
Abstract
Recent reports of increased rates of gonorrhea initiated an analysis of secular trends of gonorrhea in a young adult population. Gonorrhea is a notifiable disease in the Israel Defense Forces. The diagnosis is based on the typical clinical presentation, relevant epidemiologic data, and positive bacteriological culture. For the present study, the archives of the Epidemiology Department were reviewed for all documented cases of gonorrhea from January 1, 1978 to December 31, 2008, and the annual and seasonal incidence rates were calculated. Annual gonorrhea rates decreased from 2.3 cases per 1,000 soldiers in 1978 to an all-time low of 0.07 cases per 1,000 soldiers in 2008, representing a 97% decline. Multi-year average monthly rates varied from a low of 5.83 cases per 100,000 population in February to a high of 8.97 cases per 100,000 in August. The difference in the person-time incidence (PTI) rates for winter (5.9 cases per 100,000 person-years) and summer (6.8 cases per 100,000 person-years) was statistically significant (p < 0.01). Analyzing the long-term epidemiology of gonorrhea has shown that the infection rate is continuously decreasing and that it appears to be more prevalent in the warmer months.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Sexually transmitted diseases (STDs) constitute a major public health problem with important long-term consequences. Gonorrhea is the most prevalent of the STDs, affecting an estimated number of more than 330,000 persons annually in the USA alone [1]. Gonorrhea has a major impact on reproductive health and increases the risk of transmission of human immunodeficiency virus (HIV).
Secular trends of STDs have been traditionally enigmatic for researchers, and dynamic changes are very frequent. It is clear that, with a better understanding of the annual and seasonal trends of gonorrhea, efforts against the spread of the disease can be more timely, accurate, and effective.
Earlier studies monitoring Neisseria gonorrhoeae infection in the Israeli population reported a significant decline in the rates of occurrence starting in the early 1970s. Surprisingly, however, there has been a reversal in this trend in the last decade in the civilian sector [2].
Since the end of the 1970s, gonorrhea is a notifiable disease in the Israel Defense Forces (IDF) and physicians are required to routinely report all cases of suspected or confirmed gonorrhea in military personnel to the Military Health Branch Epidemiology Department. This mandatory notification has yielded a unique, large-population database on the disease. For the present study, we reviewed this database to investigate the annual patterns and seasonality of gonorrhea in the military sector and to suggest possible interventions.
Patients and methods
The archives of the Military Health Branch Epidemiology Department were carefully reviewed for all documented cases of gonorrhea from January 1, 1978 (start of mandatory notification) to December 31, 2008 (latest available data).
Our analysis covered all compulsory and career IDF personnel. Military duty in Israel is compulsory for all male and female citizens aged 18 years. About 10% of the men and 30% of the women are exempted from service, mainly for religious reasons. Reserve personnel were excluded from the study.
The diagnosis of gonorrhea infection in the IDF is based on the clinical presentation, relevant epidemiologic data, microscopic visualization of diplococci, and confirmation with a positive bacterial culture. For the present study, cases of gonorrhea infection were identified by the diagnosis reported by the military physician on the notification form.
The annual incidence of gonorrhea in the civilian population was extracted from publications of the Epidemiology Department of the Israeli Ministry of Health.
Statistical analysis
The annual incidence of laboratory-confirmed gonorrhea cases was calculated by dividing the number of cases each year by the military population (or civilian population, as reported by the Israel Central Bureau of Statistics) in the same year. We calculated the rate ratio between the military and the civilian incidence of gonorrhea, and analyzed the time trend of these ratios for the following periods: 1978–1988; 1989–1995; 1996–2008. The Chi-square statistic for trend was computed. The person-time incidence (PTI) rates of gonorrhea for summer (April to September) and winter (October to March) were calculated on the basis of the ratio of the number of cases during the period under study to the product of 6 months and the average monthly number of soldiers in each year. The two-tailed binomial test was used to compare PTI rates between summer and winter. All statistical tests were performed with the Computer Program for Epidemiological Analysis (PEPI, version 2.07; copyright JH Abramson & PM Gahlinger, 1993–97).
Results
The age and sex distribution of the study population for the whole period was as follows: male conscripts (aged 18–21 years), 53%; female conscripts (aged 18–20 years), 25%; male career personnel (aged 22–45 years), 19%; and female career personnel (aged 21–45 years), 3%.
Annual epidemiology
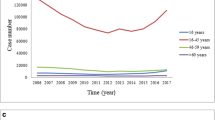
There was a steep decline in the annual incidence rates over this first decade, followed by a gradual decline from 1988–2008, punctuated by several peaks. Gonorrhea rates dropped from 2.3 cases per 1,000 soldiers in 1978 to a period low of 0.07 cases per 1,000 soldiers in 2008, representing a 97% decline (Fig. 1). Two periods were characterized by elevated annual incidence rates: between 1988 to 1990 and between 1999 to 2003 (Fig. 1). The trends of gonorrhea rates in the civilian population closely match those of the military population with some differences: between 1978 and 1988, the ratio between the military and civilian incidences declined from 12.7 in 1978 to 7.6 in 1988 (p < 0.001). In 1989, the ratio increased to 21.5 and continued to increase until 1995, when it reached a peak of 50.9 (p < 0.001). Since 1996, the ratio continuously declined to 10.8 in 1998 and 2.3 in 2008 (p < 0.001).

Gonorrhea in the Israel Defense Forces and the civil sector 1978–2008: rates per 1,000 soldiers and per 10,000 civilians
Seasonal epidemiology
The seasonal incidence of gonorrhea in the military population is presented in Fig. 2. The average monthly rates varied from a low of 5.83 cases per 100,000 population in February to a high of 8.97 cases per 100,000 in August. The difference in the PTI rates for winter (5.9 cases per 100,000 person-years) and summer (6.8 cases per 100,000 person-years) was statistically significant (p < 0.01).

Seasonal trends of gonorrhea in the Israel Defense Forces 1978–2008
Discussion
The results of this long term follow-up suggest that the rates of gonorrhea in the IDF have decreased significantly over the last 30 years, with occasional peaks. Interestingly, a clear seasonal pattern with a predominance of the infection in the warmer months of the year was noted.
The gradual decline in the incidence of gonorrhea from the last years of the 1980s to the end of 1999 in both the military and civilian populations in Israel was explained mainly by the worldwide HIV epidemic. Researchers believe that widespread fear of HIV infection led to safer sexual practices and to an overall decline in all STDs [3]. This trend was true not only for Israel, but also for Europe and the USA, and was supported by studies reporting a correlation of the rise in prevalence of anti-HIV antibodies in homosexual and bisexual men with a decline in the rates of gonorrhea [4, 5]. We were not able to see if this correlation is valid also for other STDs, such as syphilis and HIV, due to the extremely low incidence of these diseases in the IDF.
It has been interesting to notice a gradual increase in the rates of gonorrhea since 1999, in both the Israeli civilian and military populations [6]. The age group responsible for the rise in the civilian population was identified as 15–44 years, which is very similar to the ages of members in the army [5]. Interestingly, the increase in the civilian incidence which was observed in 1999 and onwards was steeper in the civilian population than the IDF population. This changing trend seems not to be unique to Israel as well, and has been observed in other countries such as Sweden and the United Kingdom [7]. The cause for this resurgence is unknown, although several possible mechanisms have been proposed. Some authors have suggested that recent advances in the prevention and treatment of acquired immune deficiency syndrome (AIDS), including pre- and post-exposure prophylaxis and the introduction of sophisticated anti-viral drugs and regimens, have helped to contain the epidemic in Western countries, but, paradoxically, has lowered the level of awareness of the disease and, thereby, led to more risky sexual behavior. It is also possible that changes in sexual habits and increasing promiscuity have contributed to the growing infection rates. Furthermore, in Israel and other Western countries, there has been a considerable influx of foreign workers from third-world countries where rates of STDs are high, and an overall increase in the availability and scope of the sex trade.
In the IDF, however, studies have failed to detect any changes in the sexual behavior of soldiers (Grotto I., unpublished data), even though the rise in gonorrhea rates up to 2002 parallel those in the general Israeli civilian population and other European countries [2, 7].
Other explanations for the trend reversal include a natural cyclical disease flux and possible changes in the immunogenicity of the culprit organism. The latter hypothesis is supported by worldwide reports of an increase in the antibiotic resistance of gonococci [8], including in Israel [9].
The rise in gonorrhea incidence in the IDF during the years 1999–2002 paralleled a similar rise in incidence rates among the general Israeli civilian population, and matched the increasing rates in the United Kingdom and several other European countries [2, 7]. Following this surge, several interventional steps were undertaken in order to control the disease incidence. The IDF and the Israel Ministry of Health intensified health education and prevention programs administered by the Public Health Service and an outreach program providing free health examinations for sex workers has been initiated by the Ministry’s District Health Offices in major metropolitan areas. Our data show that the upswing in annual incidence rates observed starting from 1999 reversed course in 2003, and has continued in a declining trend through 2008.
Our data clearly demonstrate that gonorrhea infection is more prevalent in the summer. This finding is consistent with previous reports on the seasonality of gonorrhea [10] and other STDs [11–14]. The seasonality of the disease may be, at least partly, explained by seasonal variations in sexual activity as a result of environmental or biological factors. Reinberg and Lagoguey [15], for example, demonstrated higher levels of testosterone in the fall months, peaking in October.
Military service could be a risk factor for STD, as was shown in the US army [16].
This study has several limitations. It is possible that the reporting system has a delay that may affect the seasonal analysis, although it is extremely unlikely that this factor would affect data collected over a period of 30 years. As opposed to the civilian reporting system that is based on laboratory verification, we suspect that not all physicians’ reported IDF cases of gonorrhea were indeed confirmed with a positive bacterial culture; however, it is again unlikely that this would affect a long-term analysis. Another limitation of the study is that cases of gonorrhea may have been omitted from the analysis if soldiers turned to private civilian practitioners for diagnosis and treatment while on leave. Such cases would not be reported through military channels. The database does not contain any data regarding the mode of transmission, thus, reducing the possibility of focusing on the exact causes and target populations. Finally, although gonorrhea is a notifiable disease, the possibility of both civilian and military under-reporting still exists. In this study, we could not adjust our incidence rates for age, gender, and ethnicity, which definitely makes the comparison between the military and the civilian sector inadequate.
With awareness to the changing trends of gonorrhea, preventive measures against rapid spread can be more effective. Consequently, the increased rates of gonorrhea in the civilian sector, as well as the military population, between the years 1999–2003 has drawn the attention of the Ministry of Health, and specialized free, anonymous outpatient clinics have been made available to the public. Methods for mitigating the resurgence include health education and careful epidemiologic investigation of all cases, with treatment of contacts, when necessary.
In its ongoing effort to prevent and treat STDs among soldiers, the IDF Medical Corps maintains a range of health promotion and intervention programs aimed at both the population and individual levels. All military units are required to conduct periodic health education seminars, several curricular components of which address STD prevention. An AIDS awareness campaign is conducted annually in the IDF, in conjunction with the Israel Ministry of Health, during the period around World AIDS Day. Educational and informational leaflets on sexual health are distributed on central military bases and at major transportation hubs, medical clinics, and women’s health centers. These include, among other topics, information on contraception, STD prevention, and the availability of an anonymous, non-military walk-in STD clinic in Tel Aviv, which sees soldiers unwilling to present at conventional military clinics. Furthermore, the IDF Medical Corps conducts an ongoing survey of soldiers’ knowledge, attitudes, and practices regarding sexual health, in an effort to guide and focus health education and promotion messages within the military. It appears that this intervention has contributed to the trend reversal. Our data also suggests that particular attention should be devoted to the increased rates during the summer season.
References
Centers for Disease Control and Prevention (CDC) (2009) Sexually transmitted diseases surveillance, 2008. Available online at: http://www.cdc.gov/std/stats08/gonorrhea.htm
Green MS, Anis E, Gandacu D, Grotto I (2003) The fall and rise of gonorrhoea incidence in Israel: an international phenomenon? Sex Transm Infect 79:116–118
Gellan MCA, Ison CA (1986) Declining incidence of gonorrhoea in London: a response to fear of AIDS? Lancet 2:920
Carne CA, Weller IVD, Johnson AM, Loveday C, Pearce F, Hawkins A, Smith A, Williams P, Tedder RS, Adler MW (1987) Prevalence of antibodies to human immunodeficiency virus, gonorrhoea rates, and changed sexual behaviour in homosexual men in London. Lancet 1:656–658
Ministry of Health, State of Israel (2006) Notifiable infectious diseases in Israel: 54 years of surveillance, 1951–2004. Available online at: http://www.health.gov.il/Download/pages/zihum2004_161209.pdf
Centers for Disease Control and Prevention (CDC) (2009) Sexually transmitted diseases surveillance, 2008, Table 1.Available online at: http://www.cdc.gov/std/stats08/tables/1.htm
Berglund T, Unemo M, Olcén P, Giesecke J, Fredlund H (2002) One year of Neisseria gonorrhoeae isolates in Sweden: the prevalence study of antibiotic susceptibility shows relation to the geographic area of exposure. Int J STD AIDS 13:109–114
Ehret JM, Judson FN (1998) Quinolone-resistant Neisseria gonorrhoeae: the beginning of the end? Report of quinolone-resistant isolates and surveillance in the southwestern United States, 1989 to 1997. Sex Transm Dis 25:522–526
Yagupsky P, Schahar A, Peled N, Porat N, Trefler R, Dan M, Keness Y, Block C (2002) Increasing incidence of gonorrhea in Israel associated with countrywide dissemination of a ciprofloxacin-resistant strain. Eur J Clin Microbiol Infect Dis 21:368–372
Schroeder B, Tetlow P, Sanfilippo JS, Hertweck SP (2001) Is there a seasonal variation in gonorrhea and chlamydia in adolescents? J Pediatr Adolesc Gynecol 14:25–27
Albus C, Köhler G (1988) Is there a seasonal incidence of acute adnexitis? Zentralbl Gynakol 110:824–826
Damiba AE, Vermund SH, Kelley KF (1990) Rising trend of reported gonorrhoea and urethritis incidence in Burkina Faso from 1978 to 1983. Trans R Soc Trop Med Hyg 84:132–135
Ross JD, Scott GR (1992) Seasonal variation in gonorrhoea. Eur J Epidem 8:252–255
Wright RA, Judson FN (1978) Relative and seasonal incidences of the sexually transmitted diseases. A two-year statistical review. Br J Vener Dis 54:433–440
Reinberg A, Lagoguey M (1978) Circadian and circannual rhythms in sexual activity and plasma hormones (FSH, LH, testosterone) of five human males. Arch Sex Behav 7:13–30
Seña AC, Miller WC, Hoffman IF, Chakraborty H, Cohen MS, Jenkins P, McKee KT Jr (2000) Trends of gonorrhea and chlamydial infection during 1985–1996 among active-duty soldiers at a United States Army installation. Clin Infect Dis 30:742–748
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mimouni, D., Bar-Zeev, Y., Davidovitch, N. et al. Secular trends of gonorrhea in young adults in Israel: three decades of follow-up. Eur J Clin Microbiol Infect Dis 29, 1111–1115 (2010). https://doi.org/10.1007/s10096-010-0969-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10096-010-0969-0