
Abstract
Our study aimed to study the efficacy of ILIB on periodontal parameters and glycemic control in patients with periodontitis and type II diabetes. Twenty-one patients in a randomized clinical trial were divided into 2 groups: control group (CG), conventional periodontal therapy, and test group (TG), conventional periodontal treatment associated with 10 laser applications by the ILIB-Modified (ILIB-M) technique. Fasting blood glucose levels and glycated hemoglobin (HbA1c), visible plaque index (VPI), gingival bleeding index (GBI), and periodontal clinical parameters were evaluated at baseline and after 4 months (T4). Regarding periodontal parameters, the intragroup analysis showed a statistically significant reduction (p < 0.05) between baseline and T4, for the VPI, GBI, BOP, PD, and CAL indexes. However, in the intergroup analysis, no statistically significant improvements (p > 0.05) were observed between the TG and CG for the VPI, GBI, BOP, PD, and CAL indexes. Regarding HbA1C and fasting blood glucose values, no statistically significant improvements were observed in intergroup and intragroup analyses (p > 0.05). The Modified ILIB did not improve the periodontal clinical parameters and glycemic control in patients with type II diabetes.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Diabetes mellitus (DM) is a chronic metabolic disorder that can affect the supporting periodontal tissue and exacerbate another chronic disease, periodontitis [1,2,3]. DM patients usually present with more severe periodontal disease [4]. This characteristic can be attributed to changes in function of the immune system, vascularization, sulcular fluid composition, periodontal tissue repairing process, inflammatory response, bone tissue metabolism, and morphology [5, 6]. The use of low-intensity lasers in periodontal disease as an adjunct treatment has been suggested to influence inflammatory response modulation, tissue repair, and analgesia [7]. One of the low-level laser applications is the ILIB technique. The ILIB technique irradiates blood cells, showing effectiveness in the treatment of various chronic and acute conditions [8,9,10].
The antioxidant effect of ILIB treatment has been related to the stimulation of the enzyme superoxide dismutase (SOD), which is the main endogenous antioxidant system component. SOD is responsible for the dismutation of superoxide anion (O2*-) to hydrogen peroxide (H2O2), protecting aerobic organisms against superoxide radical reactivity and toxicity. Superoxide radical reactivity and toxicity are responsible for hydroxyl radical (HO*) formation and subsequent cellular toxicity with reactive oxygen species (ROS) [8,9,10,11,12,13]. The reduction in the HO* formation and ROS is associated with a decrease in chronic inflammatory responses [9, 12, 13].
Furthermore, ILIB seems to promote a cascade of reactions in the immune system that results in inflammatory response modulation, decreased edema and healing time, and analgesic effects [9, 14]. These effects are possibly related to the regulation of expression of growth factors, with an increased production of arginine and nitrous oxide and a decrease in production of the oxygen-free radical [9, 14].
Studies using ILIB as adjunctive therapy in patients with type II diabetes have found a significant effect in reducing blood glucose levels, suggesting this therapy as an effective adjunct treatment in controlling blood glucose levels in patients with type II diabetes [9, 15].
A new form of the ILIB application has emerged, called Modified ILIB (ILIB-M), which is considered easier because it does not require peripheral venous access [8,9,10, 16]. In this technique, the laser light indirectly irradiates the blood through a guide bracelet placed at the height of the radial artery where a low-intensity laser is attached [8,9,10, 16].
Although the biological effects of chronic diseases such as inflammation modulation and hemoglobin oxygenation are well studied, there are few studies in the literature regarding the effectiveness of improving the clinical parameters of patients who undergo adjunctive treatment with ILIB. The present study is the first that aims to investigate the efficacy of Modified ILIB for glycemic control and periodontal clinical parameters of patients with periodontitis and type II diabetes mellitus. This study is important because if prediabetes and early diabetes were treated effectively, then the progression of hyperglycemia could be prevented or delayed, which may subsequently lead to reduced progression of periodontitis.
Methods
This study followed the parameters detailed in CONSORT. It was characterized as a randomized-controlled clinical, parallel-group study and blinded trial conducted at the Dentistry Department of Federal University of Rio Grande do Norte (UFRN), in partnership with the Clinical Analysis Laboratory of the UFRN Pharmacy Faculty and the Onofre Lopes University Hospital (HUOL), Natal-RN, Brazil. The study was submitted to the Research Ethics Committee and approved under the protocol number 2,932,923, and was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013. All subjects agreed to participation by signing a Free and Informed Consent Form.
This study population consisted of patients diagnosed with periodontitis and type II diabetes. The subjects of this study were enrolled from January 2019 to June 2019.
Inclusion criteria were as follows: individuals with stage II, III, and IV periodontitis [17]; at least 18 years old; and the presence of at least two sites in different sextants with attachment loss ≥ 3 mm and bleeding on probing. The included participants also presented with a type II diabetes mellitus diagnosis, being prescribed supplementation and/or diet, insulin and/or oral hypoglycemic agents, and glycated hemoglobin levels (HbA1c) ≥ 6.5%. The exclusion criteria were as follows: smokers, people who used drugs that cause gingival hyperplasia, orthodontic appliances users, pregnant women, and lactating women.
For this study, 22 individuals met all inclusion criteria, but one participant was lost due to skin burns, caused by the application of ILIB. Thus, the total sample was 21 participants, of which 11 (52.3%) were in the control group and 10 (47.6%) were in the test group. Sixteen (76.1%) individuals were female and 5 (23.8%) individuals were male. The age range was between 45 and 77 years, with the median age being 61 years.
Data collection was executed by filling out a clinical form with three parts: medical history (including fasting blood glucose and HbA1c values), data collection related to oral hygiene VPI and GBI (visible plaque index and gingival bleeding index), and periodontal evaluation BOP, PD, and CAL (bleeding on probing, probing depth, and clinical attachment level). Data collection was performed by two experienced examiners, who were submitted to interexaminer calibration obtaining a value of 0.97 for quantitative variables following the precepts of the Intra-Class Correlation Index (ICC). Only one researcher was responsible for conducting the treatment, while the other two researchers conducted the evaluations.
Randomization for the study was executed by asking the participants to draw a card from a box to determine their assignment. A box containing 30 cards was used (15 with letter A and 15 with letter B). The participants who took the A card were allocated to the test group, while those who took the B card were assigned to the control group.
After the group assignment and data collection, the individuals underwent one of the two treatments described below:
Treatment A (test group)
Oral hygiene guidance + manual or ultrasound scaling and root planning (SRP) (two sessions, 48 h apart) + irradiation with a low-intensity laser using the Modified ILIB technique. The ILIB utilization protocol consisted of 1 low power laser application from Therapy EC-DMC (Equipment’s Ltda., São Carlos, SP, Brazil) with 10 sessions, lasting 30 min each application in lighter-skinned patients and 15 min in black patients (following the manufacturer’s recommendation), with an interval of 1 day per session, excluding the weekend. The laser has been configured in wavelength: 660 mm; action mode: contínuos wave; energy density: 6.428 J/cm2 (Fig. 1). In this technique, a silicone bracelet (supplied by the LASER manufacturer) is fitted on the patient’s wrist at the height of the radial artery. The laser tip was applied in contact with the skin. The low-intensity laser tip is then attached to this bracelet (Fig. 2, 3).

Source: author
Parameters involved in determining the low-power laser application. Natal/RN, 2019.

Source: author
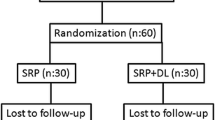
Experimental design. SRP: scaling root planning; VPI: visible plaque index; GBI: gingival bleeding index; BOP: bleeding on probing; PD: probing depth; CAL: clinical attachment level; ILIB: intravascular laser irradiation of blood.

Bracelet and laser application. A Silicone bracelet; B silicone bracelet at the height of the radial artery; C laser optic-fiber was positioned in silicone bracelet
Treatment B (control group)
Oral hygiene guidance + manual or ultrasonic manual or ultrasound SRP (two sessions, 48 h apart) (Fig. 2).
The information collected was entered into a spreadsheet in Microsoft Excel and a database was created in the Statistical Package for Social Sciences (SPSS®) program in version 20.0. Non-parametric tests were performed in the normality absence for analysis of the following variables: HbA1c, fasting blood glucose, VPI, GBI, PD, BOP, and CAL.
The Wilcoxon test was applied for intergroup analysis at each point. When a significant difference was observed, the Mann–Whitney test was applied. The 5% (p < 0.05) significance level was used for intragroup and intergroup evaluation.
Results
In this study, all oral hygiene indexes (VPI and GBI) and periodontal parameters (BOP, PD and CAL), had a statistically significant decrease of the median in the intragroup analysis from baseline to T4. However, there was no statistically significant difference in the intergroup analysis between the test and control groups in baseline and T4 (Table 1).
The patient’s glycemic control was determined by their HbA1c and fasting blood glucose values. For HbA1c, the control group showed an increase in the median between the study times, from 6.90 at baseline to 7.30 at T4. The test group showed no variation in the 8.15 median value between baseline and T4. For fasting blood glucose, there was an increase in the median of the control group from 124.00 mg/dL at baseline to 153.00 mg/dL at T4. In the test group, there was also an increase from a median of 133.50 mg/dL at baseline to 157.00 mg/dL at T4 (Table 2). In the intergroup analyses, there was no statistically significant difference between glycated hemoglobin and fasting glucose (Table 2).
The following confounding variables were evaluated: comorbidities other than diabetes, the use of drugs to control type II diabetes mellitus (oral hypoglycemic agents), or insulin and the diabetic patient’s metabolic compensation.
For the other comorbidities present and the use of drugs to control type II diabetes variables, no statistical difference was observed in the intragroup and intergroup analyses. When assessing the metabolic compensation confounding variable, a statistically significant reduction was found in the intragroup analysis for the GBI, BOP, PD, and CAL parameters. In the intergroup analyses, there was no statistically significant difference (p2 > 0.05) for metabolic compensation at baseline or T4 for GBI, PD, and CAL (Table 3). However, in the BOP baseline, a statistically significant result (p2 = 0.042) was observed in the intergroup analysis, in which the metabolically compensated patients presented 61.40% BOP, while the non-metabolically compensated patients presented 86.60% BOP (Table 3).
Discussion
Diabetic patients present with more aggressive periodontal disease, and for this reason, several studies seek adjuvant therapies to periodontal disease treatment. This was a pioneering study on the use of ILIB-M as an adjunct to basic periodontal treatment in diabetic patients. It was observed that ILIB-M use did not result in statistically significant improvements in periodontal parameters or glycemic control. Although, there was a reduction in the periodontal clinical parameters after periodontal treatment.
In our study, there was no statistically significant association (p < 0.05) when comparing the GBI, BOP, PD, and CAL periodontal parameters between test and control groups. Cheng et al. [17] carried out a systematic review with meta-analysis, which verified the use of photobiomodulatory therapy as adjunctive treatment to scaling and root planning wherein they found a reduction in BOP and PD (p < 0.05) after 3 months. When comparing the use of ILIB-M as an adjunct to periodontal treatment, we found different results than Cheng et al. [17], with no improvement in BOP and PD [18]. However, the results of our study concerning CAL do agree with Cheng et al. [17] who found no evidence to prove that clinical attachment gain with photobiomodulatory therapy use in adjuvant therapy to basic periodontal treatment [18].
There was a statically significant reduction (p < 0.05) in the intragroup analysis in both test and control groups regarding GBI, BOP, PD, and CAL periodontal indexes between baseline and T4. This result confirms the effectiveness of basic periodontal treatment with scaling and root planing and oral hygiene instruction for diabetic patients, resulting in decreased gingival inflammation and increased CAL. These findings corroborate the studies by Farman and Joshi [19], who claim that basic periodontal therapy to control periodontitis is effective [19].
Diabetic patients with periodontal disease present with an exacerbated inflammatory response and more severe clinical characteristics. Thus, the complete remission of clinical characteristics is more difficult in this patient group [1, 20]. In this study, there was a statistically significant reduction between baseline and T4 for the test and control groups in median BOP. However, even with this reduction, the median value for BOP in the control group was 38.80% and 35.44% in the test group. This shows that even after periodontal treatment, the patients still had active periodontal disease, considering that the recommended value for the periodontal health classification is less than 10% BOP [3, 21]. In this regard, the importance of periodontal support treatment for the adequate control of periodontitis in diabetic patients is highlighted [4].
Concerning the metabolic compensation, a statistically significant difference (p = 0.042) was observed for BOP in the baseline between the compensated and non-compensated diabetic patients. The metabolically compensated group had a BOP median of 61.40%, while the non-compensated group had a BOP median of 86.90%. This difference corroborates with studies by Mauri-Obradors et al. [1]; Ziukaite; Slot; Van Der Weijden [2], who report exacerbation of inflammatory response as a result from periodontitis in non-metabolically compensated diabetic patients [1, 2].
The BOP increase associated with metabolic decompensation occurs because hyperglycemia promotes excess glucose in the bloodstream and consequently in the body’s tissues [3]. This increase in glucose induces mitochondria to undergo an increase in stress and respiratory burst [3, 5]. This reaction can activate several pro-inflammatory mediator cascades. Advanced glycation end-products (AGEs) also form, which bind to their receptor, RAGE, activating a pro-inflammatory events cascade [3]. This cascade can exacerbate several inflammatory diseases, including periodontitis [3].
In this study, no improvement of glycemic control was observed in relation to the use of ILIB-M. Individuals who received ILIB-M showed no glycemic control improvement, with Hb1Ac being maintained at 8.15%.
Kazemikhoo and Ansari [9] conducted a study evaluating the efficacy of unmodified ILIB for glycemic control in patients with type II diabetes and found a 190 ± 17 reduction in the baseline to 165 ± 20 in T1 regarding the plasma glucose level reduction (p = 0.0018) [9]. In the Kazemikhoo and Ansari [21] study, T1 assessment was performed immediately after the ILIB application without assessing the treatment longevity. However, the present study found results different to those of Kazemikhoo and Ansari [21], with an increase in fasting blood glucose values in patients who received ILIB-M from 133.50 mg/dl at baseline to 154.00 mg/dl. This difference in findings can be justified by the variation of the techniques used in the studies by Kazemikhoo and Ansari [21] and Kazemikhoo et al. [9].
Kazemikhoo and Ansari [21] and Kazemikhoo et al. [9] used the unmodified ILIB technique. In this technique, peripheral venous access is recommended for laser application directly to blood cells [8, 9, 11, 14, 15, 22]. In the present study, the ILIB-M technique was used, where the laser is applied through the epidermis with a bracelet aid located at the height of the radial artery to irradiate blood cells [14, 15].
During this study, some limitations may have interfered with the final outcome, such as the lack of standardization in medical treatment for type II diabetes mellitus. The patients in this study were treated by different doctors, and the treatment for this clinical condition depends on the individual preference of each professional. Another possible study limitation may be related to the low rate of patient adherence to medical treatment for diabetes, either using the appropriate medication or reducing sugar consumption.
During the application of ILIB-M, it was observed that the patient may have performed small movements of their arm which can interfere with light absorption by the target cells, causing losses in the final result.
Patients with darker skin present a complex melanin chain, causing greater laser light absorption with little reflection [22]. Due to this characteristic, burns on the skin of these patients may occur [22, 23, 24]. For this reason, we suggest an application time of 15 min, according to the laser manufacturer’s recommendation, for dark-skinned patients. In our study, we excluded a dark-skinned patient because she presented with a skin burn after 30 min of ILIB application, characterized by hyperpigmented lesion with area of central excoriation and presence of a healing crust.
Future studies are needed that include an evaluation of SOD levels in various tissues and body fluids to assess the real ILIB-M effect in the chronic process reduction.
Conclusion
In conclusion, the use of the Modified ILIB technique did not provide a statistically significant improvement when comparing the periodontal parameters GBI, BOP, PD, and CAL and glycemic control, through Hb1Ac and fasting glycemia over 4 months. However, periodontal treatment was efficient in improving VPI, GBI, BOP, PD, and CAL in diabetic individuals, which reinforces the importance of controlling periodontitis in this population.
References
Mauri-Obradors E, Jané-Salas E, del Sabater-Recolons MM, Vinas M, López-López J (2015) Effect of nonsurgical periodontal treatment on glycosylated hemoglobin in diabetic patients: a systematic review. Odontology 103(3):301–13
Ziukaite L, Slot DE, Van der Weijden FA (2018) Prevalence of diabetes mellitus in people clinically diagnosed with periodontitis: a systematic review and meta-analysis of epidemiologic studies. J Clin Periodontol 45:650–62
Chapple ILC, Mealey BL, Van Dyke TE, Bartold PM, Dommisch H, Eickholz P, Geisinger ML, Genco RJ, Glogauer M, Goldstein M, Griffin TJ, Holmstrup P, Johnson GK, Kapila Y, Lang NP, Meyle J, Murakami S, Plemons J, Romito GA, Shapira L, Tatakis DN, Teughels W, Trombelli L, Walter C, Wimmer G, Xenoudi P, Yoshie H (2018) Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol 89 Suppl 1:S74–S84. https://doi.org/10.1002/JPER.17-0719
Miranda TS, Heluy SL, Cruz DF, da Silva HDP, Feres M, Figueiredo LC et al (2019) The ratios of pro-inflammatory to anti-inflammatory cytokines in the serum of chronic periodontitis patients with and without type 2 diabetes and/or smoking habit. Clin Oral Investig 23(2):641–650
Lalla E, Lamster IB, Feit M, Huang L, Spessot A, Qu W et al (2000) Blockade of RAGE suppresses periodontitis-associated bone loss in diabetic mice. J Clin Invest 105(8):1117–1124
Nascimento GG, Leite FRM, Vestergaard P, Scheutz F, López R (2018) Does diabetes increase the risk of periodontitis? A systematic review and meta-regression analysis of longitudinal prospective studies. Acta Diabetologica 55:653–67
Wang TF, Jen IA, Chou C, Lei YP (2014) Effects of periodontal therapy on metabolic control in patients with type 2 diabetes mellitus and periodontal disease: a meta-analysis. Medicine 93(28):e292
Huang SF, Tsai YA, Wu SB, Wei YH, Tsai PY, Chuang TY (2012) Effects of intravascular laser irradiation of blood in mitochondria dysfunction and oxidative stress in adults with chronic spinal cord injury. Photomed Laser Surg 30(10):579–586
Kazemi Khoo N, Iravani A, Arjmand M, Vahabi F, Lajevardi M, Akrami SM, et al (2013) A metabolomic study on the effect of intravascular laser blood irradiation on type 2 diabetic patients. Lasers Med Sci [Internet]. 28(6):1527–32. Available at: http://springerlink.bibliotecabuap.elogim.com/10.1007/s10103-012-1247-4https://doi.org/10.1007/s10103-012-1247-4
Mr L, Hf H, Mh H, Hdi W, Yw W, Fc H (2004) Psychometric comparisons of the timed up and go, one-leg stand, functional reach, and Tinetti balance measures in community-dwelling older people. J Am Geriatr Soc 52(8):1343–1348
Tóthová L, Celec P (2017) Oxidative stress and antioxidants in the diagnosis and therapy of periodontitis. Front Physiol 8:1055. https://doi.org/10.3389/fphys.2017.01055
L T, P C (2017) Oxidative stress and antioxidants in the diagnosis and therapy of periodontitis. Front Physiol [Internet]. 8(DEC). Available at: http://www.embase.com/search/results?subaction=viewrecord&from=export&id=L619684541%0Ahttps://doi.org/10.3389/fphys.2017.01055
Tomé RFF, Silva DFB, dos Santos CAO, de Vasconcelos Neves G, Rolim AKA, de Castro Gomes DQ (2020) ILIB (intravascular laser irradiation of blood) as an adjuvant therapy in the treatment of patients with chronic systemic diseases—an integrative literature review. Lasers Med Sci 35(9):1899–1907. https://doi.org/10.1007/s10103-020-03100-4
Kazemikhoo N, Ansari F, Nilforoushzadeh (2016) The hypoglycemic effect of intravenous laser therapy in diabetic mellitus type 2 patients; a systematic review and meta-analyses. Med Clin Rev 1(1:7). https://doi.org/10.21767/2471-299X.1000007
Kazemikhoo N, Sarafnejad AF, Ansari F, Mehdipour P (2016) Modifying effect of intravenous laser therapy on the protein expression of arginase and epidermal growth factor receptor in type 2 diabetic patients. Lasers Med Sci 31(8):1537–1545
Moshkovska T, Mayberry J (2005) It is time to test low level laser therapy in Great Britain. Postgrad Med J 81(436):41
Papapanou PN, Sanz M, Buduneli N, Dietrich T, Feres M, Fine DH, Flemmig TF, Garcia R, Giannobile WV, Graziani F, Greenwell H, Herrera D, Kao RT, Kebschull M, Kinane DF, Kirkwood KL, Kocher T, Kornman KS, Kumar PS, Loos BG, Machtei E, Meng H, Mombelli A, Needleman I, Offenbacher S, Seymour GJ, Teles R, Tonetti MS (2018) Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol 45 Suppl 20:S162–S170. https://doi.org/10.1111/jcpe.12946
Moskvin SV (2017) Low level laser therapy in Russia: history science and practice. J Lasers Med Sci 8:56–65
Cheng Y, Chen JW, Ge MK, Zhou ZY, Yin X, Zou SJ (2016). Efficacy of adjunctive laser in non-surgical periodontal treatment a systematic review and meta-analysis. Lasers Med Sci 31(151):63
Farman M, Joshi RI (2008) Full-mouth treatment versus quadrant root surface debridement in the treatment of chronic periodontitis: a systematic review. British Dent J 205
KazemiKhoo N, Ansari F (2014) Blue or red: which intravascular laser light has more effects in diabetic patients? Lasers Med Sci 30(1):363–366
Arora N, Mishra A, Chugh S (2014) Microbial role in periodontitis have we reached the top? Some unsung bacteria other than red complex. J Indian Soc Periodontol 18:9–13
Muniz FW, Nogueira SB, Mendes FL, Rösing CK, Moreira MM, de Andrade GM, de Sousa Carvalho R (2015) of antioxidant agents complimentary to periodontal therapy on oxidative stress and periodontal outcomes: A systematic review. Arch Oral Biol 60(9):1203–1214. https://doi.org/10.1016/j.archoralbio.2015.05.007
Huang YY, Chen ACH, Carroll JD, Hamblin MR (2009) Biphasic dose response in low level lightherapy. Dose-Response 7(4):358–383
Acknowledgements
The authors would like to thank the support of UFRN for allowing this study to be possible, and the Coordination for the improvement of Higher Education Personnel (CAPES) for their support during the preparation of this article.
Funding
The authors received funding from the Coordination of Improvement of Higher Education Person (CAPES).
Author information
Authors and Affiliations
Contributions
The authors have no relevant financial or non-financial interests to disclose.
Corresponding author
Ethics declarations
Ethics approval
This study was submitted to the Research Ethics Committee and approved under the protocol number 2,932,923, and was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
da Silva Júnior, F.L., de Araújo Silva, D.N., da Silva Azevedo, M.L. et al. Efficacy of ILIB on periodontal clinical parameters and glycemic control in patients with periodontitis and type II diabetes—randomized clinical trial. Lasers Med Sci 37, 1945–1952 (2022). https://doi.org/10.1007/s10103-021-03455-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-021-03455-2