
Abstract
Torque teno virus (TTV) and torque teno mini virus (TTMV) have been potentially related to liver diseases. The aim of the study was to quantify TTV and TTMV in human immunodeficiency virus (HIV)/hepatitis C virus (HCV)-coinfected patients to study the relationship between the TTV and TTMV viral loads and the severity of liver disease. We carried out a cross-sectional study in 245 patients coinfected with HIV and HCV (HIV/HCV-group), 114 patients monoinfected with HIV (HIV-group), and 100 healthy blood donors (Control-group). Plasma samples were tested for TTV and TTMV by quantitative real-time polymerase chain reaction (PCR). The prevalences of TTV and TTMV infections in the HIV/HCV-group and the HIV-group were significantly higher than the Control-group (p < 0.05). Furthermore, TTV and TTMV coinfections were found in 92.2 % (226/245) in the HIV/HCV-group, 84.2 % (96/114) in the HIV-group, and 63 % (63/100 %) in the Control-group (p ≤ 0.05). HIV/HCV-coinfected patients with HIV viral load ≥50 copies/mL and patients with severe activity grade had the highest viral loads of TTV and TTMV (p ≤ 0.05). HIV/HCV-coinfected patients with high TTV load (>2.78 log copies/μL) had increased odds of having advanced fibrosis or severe necroinflammatory activity grade in the liver biopsy. Moreover, HIV/HCV-coinfected patients with high TTMV load (>1.88 log copies/μL) had decreased odds of having no/minimal fibrosis and no/mild activity grade, and increased odds of having a high fibrosis progression rate. In conclusion, TTV and TTMV might play a role in the development of liver disease in immunodeficiency patients, such as the patients coinfected with HIV and HCV.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
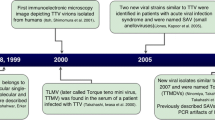
Two human anelloviruses, torque teno virus (TTV) and torque teno mini virus (TTMV), were described in the 1990s [1, 2]. TTV was first identified in a patient with post-transfusion hepatitis of unknown etiology [1] and TTMV was discovered shortly afterwards due to its homology with TTV [2]. Both anelloviruses appear to be present in the majority of individuals [3, 4]. The evidence indicates that infection with TT viruses is acquired in early childhood via perinatal and horizontal routes (fecal–oral, mother–child, and family contacts), while the parenteral and sexual routes appear to be predominant for infection in adulthood [4–6].
TTV and TTMV are persistent viruses, as shown in serial samples where the same DNA sequences were found repeatedly [7, 8], and plasma/serum viral load is the best marker of the activity or reactivation of TT viruses. Moreover, the viral load of TT viruses in healthy individuals is known to be generally low [9]; however, increased prevalence has been reported in persons infected with human immunodeficiency virus (HIV) [10, 11] and patients with hepatitis [12].
TT viruses may be in the semi-latency state and increase their level of replication in cases of immunodeficiency [13]. In addition, HIV infection predisposes to opportunistic infections, although the level of CD4+ cells was not too low [14]. The TTV load has been proposed as an indirect marker of cellular immune response at a functional level in patients infected with HIV who receive highly active antiretroviral therapy (HAART) [15] and patients who receive autologous stem cell transplantation [13].
TTV apparently replicates in liver cells, as circular double-stranded forms of TTV DNA have been detected in liver tissues [16, 17], but the exact role of TTV in liver diseases has not yet been defined. In one study, no correlation was found between the acquisition of TTV infection and the development of clinical symptoms of hepatitis [18]. However, other studies have found an association between the dynamics of TTV viremia and transient abnormalities in the liver enzyme levels that may influence the progression of liver disease in hepatitis C virus (HCV)-monoinfected patients [19, 20]. Although it does not seem that TTV infection provokes liver injury in humans, it is important to clarify whether coinfection with TTV promotes the progression of liver disease in patients with chronic hepatitis C [21–23].
The aim of this study was to quantify TTV and TTMV in patients coinfected with HIV and HCV to study the possible relationship between the viral load of TTV and TTMV and the severity of liver disease.
Patients and methods
Patients
A retrospective cross-sectional study was performed on 245 patients coinfected with HIV and HCV (HIV/HCV-group) of the Hospital Gregorio Marañón in Madrid (Spain), who underwent a liver biopsy between May 2000 and May 2007. Additionally, we included two control groups with similar age and gender values to those HIV/HCV-coinfected patients: (a) patients monoinfected with HIV (HIV-group): 114 HIV-infected patients but without HCV or human B virus (HBV) infections; b) healthy control group (Control-group): 100 healthy blood donors of the Centro de Transfusión of the Comunidad de Madrid participated as a control group, all of which were negative for HCV, HBV, and HIV [24]. The studies were conducted in accordance with the Declaration of Helsinki. All patients gave their written consent for the liver biopsy and the Institutional Ethics Committee approved the study.
On the day of the liver biopsy, the following information was obtained from medical records: age, gender, height, weight, risk category, Centers for Disease Control and Prevention (CDC) clinical category, nadir CD4+, CD4+ T-cells, antiretroviral therapy, complete blood counts, HIV and HCV viral loads, HCV genotype, and liver and basic metabolic panel.
Liver biopsy and fibrosis
Liver biopsies were only performed on patients coinfected with HIV and HCV who were potential candidates for anti-HCV therapy and had not received previous interferon therapy, following the recommendations of the Patient Care Committee of the American Gastroenterological Association [25]. All liver biopsies were performed by the same physicians (J.B. and P.M.) with a suction needle (HISTO-CUT 16G, Sterylab Srl., Milano, Italy). Ultrasound was routinely used to determine the percutaneous biopsy site. The liver tissue sections were fixed in formalin, embedded in paraffin, and stained by hematoxylin-eosin, Mason’s trichrome, and Perls’ iron. The samples were evaluated by a pathologist (E.Á.), who was unaware of the patients’ clinical or laboratory data.
Liver fibrosis was estimated following the criteria established by the METAVIR Cooperative Study Group [26]. Fibrosis was scored as follows: F0, no fibrosis; F1, portal fibrosis; F2, periportal fibrosis or rare portal–portal septa; F3, fibrous septa with architectural distortion; no obvious cirrhosis (bridging fibrosis); and F4, definite cirrhosis. Activity grade was scored as follows: A0, no activity; A1, mild activity; A2, moderate activity; A3, severe activity.
In each patient, the fibrosis progression rate (FPR) was calculated dividing the fibrosis stage (0 to 4) by the estimated duration of HCV infection in years. The duration of HCV infection was calculated assuming that HCV infection was acquired in the first year needles were shared. For patients without a history of intravenous drug use, we only had certainty of the infection date in two patients who were infected by blood transfusion and three other patients who were infected by sexual contact. We selected a cut-off of 0.08 (median value) to classify the patients with low or high fibrosis progression.
Quantitative real-time PCR
Plasma samples were obtained at the time of liver biopsy and stored at −80 °C. Viral DNA was extracted from 200 μl of plasma using the QIAamp® MiniElute® Virus Spin Kit (Qiagen, Hilden, Germany) in a QIAcube automated extractor (Qiagen), as recommended by the manufacturer.
Real-time polymerase chain reaction (RT-PCR) of a TTV and TTMV conserved region of approximately 150 nt [2] was performed in a LightCycler Instrument version 1.5 (Roche Diagnostics, Mannheim, Germany). The RT-PCR Ct scores (number of cycles required to bring the amount of product above a certain threshold) were converted to the number of viral genomes by using standard curves based on the amplification of dilutions of purified PCR products. Standard regression analyses gave reasonably linear results when plotting the Ct values against the log of template DNA copies, in the range 1.5 log10–1.5 × 1011 log10. The slope coefficients of the standard curves (−3.80 for TTV PCR and −3.51 for TTMV PCR) indicated that, with PCR products as templates, both the TTV and the TTMV real-time PCRs were nearly 100 % efficient (in a 100 % effective PCR, the slope should be −1/log 2 = −3.32). Negative and positive controls were included.
The PCR protocol was as follows: 4 μl of TaqMan Master Mix (Roche Diagnostics, Mannheim, Germany), 0.5 μM each primer, 0.2 μM TaqMan probe, and 5 μl DNA extract (or standard) in a 20-μl total reaction volume. The DNA polymerase was activated for 10 min at 95 °C, followed by 45 cycles of amplification: 10 s at 95 °C and 1 min at 62 °C. Primers were as follows: TTVf, 5′-GTT TTC TAC GCC CGT CC-3′ (115–131); TTVr, 5′-CCT TGA CTC CGG TGT GTA A-3′ (210–192); TTMVf, 5′-AGT TTA TGC CGC CAG ACG-3′ (193–210); and TTMVr, 5′-CCC TAG ACT TCG GTG GTT TC-3′ (287–268). The TaqMan probe, TTV/TTMVpb, was (6-FAM) 5′-ACT CAC CTH CGG CAC CCG C-3′ (TAMRA) (191–173) [27].
Statistics
Log transformation was performed for all variables that were not normally distributed. The analysis of variance (ANOVA) test was used to compare differences of means between two or more groups adjusted by the Bonferroni Test. Moreover, we used the Mann–Whitney test to compare the means of two groups when the data distribution did not follow a normal distribution.
For analysis of the influence of high viral load of TTV and TTMV in liver disease, logistic regression analysis was performed. For this, we selected a cut-off near the 75th percentile of TTV and TTMV viral loads in HIV patients coinfected with HCV. Next, we carried out a univariate linear regression analysis to evaluate the association of several cut-offs to the METAVIR score (fibrosis stage and activity grade of liver biopsy). Multivariate logistic regression was used to evaluate the association between high viral load of TTV and TTMV and METAVIR score adjusted for clinical and epidemiological characteristics.
All tests were two-tailed, with p-values <0.05 considered to be significant. Statistical analysis was performed by SPSS 15.0 software (SPSS, Chicago, IL, USA).
Results
Patients
This study included 245 patients coinfected with HIV and HCV, whose characteristics at the time of liver biopsy are shown in Table 1. Overall, the median age of the patients was 39.8 years, 75.1 % were males, 30.2 % had had prior acquired immunodeficiency syndrome (AIDS)-defining conditions (ADCs), the median CD4+ count was 483 cells/mm3, 69.3 % had an HIV viral load <50 copies/mL, and 57.9 % were infected with HCV genotype 1. Advanced fibrosis (F ≥ 3) was found in 24.9 % and severe activity grade (A3) in 15.1 % of the patients.
Prevalence of TTV and TTMV infection
The prevalence of TTV and TTMV infections in the HIV-group and the HIV/HCV-group were significantly higher than the Control-group (p < 0.001) (Table 2). Furthermore, more TTV and TTMV coinfections were found in the HIV/HCV-group and the HIV-group than in the Control-group (p <0.001) (Table 2).
The viral loads of TTV and TTMV were significantly higher in the HIV/HCV-group and the HIV-group than the Control-group (p < 0.05) (Fig. 1). In addition, the HIV/HCV-group had higher viral loads of TTV and TTMV than the HIV-group (p < 0.05). In the HIV/HCV-group, the 75th percentile of the TTV viral load was 2.78 log copies/μL (605 copies/μL) and for the TTMV viral load, it was 1.88 log copies/μL (77 copies/μL).

Viral loads for TTV (a) and TTMV (b) in the three main groups studied. HCV hepatitis C virus; HIV human immunodeficiency virus; TTV torque teno virus; TTMV torque teno mini virus
TTV and TTMV infections among patients infected with HIV
The viral loads of TTV and TTMV were significantly higher in HIV/HCV-coinfected patients with HIV viral load ≥50 copies/mL than in HIV/HCV-coinfected patients with HIV viral load <50 copies/mL, the HIV-group, and the Control-group (p < 0.05) (Fig. 2). Besides, HIV/HCV-coinfected patients with HIV viral load <50 copies/mL and HIV-infected patients with HIV viral load ≥50 copies/mL had higher viral loads of TTV and TTMV than the Control-group (Fig. 2).

Summary of TTV and TTMV viral loads according to HIV viral load at the time of liver biopsy in HIV/HCV-coinfected patients. Statistically significant differences (p < 0.05) among patients according to HIV viral load: (a) healthy control; (b) HIV-infected patients with HIV viral load <50 copies/mL; (c) HIV-infected patients with HIV viral load ≥50 copies/mL; (d) HIV/HCV-coinfected patients with HIV viral load <50 copies/mL. HCV hepatitis C virus; HIV human immunodeficiency virus; TTV torque teno virus; TTMV torque teno mini virus
TTV and TTMV infections and chronic hepatitis C
The viral loads of TTV and TTMV were higher in HIV/HCV-coinfected patients with severe activity grade (A3) than HIV/HCV-coinfected patients with moderate (A2) and patients with low activity grade (A0/A1), as well as compared to the HIV-group and the Control-group (p < 0.05) (Fig. 3a). Likewise, the viral loads of TTV and TTMV were significantly higher in HIV/HCV-coinfected patients with moderate (A2) and patients with low activity (A0/A1) than the HIV-group and the Control-group (p < 0.05) (Fig. 3a).

Summary of viral load values of TTV and TTMV according to METAVIR score. Statistically significant differences (p < 0.05) among patients according to activity grade (A): (a) healthy control; (b) HIV-infected patients; (c) HIV/HCV-coinfected patients with A0/A1; (d) HIV/HCV-coinfected patients with A2. Statistically significant differences (p < 0.05) among patients according to fibrosis stage (B): (a) healthy control; (b) HIV-infected patients; (c) HIV/HCV-coinfected patients with F0/F1; (d) HIV/HCV-coinfected patients with F2. Statistically significant differences (p < 0.05) among patients according to fibrosis progression rate (C): (a) healthy control; (b) HIV-infected patients; (c) HIV/HCV-coinfected patients with low fibrosis progression (FPR <0.08); (d) HIV/HCV-coinfected patients with high fibrosis progression (FPR ≥0.08). HCV hepatitis C virus; HIV human immunodeficiency virus; TTV torque teno virus; TTMV torque teno mini virus
The viral load of TTV was not significantly different between HIV/HCV-coinfected patients with different fibrosis stages and FPR, but these three groups of patients coinfected with HIV and HCV had higher viral loads of TTV compared to the HIV-group and the Control-group (Fig. 3b–c). However, HIV/HCV-coinfected patients with significant fibrosis (F2), advanced fibrosis (F ≥ 3), and high fibrosis progression (FPR ≥0.08) had the highest viral loads of TTMV (p < 0.05) (Fig. 3b–c).
Logistic regression analyses showed that HIV/HCV-coinfected patients with high TTV load (viral load >2.78 log copies/μL) had increased odds of having advanced fibrosis (F3/F4) or severe necroinflammatory activity grade (A3) in the liver biopsy (Table 3). Moreover, HIV/HCV-coinfected patients with high TTMV load (viral load >1.88 log copies/μL) had decreased odds of having no/minimal fibrosis (F0/F1) and no/mild activity grade (A0/A1), and increased odds of having a high fibrosis progression (FPR ≥0.08) (Table 3).
No association was found between the viral load of these anelloviruses and CD4+ T-cell counts, prior AIDS, HCV viral load, and HCV genotype (data not shown).
Discussion
In this study, we found a high prevalence of TTV and TTMV infections in HIV/HCV-coinfected patients and an association between the plasma viral load of these anelloviruses and advanced stages of liver disease.
The prevalence of TTV and TTMV in the European population is very high [28]. In our study, infections with TTV and TTMV were extremely prevalent in the healthy blood donors (Control-group) and more than half of the blood donors were infected by both anelloviruses. The explanation for why TTV and TTMV infections were not detected in all subjects remains unknown, but it could reflect low viral infectivity, the presence of neutralizing antibodies in blood donors, technical limitations since the TTV and TTMV might be below the limit of detection of our RT-PCR, or the presence of minor transmitted variants in recipients with an existing related infection. Moreover, in the cases of detected infection, TTV/TTMV infections might suggest the presence of mechanisms of immune evasion that have evolved in TTV and TTMV to establish a persistent infection in immunocompetent individuals [29]. The TT viruses seem to be a well-adapted human virus and have been a persistent source of infection since the distant past. It has been suggested that TT viruses are commensal in normal conditions and do not cause any disease per se [30]. However, TT viruses possibly behave as opportunistic pathogens, causing harm only under exceptional circumstances [29].
Debilitating diseases and several comorbidities that are associated with some degree of immune dysfunction have been associated with an increased prevalence of infections with TT viruses [5, 13]. Although it remains unclear what role the immune system plays in the natural course of TT viruses infection, previous studies have found associations between TTV and TTMV and severe immunodeficiency in HIV patients and other immunocompromised individuals [10, 11, 31–33]. We were unable to find a correlation between CD4+ cell count and CDC stage of HIV infection with an increased frequency of infection with TTV and TTMV or their viral loads (data not shown). Nevertheless, it must be taken into consideration that all our patients had more than 200 CD4+/mm3, and most of them were undergoing effective treatment with HAART on a long-term basis. However, we found a correlation between complete suppression of HIV viremia and lower viral load of TTV and TTMV. On one hand, previous data have shown that short-term cultures of phytohemagglutinin-stimulated peripheral lymphocytes, but not resting lymphocytes, permit a measurable level of TTV replication, indicative of at least a moderate degree of lymphotropism [34]. On the other hand, Madsen et al. reported that HAART lead to an immediate and significant reduction in HIV viral load, followed by a significant reduction in TTV load [15]. It is possible that HIV replication benefits the immune evasion of TTV and TTMV due to HIV-related immune dysfunction, resulting in higher replication rates [32]. At the same time, it has been shown that the control of HIV replication and CD4+ levels are associated with liver disease progression [35, 36]. So, HIV-related immune status, TT viruses replication level, and liver disease progression may be three possible factors interrelated in the setting of HIV/HCV coinfection.
The key finding of our study is the greater viral load of TTV and TTMV in HIV/HCV-coinfected patients, with greater severity of liver disease. However, we did not show any data on how increased replication of both TT viruses could enhance HCV-mediated liver damage. Despite this, we should not rule out the possible cytopathic effect of these TT viruses in the liver and the enhancement of liver damage caused by HCV infection. On one hand, TT viruses can replicate in the liver [16] and have the potential of causing acute liver disease by themselves [17, 37, 38]. On the other hand, TT viruses were associated with chronic liver disease in association with HCV infection [20–22, 39, 40], suggesting that both TT viruses could enhance HCV-mediated liver cirrhosis and subsequent complications. However, other reports have not shown that coinfection with TTV affects the clinicopathological course of chronic hepatitis C in HCV-monoinfected patients [18, 41].
Moreover, the exact role of TTV and TTMV in HIV/HCV-coinfected patients has not been completely defined, although there is some evidence that TTV infection is associated with higher levels of alanine aminotransferase (ALT) in HCV/HIV-coinfected patients than in patients infected with HIV or HCV alone [42]. In our study, we found an association between high TTV and TTMV loads with advanced stages of liver disease and high FPR after adjusting for the main clinical and epidemiological variables that may affect the progression of liver fibrosis. It is possible that the immune disturbance caused by HIV infection allows increased replication of TTV and TTMV in the liver, which might generate an additional inflammatory response and liver fibrosis in concert with concurrent HCV infection. Thus, TTV and TTMV loads might be an indirect marker of liver disease in chronic hepatitis C of patients infected with HIV and HCV.
There are several limitations in the current study. First, the study design is cross-sectional with a low number of patients, and we do not show any data which may confirm a direct action of TT viruses on liver disease. However, our data only confirm a direct relationship between TT viruses replication and advanced hepatic stages in liver biopsies. Second, the patients selected for our study were patients who met a specific set of criteria for starting HCV treatment (e.g., little alcohol abuse, high CD4 cell counts, controlled HIV replication, and good treatment adherence), and it is possible that this may have introduced a selection bias. Third, we did not provide any data of hepatic biopsy in HIV-infected patients without chronic hepatitis C and in blood donors. We found a large prevalence of both viruses in HIV-infected patients and in blood donors, but we did not show any association with liver disease in those groups. Fourth, we did not study other viruses like hepatitis G virus (HGV), which has been associated with hepatitis and liver disease, although the true influence between HGV and the clinical course of chronic hepatitis C remains uncertain [43, 44].
Our data show that HIV/HCV-coinfected patients have a high prevalence of both TTV and TTMV infections, and these anelloviruses were associated with advanced fibrosis and severe activity grade. These two viruses might play a role in the development of liver disease in immunodeficiency patients, such as the patients coinfected with HIV and HCV.
References
Nishizawa T, Okamoto H, Konishi K, Yoshizawa H, Miyakawa Y, Mayumi M (1997) A novel DNA virus (TTV) associated with elevated transaminase levels in posttransfusion hepatitis of unknown etiology. Biochem Biophys Res Commun 241(1):92–97
Takahashi K, Iwasa Y, Hijikata M, Mishiro S (2000) Identification of a new human DNA virus (TTV-like mini virus, TLMV) intermediately related to TT virus and chicken anemia virus. Arch Virol 145(5):979–993
Huang LY, Øystein Jonassen T, Hungnes O, Grinde B (2001) High prevalence of TT virus-related DNA (90%) and diverse viral genotypes in Norwegian blood donors. J Med Virol 64(3):381–386
Takahashi K, Hoshino H, Ohta Y, Yoshida N, Mishiro S (1998) Very high prevalence of TT virus (TTV) infection in general population of Japan revealed by a new set of PCR primers. Hepatol Res 12:233–239
Okamoto H (2009) History of discoveries and pathogenicity of TT viruses. Curr Top Microbiol Immunol 331:1–20
Davidson F, MacDonald D, Mokili JLK, Prescott LE, Graham S, Simmonds P (1999) Early acquisition of TT virus (TTV) in an area endemic for TTV infection. J Infect Dis 179(5):1070–1076
Ball JK, Curran R, Berridge S, Grabowska AM, Jameson CL, Thomson BJ, Irving WL, Sharp PM (1999) TT virus sequence heterogeneity in vivo: evidence for co-infection with multiple genetic types. J Gen Virol 80(Pt 7):1759–1768
Sugiyama K, Goto K, Ando T, Mizutani F, Terabe K, Kawabe Y, Wada Y (1999) Route of TT virus infection in children. J Med Virol 59(2):204–207
Simmonds P, Davidson F, Lycett C, Prescott LE, MacDonald DM, Ellender J, Yap PL, Ludlam CA, Haydon GH, Gillon J, Jarvis LM (1998) Detection of a novel DNA virus (TTV) in blood donors and blood products. Lancet 352(9123):191–195
Shibayama T, Masuda G, Ajisawa A, Takahashi M, Nishizawa T, Tsuda F, Okamoto H (2001) Inverse relationship between the titre of TT virus DNA and the CD4 cell count in patients infected with HIV. AIDS 15(5):563–570
Christensen JK, Eugen-Olsen J, Sorensen M, Ullum H, Gjedde SB, Pedersen BK, Nielsen JO, Krogsgaard K (2000) Prevalence and prognostic significance of infection with TT virus in patients infected with human immunodeficiency virus. J Infect Dis 181(5):1796–1799
Okamoto H, Nishizawa T, Ukita M (1999) A novel unenveloped DNA virus (TT virus) associated with acute and chronic non-A to G hepatitis. Intervirology 42(2–3):196–204
Focosi D, Maggi F, Albani M, Macera L, Ricci V, Gragnani S, Di Beo S, Ghimenti M, Antonelli G, Bendinelli M, Pistello M, Ceccherini-Nelli L, Petrini M (2010) Torquetenovirus viremia kinetics after autologous stem cell transplantation are predictable and may serve as a surrogate marker of functional immune reconstitution. J Clin Virol 47(2):189–192
Kaufmann GR, Elzi L, Weber R, Furrer H, Giulieri S, Vernazza P, Bernasconi E, Hirschel B, Battegay M; Swiss HIV Cohort Study (2011) Interruptions of cART limits CD4 T-cell recovery and increases the risk for opportunistic complications and death. AIDS 25(4):441–451
Madsen CD, Eugen-Olsen J, Kirk O, Parner J, Kaae Christensen J, Brasholt MS, Ole Nielsen J, Krogsgaard K (2002) TTV viral load as a marker for immune reconstitution after initiation of HAART in HIV-infected patients. HIV Clin Trials 3(4):287–295
Okamoto H, Ukita M, Nishizawa T, Kishimoto J, Hoshi Y, Mizuo H, Tanaka T, Miyakawa Y, Mayumi M (2000) Circular double-stranded forms of TT virus DNA in the liver. J Virol 74(11):5161–5167
Okamoto H, Nishizawa T, Kato N, Ukita M, Ikeda H, Iizuka H, Miyakawa Y, Mayumi M (1998) Molecular cloning and characterization of a novel DNA virus (TTV) associated with posttransfusion hepatitis of unknown etiology. Hepatol Res 10(1):1–16
Kao JH, Chen W, Chen PJ, Lai MY, Chen DS (2000) TT virus infection in patients with chronic hepatitis B or C: Influence on clinical, histological and virological features. J Med Virol 60(4):387–392
Charlton M, Adjei P, Poterucha J, Zein N, Moore B, Therneau T, Krom R, Wiesner R (1998) TT-virus infection in North American blood donors, patients with fulminant hepatic failure, and cryptogenic cirrhosis. Hepatology 28(3):839–842
Ikeda H, Takasu M, Inoue K, Okamoto H, Miyakawa Y, Mayumi M (1999) Infection with an unenveloped DNA virus (TTV) in patients with acute or chronic liver disease of unknown etiology and in those positive for hepatitis C virus RNA. J Hepatol 30(2):205–212
Tokita H, Murai S, Kamitsukasa H, Yagura M, Harada H, Takahashi M, Okamoto H (2002) High TT virus load as an independent factor associated with the occurrence of hepatocellular carcinoma among patients with hepatitis C virus-related chronic liver disease. J Med Virol 67(4):501–509
Zein NN, Arslan M, Li H, Charlton MR, Gross JB Jr, Poterucha JJ, Therneau TM, Kolbert CP, Persing DH (1999) Clinical significance of TT virus infection in patients with chronic hepatitis C. Am J Gastroenterol 94(10):3020–3027
Moriyama M, Matsumura H, Shimizu T, Shioda A, Kaneko M, Miyazawa K, Miyata H, Tanaka N, Uchida T, Arakawa Y (2001) Histopathologic impact of TT virus infection on the liver of type C chronic hepatitis and liver cirrhosis in Japan. J Med Virol 64(1):74–81
Alvarez do Barrio M, González Díez R, Hernández Sánchez JM, Oyonarte Gómez S (2005) Residual risk of transfusion-transmitted viral infections in Spain, 1997–2002, and impact of nucleic acid testing. Euro Surveill 10(2):20–22
Jacobs WH, Goldberg SB, Balint JA, Boyce HW, Browning TH, Cooper JN, Earnest DL, Friedman E, Greene M, Mellow MA, Pitt HA, Todaro JL; Patient Care Committee of the American Gastroenterological Association (1989) Statement on outpatient percutaneous liver biopsy. Dig Dis Sci 34(3):322–323
Bedossa P, Poynard T (1996) An algorithm for the grading of activity in chronic hepatitis C. The METAVIR Cooperative Study Group. Hepatology 24(2):289–293
Moen EM, Sleboda J, Grinde B (2002) Real-time PCR methods for independent quantitation of TTV and TLMV. J Virol Methods 104(1):59–67
Biagini P, Gallian P, Touinssi M, Cantaloube JF, Zapitelli JP, de Lamballerie X, de Micco P (2000) High prevalence of TT virus infection in French blood donors revealed by the use of three PCR systems. Transfusion 40(5):590–595
Maggi F, Bendinelli M (2009) Immunobiology of the Torque teno viruses and other anelloviruses. Curr Top Microbiol Immunol 331:65–90
Griffiths P (1999) Time to consider the concept of a commensal virus? Rev Med Virol 9(2):73–74
Zhong S, Yeo W, Tang MW, Lin XR, Mo F, Ho WM, Hui P, Johnson PJ (2001) Gross elevation of TT Virus genome load in the peripheral blood mononuclear Cells of cancer patients. Ann N Y Acad Sci 945:84–92
Touinssi M, Gallian P, Biagini P, Attoui H, Vialettes B, Berland Y, Tamalet C, Dhiver C, Ravaux I, De Micco P, De Lamballerie X (2001) TT virus infection: prevalence of elevated viraemia and arguments for the immune control of viral load. J Clin Virol 21(2):135–141
Thom K, Petrik J (2007) Progression towards AIDS leads to increased torque teno virus and torque teno minivirus titers in tissues of HIV infected individuals. J Med Virol 79(1):1–7
Mariscal LF, López-Alcorocho JM, Rodríguez-Iñigo E, Ortiz-Movilla N, de Lucas S, Bartolomé J, Carreño V (2002) TT virus replicates in stimulated but not in nonstimulated peripheral blood mononuclear cells. Virology 301(1):121–129
Reiberger T, Ferlitsch A, Sieghart W, Kreil A, Breitenecker F, Rieger A, Schmied B, Gangl A, Peck-Radosavljevic M (2010) HIV-HCV co-infected patients with low CD4+ cell nadirs are at risk for faster fibrosis progression and portal hypertension. J Viral Hepat 17(6):400–409
Thorpe J, Saeed S, Moodie EE, Klein MB; Canadian Co-infection Cohort Study (CTN222) (2011) Antiretroviral treatment interruption leads to progression of liver fibrosis in HIV-hepatitis C virus co-infection. AIDS 25(7):967–975
Shang D, Lin YH, Rigopoulou I, Chen B, Alexander GJM, Allain JP (2000) Detection of TT virus DNA in patients with liver disease and recipients of liver transplant. J Med Virol 61(4):455–461
Bendinelli M, Pistello M, Maggi F, Fornai C, Freer G, Vatteroni ML (2001) Molecular properties, biology, and clinical implications of TT virus, a recently identified widespread infectious agent of humans. Clin Microbiol Rev 14(1):98–113
Moriyama M, Matsumura H, Shimizu T, Shioda A, Kaneko M, Miyazawa K, Miyata H, Tanaka N, Uchida T, Arakawa Y (2001) Histopathologic impact of TT virus infection on the liver of type C chronic hepatitis and liver cirrhosis in Japan. J Med Virol 64(1):74–81
Sioda A, Moriyama M, Matsumura H, Kaneko M, Tanaka N, Arakawa Y (2001) Clinicopathological features of serum TTV DNA-positive non-A-G liver diseases in Japan. Hepatol Res 21(2):169–180
Masia G, Ingianni A, Demelia L, Faa G, Manconi PE, Pilleri G, Ciancio A, Rizzetto M, Coppola RC (2001) TT virus infection in Italy: prevalence and genotypes in healthy subjects, viral liver diseases and asymptomatic infections by parenterally transmitted viruses. J Viral Hepat 8(5):384–390
Shieh B, Chang MJ, Ko WC, Chen EJ, Wu JC, Lee CF, Chang TT, Li C (2003) Effects of multiple virus coinfections on disease progression in HIV-positive patients. Intervirology 46(2):105–113
Hofer H, Aydin I, Neumueller-Guber S, Mueller C, Scherzer TM, Staufer K, Steindl-Munda P, Wrba F, Ferenci P (2011) Prevalence and clinical significance of GB virus type C/hepatitis G virus coinfection in patients with chronic hepatitis C undergoing antiviral therapy. J Viral Hepat 18(7):513–517
Moriyama M, Matsumura H, Shimizu T, Shioda A, Kaneko M, Saito H, Miyazawa K, Tanaka N, Sugitani M, Komiyama K, Arakawa Y (2000) Hepatitis G virus coinfection influences the liver histology of patients with chronic hepatitis C. Liver 20(5):397–404
Acknowledgments
Additional contributions
We acknowledge the patients in this study for their participation and the Centro de Transfusión of Comunidad de Madrid for the healthy donor blood samples provided.
Potential conflicts of interest
None for all authors.
Funding/support
This work has been supported by grants from the “Instituto de Salud Carlos III (ISC-III)” (PI08/0738 and PI11/00245) to S.R.; from ISC-III (ref. ISCIII-RETIC RD06/006, PI08/0928) and the “Fundación para la Investigación y la Prevención del Sida en España” (FIPSE) (ref. 36443/03; ref. 361020/10) to J.B.; from ISC-III (INTRASALUD; RD09/0076/00103), Red RIS RD06-0006-0035, FIPSE (240800/09, 300509), and Fundación Caja Navarra and Comunidad de Madrid (S-SAL-0159-2006) to M.A.M.F. M.G.-F. and M.G.-A. are supported by a grant of Instituto de Salud Carlos III (CM09/00031 and CM08/00101, respectively). J.B. is supported by a grant from the “Programa de Intensificación de la Actividad Investigadora en el SNS” (I3SNS).
Writing assistance: Dr. Nick Weber provided writing assistance for this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
García-Álvarez, M., Berenguer, J., Álvarez, E. et al. Association of torque teno virus (TTV) and torque teno mini virus (TTMV) with liver disease among patients coinfected with human immunodeficiency virus and hepatitis C virus. Eur J Clin Microbiol Infect Dis 32, 289–297 (2013). https://doi.org/10.1007/s10096-012-1744-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-012-1744-1