
Abstract
Intracranial aneurysms (IA) occur in 3–5% of the general population and may require surgical or endovascular obliteration if the patient is symptomatic or has an increased risk of rupture. These procedures carry an inherent risk of neurological complications, and the outcome can be influenced by the physiological and pharmacological effects of the administered anesthetics. Despite the critical role of anesthetic agents, however, there are no current studies to systematically assess the intraoperative anesthetic risks, benefits, and outcome effects in this population. In this systematic review of the literature, we carefully examine the existing evidence on the risks and benefits of common anesthetic agents during IA obliteration, their physiological and clinical characteristics, and effects on neurological outcome. The initial search strategy captured a total of 287 published studies. Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, 28 studies were included in the final report. Our data showed that both volatile and intravenous anesthetics are commonly employed, without evidence that either is superior. Although no specific anesthetic regimens are promoted, their unique neurological, cardiovascular, and physiological properties may be critical to the outcome in vulnerable patients. In particular, patients at risk for perioperative ischemia may benefit from timely administration of anesthetic agents with neuroprotective properties and optimization of their physiological parameters. Further studies are warranted to examine if these anesthetic regimens can reduce the risk of neurological injury and improve the overall outcome in these patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Anesthesia for UIA obliteration differs from routine craniotomies because of specific physiological challenges associated with the underlying neurovascular disease and the planned procedure. The margin of safety between high blood pressure leading to rupture and a low blood pressure provoking ischemia is narrow in these patients; hence, immediate management of hypertensive or hypotensive events is critical. Moreover, the anesthesiologist must balance the need to maintain cerebral perfusion pressure (CPP) to promote brain oxygenation with the risk of increasing the transmural pressure gradient that can promote aneurysm rupture [1, 2] (Fig. 1). Respiratory parameters must be carefully titrated to optimize oxygenation and carbon dioxide tension; coagulation and electrolyte balance, maintained; and intraoperative events and complications, rapidly managed to prevent risk for devastating neurological injuries (Fig. 2). Procedure-related challenges such as temporary occlusion of the parent vessel require special anesthetic consideration. Temporary clipping of the parent vessel may be needed to rescue or preempt IA rupture or to facilitate a surgical step in elective IA surgeries. However, temporary clipping can lead to ischemic stroke, dissection of the vessel, or rupture of the aneurysm [3,4,5]. Prolonged occlusion of the parent vessel leads to extended hypoperfusion in its corresponding territory; therefore, proper anesthetic management such as careful blood pressure augmentation and neuroprotection may be warranted. Various anesthetic agents reduce cerebral metabolism—as listed in this review—and, therefore, could be considered. However, it is essential to choose an anesthetic approach that preserves or ideally even augments cerebral blood flow (CBF)—in particular collateral flow to the ischemic territory—while reducing cerebral metabolic rate of oxygen (CMRO2) (Table 1). Since temporary clipping during IA surgery may provoke cerebral vasospasm, cerebral function monitoring may be employed to guide blood pressure management and removal or reapplication of the temporary clip.

Systemic blood pressure should be monitored closely and controlled to minimize risk of aneurysm rupture due to hypertension while avoiding low blood pressure that can provoke cerebral ischemia. BP blood pressure, CPP cerebral perfusion pressure, ICP intracranial pressure, CBF cerebral blood flow

Anesthetic considerations during obliteration of UIA (unruptured intracranial aneurysms)
In some patients, it may become necessary to induce a transient circulatory arrest or severe hypotension in case of an aneurysm rupture or for decompression of the aneurysm to facilitate clip application. With appropriate safety precautions, adenosine boluses of up to 30 mg have been successfully used to induce a transient asystole in these patients [5]. Adenosine may also be considered when temporary clipping of proximal vessels is not desirable or possible. Although some recent reviews provide general guidelines on the anesthetic management of cerebral aneurysm surgery [1, 2, 8], there are no rigorously conducted studies or reviews to assess the intraoperative anesthetic risks and outcome effects for UIA obliteration. Therefore, we conducted a systematic review of the literature examining the hemodynamic, physiological and pharmacological effects of common anesthetic agents and regimens during endovascular and open procedures to obliterate UIA.
Methods
Study selection
All articles in English language, including adult patients, and published in indexed scientific journals were considered. Randomized controlled trials (RCT), prospective and retrospective cohorts, case series, and case reports, as well as cross-sectional studies involving patients with unruptured cerebral aneurysm or those who had undergone aneurysm obliteration or neurosurgical procedures were eligible for inclusion. Given the scarcity of studies on unruptured cerebral aneurysms, we also discuss relevant findings from selective studies on neurological effects of anesthetics and patients with aneurysmal subarachnoid hemorrhage.
Data extraction
We performed a systematic search on MEDLINE to identify studies. We used the participants, interventions, comparisons, and outcomes (PICO) search tool [9] to determine the following medical subject heading terms: “Aneurysm OR Aneurysm Surgery” AND “Nitrous Oxide OR Isoflurane OR Desflurane OR Sevoflurane OR Ketamine OR Propofol OR Barbiturate OR Thiopental OR Dexmedetomidine OR Opioids” AND “brain OR intracranial OR cerebral OR cranium” AND “Surgery OR Neurosurgery OR craniotomy OR endovascular OR Vascular Surgical Procedures” AND “Neuroprotection OR mortality OR morbidity” AND “anesthetics OR anesthesia.” Additional reports were identified from reference lists of retrieved reports and Google Scholar searches.
Method of synthesis
Two reviewers independently extracted the data from trial reports, with adherence to the PRISMA guideline [10]. Details of the patient population, type of surgery, anesthetic regimen, and outcomes were recorded. The data were extracted only from studies published in English.
Results of the review
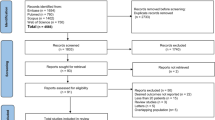
The initial search strategy captured a total of 287 studies. From these, 28 studies were included in this study (Table 2 and Fig. 3) [10].

PRISMA flow diagram showing the process of study inclusion
Anesthesia for cerebral aneurysms: intravenous or inhalational agents?
There is currently no clear consensus whether intravenous anesthesia, inhalational anesthesia, or a combination thereof should primarily be used for surgical or endovascular management of UIA. Inhalational agents commonly used for these procedures include volatile anesthetic agents such as isoflurane, desflurane, and sevoflurane, as well as nitrous oxide. Commonly used intravenous agents include propofol, ketamine, and dexmedetomidine, which are typically administered in combination with a short- or long-acting opioids. Thiopental sodium and other barbiturates are still used in certain countries, and benzodiazepines are also occasionally administered as perioperative anxiolytics or anesthetic adjuncts.
There are conflicting data on not only the perioperative risks and benefits of these agents, including direct neurotoxic effects or physiological side effects that can alter the outcome of the procedure, but also their neuroprotective properties, which become essential in cerebral aneurysm surgery due to the potential neurological insults associated with these complex procedures.
Inhalational anesthesia
Nitrous oxide
While nitrous oxide (N2O) has been used continuously in clinical anesthesia for about 180 years, discussions about its neurological effects are still ongoing [39]. In 1992, Lam et al. described the important physiological effects of N2O on cerebral metabolism and intracerebral steal [40]. Although little research has been carried out on the neurophysiological properties of N2O, it is now generally accepted that N2O lacks neuroprotective effects in anesthetic doses [41]. Furthermore, N2O is known to increase cerebral metabolism, CBF, and intracranial pressure (ICP) and can potentially exacerbate an ischemic insult, all undesirable effects in the setting of intracranial surgery [42].
The debate on N2O safety has continued to simmer, mainly without any clinical neurological outcome data [42, 43]. In 2008, McGregor et al. assessed the clinical outcomes associated with N2O by analyzing the Intraoperative Hypothermia for Aneurysm Surgery Trial (IHAST) data [11]. They evaluated neurological outcomes at two weeks (i.e., delayed ischemic neurologic deficit (DIND)) and three months after aneurysm surgery and found that in a population of patients potentially at risk for ischemic injury, the use of N2O had no overall impact on neurological outcome [11]. A subgroup analysis of patients with temporary occlusion of a major cerebral artery for permanent clipping of the aneurysm provided a more granular analysis to capture patients who experienced ischemic events intraoperatively during exposure to N2O. In this subgroup, intraoperative N2O administration was associated with an increased risk of DIND. The long-term neurological outcome was, nevertheless, not affected [12].
To our knowledge, data from more recent studies assessing the effects of N2O on neurological outcome after UIA surgery are lacking [8]. Although intraoperative use of N2O is primarily based on the anesthetist’s preference and differs between institutions, most experts agree that it is best avoided during endovascular procedures. In addition to its effects on CBF and ICP, it is well known that N2O increases the risk of expansion of micro air bubbles in enclosed spaces. This expansion is due to N2O’s low potency, which results in high blood concentrations, and its low blood/gas partition coefficient, which causes N2O to move into an air compartment faster than air moves out. Air embolization is rare during aneurysm obliteration but can happen during contrast injection or fluid irrigation; expansion of these air bubbles with N2O can augment the risk for tissue ischemia and neurological injury [44]. Furthermore, it may be reasonable to avoid N2O during open craniotomy for UIA clipping if it is difficult to achieve sufficient brain relaxation, or in patients with disrupted autoregulation, such as those with cerebral edema, ischemia, or vasospasm [45].
Isoflurane
Isoflurane is commonly used in neuroanesthesia due to its modest effects on CBF and cerebral autoregulation [46]. The neuroprotective effects of isoflurane have been studied widely in animal models. Isoflurane administration in rats during reperfusion after ischemia reduces brain injury, improves neurological outcome, and decreases neuronal apoptosis [47].
Isoflurane is generally associated with good blood pressure control without significant change in cardiac output or reflex tachycardia when administered in anesthetic concentrations to normovolemic patients [48]. To further evaluate the cerebral effects of isoflurane, Madsen et al. measured CBF and CMRO2 during isoflurane-induced controlled hypotension in ten patients undergoing craniotomy for clipping of a ruptured aneurysm. CBF and CMRO2 were measured 5–13 days after aSAH. Controlled hypotension to an average mean arterial pressure (MAP) of 50–55 mmHg was induced by increasing the inspired concentration of isoflurane, which resulted in a significant decrease in CMRO2 but no change in CBF. After clipping, the isoflurane concentration was reduced, and there was a significant increase in CBF. While CMRO2 returned to baseline, CBF increased above its pre-hypotensive value. It was suggested that this advantageous supply-demand ratio can offer protection to the brain tissue during periods of induced hypotension [49]. Following prior clinical studies that emphasized the use of high concentrations of isoflurane to induce hypotension, decrease CMRO2, and stabilize CBF, Meyer et al. used end-tidal isoflurane concentrations of 2.0 to 2.5 × minimum alveolar concentration (MAC) to induce electroencephalographic (EEG) ISO electricity (see below). At these high isoflurane concentrations, hypotension can occur due to myocardial depression and vasodilatation; therefore, a vasopressor agent was used to maintain blood pressure. The study included six patients with aSAH and extended temporary vessel occlusion time. Five of six patients made a good recovery despite prolonged occlusion of major cerebral arteries. Their findings supported the use of high dose isoflurane in selective patients to suppress cerebral metabolism during aneurysm surgery, as long as it is hemodynamically tolerated and when intraoperative EEG monitoring is used to carefully titrate the anesthetic concentration [15]. However, it should be noted that prolonged inhalation of isoflurane may reverse its protective effects, as was demonstrated by an aggravated brain injury in a rat model of transient focal ischemia [50].
Although more recent clinical studies looking at isoflurane for UIA surgeries are lacking, in 2019, a retrospective analysis of seven aSAH patients who underwent decompressive craniectomy due to a critically elevated ICP showed that deep sedation could rapidly be achieved after induction of general anesthesia with isoflurane, without a critical increase in ICP. Adequate CPP was also achieved without a need for extended vasopressor treatment [51].
Sevoflurane
The general neurological profile of sevoflurane is largely comparable to isoflurane but with relatively smaller vasodilatory effects. At concentrations of 1 MAC or less, sevoflurane maintains global CBF (if MAP is unchanged), reduces CMRO2, and minimally increases ICP, which can be blunted by mild hyperventilation [52]. Supported by animal studies, it is argued that sevoflurane may induce neuroprotection when administered during traumatic or ischemic events [53, 54]. In 2018, Xu et al. reported that early exposure to 3.4% sevoflurane for 5 h induced not only autophagy in rat hippocampal cells but also apoptosis of neurons, potentially leading to spatial learning deficits [55], raising questions about the neuroprotective role of sevoflurane. The fact that this high concentration of sevoflurane is seldom used in clinical practice, particularly without other medications such as opioid analgesics or intravenous anesthetics, makes it impossible to determine the clinical relevance of their findings. In fact, it is more likely that the co-administration of intraoperative anesthetics influences their effects on cerebral metabolism, inflammation, and injury, as was demonstrated by Bo et al. in 2018. They showed that the addition of dexmedetomidine to sevoflurane anesthesia could suppress the sevoflurane-induced cell cycle arrest, inhibition of brain-derived neurotrophic factor (BDNF), and tropomyosin receptor kinase B (TrkB) expression and concluded that dexmedetomidine could be used to prevent or mitigate sevoflurane-induced neurotoxicity [56]. The use of dexmedetomidine during sevoflurane anesthesia was also studied in a randomized clinical trial of 120 patients undergoing intracranial aneurysm embolization, and the addition of dexmedetomidine resulted in better neuroprotection, decreased incidence of postoperative delirium, faster recovery, and more stable hemodynamics [22].
Due to its bronchodilatory effects and relatively short duration of action (low blood-gas solubility coefficient), sevoflurane may be the ideal volatile agent for patients with underlying chronic obstructive pulmonary disease (COPD, Table 3). Conversely, it may not be the agent of choice in patients with kidney disease, although clinical trials have failed to confirm clinically relevant effects on renal function when higher fresh gas flows are maintained. There is currently no consensus on the neuroprotective or neurotoxic effects of sevoflurane. Specific clinical studies of the use of sevoflurane in open clipping or endovascular repair of UIA are lacking, and further investigation is warranted.
Desflurane
With its low blood-gas solubility coefficient, desflurane has favorable pharmacokinetic properties relative to isoflurane, including a more rapid emergence from anesthesia and postoperative recovery of cortical functions that have been noted in several in vitro, animal, and human studies. [57]
Several clinical and animal studies have looked at the effects of desflurane on cerebral hemodynamics. The effects of desflurane on ICP were assessed in a porcine model of intracranial hypertension, and at 0.5 to 1 MAC, desflurane was associated with cerebral vasodilatation and higher ICP levels compared to isoflurane and sevoflurane [58]. In humans, the same vasodilatory effect was observed in patients given desflurane, but the ICP did not increase significantly [59]. Although desflurane’s cerebrovascular effects in patients with intracranial hypertension have not been thoroughly investigated, it is reasonable to avoid it in these patients to minimize the risk for significant vasodilation that could lead to ICP elevation [52, 60].
Evidence regarding the use of desflurane in aneurysm clipping is limited. In 2017, Lee et al. reported that the incidence of TCD-evident vasospasm in patients who underwent emergent clipping of cerebral aneurysms was higher with propofol as compared to desflurane, but the incidence of angiographic vasospasm, cerebral infarction, and interventions to treat vasospasm were similar between the groups [61]. Another study found that in patients undergoing intracranial aneurysm clipping, the plasma concentration of endothelin was lower when desflurane was used, suggesting a potential benefit in preventing acute cerebral vasospasm during aneurysm clipping [16].
The risks and benefits of desflurane should be considered carefully for each neurosurgical patients and procedure. As an example, given its association with adverse respiratory events, it may not be the ideal anesthetic agent in patients with severe asthma or COPD. While it has advantageous pharmacokinetic features, its physiological and neuroprotective properties are not superior to other common anesthetics, including sevoflurane and propofol. Although the associated side effects of desflurane remain theoretical or experimental, its physiological properties must be carefully considered during perioperative management of patients with UIA, especially those with poor brain relaxation or intracranial hypertension [62].
Intravenous anesthetic agents
Ketamine
The use of ketamine in neuroanesthesia, including UIA obliteration, is controversial. There is evidence that it may increase ICP, CBF, and CMRO2 [63]; however, more recent animal and human studies suggest that ketamine may actually be beneficial to brain-injured patients due to its effects on NMDA receptors [64, 65].
Based on data from relevant randomized trials between 1994 and 2004, a systematic review suggested that with controlled ventilation and co-administration of a GABA receptor agonist, ketamine can be safely administered without raising the ICP [66]. In another study of 20 patients who underwent craniotomy for either brain tumor resection or cerebral aneurysm clipping, ketamine did not increase ICP during isoflurane or N2O anesthesia. The same study also showed that middle cerebral artery blood flow velocity, mean arterial blood pressure (MAP), and bilateral fronto-occipital processed EEG remained stable after the administration of ketamine, suggesting it can be used safely during neurosurgical procedures [17].
Although clinical studies of ketamine use in the anesthetic management of UIA surgery are lacking, one retrospective, observational study published in 2016 found that among 65 patients with SAH, administration of ketamine decreased ICP and was not associated with a higher rate of neurological complications. This study also found that the rate of delayed cerebral ischemia (DCI)-associated cerebral infarction and the use of vasopressors for induced hypertension were lower when ketamine was administered [18]. Currently, ketamine is avoided in patients with elevated ICP, but based on available animal and human data, it may prove to be a valuable agent for UIA obliteration in the near future. A re-evaluation of its role in these patients is suggested, particularly in those who may benefit from its systemic effects (e.g., bronchodilation in patients with COPD).
Dexmedetomidine
Based on its favorable hemodynamic properties and an ability to attenuate the cardiovascular responses to intubation, pinning, and extubation, the introduction of dexmedetomidine was met with enthusiasm among clinicians. It significantly decreases both CBF and ICP [67, 68]. As an anesthetic adjunct, it decreases the amount of intravenous or volatile anesthetic agents required for induction and the need for opioid analgesics intraoperatively [69].
Dexmedetomidine is commonly used for intracranial procedures and cerebral aneurysm surgery. A retrospective analysis of 12 patients undergoing endovascular procedures for intracranial aneurysm management confirmed a stable hemodynamic profile when dexmedetomidine was used as an anesthetic adjunct. Vital signs and the Ramsey sedation scale for depth of sedation were analyzed every 10 min and showed no statistically significant differences between time points [21]. Another retrospective analysis of 49 patients admitted to the ICU after cerebral aneurysm surgery revealed a higher sedation level in the dexmedetomidine group, with only one patient requiring physical restriction as compared to ten controls [70]. Dexmedetomidine is effectively used in combination with other anesthetics such as sevoflurane to reduce the stress response during surgical clipping of intracranial aneurysms and has also been used in selected patients as the sole sedative agent during monitored anesthesia care for coil embolization of unruptured cerebral aneurysms [22]. Randomized trials with outcome data is, nevertheless, missing in this population.
Barbiturates
The neuroprotective properties of barbiturates have been well documented in many clinical settings, including status epilepticus and traumatic brain injury. Shapiro et al. described its effects on ICP reduction in 1973 [71]. Subsequent animal studies demonstrated its neuroprotective effects by reducing CBF, ICP, and CMRO2 [72, 73]. In humans, however, these effects have not consistently resulted in improved neurological outcomes. An RCT of 300 patients undergoing coronary artery bypass grafting (CABG) did not find a reduction in the incidence of postoperative neurological deficits with thiopental [74]. Another study of 182 CABG patients found that even though thiopental was associated with a significantly lower incidence of persistent neuropsychiatric complications, hemodynamic instability was more frequent, resulting in prolonged use of inotropic support [75].
Clinical studies of barbiturate usage in the UIA population are scarce. A study of 92 patients with cerebral aneurysms in which 23 received pentobarbitone during clipping showed that the complication rate was lower in the pentobarbital group (17%) than the non-barbiturate group (21%) [76]. A case report also documented how multiple thiopental boluses were used in a patient undergoing a combined procedure involving clipping of an intracerebral aneurysm and carotid endarterectomy with an encouraging clinical outcome and a rapid recovery with no postoperative neurological deficits reported [24].
Despite their suggested neuroprotective effects, barbiturates are rarely used in the perioperative setting because of a concern for adverse effects such as cardiorespiratory depression, prolonged duration of post-infusion clinical unresponsiveness, impaired white blood cell function, hypokalemia, and hepatic and renal dysfunction [77]. While this drug class should be used cautiously during cerebral aneurysm surgeries, it can result in satisfactory intraoperative conditions and good neurological outcomes if carefully administered.
Propofol
Because of its favorable hemodynamic, pharmacological, and physiological properties, propofol remains one of the most commonly used anesthetics for neurosurgical procedures, including endovascular and open approaches to securing intracranial aneurysms. It is well tolerated by most patients [78], and its hemodynamic effects are readily managed with common vasopressors. Propofol decreases CBF, CMRO2, and ICP and has been shown to have neuroprotective effects in various models of neuronal injury. Animal models have demonstrated its direct antioxidant properties that can protect against oxidative stress as well as anti-inflammatory and antiapoptotic properties [79, 80]. Its rapid recovery profile also allows the possibility of prompt neurological examination postoperatively.
Propofol has been evaluated in aneurysm surgery in multiple studies. In 1993, Ravussin et al. evaluated 42 patients, including seven with unruptured aneurysms, who underwent cerebral aneurysm clipping using total intravenous anesthesia with propofol. The propofol infusion rate was reduced postoperatively to allow for early recovery and subsequent neurological examination, and they concluded that using a propofol infusion for maintenance of burst suppression could be a suitable alternative to isoflurane for aneurysm clipping [25]. Similarly, Guo et al. randomized 60 patients undergoing intracranial aneurysm clipping to propofol post-conditioning or sevoflurane and found improved mini mental status exam (MMSE) and Montreal Cognitive Assessment (MoCA) scores seven days after their surgery [31].
Due to its cerebral vasoconstrictive effects, propofol is generally considered to be an ideal anesthetic for effective brain relaxation during aneurysm surgery. A 2014 meta-analysis by Chui et al. showed that propofol-based anesthesia was associated with lower initial ICP values compared to maintenance with volatile anesthetics; however, this finding did not translate into better brain relaxation scores [2, 81]. A more recent study of 15 patients undergoing elective surgery for UIA found that cerebral circulation times were longer during propofol anesthesia compared to sevoflurane-based anesthesia, as were the circulation times in the internal carotid and middle cerebral arteries [30]. The presence of an unruptured intracranial aneurysm also did not affect the propofol-induced reactivity of cerebral vessels [29]. Multiple studies have compared propofol to other anesthetics for neurovascular procedures [29,30,31], but most have focused on the hemodynamic or neuroprotective effects of propofol, with only limited data regarding its effects on neurological outcomes.
Opioids
Among opioid receptors, the delta-opioid receptor (DOR) has received special attention for its proposed neuroprotective properties. Early animal studies suggested that opioid receptor agonists could increase survival rates during cerebral ischemia [82]. Zhang et al. further elucidated this concept using neuronal cultures from rat neocortex while studying glutamate-induced neuronal injury. These investigators found that activation of DORs reduced injury by half, whereas mu- or kappa-opioid receptors did not [83]. DORs are suggested to provide neuroprotection by different mechanisms such as inhibiting excitatory neurotransmitter release, increasing antioxidant capacity, and stabilizing ionic homeostasis [84].
In humans, however, mu-opioid receptor agonists are more commonly used for analgesia during surgery. Their perioperative use is limited primarily due to their respiratory depressant effects, which can lead to hypercapnia with cerebral vasodilation and increased ICP. Fentanyl can decrease CBF and CMRO2, but if ventilation is not controlled, it can lead to hypercapnia and as a result an increase in ICP. Similarly, remifentanil can reduce CBF and CMRO2, and although it is not demonstrated to directly increase the ICP, it can also cause respiratory depression and hypercapnia that can result in cerebral vasodilation [85].
Evidence from clinical studies on the use of opioids in UIA is scarce; however, a few have shed light on the subject. Degoute et al. found that remifentanil in combination with propofol or an inhalational agent could produce reliable hypotension when needed for certain phases of aneurysm surgery [86]. In another study, Uchida et al. conducted a propensity score-matched analysis of more than four thousand patients who underwent open intracranial aneurysm clipping and found that the group who received remifentanil had significantly lower in-hospital mortality than controls [32]. Remifentanil can be a good adjunct to the anesthetic regimen if rapid recovery and postoperative neurological evaluation are desired or if opioid-induced respiratory depression is contraindicated (e.g., patients with severe COPD), but more clinical studies are needed to determine if its administration is associated with improved outcomes after UIA.
Discussion
Obliteration of UIA can result in devastating complications despite advances in surgical and endovascular techniques, careful preoperative optimization, and enhanced anesthetic and perioperative management of the patient. A thorough understanding of the anatomical features of the aneurysm, the technical approach, physiological and metabolic challenges, and the systemic and neurological effects of the anesthetic agents is crucial for reducing the risk of neurological injury in these patients. These cases also require preparedness for perioperative complications, and implementation of resuscitative and neuroprotective measures should these complications occur [87]. Animal and human studies have documented the neurophysiological and neuroprotective properties of common anesthetics, but there is only limited data regarding their effects on neurological outcomes, particularly in patients with UIA [41, 47, 62, 72, 73, 79, 80, 82, 88, 89]. Pharmacodynamic, cardiovascular, and neurophysiological effects of common anesthetics have been extensively studied, but not in the specific context of EVT or aneurysm clipping. Endovascular aneurysm coiling can be complicated by intra-procedural perforation by the microcatheter, guidewire, or coil [87]. Thromboembolic events or vasospasm can also occur and lead to cerebral ischemia with devastating neurological injury [90]. Intra-arterial vasodilators are sometimes administered, requiring careful titration of systemic vasopressors and anesthetics to avoid hypotension and cardiovascular collapse. Blood pressure fluctuations along with respiratory and other physiological parameters such as temperature and glucose levels must be meticulously controlled, and patient movement should be avoided [1, 2, 8]. Similar to EVT, successful open clipping of UIA is critically dependent on the perioperative control of hemodynamic perturbations, optimization of cerebral perfusion and metabolism, careful fluid management, and maintenance of cellular homeostasis. Blood pressure augmentation with common vasopressors such as phenylephrine may be required to improve the collateral blood supply by increasing the CPP and should be considered especially when the duration of temporary clipping is anticipated to exceed two minutes. Increasing brain tolerance for ischemia by pharmacologically inducing electroencephalogram (EEG) silence or burst suppression is another consideration. It is important to note, nevertheless, that despite supporting evidence in patients with prolonged (> 10 min) temporary clipping [91], pharmacological burst suppression or EEG silence is currently not recommended for routine use in cases with temporary arterial occlusion. Also, available literature provides limited data to support a specific anesthetic regimen, and our understanding of their physiological and outcome effects continues to evolve. It is unlikely that smaller trials will have the required power to identify significant outcome differences following uncomplicated procedures, as long as the above perioperative goals are met (Fig. 1). It is possible, however, that outcomes in a subgroup of patients at risk for perioperative neurological injury (e.g., those with aneurysm rupture, severe vasospasm, or prolonged temporary clipping) are critically dependent on the physiological and neuroprotective properties of the anesthetic agents used, in addition to perioperative hemodynamic, metabolic, and respiratory parameters [6, 7, 77, 92, 93]. This at-risk population would be an ideal target for future randomized trials to assess the protective effects of different anesthetic agents during UIA obliteration.
Conclusion
The existing literature does not support any specific anesthetic regimen during EVT or open craniotomy for the management of UIA. Further studies are needed to compare the perioperative physiological and clinical effects of different anesthetic regimens and define their influence on neurological outcomes.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
References
Bruder N, Boussen S, Velly L (2019) Anesthesia for aneurysmal subarachnoid hemorrhage. In: Prabhakar H, Ali Z. (eds) Textbook of neuroanesthesia and neurocritical care. Singapore: Springer Nature Singapore Pte Ltd, pp 115–130
Lecours M, Gelb AW (2015) Anesthesia for the surgical treatment of cerebral aneurysms. Rev Colom Anestesiol 43:45–51
Abd-Elsayed AA, Wehby AS, Farag E (2014) Anesthetic management of patients with intracranial aneurysms. Ochsner J 14(3):418–425
Malinova V, Schatlo B, Voit M, Suntheim P, Rohde V, Mielke D (2017) The impact of temporary clipping during aneurysm surgery on the incidence of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. J Neurosurg 129(1):84–90
Desai VR, Rosas AL, Britz GW (2017) Adenosine to facilitate the clipping of cerebral aneurysms: literature review. Stroke Vasc Neurol 2(4):204–209
Inhalational anesthetics. In: Butterworth JF, IV, Mackey DC, Wasnick JD. (eds) Morgan & Mikhail’s clinical anesthesiology, 5e. McGraw-Hill. https://accessmedicine.mhmedical.com/Book.aspx?bookid=2444. Accessed 22 Nov 2020
Drummond John C, Dao Andrew V, Roth David M, Cheng C-R, Atwater BI, Minokadeh A, Pasco LC, Patel PM (2008) Effect of dexmedetomidine on cerebral blood flow velocity, cerebral metabolic rate, and carbon dioxide response in normal humans. Anesthesiology 108(2):225–232. https://doi.org/10.1097/01.anes.0000299576.00302.4c
Chowdhury T, Petropolis A, Wilkinson M, Schaller B, Sandu N, Cappellani RB (2014) Controversies in the anesthetic management of intraoperative rupture of intracranial aneurysm. Anesthesiol Res Pract 2014:1–10
Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S (2014) PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv Res 14:579–579. https://doi.org/10.1186/s12913-014-0579-0
Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D, Antes G, Atkins D, Barbour V, Barrowman N, Berlin JA (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement (Chinese edition). J Chin Integrat Med 7(9):889–896
McGregor DG, William L, Pasternak J, Rusy D, Hogan K, Samra S, Hindman B, Todd MM, Schroeder DR, Bayman EO, Clarke W, Torner J, Weeks J (2008) Effect of nitrous oxide on neurologic and neuropsychological function after intracranial aneurysm surgery. Anesthesiology 108(4):568–579. https://doi.org/10.1097/ALN.0b013e31816721fa
Pasternak JJ, McGregor DG, Lanier WL, Schroeder DR, Rusy DA, Hindman B, Clarke W, Torner J, Todd MM (2009) Effect of nitrous oxide use on long-term neurologic and neuropsychological outcome in patients who received temporary proximal artery occlusion during cerebral aneurysm clipping surgery. Anesthesiology 110(3):563–573
Madsen JB, Cold GE, Hansen ES, Bardrum B, Kruse-Larsen C (1987) Cerebral blood flow and metabolism during isoflurane-induced hypotension in patients subjected to surgery for cerebral aneurysms. Br J Anaesth 59(10):1204–1207. https://doi.org/10.1093/bja/59.10.1204
Roth S, Jones SC, Ebrahim ZY, Friel H, Little JR (1989) Local cortical blood flow and oxygen consumption during isoflurane-induced hypotension. Results in patients undergoing intracranial aneurysm clipping. Cleve Clin J Med 56(8):766–770. https://doi.org/10.3949/ccjm.56.8.766
Meyer FB, Muzzi DA (1992) Cerebral protection during aneurysm surgery with isoflurane anesthesia. J Neurosurg 76(3):541–543
Wang T, Luo F, Shan R, Zhen Y, Zhao J, Zhang S (2004) Changes of endothelin and calcitonin gene-related peptide during desflurane anesthesia in patients undergoing intracranial aneurysm clipping. J Neurosurg Anesthesiol 16(3):236–239. https://doi.org/10.1097/00008506-200407000-00009
Mayberg TS, Lam AM, Matta BF, Domino KB, Winn HR (1995) Ketamine does not increase cerebral blood flow velocity or intracranial pressure during isoflurane/nitrous oxide anesthesia in patients undergoing craniotomy. Anesth Analg 81(1):84–89. https://doi.org/10.1097/00000539-199507000-00017
Von der Brelie C, Seifert M, Rot S, Tittel A, Sanft C, Meier U, Lemcke J (2017) Sedation of patients with acute aneurysmal subarachnoid hemorrhage with ketamine is safe and might influence the occurrence of cerebral infarctions associated with delayed cerebral ischemia. World Neurosurg 97:374–382. https://doi.org/10.1016/j.wneu.2016.09.121
Souza KM, Anzoategui LC, Pedroso WC, Gemperli WA (2005) Dexmedetomidine in general anesthesia for surgical treatment of cerebral aneurysm in pregnant patient with specific hypertensive disease of pregnancy: case report. Rev Bras Anestesiol 55(2):212–216. https://doi.org/10.1590/s0034-70942005000200008
Yokota H, Yokoyama K, Noguchi H, Nishioka T, Umegaki O, Komatsu H, Sakaki T (2011) Post-operative dexmedetomidine-based sedation after uneventful intracranial surgery for unruptured cerebral aneurysm: comparison with propofol-based sedation. Neurocrit Care 14(2):182–187. https://doi.org/10.1007/s12028-010-9485-4
Lee HH, Jung YJ, Choi BY, Chang CH (2014) Usefulness of dexmedetomidine during intracerebral aneurysm coiling. J Korean Neurosurg Soc 55(4):185–189. https://doi.org/10.3340/jkns.2014.55.4.185
Tang CL, Li J, Zhang ZT, Zhao B, Wang SD, Zhang HM, Shi S, Zhang Y, Xia ZY (2018) Neuroprotective effect of bispectral index-guided fast-track anesthesia using sevoflurane combined with dexmedetomidine for intracranial aneurysm embolization. Neural Regen Res 13(2):280–288. https://doi.org/10.4103/1673-5374.226399
McDermott MW, Durity FA, Borozny M, Mountain MA (1989) Temporary vessel occlusion and barbiturate protection in cerebral aneurysm surgery. Neurosurgery 25(1):54–61; discussion 61-52. https://doi.org/10.1097/00006123-198907000-00010
McConkey PP, Kien ND (2002) Cerebral protection with thiopentone during combined carotid endarterectomy and clipping of intracranial aneurysm. Anaesth Intensive Care 30(2):219–222. https://doi.org/10.1177/0310057x0203000217
Ravussin P, de Tribolet N (1993) Total intravenous anesthesia with propofol for burst suppression in cerebral aneurysm surgery: preliminary report of 42 patients. Neurosurgery 32(2):236–240 discussion 240. https://doi.org/10.1227/00006123-199302000-00013
Schmieder K, Schregel W, Engelhardt M, Harders A, Cunitz G (2003) Cerebral vascular reactivity response to anaesthetic induction with propofol in patients with intracranial space-occupying lesions and vascular malformations. Eur J Anaesthesiol 20(6):457–460. https://doi.org/10.1017/s0265021503000711
Yamada M, Nishikawa K, Kawahara F, Yoshikawa D, Saito S, Goto F (2003) Anesthetic management for clipping a giant basilar artery aneurysm with moderate hypothermia, extracorporeal circulation assistance, and propofol infusion. J Neurosurg Anesthesiol 15(3):274–277. https://doi.org/10.1097/00008506-200307000-00018
Mahajan C, Chouhan RS, Rath GP, Dash HH, Suri A, Chandra PS, Mahajan A (2014) Effect of intraoperative brain protection with propofol on postoperative cognition in patients undergoing temporary clipping during intracranial aneurysm surgery. Neurol India 62(3):262–268. https://doi.org/10.4103/0028-3886.136908
Karwacki Z, Niewiadomski S, Witkowska M, Dzierzanowski J, Szczyrba S, Cichomska M (2018) The influence of propofol on middle cerebral artery flow velocity (VMCA) in patients with unruptured intracranial aneurysms during induction of general anaesthesia. Anaesthesiol Intensive Ther 50(5):349–358. https://doi.org/10.5603/ait.2018.0047
Ishibashi T, Toyama S, Miki K, Karakama J, Yoshino Y, Ishibashi S, Tomita M, Nemoto S (2019) Effects of propofol versus sevoflurane on cerebral circulation time in patients undergoing coiling for cerebral artery aneurysm: a prospective randomized crossover study. J Clin Monit Comput 33(6):987–998. https://doi.org/10.1007/s10877-018-00251-2
Guo D, Li Y, Wang H, Wang X, Hua W, Tang Q, Miao L, Wang G (2019) Propofol post-conditioning after temporary clipping reverses oxidative stress in aneurysm surgery. Int J Neurosci 129(2):155–164. https://doi.org/10.1080/00207454.2018.1483920
Uchida K, Yasunaga H, Sumitani M, Horiguchi H, Fushimi K, Yamada Y (2014) Effects of remifentanil on in-hospital mortality and length of stay following clipping of intracranial aneurysm: a propensity score-matched analysis. J Neurosurg Anesthesiol 26(4):291–298. https://doi.org/10.1097/ana.0000000000000039
Lavine SD, Masri LS, Levy ML, Giannotta SL (1997) Temporary occlusion of the middle cerebral artery in intracranial aneurysm surgery: time limitation and advantage of brain protection. Neurosurg Focus 2(6):e4. https://doi.org/10.3171/foc.1997.2.1.5
Foroohar M, Macdonald RL, Roth S, Stoodley M, Weir B (2000) Intraoperative variables and early outcome after aneurysm surgery. Surg Neurol 54(4):304–315. https://doi.org/10.1016/s0090-3019(00)00294-9
Allen G, Farling P, McAtamney D (2006) Anesthetic management of the pregnant patient for endovascular coiling of an unruptured intracranial aneurysm. Neurocrit Care 4(1):18–20. https://doi.org/10.1385/ncc:4:1:018
Magni G, La Rosa I, Gimignani S, Melillo G, Imperiale C, Rosa G (2007) Early postoperative complications after intracranial surgery: comparison between total intravenous and balanced anesthesia. J Neurosurg Anesthesiol 19(4):229–234. https://doi.org/10.1097/ANA.0b013e31806e5f5a
Karwacki Z, Witkowska M, Niewiadomski S, Wiatr A, Bukowski P, Wierzchowska J, Zapasnik A (2013) Anaesthetic management for endovascular treatment of unruptured intracranial aneurysms. Anaesthesiol Intensive Ther 45(3):145–148. https://doi.org/10.5603/ait.2013.0030
Hoffman WE, Charbel FT, Edelman G, Ausman JI (1998) Thiopental and desflurane treatment for brain protection. Neurosurgery 43(5):1050–1053. https://doi.org/10.1097/00006123-199811000-00026
Courville CB (1939) Untoward effects of nitrous oxide anesthesia with particular reference to residual neurologic and psychiatric manifestations. California: Pacific Press Publishing Association, p 174
Lam AM, Mayberg TS (1992) Use of nitrous oxide in neuroanesthesia: why bother? J Neurosurg Anesthesiol 4:284–284
Haelewyn B, David HN, Rouillon C, Chazalviel L, Lecocq M, Risso J-J, Lemaire M, Abraini JH (2008) Neuroprotection by nitrous oxide: facts and evidence. Crit Care Med 36(9):2651–2659
Culley DJ, Crosby G (2008) Nitrous oxide in neuroanesthesia: tried and true or toxin? Anesthesiology 108(4):553–554
Pasternak JJ, Lanier WL (2010) Is nitrous oxide use appropriate in neurosurgical and neurologically at-risk patients? Curr Opin Anaesthesiol 23(5):544–550. https://doi.org/10.1097/ACO.0b013e32833e1520
Varma MK, Price K, Jayakrishnan V, Manickam B, Kessell G (2007) Anaesthetic considerations for interventional neuroradiology. Br J Anaesth 99(1):75–85. https://doi.org/10.1093/bja/aem122
Frost EA (2017) Nitrous oxide in neuroanesthesia: does it have a place? In: Scher CS, Clebone A, Miller SM, Roccaforte JD, Capan LM (eds) You’re wrong, I’m right: dueling authors reexamine classic teachings in anesthesia. Cham: Springer International Publishing, pp 207–208
Frawley G, Davidson A (2016) Inhaled anestheteic agents. In: Davis PJ, Cladis FP (eds) Smith’s anesthesia for infants and children. Philadelphia: Elsevier Health Sciences, pp 200–213
Lee JJ, Li L, Jung H-H, Zuo Z (2008) Postconditioning with isoflurane reduced ischemia-induced brain injury in rats. Anesthesiology 108(6):1055–1062
Lam AM, Gelb AW (1983) Cardiovascular effects of isoflurane-induced hypotension for cerebral aneurysm surgery. Anesth Analg 62(8):742–748
MADSEN JB, COLD GE, HANSEN ES, BARDRUM B, KRUSE-LARSEN C (1987) Cerebral blood flow and metabolism during isoflurane-induced hypotension in patients subjected to surgery for cerebral aneurysms. BJA 59(10):1204–1207. https://doi.org/10.1093/bja/59.10.1204
Gaidhani N, Sun F, Schreihofer D, Uteshev VV (2017) Duration of isoflurane-based surgical anesthesia determines severity of brain injury and neurological deficits after a transient focal ischemia in young adult rats. Brain Res Bull 134:168–176. https://doi.org/10.1016/j.brainresbull.2017.07.018
Lehmann F, Müller M, Zimmermann J, Güresir Á, Lehmann V, Putensen C, Vatter H, Güresir E (2020) Inhalational isoflurane sedation in patients with decompressive craniectomy suffering from severe subarachnoid hemorrhage: a case series. J Neuroanaesthesiol Crit Care 7:27–33
Cottrell JE, Patel P (2017) Cottrell and Patel's neuroanesthesia, Sixth edn. Elsevier, Edinburgh
Brioni JD, Varughese S, Ahmed R, Bein B (2017) A clinical review of inhalation anesthesia with sevoflurane: from early research to emerging topics. J Anesth 31(5):764–778. https://doi.org/10.1007/s00540-017-2375-6
Schifilliti D, Grasso G, Conti A, Fodale V (2010) Anaesthetic-related neuroprotection: intravenous or inhalational agents? CNS Drugs 24(11):893–907. https://doi.org/10.2165/11584760-000000000-00000
Xu L, Shen J, Yu L, Sun J, McQuillan PM, Hu Z, Yan M (2018) Role of autophagy in sevoflurane-induced neurotoxicity in neonatal rat hippocampal cells. Brain Res Bull 140:291–298. https://doi.org/10.1016/j.brainresbull.2018.05.020
Bo LJ, Yu PX, Zhang FZ, Dong ZM (2018) Dexmedetomidine mitigates sevoflurane-induced cell cycle arrest in hippocampus. J Anesth 32(5):717–724. https://doi.org/10.1007/s00540-018-2545-1
Eger EI 2nd, Gong D, Koblin DD, Bowland T, Ionescu P, Laster MJ, Weiskopf RB (1998) The effect of anesthetic duration on kinetic and recovery characteristics of desflurane versus sevoflurane, and on the kinetic characteristics of compound A, in volunteers. Anesth Analg 86(2):414–421. https://doi.org/10.1097/00000539-199802000-00037
Holmstrom A, Akeson J (2004) Desflurane increases intracranial pressure more and sevoflurane less than isoflurane in pigs subjected to intracranial hypertension. J Neurosurg Anesthesiol 16(2):136–143. https://doi.org/10.1097/00008506-200404000-00005
Sponheim S, Skraastad O, Helseth E, Due-Tonnesen B, Aamodt G, Breivik H (2003) Effects of 0.5 and 1.0 MAC isoflurane, sevoflurane and desflurane on intracranial and cerebral perfusion pressures in children. Acta Anaesthesiol Scand 47(8):932–938. https://doi.org/10.1034/j.1399-6576.2003.00199.x
Kundra S, Mahendru V, Gupta V, Choudhary AK (2014) Principles of neuroanesthesia in aneurysmal subarachnoid hemorrhage. J Anaesthesiol Clin Pharmacol 30(3):328–337. https://doi.org/10.4103/0970-9185.137261
Lee JW, Woo JH, Baik HJ, Kim DY, Chae JS, Yang NR, Seo EK (2018) The effect of anesthetic agents on cerebral vasospasms after subarachnoid hemorrhage: a retrospective study. Medicine (Baltimore) 97(31):e11666. https://doi.org/10.1097/MD.0000000000011666
Srivastava S (2017) Use of desflurane in neurosurgery: cons. J Neuroanaesthesiol Crit Care 04. https://doi.org/10.4103/2348-0548.199955
Urwin SC, Menon DK (2004) Comparative tolerability of sedative agents in head-injured adults. Drug Saf 27(2):107–133. https://doi.org/10.2165/00002018-200427020-00003
Luthra A, Rath G (2018) Ketamine: a neuroanesthesiologist's friend or foe? J Neuroanaesthesiol Crit Care 05:77–82. https://doi.org/10.1055/s-0038-1654746
Soriano FX, Papadia S, Hofmann F, Hardingham NR, Bading H, Hardingham GE (2006) Preconditioning doses of NMDA promote neuroprotection by enhancing neuronal excitability. J Neurosci 26(17):4509–4518. https://doi.org/10.1523/jneurosci.0455-06.2006
Himmelseher S, Durieux ME (2005) Revising a dogma: ketamine for patients with neurological injury? Anesth Analg 101(2):524–534, table of contents. https://doi.org/10.1213/01.Ane.0000160585.43587.5b
Prielipp RC, Wall MH, Tobin JR, Groban L, Cannon MA, Fahey FH, Gage HD, Stump DA, James RL, Bennett J, Butterworth J (2002) Dexmedetomidine-induced sedation in volunteers decreases regional and global cerebral blood flow. Anesth Analg 95(4):1052–1059, table of contents. https://doi.org/10.1097/00000539-200210000-00048
Singh S, Chouhan RS, Bindra A, Radhakrishna N (2018) Comparison of effect of dexmedetomidine and lidocaine on intracranial and systemic hemodynamic response to chest physiotherapy and tracheal suctioning in patients with severe traumatic brain injury. J Anesth 32(4):518–523. https://doi.org/10.1007/s00540-018-2505-9
Batra A, Verma R, Bhatia VK, Chandra G, Bhushan S (2017) Dexmedetomidine as an anesthetic adjuvant in intracranial surgery. Anesth Essays Res 11(2):309–313. https://doi.org/10.4103/0259-1162.194555
Iwasaki Y, Nakamura T, Hamakawa T (2010) Retrospective evaluation of dexmedetomidine for postoperative sedation in patients for cerebral aneurysm surgery. Masui 59(11):1396–1399
Shapiro H, Galindo A, Wyte S, Harris A (1973) Rapid intraoperative reduction of intracranial pressure with thiopentone. BJA 45(10):1057–1062
Smith AL, Hoff JT, Nielsen SL, Larson CP (1974) Barbiturate protection in acute focal cerebral ischemia. Stroke 5(1):1–7. https://doi.org/10.1161/01.str.5.1.1
Hoff JT, Smith AL, Hankinson HL, Nielsen SL (1975) Barbiturate protection from cerebral infarction in primates. Stroke 6(1):28–33. https://doi.org/10.1161/01.str.6.1.28
Zaidan JR, Klochany A, Martin WM, Ziegler JS, Harless DM, Andrews RB (1991) Effect of thiopental on neurologic outcome following coronary artery bypass grafting. Anesthesiology 74(3):406–411. https://doi.org/10.1097/00000542-199103000-00003
Nussmeier NA, Arlund C, Slogoff S (1986) Neuropsychiatric complications after cardiopulmonary bypass: cerebral protection by a barbiturate. Anesthesiology 64(2):165–170. https://doi.org/10.1097/00000542-198602000-00006
Belopavlovic M, Buchthal A, Beks JW (1985) Barbiturates for cerebral aneurysm surgery. A review of preliminary results. Acta Neurochir 76(3–4):73–81. https://doi.org/10.1007/bf01418464
Vuyk J, Sitsen E, Reekers M (2020) Intravenous anesthetics. In: Gropper MA, Cohen NH, Eriksson LI, Fleisher LA, Leslie K, Wiener-Kronish JP. (eds) Miller’s anesthesia, 9th edition. Philadelphia: Elsevier Health Sciences, pp 638–679
Ravussin P, Revelly JP, Chiolero R (1991) clinical use of propofol in neuroanesthesia. Agressologie 32(8-9 spec):407–411
Acquaviva R, Campisi A, Murabito P, Raciti G, Avola R, Mangiameli S, Musumeci I, Barcellona ML, Vanella A, Li Volti G (2004) Propofol attenuates peroxynitrite-mediated DNA damage and apoptosis in cultured astrocytes: an alternative protective mechanism. Anesthesiology 101(6):1363–1371. https://doi.org/10.1097/00000542-200412000-00017
Sagara Y, Hendler S, Khoh-Reiter S, Gillenwater G, Carlo D, Schubert D, Chang J (1999) Propofol hemisuccinate protects neuronal cells from oxidative injury. J Neurochem 73(6):2524–2530. https://doi.org/10.1046/j.1471-4159.1999.0732524.x
Chui J, Mariappan R, Mehta J, Manninen P, Venkatraghavan L (2014) Comparison of propofol and volatile agents for maintenance of anesthesia during elective craniotomy procedures: systematic review and meta-analysis. Can J Anesthesia 61(4):347–356
Hayward NJ, McKnight AT, Woodruff GN (1993) Neuroprotective effect of the kappa-agonist enadoline (CI-977) in rat models of focal cerebral ischaemia. Eur J Neurosci 5(7):961–967. https://doi.org/10.1111/j.1460-9568.1993.tb00947.x
Zhang J, Haddad GG, Xia Y (2000) Delta-, but not mu- and kappa-, opioid receptor activation protects neocortical neurons from glutamate-induced excitotoxic injury. Brain Res 885(2):143–153. https://doi.org/10.1016/s0006-8993(00)02906-1
He X, Sandhu HK, Yang Y, Hua F, Belser N, Kim DH, Xia Y (2013) Neuroprotection against hypoxia/ischemia: delta-opioid receptor-mediated cellular/molecular events. Cell Mol Life Sci 70(13):2291–2303. https://doi.org/10.1007/s00018-012-1167-2
Girard F, Moumdjian R, Boudreault D, Chouinard P, Bouthilier A, Ruel M (2009) The effect of sedation on intracranial pressure in patients with an intracranial space-occupying lesion: remifentanil versus propofol. Anesth Analg 109(1):194–198. https://doi.org/10.1213/ane.0b013e3181a3ea3a
Degoute CS (2007) Controlled hypotension: a guide to drug choice. Drugs 67(7):1053–1076. https://doi.org/10.2165/00003495-200767070-00007
Ihn YK, Shin SH, Baik SK, Choi IS (2018) Complications of endovascular treatment for intracranial aneurysms: management and prevention. Interv Neuroradiol 24(3):237–245. https://doi.org/10.1177/1591019918758493
Hoffman WE, Edelman G (2000) Enhancement of brain tissue oxygenation during high dose isoflurane anesthesia in the dog. J Neurosurg Anesthesiol 12(2):95–98. https://doi.org/10.1097/00008506-200004000-00004
Tsai YC, Huang SJ, Lai YY, Chang CL, Cheng JT (1994) Propofol does not reduce infarct volume in rats undergoing permanent middle cerebral artery occlusion. Acta Anaesthesiol Sin 32(2):99–104
Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, Floyd J, Fornage M, Gillespie C, Isasi C (2017) Heart disease and stroke statistics-2017 update: a report from the American Heart Association. Circulation 135(10):e146–e603
Lavine SD, Masri LS, Levy ML, Giannotta SL (1997) Temporary occlusion of the middle cerebral artery in intracranial aneurysm surgery: time limitation and advantage of brain protection. J Neurosurg 87(6):817–824. https://doi.org/10.3171/jns.1997.87.6.0817
Hadler RA, Neuman MD, FLeisher LA (2020) Risk of anesthesia. In: Gropper MA, Cohen NH, Eriksson LI, Fleisher LA, Leslie K, Wiener-Kronish JP. (eds) Miller’s anesthesia, 9th edition. Philadelphia: Elsevier Health Sciences, pp 892–917
Fukuda M, Vazquez AL, Zong X, Kim S-G (2013) Effects of the α2-adrenergic receptor agonist dexmedetomidine on neural, vascular and BOLD fMRI responses in the somatosensory cortex. Eur J Neurosci 37(1):80–95. https://doi.org/10.1111/ejn.12024
Author information
Authors and Affiliations
Contributions
SE, JV, ABB, and SG: study design, data collection, data analysis, and writing up the first draft of the manuscript. LKB, ME, CF, RP, AT, CSO, SS, and AN: study design, data review and analysis, revision, and finalization of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This hospital registry study was approved by the Institutional Review Board at the Beth Israel Deaconess Medical Center.
Informed consent
Waived.
Consent to participate
NA, review of published literature.
Consent for publication
All authors participated in the development of the manuscript and give consent for the article to be published in Neurosurgical Review.
Code availability
NA, review of published literature.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Esmaeeli, S., Valencia, J., Buhl, L.K. et al. Anesthetic management of unruptured intracranial aneurysms: a qualitative systematic review. Neurosurg Rev 44, 2477–2492 (2021). https://doi.org/10.1007/s10143-020-01441-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-020-01441-w