
Abstract
Minimally invasive transcranial approaches (MITAs) continue to expand in popularity in neurosurgery. Only few MITAs allow sufficient sylvian exposure to enable wide use of the transsylvian corridor. In this study, we aim to compare the transsylvian corridor in two MITAs: the minipterional (MPTa) and the extended supraorbital eyebrow approaches (XSEa). Eight cadaver heads were used to quantify the surgical exposure and maneuverability along the sylvian fissure and the insular lobe provided by the MPTa and the XSEa. Surgical exposure was calculated by means of the exposed length of the sylvian fissure and by the area framed within three extreme points in the insular lobe. Maneuverability was assessed by means of the surgical freedom along the sylvian cistern. XSEa provides twice the frontal exposure and half of the temporal exposure in comparison to the MPTa (p < 0.001 and p = 0.02, respectively). No significant differences were found between the two craniotomies in the length of the exposure of the sylvian fissure, area of insular exposure, or surgical freedom. Both the MPTa and the XSEa afford sufficient grades of exposure along the sylvian fissure and the insular lobe, although the viewing angle is significantly different between the two approaches. Such properties allow either to be used for microsurgery deep within the sylvian cistern. The use of additional corridors, such as the subfrontal route (XSEa) and pretemporal route (MPTa), may influence selection of either the minipterional or the extended supraorbital approaches according to the origin of the surgical pathology addressed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The current trend of minimally invasive transcranial approaches (MITAs) in neurosurgery must balance the advantages of reduced approach-related morbidity with the disadvantages of potential limited surgical exposure. Several MITAs have been proposed as less disruptive alternatives for treating selected lesions in the anterior and middle cranial fossae [1, 3, 4, 9, 12, 15, 21, 22, 24]. However, simply minimizing the craniotomy size does not justify MITA use if the tradeoff is reduced surgical instrument maneuverability and operative comfort [19].
Sylvian fissure splitting is a microsurgical technique that is regarded as a key step to address pathologies harbored in the insular lobe and the middle cerebral artery (MCA), including MCA aneurysms, insular gliomas, and cavernous malformations [20]. Sylvian fissure dissection allows atraumatic brain retraction and improves instrument maneuverability and visualization along the sylvian and deep basal cisterns [5]. Although several clinical series have reported the suitability of MITA for accessing the sylvian fissure and treating middle cerebral aneurysms [3, 18, 23, 26], the limited exposure has raised concerns of its application in the treatment of large tumoral or vascular lesions [6, 9, 11].
Similar to the minipterional approach (MPTa) [9], the extended supraorbital eyebrow approach (XSEa) [22] provides access to the proximal sylvian fissure by expanding the craniotomy limits beneath the pterion [13, 15]. While the sylvian fissure is accessible in both MPTa and XSEa, little is known whether different viewing angles afford a quantitative superiority of one over the other in terms of surgical exposure and instrument maneuverability along the deep basal cisterns, MCA, and insular region.
The aim of the present study is to quantitatively evaluate and compare the surgical exposure and instrument maneuverability along the insula and the MCA bifurcation in two MITAs (MPTa and XSEa).
Methods
The present study was performed in accordance with institutionally approved guidelines for cadaver dissection. Eight unidentified silicone injected cadaver heads (16 sides) without any known intracranial pathology were used. A high-resolution computed tomographic scan was performed on each specimen and uploaded in a navigation system (iNtellect - Stryker Inc., Kalamazoo, MI) used for assessment of the approaches. Then, heads were registered for neuronavigation using surface recognition, ensuring an error lower than 0.5 mm.
Heads were positioned in the Mayfield headholder simulating the clinical scenario. Both the XSEa and the MPTa were performed in all heads (1 approach per side of the head) through macroscopic and microsurgical techniques, using microsurgery instruments (KLS Martin Group, GmbH & Co., Tuttlingen, Germany) and drills (Stryker-Leibinger Corp., Kalamazoo, USA) (Figs. 1 and 2). Once the dura was incised, dissections were carried out under microscopic visualization (Carl Zeiss Co., Jena, Germany). Both approaches were equally distributed among each side of the head (e.g., XSEa and MPTa were performed in 4 left sides and 4 right sides each).

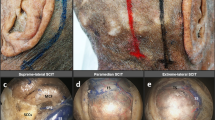
Skin incision in minimally invasive approaches. a In the extended supraorbital eyebrow approach, the skin incision (blue line) extends lateral to the supratrochlear notch over the superior third of the eyebrow, to avoid injuries to the supratrochlear nerve (yellow line). At the most lateral end of the eyebrow, the skin incision is turned posteriorly, over 15 to 20 mm, to increase the bone exposure and facilitate the visualization of the temporalis muscle. b The skin incision in the minipterional craniotomy is placed one finger breath anterior to the tragus to avoid damaging of the parietal branch of the superficial temporal artery (red line). Then, the incision is directed superiorly 1 cm behind the hairline and is extended up to the vertical pupillary line (white line). If an interfascial dissection of the temporalis muscle is performed, such a skin incision is generally enough to expose the anterior third of the superior temporal line and the pterion, as required in the minipterional approach. MPT, minipterional; STA, superficial temporal artery; XSE, extended supraorbital eyebrow; VPN, vertical pupillary line

Minimally invasive craniotomies. a In the extended supraorbital eyebrow approach (blue shadow area), the craniotomy extends from the supratrochlear notch medially, to the pterion inferiorly. b The minipterional craniotomy (red shadow area) is a pterion-centered craniotomy entirely located beneath the superior temporal line (dashed line). c Direct comparisons between the extended supraorbital eyebrow, minipterional, and pterional craniotomies allow to understand differences in the viewing angle, as well as their relationships with bony landmarks
Surgical approaches
Extended supraorbital eyebrow approach
Technical nuances of this approach have been recently discussed in detail [15]. In brief, the skin incision of the XSEa has a medial component consisting on an eyebrow incision lateral to the supraorbital notch and extending up to the lateral epicanthus, and a lateral component extending laterally from this point over 15 mm in the direction of the tragus (Fig. 1). Thereafter, using an interfascial technique, the temporalis muscle was released from the orbital rim until exposure of the pterion. The XSEa is performed with a craniotomy extending from the supratrochlear notch to the pterion and 2 to 3 cm width (Fig. 2). Then, the sphenoid ridge is drilled away until reaching the superior orbital fissure. After dural opening using a curvilinear incision with the base directed towards the orbit, sylvian fissure dissection is performed. Sylvian splitting is done from proximal to distal, using the inside-to-outside technique [5]. Concurrently, the opticocarotid and parapeduncular cisterns are dissected to expose the ICA bifurcation and the proximal M1 segment of the middle cerebral artery. Distal dissection of the sylvian fissure is carried out until technically feasible, given the surgical instruments maneuverability allowed by the approach.
Minipterional approach
MPTa has been widely described in previous reports [9, 17]. Briefly, an arcuate frontotemporal skin incision extending is carried out and anteriorly reflected (Fig. 1). Then, the periosteum and the superficial layer of the temporalis fascia are incised 2 cm behind the orbital rim, and the temporalis muscle is dissected in an interfascial fashion. The temporalis muscle is inferiorly retracted until the pterion and the squamous part of temporal bone are exposed. A minipterional craniotomy centered over the pterion is performed with posterior limit right behind the pterion and the superior limit at the level of the superior temporal line (Fig. 2). The sphenoid wing is flattened until exposure of the meningo-orbital band at the level of the superior orbital fissure. The dura is opened in a curvilinear fashion and retracted anteriorly. Once the intradural space is exposed, a proximal sylvian dissection is carried out anteriorly starting at the anterior sylvian point (ASyP). Opticocarotid, parapeduncular, and chiasmatic cisterns are then dissected to expose the internal carotid artery, and optic nerve.
Anatomical observations and quantitative assessment
The qualitative and quantitative assessments were performed in each approach (XSEa and MPTa). Stereotactic points (x, y, z coordinates) were obtained with the neuronavigation system and were subsequently processed using a dedicated software (Microsoft Office Excel 2013; Microsoft Corp., Redmond, WA, USA) that calculates distances (length) and areas from a spreadsheet of 3D coordinates. Mean values of the variables studied were used for comparison between the two approaches.
Temporal and frontal lobe cortical exposure was assessed by determining the length (mm) from the surface of the sylvian fissure to the edge of the widest point of the craniotomy (either temporal or frontal), following a plane orthogonal to the fissure.
Depth of the surgical corridor was assessed calculating the distance from the center point of the MITA craniotomies to the following 4 points along the sylvian cistern: (1) ipsilateral bifurcation of the MCA bifurcation; (2) limen insulae; (3) most distal reachable point along the axis of the insular lobe.
Length of sylvian exposure was calculated as the length (in mm) of the sylvian fissure that is exposed from the ASyP to the craniotomy margin.
Insular exposure was defined as the area (in mm2) of a triangular-shaped region framed between three extreme points along the insular lobe: one fixed point, located at the anteroinferior limit of the insular lobe, or limen insulae; and two mobile points, one located at the anterosuperior limit of the insular lobe and at the most distal reachable point within the insular lobe (Fig. 3).

a Cadaver dissection illustrating methods for calculations of the surgical exposure and maneuverability along the transsylvian corridor. b The area of exposure of the insular lobe was calculated by the area frame within a triangle delimited by the following: one fixed point (A′), located at the anteroinferior limit of the insular lobe, or limen insulae; and two mobile points, one located at the superoinferior limit of the insular lobe (B′) and at the most distal reachable point within the insular lobe (C′). c Surgical freedom was determined by calculating the area framed within a quadrangular-shaped region delimited by 4 extreme permissible working positions of the proximal end of a 25-cm endoscopic dissector while its distal tip was held fixed on the middle cerebral artery bifurcation
Surgical maneuverability was assessed by means of the surgical freedom and Ammirati’s maneuverability scale [2] at the MCA bifurcation. This scale assesses the degree of exposure based on the possibility of performing microsurgical maneuvers on a selected target of interest as follows: 0, target not visible; 1, target visible, maneuvers are not possible; 2, target visible, maneuvers are difficult; 3, target visible, maneuvers are possible; 4, target visible, maneuvers are facilitated [2]. The MCA bifurcation was selected as the target of interest for being the most representative vascular point at the sylvian cistern. Surgical freedom was determined by calculating the area (in mm2) framed within a quadrangular-shaped region delimited by 4 extreme permissible working positions of the proximal end of a 25-cm endoscopic dissector while its distal tip was held fixed on a particular target of interest as previously described [7] (Fig. 3).
Results
Sylvian fissure dissection allowed exposing the MCA bifurcation in all specimens. Examples of the intradural view along the sylvian cistern (proximal and distal) for both approaches (MPTa and XSEa) are displayed in Fig. 4. Similarly, a graphic representation of the craniotomy orientation in relation to the most relevant neurovascular targets in the anterior circulation is represented in Fig. 5. Table 1 summarizes surgical exposure and maneuverability along different targets.

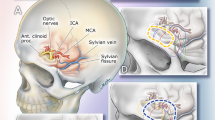
Comparisons of the intradural view in two minimally invasive anterolateral approaches. a, b Extended supraorbital eyebrow approach (a, at the level of the opticocarotid cistern, and b, at the level of the sylvian cistern). c, d Minipterional approach (c, at the level of the opticocarotid cistern, and d, at the level of the sylvian cistern). ACA, anterior cerebral artery; ACP, anterior clinoid process; Bas, basilar artery; Bifurc, bifurcation; ICA, internal carotid artery; Opt, optic; ON, optic nerve

Skull base cadaver dissections illustrating differences in the viewing angles, as well as in the reachable targets through the extended supraorbital eyebrow (a, b blue shadow area) and minipterional approaches (c, d red shadow area)
Cortical exposure
The XSEa provided larger exposure of the frontal lobe in comparison to the MPTa (36.35 mm, IQR 2.5 vs 16.12 mm, IQR 3.2; p < 0.001), while the MPTa was superior in terms of exposure of the temporal lobe (12.53 mm, IQR 4 vs 6.5 mm, IQR 2.2; p = 0.02).
Depth of the surgical corridor
The distance from the MPTa to the insular region was approximately half the distance from the XSEa to the same key points in the insular region (p < 0.05; see Table 1).
Sylvian and insular exposure
No significant differences were found in the exposure of the transsylvian corridor, by means of the length of the sylvian fissure exposure (MPTa 10.7 mm, IQR 1.8 vs XSEa 11.55 mm, IQR 2; p = 0.87), nor by means of the area of the insular exposure (MPTa 33.65 mm2, IQR 7.5 vs XSEa 31.78 mm2, IQR 9.3; p = 0.7) (Fig. 6).

Boxplots showing the length of exposure of the sylvian fissure and the area of surgical exposure in the insular lobe for the minipterional approach (MPTa) and the extended supraorbital eyebrow approach (XSEa), respectively. The length of the boxplot gives an idea of the dispersion of the sample, as each extreme represents the 25th and 75th percentiles. The horizontal line within the box marks the median value, and each extreme of the perpendicular line means the minimum and maximum value
Surgical maneuverability
There were no significant differences in the surgical freedom provided by the MPTa, as opposed to that provided by the XSEa (2256 mm2, IQR 581 vs 2132 mm2, IQR 400; p = 0.57) (Fig. 7). Degree of surgical maneuverability assessed by means of Ammirati’s score was similar in both approaches (4, IQR 0 vs 4, IQR 0.5; p = 0.59).

Boxplots showing differences in the surgical freedom along the middle cerebral artery bifurcation (surgical maneuverability) between the minipterional approach (MPTa) and the extended supraorbital eyebrow approach (XSEa)
Discussion
Lack of access to the sylvian fissure and the limited maneuverability along deep basal cisterns are major limitations of most of the MITA [6]. Sylvian splitting is key to atraumatic brain retraction and it is an essential tool in the vascular neurosurgeon’s armamentarium. However, there is still controversy regarding the length of the sylvian splitting needed to safely reach the deep basal cisterns with minimal brain retraction.
Results of the present study demonstrate that the XSEa and the MPTa provide good maneuverability through the transsylvian corridor and may be considered MITA alternatives to access the MCA and the insular lobe. While differing in the degree of exposure of the temporal and frontal lobes, both approaches are equivalent in terms of surgical freedom and exposure along the sylvian cistern.
The MPTa consists on a pterion-centered craniotomy entirely performed beneath the superior temporal line, so that the defect is entirely covered by the temporalis muscle, reducing the cosmetic impact [9, 26]. In their original description, Figueiredo et al. established the posterior limit of the craniotomy at the level of the pterion [9]. Such a landmark corresponds with the ASyP, which permits exposing the anterior rami of the sylvian fissure and offering the possibility to perform a proximal sylvian fissure dissection [9, 14, 16]. Our work shows that the XSEa is also successful in providing exposure and good maneuverability along the sylvian cistern, as long as the inferior limit of the craniotomy reaches the pterion and ASyP.
Previous studies have pointed out the limitations of middle fossa reach of the traditional supraorbital approach, considering it suboptimal to the MPTa for the treatment of MCA aneurysms. In addition, traditional supraorbital approach has also been considered a poor option for the treatment of ruptured intracranial aneurysms given the restraints to obtain proximal control [8, 11]. As shown in our previous work, the XSEa seems to solve most of these limitations by increasing the surgical exposure along the lateral compartment in 61% [13]. The extra bone removal added in the XSEa not only further enhances the lateral view along the anterior fossa but also increases the surgical maneuverability below the lesser sphenoid wing. These properties allow to dissect the proximal sylvian fissure and comfortably reach the middle cerebral artery bifurcation, similarly to the MPTa.
Transsylvian corridor in minimally invasive transcranial approaches
If both the MPTa and the XSEa afford equivalent degrees of the sylvian fissure and insular exposures, what are the disparities that make any of these two approaches more suitable for a given indication? We found that the frontal exposure provided by the MPTa is half of the XSEa exposure. The reduced exposure of the frontal lobe by the MPTa hinders the possibility to retract the frontal lobe and approaching the anterior communicating complex and lesions located in the anterior cranial fossa [14]. However, the subfrontal corridor provided by the XSEa is a direct route to the midline and the anterior cranial fossa, as per its shorter distance to this target and the favorably attacking angle from an anterior perspective [13]. Our results confirmed, in fact, that the distance from the MPTa to the insular region was approximately half the distance from the XSEa to the same key points in the insular lobe. Conversely, the exposure of the temporal lobe is optimal when using a MPTa. This surgical exposure is ideal to expand and use the pretemporal route, along with the transsylvian corridor, to reach lesions located in the middle fossa floor below the sphenoid ridge [17, 25].
Because both approaches expose the insular lobe and the sylvian cistern in a similar degree, the specific indications for each MITA are based on the need to address primarily the anterior or middle fossa. For instance, the MPTa should be advocated for lesions located primarily in the middle fossa with secondary extension above the sphenoid ridge, whereas the XSEa should be planned for anterior fossa tumors with secondary extension to the middle fossa. Similarly, MPTa is an effective and a more direct approach for single MCA aneurysms, whereas the XSEa seems to represent a reasonable alternative to access the midline and sylvian fissure (e.g., association of aneurysms of the anterior communicating and the middle cerebral artery).
Esthetically, the XSEa incision is 10 to 15 mm shorter and it might be preferred over the MPT incision in bald patients or in those with posteriorly implanted hairline. Moreover, the MPT requires retracting the skin flap anteriorly, requiring longer times to achieve full bone exposure for performing the craniotomy. Additionally, temporalis muscle atrophy, although minimal in comparison to the classic pterional approach (benefits), is more likely to happen in the MPTa, as the muscle dissection required to expose the pterion is minimal in the XSEa. Inversely, the MPTa incision is well tolerated by many patients with an anterior hairline. It may be preferred in patients with thin eyebrows or young patients in which the absence of wrinkles does not allow to hide the lateral extension of the XSEa incision. The XSEa craniotomy extends above and below the craniotomy, as opposed to the MPTa that is entirely performed beneath the superior temporal line. The risk of frontal sinus violation is increased when the craniotomy extends above this limit [10]. Hence, patients with a large frontal sinus pneumatization are poor candidates for performing an XSEa.
Study limitations
This study is limited by the design itself. Although valid models to assess techniques and surgical approaches, cadaveric heads do not fully replicate a clinical scenario. The amount of brain retraction required to access the sylvian cistern might vary, contingent upon the degree of tissue fixation. Further clinical studies are warranted in order to confirm our preliminary results and refine the effectiveness of using the transsylvian corridor in these two relatively new approaches.
Conclusions
Both the MPTa and the XSEa, while differing in the working angle and the use of the subfrontal corridor, expose in a similar degree the sylvian fissure and the insular lobe. Such properties allow to safely perform delicate maneuvers along the MCA bifurcation, such as aneurysm clipping. Further clinical studies are required to compare safety and effectiveness of the XSEa in comparison to more established techniques, such as the MPTa.
References
Almeida JP, Ruiz-Treviño AS, Shetty SR, Omay SB, Anand VK, Schwartz TH (2017) Transorbital endoscopic approach for exposure of the sylvian fissure, middle cerebral artery and crural cistern: an anatomical study. Acta Neurochir 159:1893–1907. https://doi.org/10.1007/s00701-017-3296-8
Ammirati M, Bernardo A (1998) Analytical evaluation of complex anterior approaches to the cranial base: an anatomic study. Neurosurgery 43:1398–1407; discussion 1407-1408. https://doi.org/10.1097/00006123-199812000-00081
Andrade-Barazarte H, Jägersberg M, Belkhair S, Tymianski R, Turel MK, Schaller K, Hernesniemi JA, Tymianski M, Radovanovic I (2017) The extended lateral supraorbital approach and extradural anterior clinoidectomy through a frontopterio-orbital window: technical note and pilot surgical series. World Neurosurg 100:159–166. https://doi.org/10.1016/j.wneu.2016.12.087
Chabot JD, Gardner PA, Stefko ST, Zwagerman NT, Fernandez-Miranda JC (2017) Lateral orbitotomy approach for lesions involving the middle fossa: a retrospective review of thirteen patients. Neurosurgery 80:309–322. https://doi.org/10.1093/neuros/nyw045
Cohen-Gadol AA (2020) Atraumatic sylvian fissure split: nuances and pitfalls. Oper Neurosurg (Hagerstown) 18:217–224. https://doi.org/10.1093/ons/opz074
Davies JM, Lawton MT (2014) Advances in open microsurgery for cerebral aneurysms. Neurosurgery 74 Suppl 1:S7–S16. https://doi.org/10.1227/NEU.0000000000000193
Elhadi AM, Hardesty DA, Zaidi HA, Kalani MYS, Nakaji P, White WL, Preul MC, Little AS (2015) Evaluation of surgical freedom for microscopic and endoscopic transsphenoidal approaches to the sella. Neurosurgery 11 Suppl 2:69–78; discussion 78-79. https://doi.org/10.1227/NEU.0000000000000601
Eroglu U, Shah K, Bozkurt M, Kahilogullari G, Yakar F, Dogan İ, Ozgural O, Attar A, Unlu A, Caglar S, Cohen Gadol AA, Ugur HC (2019) Supraorbital keyhole approach: lessons learned from 106 operative cases. World Neurosurg 124:e667–e674. https://doi.org/10.1016/j.wneu.2018.12.188
Figueiredo EG, Deshmukh P, Nakaji P, Crusius MU, Crawford N, Spetzler RF, Preul MC (2007) The minipterional craniotomy: technical description and anatomic assessment. Neurosurgery 61:256–264; discussion 264-265. https://doi.org/10.1227/01.neu.0000303978.11752.45
Flanigan P, Kshettry VR, Mullin JP, Jahangiri A, Recinos PF (2016) Frontal sinus morphometry in relation to surgically relevant landmarks in the United States population. World Neurosurg 91:12–15. https://doi.org/10.1016/j.wneu.2016.03.008
Heros RC (2011) The supraorbital “keyhole” approach. J Neurosurg 114:850–851; discussion 851. https://doi.org/10.3171/2010.6.JNS10878
Jeon C, Hong C-K, Woo KI, Hong SD, Nam D-H, Lee J-I, Choi JW, Seol HJ, Kong D-S (2018) Endoscopic transorbital surgery for Meckel’s cave and middle cranial fossa tumors: surgical technique and early results. J Neurosurg 131:1–10. https://doi.org/10.3171/2018.6.JNS181099
Martinez-Perez R, Albonette-Felicio T, Hardesty DA, Carrau RL, Prevedello DM (2020) Same viewing angle, minimal craniotomy enlargement, extreme exposure increase: the extended supraorbital eyebrow approach. Neurosurg Rev. https://doi.org/10.1007/s10143-020-01306-2
Martínez-Pérez R, Albonette-Felicio T, Hardesty DA, Prevedello DM (2020) Comparative anatomical analysis between the minipterional and supraorbital approaches. J Neurosurg:1–9. https://doi.org/10.3171/2019.12.JNS193196
Martinez-Perez R, Hardesty DA, Carrau RL, Prevedello DM (2020) The extended eyebrow approach a cadaveric stepwise dissection. Acta Neurochir 162:617–621. https://doi.org/10.1007/s00701-019-04203-w
Martinez-Perez R, Hardesty DA, Li R, Carrau RL, Prevedello DM (2020) Sylvian and insular exposure in the extended minipterional approach: landmarks, benefits, and quantitative analysis using a cadaveric study. World Neurosurg 138:e859–e866. https://doi.org/10.1016/j.wneu.2020.03.126
Martínez-Pérez R, Hernández-Álvarez V, Maturana R, Mura JM (2019) The extradural minipterional pretemporal approach for the treatment of spheno-petro-clival meningiomas. Acta Neurochir 161:2577–2582. https://doi.org/10.1007/s00701-019-04064-3
Martinez-Perez R, Joswig H, Tsimpas A, Poblete T, Albiña P, Perales I, Mura JM (2019) The extradural minipterional approach for the treatment of paraclinoid aneurysms: a cadaver stepwise dissection and clinical case series. Neurosurg Rev 43:361–370. https://doi.org/10.1007/s10143-019-01219-9
Martinez-Perez R, Mura JM (2019) The extradural minipterional approach: “think small, play wider.”. World Neurosurg 125:534–535. https://doi.org/10.1016/j.wneu.2018.10.240
Muhammad S, Tanikawa R, Lawton M, Regli L, Niemelä M, Korja M (2019) Microsurgical dissection of sylvian fissure-short technical videos of third generation cerebrovascular neurosurgeons. Acta Neurochir 161:1743–1746. https://doi.org/10.1007/s00701-019-03999-x
Raza SM, Quinones-Hinojosa A, Lim M, Boahene KDO (2013) The transconjunctival transorbital approach: a keyhole approach to the midline anterior skull base. World Neurosurg 80:864–871. https://doi.org/10.1016/j.wneu.2012.06.027
Reisch R, Perneczky A (2005) Ten-year experience with the supraorbital subfrontal approach through an eyebrow skin incision. Neurosurgery 57:242–255; discussion 242-255. https://doi.org/10.1227/01.neu.0000178353.42777.2c
Rychen J, Croci D, Roethlisberger M, Nossek E, Potts M, Radovanovic I, Riina H, Mariani L, Guzman R, Zumofen DW (2018) Minimally invasive alternative approaches to pterional craniotomy: a systematic review of the literature. World Neurosurg 113:163–179. https://doi.org/10.1016/j.wneu.2018.02.016
Sattur MG, Abi-Aad KR, Welz ME, Aoun RJ, Krishna C, Purnell C, Alghoul M, Bendok BR (2020) Extended lateral orbital craniotomy: anatomic study and initial clinical series of a novel minimally invasive pterional approach. J Neurol Surg B Skull Base 81:88–96. https://doi.org/10.1055/s-0038-1677470
Tra H, Huynh T, Nguyen B (2018) Minipterional and supraorbital keyhole craniotomies for ruptured anterior circulation aneurysms: experience at single center. World Neurosurg 109:36–39. https://doi.org/10.1016/j.wneu.2017.09.058
Welling LC, Figueiredo EG, Wen HT, Gomes MQT, Bor-Seng-Shu E, Casarolli C, Guirado VMP, Teixeira MJ (2015) Prospective randomized study comparing clinical, functional, and aesthetic results of minipterional and classic pterional craniotomies. J Neurosurg 122:1012–1019. https://doi.org/10.3171/2014.11.JNS146
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
Daniel M. Prevedello is a consultant for Integra LifeSciences Corp. and Stryker Corporation. Daniel Prevedello has equity on 3 rivers LLC, eLUM Technologies, LLC, and Soliton LLC. Daniel Prevedello receives royalties from ACE Medical, KLS Martin, and Mizuho.
Ethical approval and informed consent
Informed consent and ethical approval were not deemed necessary by the local ethics in view of the design of the study. Anatomical dissections, measurements, and analysis were performed at the Anatomical Laboratory for VisuoSpatial Innovations in Otolaryngology and Neurosurgery (ALT-VISION) at The Ohio State University.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Martinez-Perez, R., Beer-Furlan, A., Albonette-Felicio, T. et al. The transsylvian corridor through minimally invasive transcranial approaches: a comparative anatomical study. Neurosurg Rev 44, 2619–2627 (2021). https://doi.org/10.1007/s10143-020-01439-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10143-020-01439-4