
Abstract
Laser endodontic tips appear to provide a promising alternative to available treatment modalities in the field of endodontology. With the shortcomings in published results regarding the intra-canal behavioural aspects of those tips, it was the aim of this study to investigate the extent of the intra-canal ablation zone and the pattern associated with those tips. Ninety intact extracted bovine teeth were used to prepare mid-root testing cylinders. The samples were divided into three groups (A, B, C), corresponding to the tip diameters. Each group was further subdivided to be irradiated at three different power settings (1500 mW, 1750 mW, 2000 mW) with an erbium, chromium:yttrium–scandium–gallium–garnet (Er,Cr:YSGG) laser with a 65% water to 35% air ratio. Collected data were subjected to analysis of variance (ANOVA) and the Tukey test. At a chosen significance level of α = 1%, no statistical difference was found among the groups (P > 0.01). The results suggest that shortening of the estimated working length is mandatory for the use of those tips within the canal, and that, provided that certain measurements are used for intra-canal laser ablation, this is a secure mode of treatment. Further investigation and system improvement will be required for more satisfactory results.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Currently available dental laser systems represent an advanced state of scientific and technical refinement in terms of performance and user features, with a wide variety of wavelengths and pulse widths.
Such innovations allow those systems to be incorporated into many endodontic applications, including; direct pulp capping, drying of the canal, modification of canal walls, canal disinfection, shaping and preparation [1–3]. Yet, there are still restrictions that may be associated with the intra-canal use of laser that cannot be disregarded. Topics such as laser preparation and shaping of the root canal have always been subjects of controversy and discussion, ever since the concept was suggested in the early 1990s [2, 4–7].
The most critical aspect associated with such applications is the laser beam interaction inside the canal lumen. In this context, the fact points out that laser activity extending beyond the distal end of the fibre tips represents an essential issue to be investigated. In this regard, the emission of the laser beam in the area surrounding the apical third of the canal may result in transmission of the irradiation beyond the foramen, with the possible hazard of adversely affecting the supporting tissue of the root [8].
However, to date, there is still insufficient information regarding the choice of the optimum preparation parameters that will lead to the desired clinical treatment goals without causing iatrogenic damage to the root canal system and the surrounding tissue [9–12]. Also, to our knowledge, papers investigating criteria such as the extent of the ablation zone associated with different pulse energies and tip diameters have not yet been published.
Therefore, it was our purpose to determine the extent of the ablation zone (the limitation of the changes in intra-canal dentine, measured from the zero level) of the available endodontic tips under specific experimental environments and using different power settings.
Material and methods
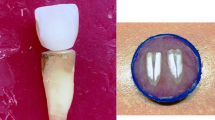
Selection of samples
Ninety intact extracted bovine teeth were selected as the sample material [13–15]. All samples were cleaned and sterilized, and the crown of each tooth was resected at the cemento-enamel junction with a water-cooled diamond saw (Exact Apparatus GmbH, Hamburg, Germany).
Each root was further sectioned and polished to provide cylinders of middle root dentine 10 mm long and 1.5–4 mm in internal canal diameter, with a flat base that was marked to indicate zero reference level.
The samples were divided according to internal canal diameters into three main groups that corresponded to different endodontic tip sizes. Also, each was further sub-divided into ten samples to be irradiated at three laser power settings (1500 mW, 1750 mW, 2000 mW, respectively).
To reduce possible experimental error, we investigated the actual power outputs at the distal end of endodontic tips using an energy meter (Coherent Zone Master, USA) and an energy detector (Coherent, model LM-P10i, USA). Complete calibration data list for each tip size and length were obtained (Fig. 1); accordingly, certain fibre lengths and sizes were selected. The average calibration factors calculated were 0.31 for 200 µm tips (Z2), 0.61 for 320 µm tips (Z3), and 0.65 for 400 µm tips (Z4).

Actual power output measured at the distal ends of three endodontic tips, plotted against the display setting power
The sample grouping, tip sizes, lengths and actual power outputs with calibration factors are summarized in Table 1.
Source of laser radiation and delivery system
An erbium, chromium:yttrium–scandium–gallium–garnet (Er,Cr:YSGG) laser (Waterlase Millennium®, Biolase Technology Inc., San Clemente, CA, USA), emitting at a wavelength of 2.78 µm, was used for this investigation. For all experiments, the pulse duration was 140 µs, with a pulse repetition rate of 20 Hz. The laser beam was delivered into the canal with a fibre-optic tube terminated by silica endodontic tips of different diameters, Z2, Z3 and Z4.
Each subgroup was irradiated according to selected parameters. The protocol involved insertion of the specific tip size into the canal to a previously marked 3 mm level, following which, each canal was irradiated for 60s with a circumferential movement of the tip inside the canal.
The experiments were performed according to the manufacturer’s instructions under a 65% air and 30% water level.
Evaluation of ablation zone extent and pattern
For evaluation of the extent and pattern of the achieved ablation zone, the samples were longitudinally sectioned to provide two symmetrical semi-cylinders. The extent of the ablation zone in the internal surface of each part was examined under a refractory light microscope (Leica MZ6 with integrated Hitachi HV-C20A camera, Wetzlar, Germany), and the means of at least six readings per single sample were calculated by a computer program (Diskus, Koenigswiner, Germany). As a result, average readings were obtained that demonstrated the extent of the ablation zone for each single application.
Meanwhile, the morphological changes associated with the ablation zones were investigated, and the different shapes and patterns were identified.
Data analysis and statistics
The results were statistically processed with SAS software to demonstrate that the testing variables interacted. At a chosen significance level of α = 1%, two-way analysis of variance (ANOVA) was used for multiple comparisons to calculate the P value for the means of the extent of the ablation in the perspective of two independent variables (tip size and power setting) followed by a Tukey test to distinguish the specific different groups if present.
Furthermore, we used Pearson’s product moment correlation coefficient (PMCC) to estimate the correlation value for the tested criteria.
Results
Independent of the experimental group, ablation was detected in all irradiated samples. The results of the descriptive statistical analysis are summarized in Table 2.
Extent of ablation (ANOVA and Tukey statistical models)
Depending on descriptive statistical findings and as demonstrated in Fig. 2, the ablation zone showed a trend of increasing linear correlation with increased display power level, for both different tip diameters and a single tip diameter.

Extent of intra-canal ablation zone plotted against the tip diameters
Moreover, a similar linear increase could be achieved with increasing tip diameter using similar display power levels. Nevertheless, the inferential statistical results revealed no significant difference between the groups for both tip and power variances, as shown in Table 3.
Additionally, altered ablation pattern was demonstrated in group B when both 1500 mW and 1750 mW display power levels were compared.
For 3 tested tip diameters the maximum ablation zone was achieved at a level of 2000 mW.
Pearson’s PMCC
The results of the correlation analysis according to Pearson’s PMCC showed that high correlation tendency (>0.7) was found between both the power level and tip diameter vs the extent of the ablation zone.
Analysis of surface morphology and ablation pattern
Macroscopically, the ablation fields generally were presented as a perceived zone among the normal appearing dentine structure. The appearances varied, from slight changes in the colour to distinguishable texture alterations that could be recognized easily from the surrounding normal dentine structure.
Microscopically, two of the 90 samples showed no visible ablation zone (Table 2); the remaining samples revealed different patterns of ablation zones.
When the different ablation zones were examined, the images of the sections from a single sample revealed irregular and asymmetrical distribution of those zones, both of pattern and location. The images revealed the uneven extent of a single zone, both parallel and perpendicular to the beam axis, with two main ablation patterns of longitudinal and annular shape.
While some sections showed a well-defined distal margin for the ablation zone, where they were easily differentiated from the adjacent normal dentine structure, others showed indistinct and vague margins, in which both zones (ablated and normal) were overlapping and disrupting each other. Those findings were demonstrated independently and could not be assigned to any particular power level setting or tip diameter.
The different patterns of the ablation fields are demonstrated in Fig. 3.

Representative photographs demonstrate the different patterns of the dentine ablation zones within the canal that were obtained in this study. a Continuous ablation zone with marked alteration of the dentine surface. b Fine patches with indistinct ablation margins. c Poorly defined ablation margin with moderate surface alteration. d Well-defined ablation margin with modified dentine surface. ×40
With regard to the characteristic features of specific ablation zones associated with different tip groups, the following could be summarized.
-
1.
Group A. The zones showed a common feature of more superficial ablation, with the shape ranging from very fine and widely distributed white spots to well-defined patches of textural alterations (Fig. 4).
-
2.
Group B. The zones were more recognizable, with distinguishable colour and texture alterations. Also, the shapes ranged from irregularly distributed patches of ablation to a well-defined finger/wave-shaped zone with a well-recognizable area of dentine surface indentation and scraping (Fig. 5).
-
3.
Group C. Results similar to those for Group B were demonstrated, with higher distinguishable zones of dentine removal that was mostly in the form of undulating projections of changed dentine texture (Fig. 6).

Representative photographs demonstrate the pattern of dentine ablation within the canal observed in group A. ×40

Representative photographs demonstrate the pattern of dentine ablation within the canal observed in group B. ×40

Representative photographs demonstrate the pattern of dentine ablation within the canal observed in group C. ×40
At the chosen level of magnification, no cracks or fractures were discernible. Furthermore, for all the groups tested, no carbonization in the ablation field was detected and the remaining tooth structure was free of any charring.
Discussion
As more conservative approaches for root canal preparation have been proposed, to prevent extensive substance loss and preserve the original shape of the canal, the therapeutic armamentarium for endodontic practice has been widely broadened. As a replacement for traditional methods or/and for use in conjunction, lasers have demonstrated beneficial effects in endodontic practice over the past decade.
In this study, the intra-canal ablation pattern of a pulsed infrared Er,Cr:YSGG laser beam was investigated. The ablation zones achieved were evaluated as a function of power and tip diameter.
Interestingly, the data obtained from the extent of the ablation zone observed for the three different groups showed no statistical difference. Nevertheless, for the recorded average value of 1.77 mm for all the groups tested, our findings agree only with those of George and Walsh [16] and support the tip shortening protocol suggested by Matsuoka et al. [12], while they agree partially with those of Berk et al. [17]. As none of the achieved results for Z4 tip size would indicate 4 mm shorting in the working length of the tip as proposed by the this group, accordingly decreasing the working length for the tips to be used is strongly recommended to preserve the apical seat and to prevent any damaging effect to the peri-apical surrounding tissue.
Morphologically, although the achievable ablated surface qualities were varied, it has been shown that the use of this instrument allows the removal of intra-canal dentine while maintaining the normal dentine structure of the surrounding tissues [12, 18].
Furthermore, due to the small laser beam angulation obtained during the movement of those tips inside the canal lumen, and the axial beam distribution pattern incorporated in the tested tip design, the specific tip energy density seems to have a minor effect on the surface alteration. More pronounced morphological changes were found with increasing tip diameter; this could be mainly attributed to the higher average actual powers recorded for Z4 tips than for Z3 and Z2 tips (1,133, 1,032, 533 mW, respectively). Finally, the above morphological findings showed distinctive difference from those obtained with laser ablation during cavity preparation. This was mainly attributed to the different tip angulation used in both procedures as well as higher energy and pulse fluence setting used in cavity preparation [19–21].
Conclusion
The results obtained in this study showed no noticeable differences between the groups with regard to the criteria for the extent of the ablation zone. A minimum of 2 mm shortening of the estimated working length for all tips is compulsory if the apical root region is to be preserved.
With the characteristic patterns of the ablation zones obtained with the tips in this study, it is our belief that alteration in the tip design to ensure that there is a more annular profile of the side firing beam inside the canal is mandatory if we are to produce a more uniform and homogeneous ablation pattern that will positively improve the final outcome of the application. Moreover, further investigations are necessary to demonstrate the effect of other factors that might influence the energy distribution of the laser beam within the canal.
Finally, this study was only an initial attempt at evaluating important aspects of laser beam interactions within the canal under restricted experimental conditions in vitro. Additional clinical studies are necessary to confirm the results that we obtained.
References
Walsh LJ (2003) The current status of laser application in dentistry. Aust Dent J 48:146–155
Stabholz A, Sahar-Helft S, Moshonov J (2004) Lasers in endodontics. Dent Clin North Am 48:809–832
Albert M, Kremer L, Salzmann K, Hickel R (1997) 3D volume–ablation rate and thermal side effects with Er:YAG and Nd:YAG laser. Dent Mater 13:246–251
Kimura Y, Wilder-Smith P, Matsumoto K (2000) Laser in endodontics: a review. Int Endod J 33:173–185
Gutknecht N (2003) Laser in endodontics: preconditions for therapeutically success. Int Congr Ser 1248:101–108
Levy G (1992) Cleaning and shaping the root canal with a Nd:YAG laser beam: a comparative study. J Endod 18:123–127
Mazeki K, Kojy R, Saito K, Funato A, Matsumoto K (1998) Morphological study on preparation of root canal orifices by Er:YAG laser. J Jpn Endod Assoc 19:5–9
Matsuoka E, Yonaga K, Kinoshita J, Kimura Y, Matsumoto K (2000) Morphological study on the capability of Er:YAG laser irradiation for root canal preparation. J Clin Laser Med Surg 18:215–219
Ishizaki NT, Matsumoto K, Kimuro Y, Wang X, Kinoshita JI, Okano S, Jayewardena JA (2004) Thermographical and morphological studies of Er, Cr:YSGG laser irradiation on root canal walls. Photomed Laser Surg 22:291–297
Ali MN, Hossain M, Aakamura Y, Matsoka E, Kinoshita JI, Latsumoto K (2005) Efficacy of root canal preparation by Er, Cr:YSGG laser irradiation with crown-down technique in vitro. Photomed Laser Surg 23:196–201
Jahan KM, Hossain M, Nakamura Y, Yoshishige Y, Kinoshita JI, Matsumoto K (2006) An assessment following root canal preparation by Er, Cr:YSGG laser irradiation in straight and curved roots, in vitro. Lasers Med Sci 21:229–234
Matsuoka E, Jayawardena JA, Matsumoto K (2005) Morphological study of the Er, Cr:YSGG laser for root canal preparation in mandibular incisors with curved root canals. Photomed Laser Surg 23:480–484
Schilkea R, Lissonb JA, Bauûa O, Geurtsena W (2000) Comparison of the number and diameter of dentinal tubules in human and bovine dentine by scanning electron microscopic investigation. Arch Oral Biol 45:355–361
Fonseca RB, Haiter-Neto F, Fernandes-Neto AJ, Barbosa GA, Soares CJ (2004) Radiodensity of enamel and dentin of human, bovine and swine teeth. Arch Oral Biol 49:919–922
Dutra-Correa M, Anauate-Netto C, Arana-Chavez VE (2007) Density and diameter of dentinal tubules in etched and non-etched bovine dentine examined by scanning electron microscopy. Arch Oral Biol 52:850–855
George R, Walsh LJ (2008) Apical extrusion of root canal irrigants when using Er:YAG and Er, Cr:YSGG lasers with optical fibers: an in vitro dye study. J Endod 34:706–708
Berk G, Ulucam S, Berk N (2004) Clinical healing process and symptoms of two cases of chronic periapical lesions treated with Er, Cr:YSGG laser. J Oral Laser Appl 4:211–215
Eversole LR, Rizoiu I, Kimmel AI (1997) Pulpal response to cavity preparation by an erbium, chromium:YSGG laser-powered hydrokinetic system. J Am Dent Assoc 128:1099–1106
Harashima T, Kinoshita JI, Kimura Y, Brugnera A Jr, Zanin F, Pecora JD, Matsumoto K (2005) Morphological comparative study on ablation of dental hard tissues at cavity preparation by Er:YAG and Er, Cr:YSGG lasers. Photomed Laser Surg 23:52–55
Mir M, Meister J, Franzen R, Sabounchi SS, Lampert F, Gutknecht N (2008) Influence of water-layer thickness on Er:YAG laser ablation of enamel of bovine anterior teeth. Lasers Med Sci 23:451–457
Iaria G (2008) Clinical, morphological, and ultrastructural aspects with the use of Er:YAG and Er, Cr:YSGG lasers in restorative dentistry. Gen Dent 56:636–639
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Minas, N.H., Gutknecht, N. & Lampert, F. In vitro investigation of intra-canal dentine–laser beam interaction aspects: II. Evaluation of ablation zone extent and morphology. Lasers Med Sci 25, 867–872 (2010). https://doi.org/10.1007/s10103-009-0722-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10103-009-0722-z