies: Psychology and public health implications. New York: Plenum Press.
Reger, M., Welsh, R., Razani, J., Martin, D. J., & Boone, K. B. (2002). A meta-analysis of the neuropsychological sequelae of HIV infection. Journal of the International Neuropsychological Society: JINS, 8(3), 410–424.
Reitan, R., & Wolfson, D. (1993). The helstead-reitan neuropsychological test battery: Theory and clinical interpretation. Tucson, AZ: Neuropsychological Press.
Rosselli, M., & Ardila, A. (1996). Cognitive effects of cocaine and polydrug abuse. Journal of Clinical and Experimental Neuropsychology: Official Journal of the International Neuropsychological Society, 18(1), 122–135.
Sankar, A., Golin, C., Simoni, J. M., Luborsky, M., & Pearson, C. (2006). How qualitative methods contribute to understanding combination antiretroviral therapy adherence. Journal of Acquired Immune Deficiency Syndromes (1999), 43(Suppl. 1), S54–S68.
Shannon, K., Kerr, T., Lai, C., Ishida, T., Wood, E., & Montaner, J. S. et al. (2005). Nonadherence to antiretroviral therapy among a community with endemic rates of injection drug use. Journal of the International Association of Physicians in AIDS Care (Chicago, IL: 2002), 4(3), 66–72.
Starace, F., Bartoli, L., Aloisi, M. S., Antinori, A., Narciso, P., & Ippolito, G. et al. (2002). Cognitive and affective disorders associated to HIV infection in the HAART era: Findings from the NeuroICONA study. Cognitive impairment and depression in HIV/AIDS. the NeuroICONA study. Acta Psychiatrica Scandinavica, 106(1), 20–26.
Tombaugh, T. N. (2004). Trail making test A and B: Normative data stratified by age and education. Archives of Clinical Neuropsychology: The Official Journal of the National Academy of Neuropsychologists, 19(2), 203–214.
Tozzi, V., Balestra, P., Galgani, S., Narciso, P., Sampaolesi, A., & Antinori, A. et al. (2001). Changes in neurocognitive performance in a cohort of patients treated with HAART for 3 years. Journal of Acquired Immune Deficiency Syndromes (1999), 28(1), 19–27.
Tozzi, V., Balestra, P., Murri, R., Galgani, S., Bellagamba, R., & Narciso, P. et al. (2004). Neurocognitive impairment influences quality of life in HIV-infected patients receiving HAART. International Journal of STD and AIDS, 15(4), 254–259.
Treisman, G. J., Angelino, A. F., & Hutton, H. E. (2001). Psychiatric issues in the management of patients with HIV infection. JAMA: The Journal of the American Medical Association, 286(22), 2857–2864.
Turner, C. F., Ku, L., Rogers, S. M., Lindberg, L. D., Pleck, J. H., & Sonenstein, F. L. (1998). Adolescent sexual behavior, drug use, and violence: Increased reporting with computer survey technology. Science, 280(5365), 867–873.
Valcour, V., & Paul, R. (2006). HIV infection and dementia in older adults. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America, 42(10), 1449–1454.
Wagner, G. J. (2002). Predictors of antiretroviral adherence as measured by self-report, electronic monitoring, and medication diaries. AIDS Patient Care and STDs, 16(12), 599–608.
Wagner, G. J., & Rabkin, J. G. (2000). Measuring medication adherence: Are missed doses reported more accurately then perfect adherence? AIDS Care, 12(4), 405–408.
Wainberg, M. A., & Friedland, G. (1998). Public health implications of antiretroviral therapy and HIV drug resistance. JAMA: The Journal of the American Medical Association, 279(24), 1977–1983.
Waterhouse, D. M., Calzone, K. A., Mele, C., & Brenner, D. E. (1993). Adherence to oral tamoxifen: A comparison of patient self-report, pill counts, and microelectronic monitoring. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 11(6), 1189–1197.
Watters, J. K., & Biernacki, P. (1989). Targeted sampling: Options and considerations for the study of hidden populations. Social Problems, 36, 416–430.
Acknowledgments
This research was funded by a grant from the National Institute on Drug Abuse (Contract #R01DA12816).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Solomon, T.M., Halkitis, P.N. Cognitive Executive Functioning in Relation to HIV Medication Adherence Among Gay, Bisexual, and other Men who have Sex with Men. AIDS Behav 12, 68–77 (2008). https://doi.org/10.1007/s10461-007-9273-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10461-007-9273-0