
Abstract
The objective of the study is to describe the causes of cardiac arrest and complications of cardiopulmonary resuscitation (CPR) on thoraco-abdominal CT examinations for resuscitated patients in our institution. We evaluated the causes of cardiac arrest on thoraco-abdominal CT scans, which was compared with the final diagnosis (determined by consensus of two emergency physicians based on the clinical, imaging, and laboratory findings). Additionally, we evaluated the complications of CPR on thoraco-abdominal CT scans. From March 2005 to August 2011, 82 patients underwent CT of the thorax (n = 77) and abdomen (n = 23) within 24 h after CPR. Final diagnosis was as follows: cardiac (n = 29), respiratory (n = 28), metabolic (n = 11), exsanguination (n = 5), cerebral (n = 2), sepsis (n = 1), and indeterminate (n = 6). In 25 patients (30 %), thoraco-abdominal CT scans made the role either as a definitive study (n = 22) or as a supportive test (n = 3) for the diagnosis. In particular, CT was critical in diagnosis of many respiratory causes (64 %) and all exsanguinations. The most common complications following CPR were skeletal chest injuries (n = 48), followed by lung contusion (n = 45). Thoraco-abdominal CT examinations are helpful for the diagnosis of cause of cardiac arrest and complications of CPR.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The rate of survival after out-of-hospital cardiac arrest is generally low; however, with continued implementation of each link of the survival chain, it has shown an increasing trend. In Arizona, overall rate of survival from out-of-hospital improved from 4 % in 2005 to 10 % in 2009, after beginning Save Hearts in Arizona Registry and Education [1–3]. Findings from several reports have demonstrated the prognostic significance and therapeutic implications of computed tomography (CT) examinations of the brain for the resuscitated patients. However, to the best of our knowledge, there has been no report on the diagnostic efficacy of thoraco-abdominal CT examinations for resuscitated patients despite increasing use of the examinations in clinical practice. The purpose of the study is to describe the causes of cardiac arrest and complications of cardiopulmonary resuscitation (CPR) on thoraco-abdominal CT examinations for resuscitated patients.
Methods
This retrospective cohort study was approved by the institutional review board of our hospital, and the requirement for informed patient consent was waived.
Patients and CT examinations
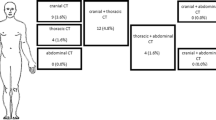
From March 2005 to August 2011, a total of 386 resuscitated patients underwent CT examinations (386 brain CTs, 113 chest CTs, and 52 abdominal CTs) in our emergency department. After exclusion of 139 patients who underwent CPR for a known traumatic cause of cardiac arrest, 4 patients who underwent CPR for in-hospital cardiac arrest, and 161 patients who underwent brain CT only, we finally included 82 patients who underwent CTs of the brain (n = 82), thorax (n = 77), and abdomen (n = 23; Fig. 1).

Flow diagram of the study
In our hospital, a multi-detector CT (Somatom Sensation 16 scanner, Siemens Medical Solutions, Germany) has been exclusively used for emergency patients since March 2005.
Data analysis
In order to evaluate the underlying disease, cause of cardiac arrest, management, and outcome of the patients, two emergency medicine physicians conducted a retrospective review of patients’ medical records. The cause of cardiac arrest was determined by consensus of them based on the clinical, imaging, and laboratory findings all together and, according to the previous description [4], that was classified as follows: cardiac, respiratory, cerebral, metabolic, exsanguination, and indeterminate. Respiratory causes included pulmonary embolism, asphyxia by upper airway obstruction, status asthmaticus, and pneumonia. Cerebral causes included cerebral hemorrhage and infarction/ischemia. Exsanguinations included gastrointestinal bleeding and ruptured aortic aneurysm. We defined exsanguination as the cause of cardiac arrest when the patients had (1) a clinical history of significant amount of hemoptysis or hematochezia and hematemesis, or (2) positive CT findings indicated bleeding (i.e., hemothorax, hemoperitoneum, aortic dissection, or aneurysm).
Two radiologists retrospectively reviewed for the cause of cardiac arrest on thoraco-abdominal CT images by consensus. We divided the role of CT as a definitive study and a supportive test for the diagnosis. Definitive study means when CT is considered as a confirmative study for the diagnosis. We regarded the CT did a supportive role for the diagnosis when CT was used to suspect the disease; however, additional studies are required for the confirmation. Additionally, we evaluated how many CPR-associated complications were detected on CT examinations in terms of skeletal chest injuries (rib and sternal fractures), lung injuries (lung contusion and laceration), other chest injuries (hemothorax, pneumothorax), and vascular and abdominal injuries.
Statistical analysis
The chi-squared test and two-sample t test were used as appropriate for comparison of clinical data (sex, age, and the presence of underlying disease) between patients for whose thoraco-abdominal CT could reveal the cause of cardiac arrest, and not. Statistical significance was calculated at a 95 % confidence interval (P < 0.05). Data processing and analysis were performed using commercially available software (PASW, version 17.0; SPSS, Chicago, IL, USA).
Results
Clinical characteristics
Clinical presentations of the study population are shown in Table 1. Patients included 49 men and 33 women, who ranged in age from 14 to 90 years (mean age, 58 years). Known medical diseases in 51 patients were as follows: hypertension (n = 30), diabetes mellitus (n = 14), chronic obstructive pulmonary disease (n = 13), stroke (n = 6), malignancies (n = 4; thyroid, breast, stomach, and colon cancer), chronic liver disease (n = 4), chronic renal disease (n = 2), and Grave’s disease (n = 1). All the patients experienced out-of-hospital cardiac arrest; 49 patients underwent standard CPR in the hospital and 33 patients received bystander CPR as well. Seventy-three patients underwent endotracheal intubation prior to CT examinations. According to medical charts, the mean duration of CPR was 11 ± 8 min (range, 2–40 min) for 64 patients, and the duration of CPR was not available for 18 patients. The cause of cardiac arrest, which was determined by clinical, imaging, and laboratory findings all together, were as follows: cardiac (n = 29), respiratory (n = 28), metabolic (n = 11), exsanguination (n = 5), cerebral (n = 2), sepsis (n = 1), and indeterminate (n = 6; Table 1).
Thirty-four patients expired in the median hospital day of 3 ± 11 days (range, 1–57 days; mean, 7 days) after resuscitation (mortality rate = 41.5 %), and 31 patients showed improvement and were discharged in the median LOS of 18 ± 16 days (range, 4–85 days; mean, 23 days). The remaining 17 patients could not be evaluated for the final outcome since they had transferred to other hospitals.
Cause of cardiac arrest detected on thoraco-abdominal CT examinations
In 25 patients (30 %), cause of cardiac arrests was detected on thoraco-abdominal CT scans, and the examinations were regarded as a definitive study (n = 22) and as a supportive test (n = 3) for the diagnosis. Particularly, thoraco-abdominal CT examination was considered critical in the diagnosis of many of the respiratory problems (64 %) as follow: pulmonary embolism (n = 8), acute infection (n = 4), lung cancer with airway obstruction (n = 3), and tension pneumothorax (n = 1). A patient who had tension pneumothorax was treated with chest tube insertion immediately after the examination. And all the patients who had pulmonary embolism (n = 8) were received anticoagulation therapy.
Exsanguination cases were as follows: acute aortic syndrome (n = 4; one of aortic dissection, two of intramural hematoma, one of ruptured aortic aneurysm; Fig. 2) and ruptured pseudoaneurysm of the uterine artery following hysterectomy (n = 1). Cardiomegaly and mediastinal widening were observed on chest radiographies for patients who had acute aortic syndromes; however, the radiographic results were insufficient for the confirmation or to demonstrate the site of rupture. After the CT examinations, the patients underwent surgical operation (n = 3), stent graft insertion (n = 1), and coil embolization therapy (n = 1).

A 90-year-old male who underwent cardiopulmonary resuscitations for intramural hematoma in the aorta. a Chest radiography (anterior-posterior view) shows mild mediastinal widening. b, c Axial image of chest CT (mediastinal setting) shows intramural hematoma in the aortic arch (arrows in b) and hemorrhage in the mediastinum (arrows in c)
Thorax CT confirmed one cardiac tamponade due to myocardial rupture and made suspicions on three cardiac abnormalities (anomalous origin of the coronary artery, hypertrophic cardiomyopathy, and acute myocardial infarction), which were subsequently confirmed with additional diagnostic tests (electrocardiogram, ECG; cardiac markers; invasive coronary angiogram).
The sex, age, and the presence of underlying disease in patients whose thoraco-abdominal CT examinations could diagnose the cause of cardiac arrest did not differ significantly from those in patients whose CT examinations could not be able to diagnose the cause of cardiac arrest (P = 0.16, 0.16, and 0.12, respectively).
Complications secondary to CPR on thoraco-abdominal CT examinations
Thoraco-abdominal CT examinations demonstrated various complications of CPR. The most common complications were skeletal chest injuries (rib fractures in 48 patients and sternal fractures in 19 patients), followed by lung contusion (n = 45), hemothorax (n = 31), pneumothorax (n = 5), and subclavian vein injury (n = 1; Fig. 3).

A 51-year-old man who underwent cardiopulmonary resuscitations for septic shock. a Bone setting image of chest CT shows fracture in the anterior arc of left fifth rib (arrow). b Lung setting image of the same section with a demonstrates consolidation and ground-glass opacities in the left lower lobes, representing pulmonary contusion
The majority of rib fractures were located in the anterior part (n = 43/48, 90 %) or lateral part of the thoracic cage in the second through seventh ribs or ribs within this region. Most rib fractures were bilateral (n = 37, 77 %) and multiple (n = 43, 90 %), ranging from 2 to 14 (mean number of fractured ribs = 7). Sternal fractures were located predominantly in the middle-third (n = 12) and lower-third (n = 5) of the sternal body, and transverse fracture (n = 17) was more common than oblique fracture (n = 2). Only two of 48 patients who had rib fractures were visualized on chest radiograph images.
Pulmonary contusion was observed on chest CT in 45 patients. The CT findings of CPR-associated pulmonary contusion were bilateral (n = 32), ground-glass opacity (n = 41), and consolidation (n = 38), which were distributed along the bronchovascular bundles (n = 20). Most abnormalities were located in the posterior area of upper lobes and lower lobes (n = 36). Other chest complications (hemothorax, pneumomediastinum, pneumothorax, and subclavian vein injury) were observed in 37 patients who had multiple rib fractures in the thorax.
Discussion
The utility of CT examinations has increased in the medical environment because of its superior accuracy, with technical improvements including the capability of thinner image sections, greater speed, and multiplanar reconstructions [5–7]. Multi-detector CT (MDCT) is particularly useful for patients in emergency conditions because it requires minimal effort, and the examination can be completed within a short period of time.
Several reports have demonstrated the prognostic significance and therapeutic implications of CT examinations of the brain for the resuscitated patients; Robin et al. [8] reported that abnormalities on brain CT examinations were not uncommon and showed the therapeutic and diagnostic alterations in a significant number of the resuscitated patients (39 %) after the examinations. And Inamasu et al. [9] revealed that positive findings for ischemia on brain CT scans could predict unfavorable patients’ outcome. However, to the best of our knowledge, there has been no report regarding findings of thoraco-abdominal CT examinations for resuscitated patients. In our institution, emergency physicians initially perform history taking, physical examinations, and laboratory examinations including cardiac markers, ECG, and brain CT examinations. And if the patients have no abnormal findings or borderline results in the initial examinations, the resuscitated patients were generally recommended thoraco-abdominal CT examinations within 1 day after CPR for evaluating cause of cardiac arrest and complications of CPR in our institution. We report here on the findings of thoraco-abdominal CT examinations for these resuscitated patients. Thoraco-abdominal CT examinations demonstrated the cause of cardiac arrest in 30 % of patients. The examinations were particularly useful for the diagnosis of respiratory causes and exsanguinations. Routine anterior-posterior view of expiratory chest radiography in emergency department was an inappropriate study for the early diagnosis of pulmonary embolism or acute aortic syndrome, and CT examinations have been regarded as a definitive study for the diagnosis, and even for the rule out of the disease [10].
Among 30 patients who had cardiogenic causes, CT diagnosed one cardiac tamponade and made suspicions on three cardiac pathologies and recommended appropriate further studies for the confirmations. The most common cause of cardiac arrest is cardiac origin (myocardial infarction), and cardiac markers and ECG are sufficient for the diagnosis in most of the cases [4, 11]. However, thoracic CT could help to diagnose some of cardiac pathologies, such as cardiac rupture, tamponade, and to rule out other diseases that could manifest acute chest pain. Moreover, with the recently introduced ECG-gated MDCT, CT examinations were expected to diagnose a greater number of cardiac pathologies [12–14]. Moreover, since the origin of cardiac arrest is not easily recognized in routine clinical practice [4, 11, 15], thoraco-abdominal CT scans could be recommended for the early diagnosis and appropriate management in resuscitated patients, particularly in the patients who are hemodynamically unstable after initial exclusion of brain and cardiogenic problems with brain CT, cardiac markers, and ECG.
Compared with radiography, CT examination is also useful for evaluation of complications following CPR [16, 17]. The most common complications after chest compression were skeletal chest injuries, followed by lung contusion. Other chest injuries (hemothorax, pneumothorax, pneumomediastinum, and vascular injury) were observed adjacent to the fractured ribs. Although CPR-related abdominal injuries such as laceration of liver and spleen, and perforation of the gastrointestinal tract have been reported [18–21]; no case of abdominal complication was observed in our patients.
Limitations
This study had several limitations. First, since this study was conducted at a single institution, the number of patients was small. Second, we simply described the findings of thoraco-abdominal CT examinations (causes of cardiac arrest and complications of CPR) in resuscitated patients and did not specifically evaluate prognostic significance. Further randomized prospective studies are required to evaluate the prognostic implications of thoraco-abdominal CT examinations for the resuscitated patients. Third, findings of this study could not be pathologically confirmed because members of this study population survived from successful CPR. Even patients who finally died during hospitalization after CPR did not undergo autopsy. Finally, there might be a limitation to generalize the results since we analyzed 16-slice MDCT scan exclusively. Nowadays, CT machines tend to be developed as a 64- or 128-slice.
Conclusion
Thoraco-abdominal CT examinations might be useful for diagnosis of the cause of cardiac arrest and CPR-associated complications in resuscitated patients. In particular, these would be helpful to diagnose respiratory causes and exsanguinations for hemodynamically unstable resuscitated patients after initial exclusion of cardiogenic and brain problems with cardiac markers, ECG, and brain CT examinations.
References
Cummins RO, Ornato JP, Thies WH, Pepe PE (1991) Improving survival from sudden cardiac arrest: the “chain of survival” concept. A statement for health professionals from the Advanced Cardiac Life Support Subcommittee and the Emergency Cardiac Care Committee, American Heart Association. Circulation 83:1832–1847
Neumar RW, Barnhart JM, Berg RA, Chan PS, Geocadin RG, Luepker RV, Newby LK, Sayre MR, Nichol G (2011) Implementation strategies for improving survival after out-of-hospital cardiac arrest in the United States: consensus recommendations from the 2009 American Heart Association Cardiac Arrest Survival Summit. Circulation 123:2898–2910
Rea TD, Eisenberg MS, Sinibaldi G, White RD (2004) Incidence of EMS-treated out-of-hospital cardiac arrest in the United States. Resuscitation 63:17–24
Kurkciyan I, Meron G, Behringer W, Sterz F, Berzlanovich A, Domanovits H, Mullner M, Bankl HC, Laggner AN (1998) Accuracy and impact of presumed cause in patients with cardiac arrest. Circulation 98:766–771
Brody AS, Seidel FG, Kuhn JP (1989) CT evaluation of blunt abdominal trauma in children: comparison of ultrafast and conventional CT. AJR Am J Roentgenol 153:803–806
Mirvis SE (2005) Imaging of acute thoracic injury: the advent of MDCT screening. Semin Ultrasound CT MR 26:305–331
Sivit CJ, Taylor GA, Eichelberger MR (1989) Chest injury in children with blunt abdominal trauma: evaluation with CT. Radiology 171:815–818
Naples R, Ellison E, Brady WJ (2009) Cranial computed tomography in the resuscitated patient with cardiac arrest. Am J Emerg Med 27:63–67
Inamasu J, Miyatake S, Suzuki M, Nakatsukasa M, Tomioka H, Honda M, Kase K, Kobayashi K (2010) Early CT signs in out-of-hospital cardiac arrest survivors: temporal profile and prognostic significance. Resuscitation 81:534–538
Stein PD, Fowler SE, Goodman LR, Gottschalk A, Hales CA, Hull RD, Leeper KV Jr, Popovich J Jr, Quinn DA, Sos TA, Sostman HD, Tapson VF, Wakefield TW, Weg JG, Woodard PK (2006) Multidetector computed tomography for acute pulmonary embolism. N Engl J Med 354:2317–2327
Kuisma M, Alaspaa A (1997) Out-of-hospital cardiac arrests of non-cardiac origin. Epidemiology and outcome. Eur Heart J 18:1122–1128
Hoffmann U, Pena AJ, Moselewski F, Ferencik M, Abbara S, Cury RC, Chae CU, Nagurney JT (2006) MDCT in early triage of patients with acute chest pain. AJR Am J Roentgenol 187:1240–1247
White C, Read K, Kuo D (2006) Assessment of chest pain in the emergency room: what is the role of multidetector CT? Eur J Radiol 57:368–372
Malbranque G, Serfaty JM, Himbert D, Steg PG, Laissy JP (2011) Myocardial infarction after blunt chest trauma: usefulness of cardiac ECG-gated CT and MRI for positive and aetiologic diagnosis. Emerg Radiol 18:271–274
Taki K, Kato H, Hirahara K, Ito Y (1998) Difficulty to diagnose the cause of death in emergency room. Nihon Hoigaku Zasshi 52:223–226
Cho SH, Kim EY, Choi SJ, Kim YK, Sung YM, Choi HY, Cho J, Yang HJ (2013) Multidetector CT and radiographic findings of lung injuries secondary to cardiopulmonary resuscitation. Injury 44:1204–1207
Kim EY, Yang HJ, Sung YM, Cho SH, Kim JH, Kim HS, Choi HY (2011) Multidetector CT findings of skeletal chest injuries secondary to cardiopulmonary resuscitation. Resuscitation 82:1285–1288
Camden JR, Carucci LR (2011) Liver injury diagnosed on computed tomography after use of an automated cardiopulmonary resuscitation device. Emerg Radiol 18:429–431
Engelken FJ, Bosse G, Diederichs G (2011) A complication of cardiopulmonary resuscitation. Emerg Med J 28:173
Fitchet A, Neal R, Bannister P (2001) Lesson of the week: splenic trauma complicating cardiopulmonary resuscitation. BMJ 322:480–481
Offerman SR, Holmes JF, Wisner DH (2001) Gastric rupture and massive pneumoperitoneum after bystander cardiopulmonary resuscitation. J Emerg Med 21:137–139
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Seung Joon Choi and Hyung Sik Kim contributed equally to this work.
Rights and permissions
About this article

Cite this article
Choi, S.J., Kim, H.S., Kim, E.Y. et al. Thoraco-abdominal CT examinations for evaluating cause of cardiac arrest and complications of chest compression in resuscitated patients. Emerg Radiol 21, 485–490 (2014). https://doi.org/10.1007/s10140-014-1218-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-014-1218-0