
Abstract
Purpose
Individuals with chronic ankle instability (CAI) have deficits in closed kinetic chain dorsiflexion that may perpetuate injury. Determining the characteristics of muscle stiffness in the plantar flexors of individuals with CAI may help in developing appropriate treatments. We aimed to highlight the characteristics of static muscle stiffness in ankle plantar flexor muscles during the passive dorsiflexion of the ankle joint in individuals with CAI.
Methods
A total of 30 patients were included in the study based on the International Ankle Consortium criteria. The patients were categorized evenly into healthy, coper, and CAI groups (i.e., 10 patients in each group). After measuring the dorsiflexion range of motion (non-weight-bearing/weight-bearing) of the ankle joint, the static muscle stiffness measurements of the medial gastrocnemius, lateral gastrocnemius, soleus, and peroneus longus were obtained. The measurements were performed during the knee joint's extension and 50° flexion and passive dorsiflexion between the range of 40° plantar flexion and 20° dorsiflexion.
Results
The dorsiflexion range of motion of the CAI group was significantly smaller than that of the healthy and coper groups in the weight-bearing position. No interaction was observed for muscle stiffness in both the knee flexion and extension positions, and no significant differences were identified among the three groups. The shear modulus of the soleus at 20° ankle dorsiflexion with knee flexion had a significant negative correlation with the weight-bearing range of motion of the ankle.
Conclusion
The limitation in the weight-bearing dorsiflexion range of motion in CAI was largely due to factors other than the increased elasticity of the ankle plantar flexor muscles.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
An ankle sprain is one of the most common lower extremity injuries; it has a high recurrence rate, and recurrent ankle sprains lead to chronic ankle instability (CAI) [1]. Moreover, CAI causes a variety of structural and functional joint impairments, such as limited joint range of motion, muscle strength deficits, balance impairments, or arthritic degeneration, which lead to a decline in health-related quality of life and reduce physical activity [1, 2]. Furthermore, the complex pathogenesis of ankle sprains has led to a lack of consensus regarding optimal treatment. Therefore, an accurate understanding of the pathophysiology of CAI is important.
Recently published pathological models of CAI have demonstrated that CAI involves three major factors: pathomechanical impairments, sensory–perceptual impairments, and motor–behavioral impairments [1]. A deficit in the dorsiflexion range of motion of the ankle joint, which is categorized as a pathomechanical impairment, is associated with the occurrence and recurrence of ankle sprains [3, 4]. Additionally, a limited range of motion in ankle dorsiflexion is associated with decreased dynamic balance in CAI, and a limited range of motion may be associated with various pathologies of CAI [5, 6]. Although multiple factors, including the decreased extensibility of the plantar flexor muscles of the ankle joint [7] and abnormal arthrokinematics [8], are considered limiting factors in the dorsiflexion range of motion in CAI. However, the muscle stiffness of plantar flexors also plays a significant role during jump landing or running, particularly in energy absorption and energy generation, and a role as potential dynamic stabilizers at the ankle joint [9, 10]. Nevertheless, the cause of limitations in ankle dorsiflexion during loading movements in CAI is not fully understood.
Abnormal muscle stiffness is one of the most common causes of limited range of motion of the joint [11]. Recently, the usefulness of the muscle shear modulus as an indicator of muscle stiffness in shear wave elastography (SWE) has been reported [12, 13]. The muscle shear modulus has a strong linear relationship to passive force during the passive stretching of a muscle [14], and is related to diseases resulting in limitations in joint range of motion [15]. However, to our knowledge, the muscle stiffness of the ankle plantar flexors in CAI with limitations in ankle dorsiflexion range of motion has not been characterized.
We aimed to elucidate the characteristics of static muscle stiffness of the ankle plantar flexor muscle during the passive dorsiflexion of the ankle joint in individuals with CAI.
Materials and methods
The study protocol was approved by the ethics committee of the principal investigator’s institution. Before participation, all subjects signed an informed consent form that was approved by the Institutional Review Board (CR17009).
Subjects
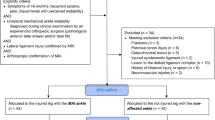
A power analysis with an alpha error of 0.05, power of 0.80, and effect size of 0.65 was performed using G*Power 3.1.9.2 analysis software (Heinrich Hein University, Duesseldorf, Germany); the aforementioned parameters were based on a previous study [16] that compared the ankle dorsiflexion range of motion of healthy participants with that of participants with CAI. The analysis produced a minimum total sample size of nine per group. Additionally, 244 healthy university students answered a questionnaire regarding their history of ankle sprains. On the basis of the questionnaire results, the healthy group was defined as those with no history of bilateral ankle sprains. The CAI selection criteria were based on the recommendations of the International Ankle Consortium [17]. In other words, copers were defined as those with a Cumberland ankle instability tool (CAIT) [18] score of 25 or higher and without symptoms within the past 12 months. Participants with a CAIT score of 24 or lower were categorized into the CAI group. Among the 53, 16, and 22 participants in the healthy, coper, and CAI groups, respectively, 10 participants from each group who gave their consent to participate in the study were included. To eliminate the influence of gender effects related to muscle stiffness [19], the sex ratio was standardized as much as possible.
Protocol
All participants underwent measurements for ankle dorsiflexion range of motion, followed by measurements for static muscle stiffness. All measurements were performed by a single examiner with 10 years of ultrasound experience.
Range of motion
The non-weight-bearing dorsiflexion range of motion of the ankle joint was measured once in 1° increments using a goniometer (KO goniometer; Tsutsumi, Tokyo, Japan) in the supine position with knee extension and 50° flexion. The weight-bearing dorsiflexion range of motion of the ankle joint was measured using the weight-bearing lunge test (WBLT) (Fig. 1). The subject performed dorsiflexion by flexing the knee toward the wall, and the maximum distance at which the knee could come into contact with the wall (wall-to-toe distance) was measured using a tape measure (PM-1320 KD; Niigata Seiki, Niigata, Japan) [20, 21].

The weight-bearing lunge test
Static muscle stiffness
Four muscles were tested: the medial gastrocnemius (MG), lateral gastrocnemius (LG), soleus (SOL), and peroneus longus (PL). The shear elastic modulus of the muscle was measured using SWE with a 2–10-MHz linear ultrasound transducer (Aixplorer Ver. 6 and SL10-2; Supersonic Imagine, Aix-en-Provence, France). The SWE system was set up as follows: the clinical preset was set in the musculoskeletal mode with a B-scan depth of 3.5 cm and a frequency range of 2–10 MHz. The SWE Opt was set in penetration mode with an elastogram frame rate of 1.4 Hz. The persistence was set to high, the opacity was set to 100%, and the smoothing of SWE was set to five. Young’s modulus ranged from 0 to 300 kPa. The blue and red colors in the color scale used for Young’s modulus (in kPa) corresponded to the lowest and highest values, respectively. The measurement site for each muscle was determined according to the methods of previous studies that used similar techniques [22], i.e., MG and LG were set at 30% proximal to the long axis of the lower leg, SOL was set at 50%, and PL was set at 20% proximal [22]. The probe was placed in the direction of the long axis of the muscle, and the clearest fascial region for each site was selected without visualizing any structures other than the fascia, such as blood vessels or intramuscular tendon areas. An acoustic gel (SONO JELLY Hard; Canon Medical Supply, Ltd., Tokyo, Japan) was used in each region as an interface between the probe and skin. The probe was gently held over the skin without applying pressure.
Static muscle stiffness measurements were performed in the knee joint during extension and flexion with the foot immobilized using BIODEX System 3 Pro (Shirley, NY, USA). Knee joint extension was measured in the supine position, and its flexion was measured using the BIODEX system set at a seat angle of 55° with the participant sitting squarely against the seat surface to achieve a knee joint flexion angle of 50° (Fig. 2). For each measurement, the participant performed passive dorsiflexion with an angular velocity of 2°/s from 40° of plantar flexion to 20° of dorsiflexion, as in the previous study [22]. The order of measurement of the knee joint position and tested muscles was randomized. Moreover, SWE images were saved at 2 Hz in BMP format (width: 1680 pixels; height: 1050 pixels; resolution: 72 dpi) for imaging analysis using a capture board (Epiphan video DVI2USB 3.0; Argo Co., Ltd., Osaka, Japan) and a capture tool (Epiphan Capturetool Ver. 3.30; Argo Co., Ltd., Osaka, Japan) (Fig. 3).

Testing position. ext. extension, flex. flexion, PF plantar flexion, DF dorsiflexion

Shear wave elastography images. MG medial gastrocnemius, LG lateral gastrocnemius, SOL soleus, PL peroneus longus, PF plantar flexion, DF dorsiflexion
Electromyography
Electromyography (EMG) was used to confirm the static state of the muscles during ankle dorsiflexion. A surface EMG (Telemaior DTS EM-801, Noraxon) and electrode pads (M-00-s/50) were used to measure muscle activity in each test and the tibialis anterior muscle. The electrode application site was set according to Surface EMG for Non-Invasive Assessment of Muscles (SENIAM) [23], and the distance between electrodes was 2 cm. Additionally, before the electrodes were applied, the skin was shaved, rubbed, and cleaned with alcohol. After muscle stiffness measurements, the participants performed maximal voluntary contractions (MVICs) for each muscle under isometric conditions according to the manual muscle test [24] to normalize the EMG.
Data analysis
The shear waves were generated by SWE within the soft tissue, and Young’s modulus was quantified in kPa based on the shear wave propagation velocity c. Young’s modulus (E) was color mapped to a 10 mm × 10 mm region of interest (ROI) in each fascial region. For each pixel of the ROI, Young’s modulus (E) was calculated (E = 3ρc2), where ρ is the muscle mass density (1000 kg/m3). In this device, Young’s modulus was obtained by applying a constant of three and with the assumption that the soft tissue was isotropic; however, the skeletal muscle could not be assumed isotropic. Therefore, the obtained Young’s modulus (E) was divided by three to obtain the shear modulus [25].
An elastic image analysis program (S-17115 Ver. 1.3.0; Takei Scientific Instruments Co., Ltd., Niigata, Japan) was used to analyze the shear modulus [26]. Moreover, SWE image (BMP) processing converted each pixel of the color map into a shear modulus value based on the recorded color scale. A rectangular region (10 mm wide and 5 mm high) containing clear fascia without connective tissue was selected, and the spatial average of the shear modulus of the selected region was calculated in kPa. The shear modulus was compared among the three groups at every 10° ankle joint angle.
All sections of the myoelectric signals were sampled, excluding the pulse noise (frequency of occurrence: approximately 1 Hz) due to SWE, and were filtered using a low-pass filter (cut-off frequency: 10 Hz). The muscle activity rate was obtained by dividing the root mean square during each passive ankle dorsiflexion by that during MVIC.
Statistical analysis
The Kruskal–Wallis test was used to compare the age, height, body weight, and ankle dorsiflexion range of motion among the three groups. Adjusted significance probabilities were obtained for the differences between groups using the Dunn–Bonferroni method. The sex ratio between the three groups was compared using Fisher’s exact test. Repeated-measures two-way analysis of variance (group × angle) was used to compare the muscle activity rate and muscle stiffness, and the Bonferroni method was used for post hoc tests. Pearson’s correlation analysis was used to examine the correlation between the ankle dorsiflexion range of motion (knee extension, knee flexion, and WBLT) and the static muscle stiffness of each muscle at 20° ankle dorsiflexion. SPSS software (version 25.0; SPSS, Chicago, IL, USA) was used for the statistical analysis, and a significance level of less than 5% was considered statistically significant.
Results
Physical characteristics and range of motion
Sex, age, height, and body weight were not significantly different among the three groups (Table 1). No significant difference in the dorsiflexion range of motion of the ankle joint in the non-weight-bearing position among the three groups was observed. By contrast, the dorsiflexion range of motion of the CAI group was significantly smaller than that of the healthy and coper groups in the weight-bearing position. Moreover, no significant difference in the ankle plantar flexion range of motion among the three groups was observed (Table 2).
Muscle activity rate
Very low muscle activity rates (less than 2.12 ± 0.8%) were observed in all muscles. No significant main effect of angle or group on any of the muscles was identified.
Static muscle stiffness
A main effect of angle was observed for all muscles (p < 0.001), and the shear modulus increased significantly during dorsiflexion. No interaction was observed for any of the muscles in both knee flexion and extension, and no significant differences were identified among the three groups (Fig. 4). The shear modulus of SOL at 20° ankle dorsiflexion with knee flexion had a significant negative correlation (p = 0.001, r = − 0.556) with the WBLT (Fig. 5). No significant correlations were found between the ankle dorsiflexion range of motion and the other muscles (Figs. 6 and 7).

Static muscle stiffness. MG medial gastrocnemius, LG lateral gastrocnemius, SOL soleus, PL peroneus longus, PF plantar flexion, DF dorsiflexion, n.s. no significance

Relationship between shear modulus at 20° ankle dorsiflexion and WBLT. WBLT weight-bearing lunge test

Relationship between shear modulus at 20° ankle dorsiflexion and ankle dorsiflexion range of motion in the knee extension position. DF dorsiflexion, ROM range of motion

Relationship between shear modulus at 20° ankle dorsiflexion and ankle dorsiflexion range of motion in the knee flexion position. DF dorsiflexion, ROM range of motion
Discussion
We compared the shear modulus of the ankle plantar flexor muscle group during passive dorsiflexion of the ankle joint of 10 subjects in the healthy, coper, and CAI groups to clarify the characteristics of the static muscle stiffness of the ankle plantar flexor muscle group in CAI. The results demonstrated that the CAI group had a significantly smaller weight-bearing dorsiflexion range of motion than the healthy and coper groups; however, no significant differences were observed in the static muscle stiffness of the ankle plantar flexor ankle muscles between the groups.
In the three groups, ankle plantar flexors exhibited a significant increase in muscle stiffness with ankle dorsiflexion. Studies have demonstrated that the muscle shear modulus increases with muscle lengthening in several muscles, including the MG and SOL muscles [11, 22, 26,27,28,29,30]. The results of the current study also reflected passive force, because the shear modulus increased with passive elongation.
The results confirmed that there was no significant increase in the static muscle stiffness of the plantar flexor ankle muscles in the CAI group with a limitation in the weight-bearing ankle dorsiflexion range of motion. By contrast, SOL elasticity during ankle dorsiflexion in the knee flexion position exhibited a significant negative correlation with the ankle dorsiflexion range of motion in the weight-bearing position. Several studies have shown that restrictions on the ankle joint dorsiflexion range of motion occur after an ankle sprain [31, 32], and the limitation might lead to the reduced flexibility of the plantar flexor ankle muscles owing to abnormal kinematics patterns [33]. Therefore, studies have demonstrated that patients with CAI have a limited dorsiflexion range of motion of the ankle joint during weight-bearing, and ankle dorsiflexion range of motion testing using WBLT is recommended in the rehabilitation of patients with CAI [3, 4]. Given that the decreased extensibility of the plantar flexor muscles of the ankle joint may be a limiting factor in the dorsiflexion range of motion, improvement of the flexibility of the muscles may be used as a treatment method for CAI [7, 34, 35]. The results of the current study suggest that a therapeutic intervention such as stretching while in the knee flexion position to improve the selective elasticity of the SOL is effective in improving the weight-bearing ankle dorsiflexion range of motion in CAI.
Given that CAI causes abnormal joint alignment and kinematics such as anterior displacement and excessive internal rotation of the talus [36,37,38], manual mobilization is assumed to improve the dorsiflexion range of motion, dynamic balance, and self-reported function in CAI [6, 8, 39]. In addition, CAI is associated with a variety of joint pathologies, including synovitis, cartilage damage, and soft-tissue impingement [1]. The current study demonstrated no significant differences in ankle plantar flexor stiffness between healthy individuals and patients with CAI, and limitations in weight-bearing ankle dorsiflexion range of motion were observed. The results suggested that abnormal arthrokinematics or other types of plantar flexor muscle stiffness, such as flexor hallucis longus, were also involved in the limitations in weight-bearing ankle dorsiflexion in patients with CAI. Therefore, rehabilitation to improve the dorsiflexion range of motion of the ankle joint in CAI should aim not only to stretch the plantar flexor muscles but also to improve joint alignment and kinematics via manual therapy and other interventions. In addition, imaging evaluations using ultrasound or magnetic resonance imaging for intra-articular lesions causing joint impingement may also be important.
This study had some limitations. First, static muscle stiffness was measured only in the non-weight-bearing position. Measurement of muscle elasticity during weight-bearing may show a different trend; therefore, this topic should be considered in future research. Second, as this study was conducted in young adults, different results may be observed in middle-aged and older patients with CAI and significant dorsiflexion limitations. Third, previous studies examining sex differences in the muscle elastic modulus of the MG and SOL muscles have shown some sex differences in the elastic modulus; however, a consensus has not been reached [40,41,42]. Although the current study did not identify significant differences between the sexes, it may be necessary in the future to examine the sexes separately. Finally, we were unable to evaluate the presence or absence of ligamentous injuries, such as the anterior talofibular ligament, in the CAI and coper groups. Future studies should examine the characteristics of muscle elasticity in subjects with and without ligamentous injuries.
Conclusion
We compared the shear modulus of the ankle plantar flexor muscle groups during passive ankle dorsiflexion in the healthy, coper, and CAI groups. The results demonstrated that there were no significant differences in the static muscle stiffness of the MG, LG, SOL, and PL muscles between the three groups. The limitations in the weight-bearing dorsiflexion range of motion in CAI were thought to be largely due to factors other than the increased elasticity of the ankle plantar flexor muscles.
Data availability
Authors are prepared to release data upon request.
References
Hertel J, Corbett RO. An updated model of chronic ankle instability. J Athl Train. 2019;54:572–88.
Houston MN, Hoch JM, Hoch MC. Patient-reported outcome measures in individuals with chronic ankle instability: a systematic review. J Athl Train. 2015. https://doi.org/10.4085/1062-6050-50.9.01.
Martin RL, Davenport TE, Fraser JJ, et al. Ankle stability and movement coordination impairments: lateral ankle ligament sprains revision 2021. J Orthop Sports Phys Ther. 2021;51:CPG1–80.
Vuurberg G, Hoorntje A, Wink LM, et al. Diagnosis, treatment and prevention of ankle sprains: update of an evidence-based clinical guideline. Br J Sports Med. 2018;52:956.
Gabriner ML, Houston MN, Kirby JL, et al. Contributing factors to star excursion balance test performance in individuals with chronic ankle instability. Gait Posture. 2015;41:912–6.
Weerasekara I, Osmotherly P, Snodgrass S, et al. Clinical benefits of joint mobilization on ankle sprains: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2018;99:1395-1412 e5.
Handoll HH, Rowe BH, Quinn KM, et al. Interventions for preventing ankle ligament injuries. Cochrane Database Syst Rev. 2001;3: CD000018.
Doherty C, Bleakley C, Delahunt E, et al. Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med. 2017;51:113–25.
Judson LJ, Churchill SM, Barnes A, et al. Joint moments and power in the acceleration phase of bend sprinting. J Biomech. 2020;101: 109632.
Weinhandl JT, Smith JD, Dugan EL. The effects of repetitive drop jumps on impact phase joint kinematics and kinetics. J Appl Biomech. 2011;27:108–15.
Maisetti O, Hug F, Bouillard K, et al. Characterization of passive elastic properties of the human medial gastrocnemius muscle belly using supersonic shear imaging. J Biomech. 2012;45:978–84.
Koo TK, Guo JY, Cohen JH, et al. Relationship between shear elastic modulus and passive muscle force: an ex-vivo study. J Biomech. 2013;46:2053–9.
Liu J, Qian Z, Wang K, et al. Non-invasive quantitative assessment of muscle force based on ultrasonic shear wave elastography. Ultrasound Med Biol. 2019;45:440–51.
Eby SF, Song P, Chen S, et al. Validation of shear wave elastography in skeletal muscle. J Biomech. 2013;46:2381–7.
Le Sant G, Nordez A, Hug F, et al. Effects of stroke injury on the shear modulus of the lower leg muscle during passive dorsiflexion. J Appl Physiol (1985). 2019;126:11–22.
Kobayashi T, Watanabe K, Ito T, et al. The Effect of novel ankle-realigning socks on dynamic postural stability in individuals with chronic ankle instability. Int J Sports Phys Ther. 2019;14:264–72.
Gribble PA, Delahunt E, Bleakley C, et al. Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the International Ankle Consortium. Br J Sports Med. 2014;48:1014–8.
Hiller CE, Refshauge KM, Bundy AC, et al. The Cumberland ankle instability tool: a report of validity and reliability testing. Arch Phys Med Rehabil. 2006;87:1235–41.
Morse CI. Gender differences in the passive stiffness of the human gastrocnemius muscle during stretch. Eur J Appl Physiol. 2011;111:2149–54.
Bennell KL, Talbot RC, Wajswelner H, et al. Intra-rater and inter-rater reliability of a weight-bearing lunge measure of ankle dorsiflexion. Aust J Physiother. 1998;44:175–80.
Powden CJ, Hoch JM, Hoch MC. Reliability and minimal detectable change of the weight-bearing lunge test: a systematic review. Man Ther. 2015;20:524–32.
Le Sant G, Nordez A, Andrade R, et al. Stiffness mapping of lower leg muscles during passive dorsiflexion. J Anat. 2017;230:639–50.
Hermens HJ, Freriks B, Disselhorst-Klug C, et al. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol. 2000;10:361–74.
Hislop HJ, Avers D, Brown M. Daniels and Worthingham’s muscle testing: techniques of manual examination and performance testing. 10th ed. St. Louis: Elsevier; 2018.
Shiina T. JSUM ultrasound elastography practice guidelines: basics and terminology. J Med Ultrason. 2013;40:309–23.
Kodesho T, Taniguchi K, Kato T, et al. Intramuscular differences in shear modulus of the rectus femoris muscle during passive knee flexion. Eur J Appl Physiol. 2021;121:1441–9.
Freitas SR, Antunes A, Salmon P, et al. Does epimuscular myofascial force transmission occur between the human quadriceps muscles in vivo during passive stretching? J Biomech. 2019;83:91–6.
Hug F, Lacourpaille L, Maisetti O, et al. Slack length of gastrocnemius medialis and Achilles tendon occurs at different ankle angles. J Biomech. 2013;46:2534–8.
Koo TK, Guo JY, Cohen JH, et al. Quantifying the passive stretching response of human tibialis anterior muscle using shear wave elastography. Clin Biomech (Bristol, Avon). 2014;29:33–9.
Xu J, Hug F, Fu SN. Stiffness of individual quadriceps muscle assessed using ultrasound shear wave elastography during passive stretching. J Sport Health Sci. 2018;7:245–9.
Denegar CR, Hertel J, Fonseca J. The effect of lateral ankle sprain on dorsiflexion range of motion, posterior talar glide, and joint laxity. J Orthop Sports Phys Ther. 2002;32:166–73.
Tabrizi P, McIntyre WM, Quesnel MB, et al. Limited dorsiflexion predisposes to injuries of the ankle in children. J Bone Joint Surg Br. 2000;82:1103–6.
Terada M, Pietrosimone BG, Gribble PA. Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: a systematic review. J Athl Train. 2013;48:696–709.
Pope R, Herbert R, Kirwan J. Effects of ankle dorsiflexion range and pre-exercise calf muscle stretching on injury risk in Army recruits. Aust J Physiother. 1998;44:165–72.
Youdas JW, Krause DA, Egan KS, et al. The effect of static stretching of the calf muscle-tendon unit on active ankle dorsiflexion range of motion. J Orthop Sports Phys Ther. 2003;33:408–17.
Caputo AM, Lee JY, Spritzer CE, et al. In vivo kinematics of the tibiotalar joint after lateral ankle instability. Am J Sports Med. 2009;37:2241–8.
Kobayashi T, Saka M, Suzuki E, et al. In vivo kinematics of the talocrural and subtalar joints during weightbearing ankle rotation in chronic ankle instability. Foot Ankle Spec. 2014;7:13–9.
Kobayashi T, Suzuki E, Yamazaki N, et al. Fibular malalignment in individuals with chronic ankle instability. J Orthop Sports Phys Ther. 2014;44:872–8.
Powden CJ, Hoch JM, Hoch MC. Rehabilitation and improvement of health-related quality-of-life detriments in individuals with chronic ankle instability: a meta-analysis. J Athl Train. 2017;52:753–65.
Chino K, Takahashi H. Measurement of gastrocnemius muscle elasticity by shear wave elastography: association with passive ankle joint stiffness and sex differences. Eur J Appl Physiol. 2016;116:823–30.
Miyamoto N, Hirata K, Miyamoto-Mikami E, et al. Associations of passive muscle stiffness, muscle stretch tolerance, and muscle slack angle with range of motion: individual and sex differences. Sci Rep. 2018;8: 8274.
Saeki J, Ikezoe T, Yoshimi S, et al. Menstrual cycle variation and gender difference in muscle stiffness of triceps surae. Clin Biomech (Bristol, Avon). 2019;61:222–6.
Acknowledgements
The study was supported by the Japan Society for the Promotion of Science (Grant No. 19K19916).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Ethical statements
The study protocol was approved by the ethics committee of the author’s institution.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Kobayashi, T., Kodesho, T., Kinami, K. et al. Characteristics of the static muscle stiffness of ankle plantar flexors in individuals with chronic ankle instability. J Med Ultrasonics 50, 561–570 (2023). https://doi.org/10.1007/s10396-023-01360-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10396-023-01360-5